Embed Size (px)
Citation preview

The Case for SIF Investigation
Serious Injury and Fatality Events
Paul English, CSP, CHST
ASSP Region III PDC

Learning Outcomes
1. Define what a SIF event is for your organization
2. Tools to remove subjectivity from identifying SIF events
3. Information to help categorize events to create SIF trends
2

What is a SIF?
• https://www.youtube.com/watch?v=myNSOBv18uY
3

What are Serious Injury or Fatality Events,SIF?
Life Threatening Event or Exposure
• An incident that if not immediately addressed is likely to lead to the death of the affected individual, and will usually require intervention of internal and/or external emergency response personnel to provide life-sustaining support.
• Laceration or crushing injuries that result in significant blood loss
• An injury involving damage to the brain or spinal cord
• An event that requires application of CPR or an external defibrillator
• Chest or abdominal trauma affecting vital organs
• Serious burns
Life Altering Event or Exposure
• An incident that results in permanent and significant loss of a major body part or organ function that permanently changes or disables that person’s normal life.
• Significant head injuries
• Spinal cord injuries
• Paralysis
• Major amputations
• Broken or fractured bones
• Serious burns
4

When we look for SIF events, we are looking for potential..
Injury Case Description SIF?
Fractured Foot
AEE was caught between a forklift that was backing up.
The forklift did not have an audible backup alarm working.
BEE was climbing out of a forklift when they slipped
and fell due to loose rock on the ground.
Strained Back
AEE was walking across the floor and slipped on some grease. He caught himself on a handrail before failing
to the ground.
B
EE was working on the top of a railcar when the railcar he was on was struck by another when the switching
crew was spotting railcars. EE fell off railcar to the ground sustaining some bruises and a sprained back.
Source: Determining SIF Exposure Potential, Martin and Stricoff, 2012 pg. 3
5

Is this a SIF Event?
6

Did the incident involve a lifesaving safety policy….• Lockout-Tagout
• Confined Space Entry
• Equipment Related• Caught Between• Line of Fire• Release of Significant Energy or Mass
• Mobile Equipment Collisions
• Liquid Metal Breach or Contact
• Working at Heights
• Machine Guarding & Barricades
• Electrical Hazards
• Suspended Loads
• Cardinal Rule Violations• LOTO• Rail Safety• Confined Space• Suspended Loads• Fall Protection
7

What is the Worst Probable Outcome?
• A PROBABLE outcome is not the same as a POSSIBLE outcome.
• For Example…….
• A slip/fall on a sidewalk could result in permanent disability or death, but this is not probable.
• When a stack of crushed cars falling off a flatbed trailer narrowly misses the driver, the worst probable outcome is clearly a fatality.
8

Do facilities that fall under PSM rule already do this??• Process Hazard Analysis, PHA
• 1910.119(e)• What-if• Checklist• What-if/Checklist• Hazard and Operability Study HAZOP• Failure Mode and Effects Analysis
FMEA• Fault Tree Analysis
• Are we trying to increase Subjectivity?
9

Tools to remove subjectivity from
identifying SIF eventsThe Case for SIF Investigation
10

What’s the main concern about rolling out a program like this?
11

Avoid Complicated Severity Tools
• ALARP
• Possible
• ALARA
• Achievable
• SFAIRP
• So Far As Is Reasonably Practicable
12

13

Establish Your Own Process..
14

15

Is this a SIF Event?
16

Define Low Frequency/High Hazard Work..
• Excavation Projects
• Demolition / Construction Projects
• Asbestos / Lead Work Projects
• Scaffold Projects
• Crane / Rigging
• Working at Heights
• Machine Removal and Installation
• Other High Risk Projects identified by Engineering and Safety
17

Opposite of Subjectivity…
• Objectivity..
• Neutrality..
• Detachment..
• Impartiality..
• Avoid WHATABOUTISM….
• Avoid the “What If” Monster…
• Avoid stringing “what-ifs” together. If two or more “what-ifs” are needed to reach the worst probable outcome, the event would likely not be a SIF.
18

WHATABOUTISM…
19

Critical Thinking Skills
• Productive• Thinking that goes beyond observing and recalling facts
• Critical• Being able to ask questions and gather information
• Weighing & Solving• When you think critically you weigh evidence, solve
problems and make decisions
• Creating & Applying• When you think critically you create new ideas, and
turn information into a tool by applying what you have learned in previous situations to new situations
Productive
Critical
Weighing
Solving
Creating
Applying
20

Variation-The Silent Killer
• Shift your thinking from “Why” to “How”-Conklin
• Must look at the system, not the person
• Why did they feel that what they did was the right thing to do
• People do not intend to do a bad job
• Investigators keep digging until you understand why the decision was made
• Move past Human Error
Conklin, Pre-Accident Investigations pg. 71 21

What does the Blue Line represent from a quality standpoint?
• Deming’s Knowledge of Variation• “Why did something go wrong?”
• “Why are results so poor?”
• “How can we repeat this success?”
• Where is the Operational Safety Gap?
22

Information to help categorize events to
create SIF trendsThe Case for SIF Investigation
23

Categorize..
Controlling ProgramsConfined Space
Contractor/Visitor/Vendor
EAP/Fire PreventionElectrical
ErgonomicsHand Tools/Non-Powered
Hand Tools/PoweredHearing Conservation
Hot WorkHousekeeping
Incoming QualityLifting & RiggingLockout Tagout
Machine GuardingMobile Equipment
No Program or StandardOverhead Cranes
PPEPreventative Maintenance
Process ControlRail
Walking/Working SurfacesWork Instructions
Working at Heights
Substandard ActsCardinal Rule Violation
Failure to use PPE Properly
Failure to SecureFailure to Warn
Improper Manual Material HandlingImproper Position for Task
Making Safety Devices InoperableNo Substandard ActNon-Work Actions
Operating at Improper SpeedOperating Equipment without Authority
OtherRemoving Safety Devices
Servicing Equipment in OperationUnder Influence of Alcohol/Drugs
Using Defective EquipmentUsing Equipment Improperly
Substandard ConditionsCongestion or Restricted Action
Defective Tools, Equipment or Material
Ergonomics (tools/layout/process)Fire & Explosion Hazards
Improper Written ProceduresInadequate or Excessive Illumination
Inadequate Design
Inadequate Guards & BarriersInadequate or Improper Protective
Equipment
Inadequate VentilationInadequate Warning Systems
No Substandard Condition
Poor Housekeeping/Disorderly WorkplaceWorking/Walking Surfaces
Task/ActivityDriving, Operating, riding in Motor Vehicle
Maintenance and Repair (Emergency/Breakdown)
Maintenance/Construction/Repair - RoutineManual Assembly/Diassembly
Material Handling (including PIT & Crane)Not Performing Task (walking, breaks, etc.)
Office and Sales TasksOperating Machine/Tool/Equipment
OtherUnknown
Corrective Action(s) Permanent or Interim?Counseling/Advisement
Education
Enforcement
EngineeringMaintenance
Other
24

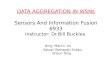
11 months of data…
Mobile Equipment
31%
Work Instruction/JS
A19%LOTO
18%
Rail Safety8%
Overhead Crane
8%
Process Control
16%
CONTROLLING POLICIES/PROGRAMS
Medical Treatment
10%
First Aid19%
Near Miss54%
Property Damage
13%
Liquid Metal Breach
4%
INCIDENT OUTCOMES
25

Why does data look like from a Contact Type standpoint?
Cardinal Rule Violation8%
Caught In/On/Between12%
Electrical Contact13%
Molten Metal7%
Struck by53%
Uncontrolled Energy/Line of Fire
7%
26

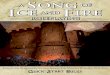
Incidents by Business Unit
Business A32%
Business B51%
Business C4%
Business D1% Business E
12%
LINES OF BUSINESS • Is this data skewed?
• What are the Business B Managers worried about?
• Why is your SIF rate so high?• Why are you having SIF events?
• Dr. Krause argues to create a SIF Rate• The SIF Rate is the number of serious and fatal
injuries and recordable injuries with high potential divided by hours worked.
• Data on the SIF Rate should be gathered for the past two-three years and from here forward monthly.
• The SIF Rate should be given high visibility throughout the organization.
Source: SIFs A New Framework for Serious Injury and Fatality Prevention, Thomas R. Krause, Ph.D. www.iup.edu/workspace 27

What would the SIF rate be?
• The SIF Rate is the number of serious and fatal injuries and recordable injuries with high potential divided by hours worked.
1. Gives visibility to SIF performance-as a leading and lagging indicator.
2. Enables new research needed to develop intervention strategies.
3. Enables root cause analysis of large numbers of SIF events.
4. Sets the stage for Predictive Analytics.
Source: SIFs A New Framework for Serious Injury and Fatality Prevention, Thomas R. Krause, Ph.D. www.iup.edu/workspace 28

SIF Event?
29

How are SIF events communicated?
30

Summary1. SIF Event Processes are not a magic bullet safety
program..
2. Expect a high level of incidents if you do start a SIF surveillance program. It will highlight incidents that should be getting due diligence..
3. Avoid subjectivity when identifying SIF events..
4. Categorize and quantify:
1. Controlling Programs
2. Substandard Acts & Conditions
3. Task/Activity
4. Corrective Action (Interim & Permanent)
5. DO NOT create a SIF Event Rate to measure incidents when starting program..
31

Suggested Reading on SIFs
• PREVENTING SERIOUS INJURIES AND FATALITIES (SIFs): A NEW STUDY REVEALS PRECURSORS AND PARADIGMS WHITE PAPER By Donald K. Martin and Alison Black
• A New Framework for Serious Injury and Fatality Prevention, Thomas R. Krause, Ph.D. IUP.EDU
• Todd Conklin: Pre-Accident Investigations
• Sidney Dekker: The Field Guide to Understanding Human Error
• Fred Manuele on Safety Management
32

Dr. Scotty Dunlap, EdD, CSP
• Article in Professional Safety for May Edition titled:• “Remodeling Heinrich: An Application for Modern Safety Management”
• Presented at National PDC, 6/10/19 Session S5118
33

Paul English, CSP, CHST
34