Embed Size (px)
DESCRIPTION
The Autopsy Pathology of Sepsis
Citation preview

ARTICLE IN PRESS
Current Diagnostic Pathology (2007) 13, 375–388
0968-6053/$ - sdoi:10.1016/j.c
�Tel.: +44 20E-mail addr
www.elsevier.com/locate/cdip
MINI-SYMPOSIUM: THE AUTOPSY IN SUDDEN UNEXPECTED ADULT DEATH
The autopsy pathology of sepsis-related death
Sebastian Lucas�
Department of Histopathology, KCL School of Medicine, St. Thomas’ Hospital, London SE1 7EH, UK
KEYWORDSSepsis;Shock;Autopsy;Apoptosis;Cirrhosis;Haemophagocytosis;Acute lung injury;Microbiological diag-nosis;Disseminated intra-vascular coagulation
ee front matter & 2007dip.2007.06.001
7188 2945; fax: +44 20 7ess: Sebastian.lucas@kc
Summary There is a clinico-pathological continuum of infection-driven sepsissyndromes, the most severe being septic shock with multi-organ failure. The organdysfunctions are due to inflammatory cytokines from remote sources (the site ofinfection) and constitute the systemic inflammatory response syndrome (SIRS). Thecommon causes are Gram-positive and Gram-negative infections; the commoninfection sites are (in descending frequency) lung, blood stream, intra-abdominaldisease, urological sepsis and surgical wounds; the commonest organ dysfunctionsare systemic shock, kidney, lung, and heart. The differential diagnosis of severesepsis includes disseminated malignancy, atherosclerosis, and haemophagocyticsyndrome. New treatments for severe sepsis are being trialled to raise the poorsurvival rates in intensive care. The role of the autopsy is to describe carefully theorgan lesions, provide microbiological evidence of infection, and to correlate thesewith the clinical features and therapeutic variables.& 2007 Elsevier Ltd. All rights reserved.
Introduction
Autopsy pathologists not infrequently use the term‘septicaemia’ (implying blood infection) as the finalprocess causing death, implying that there wasbacteraemia—hopefully proven but sometimesassumed—associated with one or more organfailures. This is an uneasy combination of clinical,laboratory and gross pathological features,because:
1.
There are no specific morbid anatomical fea-tures of ‘septicaemia’� the ‘diffluent’ or ‘septic’ spleen is a deba-table gross entity1;
Elsevier Ltd. All rights reserved.
401 3661.l.ac.uk
� ‘shock lung’ and ‘acute tubular necrosis’ aredifficult to diagnose on gross examinationalone.
2.
The interpretation of pre-mortem, let alonepost-mortem, blood cultures is not easy.23.
There are no standard histopathological featuresthat reliably point to ‘septicaemia’.4.
There is no agreed definition of ‘septicaemia’.It is more logical to consider ‘sepsis’: its localorigins, systemic consequences, and degrees ofseverity.
Within intensive care units (ICU), where mostpatients with severe sepsis are cared for,3 autopsyanalysis still reveals previously unknown diagnoses

ARTICLE IN PRESS
Table 1 Clinical definitions of sepsis.
Diagnosis Definition
Systemic inflammatory responsesyndrome (SIRS)
Temperature 438 or o36 1C
Heart rate 490/minRespiratory rate 420/min or PaCO2
o32mmHgBlood white cell count 412� 109/l or o4� 109/l, or 410% immature bandforms
Sepsis Systemic response to infection, as manifested by two or more of the above list(i.e. SIRS+infection)
Severe sepsis Sepsis with associated organ dysfunction, hypoperfusion, or hypotensionincluding lactic acidosis, oliguria, or acute alteration in mental state
Septic shock Sepsis-induced hypotension despite adequate fluid resuscitation, along withpresence of severe sepsis
Multiple organ dysfunctionsyndrome (MODS)
The presence of altered organ functions in an acutely ill patient such thathomoeostasis cannot be maintained without intervention
S. Lucas376
that could, if treated differently, have altered theoutcome; and this despite the panoply of investi-gative procedures now available to modern ICUmedicine. From the 21st century, a USA study4
found that 16% Goldman class 1 discrepancies (i.e.missed opportunity to change therapy and prolongsurvival5), and fungal infections were notablyunder-diagnosed pre-mortem. In a recent Frenchstudy6 32% of autopsies revealed Goldman classes 1or 2 discrepancies, particularly among the immuno-compromised patients. The diseases missed includedcancer, stroke, myocardial infarction, endocarditis,and pulmonary embolism. A British study7 noted thatonly 7.7% of ICU deaths were followed by an autopsy,and found similar discrepancy patterns to the Frenchstudy. Few studies address the precise contributionof sepsis and its management to death, althoughsevere sepsis is noted to be both under- and over-diagnosed pre-mortem.7,8
Epidemiology
The incidence of severe sepsis (as defined below) inindustrialised countries is 50–95 cases per 100,000population and is rising by up to 9% each year, forreasons still unexplained. It accounts for 2% ofhospital admissions in the USA, affecting about700,000 people per year, causing death in 210,000;and is the tenth leading cause of death.9–11
Clinical case definitions
As a result of consensus meetings in the early1990s—intended to improve not only patientmanagement but also the comparability of clinical
trials in ICU settings—there are agreed clinical casedefinitions of sepsis, including severity and organsyndromes (see Table 1).10,12 The recognition of thesystemic inflammatory response syndrome (SIRS) iscentral to the definitions.
The most common sites of infection associated withsepsis are pneumonia, blood stream infections (in-cluding infective endocarditis), intravascular cathe-ter-related sepsis, intra-abdominal infections,urological sepsis, and surgical wound infections.Florid septic shock syndromes also arises post-delivery, from necrotising fasciitis, and menstrualtoxic shock syndrome (see Table 2). Further consensusmeetings have arrived at agreed organ-specific casedefinitions, with emphasis on the stringency of theclinical characteristics and the microbiological inves-tigations.13 Table 3 indicates that for pneumonia.
The purpose of detailing these clinical case defini-tions is to contrast them with the morbid anatomicalfeatures of sepsis, which are less well depicted.Pathologists can assist clinical colleagues in evaluatingpatients dying of known or suspected sepsis, provingsepsis or identifying the differential diagnoses. Theycould thereby more usefully contribute to audit andthe evaluation of novel therapies in sepsis.
Infections causing septic shocksyndromes
The spectrum of infections has changed. In the1970–80s, Gram-negative bacteria predominated.The current in-hospital case pattern is9:
�
25–30% Gram-negative infections, � 30–50% Gram-positive infections,
ARTICLE IN PRESS
Table 2 The three most severe fulminant and toxic shock syndromes (TSS) and some of their character-istics.15,47,48
Syndrome Clinical features
Meningococcal (Neisseria meningitidis) bacteraemic shock � DIC prominent� Haemorrhagic rash� Mortality ¼ 10–20%
Staphylococcal (S. aureus) toxic shock syndrome � Menstrual (tampon-related)� Non-menstrual� Skin wounds, surgical wounds� Pneumonia� Catheter infections� Mortality ¼ 5%
Streptococcal (group A) toxic shock syndrome � Deep seated infections� Necrotising fasciitis� Surgical operation sites� Puerperal sepsis� Mortality ¼ 50%
The staphylococcal and streptococcal TSS have a rapid onset because the bacteria secrete superantigens which directly activateT-cells, with release of TNF-a, and a rapid cytokine storm.
Table 3 Pneumonia definitions.
Level of Certainty Definition
Microbiologically confirmed(i.e. definite)
� New or progressive radiological infiltrate� Clinical suspicion of pneumonia, or a Clinical Pulmonary Infection Score(CPIS)X6; this six-feature scale includes identification of bacteria onGram stain of lower respiratory tract samples� Identification of a pathogen—one or more of the following categories:
(a) Uncontaminated sample (blood, pleural fluid, transthoracic ortranstracheal aspirate)
(b) Respiratory secretions, not a pathogen that colonises the upperairways
(c) A likely pathogen using quantitative cultures of lower respiratorytract samples
(d) Positive infection serology
Probable Clinically as above, but the identification of a pathogen is:(a) Below the diagnostic threshold, or(b) Negative within 72 h of starting a new antibiotic regime
Possible Abnormal chest radiograph of uncertain cause in a patient with moderateor low suspicion of pneumonia, but with microbiological or serologicalevidence of definite or probable pneumonia (as defined above)
The autopsy pathology of sepsis-related death 377
�
25% polymicrobial infections, � 25% multi-drug resistant organisms (e.g., MRSAand fungi),
� 2–4% viral and parasitic infections (but probablyunderestimated):J e.g., HHV8/HIV co-infection,14
�
�30% negative cultures (community-acquiredsepsis treated with antibiotics before admission).Pathogenesis of the sepsis syndromes
SIRS is characterised as ‘an abnormal generalisedinflammatory reaction in organs remote from the ini-tial insult’.15 SIRS can result from non-infectivecauses, such as trauma, pancreatitis and cardiac-by-pass procedures, and the pathologist needs to considerthis when evaluating deaths presented as ‘sepsis’.

ARTICLE IN PRESS
S. Lucas378
Enormous research has gone into identifying thepathogenesis of the remote organ damage thatcharacterises severe sepsis; three recent re-views9,13,15 emphasise how much we do not under-stand.
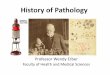
Infections trigger a cytokine cascade, with theexcess secretion of mediators including IL-1, TNFa,IL-6, nitric oxide (NO), and platelet-activatingfactor (PAF).16 Systemically, these affect organfunction via damage to epithelia and endothelialcells (with abnormal microcirculation), inflamma-tory cell infiltration, initiation of the coagulationsystem, endocrine stimulation, and activation ofthe autonomic nervous system. Microbial triggersinclude endotoxin (lipopolysaccharide) in Gram-negative bacilli and superantigens in Gram-positivecocci. Figure 1 indicates the conventional under-standing of the sequence of events that result inmulti-organ damage.
Two interesting underlying processes have beenhighlighted in severe sepsis:
1.
M& ac
EnAc
Loda
FigsepSAg
There is apoptosis of lymphocytes in the spleenand gut.17 It is hypothesised that this leads toimpairment of immune responses in sepsis.
2.
Organ failure is not always from observablenecrosis and/or fibrosis (i.e. structural) but isfunctional. Cellular mitochondrial activity isreduced, and this ‘hibernation’ may be aprotective response.18,19There are significant controversies, including:
1.
The significance of bacteraemia: Does thistrigger severe sepsis, or is it a transient leakagephenomenon, and contribute little, per se, tooutcome?INFECTION
Local site +/- bacteraemia
acrophageneutrophiltivation
dothelial celltivation
cal tissuemage
SecretionTNFα, IL-1IL-6, NO, etc
LPSSAgsetc
SEPSIS
Acute phasereactants
Fever
Leukocytosis
SEPTIC SHOCK
Cardiac hypo-function
Acute renal tubular injury
Diffuse alveolar damageDisseminated intra-vascular coagulation
Cholestasis
Ischaemic tissue damage
ure 1 Sequence of events from infection to sepsis andtic shock. LPS ¼ bacterial lipopolysaccharide;¼ bacterial superantigen.
2.
The continuum of the sepsis syndromes: Is this atrue final common path, independent of theactual initiating infection? Or do differentinfection–host interactions produce severe sep-sis and septic shock through different mechan-isms?153.
The concept that a major determining factorin patient outcome, for any given aetiology andset of co-morbidities, is not the particulartherapy in ICU but the individual’s genetic makeup9,20?4.
It is not always evident grossly and histologicallywhy patients with sepsis have died. A newparadigm is needed.17Autopsy protocols
In UK, 495% of adult autopsies are performedunder medico-legal conditions. Since the basicremit of the medico-legal autopsy is to excludeunnatural or violent death, and if possible, to avoidhaving an inquest,21 the level of detail of the exa-mination of cases that may have a sepsis syndromeis varied. Often the autopsy does not address thequestions raised by the clinical course of thepatient with sepsis. This review, does not attemptto address the requirements of what coroners mightwant from pathologists in ‘sepsis’ cases.
Microbiology sampling
One of the problems in the septic autopsy is thelack of agreed methods of sampling blood, tissuesand other fluids so that:
�
contamination from other organs is minimised; � the consequences of the post-mortem spread ofgut flora bacteria into the blood and tissues isminimised.2
There are no agreed strategies of what to samplefor each clinico-pathological-microbiological sce-nario. In all cases, sampling as soon after death aslogistically feasible reduces problems in the inter-pretation of bacterial culture results. See Table 4for interim recommended practice.
Interpretation of bacteriological cultures
The microbiology department must be advisedwhat range of organisms is being sought; cultureset-ups and molecular diagnostic techniquesvary accordingly. Interpretation of positive resultsis often difficult, and consultation with an

ARTICLE IN PRESS
Table 4 Sampling autopsy tissues for microbiological culture.
Tissue Sampling method
Cerebrospinalfluid
With syringe and needle through alcohol-cleaned skin, via:
� Cisternal puncture (posterior neck below the occipital protruberance; aim anteriorly forthe eyes); or� Lumbar puncture (between L4 and L5)
Urine Syringe and needle through cleaned suprapubic skinBlood Cardiac puncture blood, through the left 4th intercostal space, or peripheral venous blood:
� Subclavian vein (above clavicle), or� once the body is opened and before any organs opened or removed (particularly theintestines), tie off an iliac vein proximally, insert syringe needle pointing distally andwithdraw 10ml blood� Inoculate 5ml into each of aerobe and anaerobe blood culture bottles
Cardiacvegetations
Divide between a sterile bottle for culture and histopathology
Lung tissue Attempts to sterilise the outer surface are probably futile. A compromise is to cut the lungwith a clean organ-slicing blade on a clean surface and sample the relevant areas with asterile scalpel blade
The autopsy pathology of sepsis-related death 379
experienced microbiologist is critical. In cultures,great confidence that the identified organism issignificant is held if there is Mycobacteriumtuberculosis, Streptococcus group A (pyogenes),Streptococcus pneumoniae, or Neisseria meningiti-dis, since these are most unlikely to be presentincidentally or from contamination.
Figure 2 Lung. Endothelial cell activation indicated bystrong ICAM-1 expression. CD54 immunostain.
Non-microbiological means of identifyingsevere sepsis
In many autopsies, the need to confirm or excludesepsis happens without positive microbiology,either because all attempts (including pre-mortem)were negative (perhaps due to anti-microbialchemotherapy), or because samples were nottaken. Where histological evidence of pyogenicinfection with definite bacteria or fungi is present,this can indicate the organ-site of the sepsis.
If no infection is identified, immunocytochemicaltechniques may assist. In SIRS, endothelial cells areupregulated, and express cell adhesion moleculesintercellular adhesion molecule-1 (ICAM-1; CD54)and E-selectin (CD62E). It is possible to immunos-tain for these (Figure 2) and at least one authorholds that positive ICAM-1 staining of alveolarcapillary endothelial cells indicates septic shockwith high sensitivity and specificity.22
There are suggestive reports on the estimation ofpost-mortem serum endotoxin level as an indicatorof sepsis.23
Simulators of septic shock
Patients with clinical manifestations similar to thoseof septic shock come to ICU and die despite empiricaltherapy. The differential diagnosis includes:
�
disseminated cancer, including carcinoma andlymphoma. For example, pulmonary micro-em-boli from an occult carcinoma can obstructpulmonary arterioles and cause cardio-respira-tory failure24; � haemophagocytic syndrome; � thrombotic microangiopathy (TMA) syndromes;
ARTICLE IN PRESS
S. Lucas380
�
other conditions that mimic SIRS, but notconsidered in more detail15:J multi-organ atherosclerosis, NO expressionbeing a common factor;J burns;J adrenal insufficiency;J thyroid storm;J major trauma;J pancreatitis;J cardio-pulmonary bypass;J drug hypersensitivity reaction and acute
anaphylaxis;J malignant hyperthermia and heat stroke.
Tab
MyInfReinjInococSepInfendCares
Specific organs at autopsy
Heart
The syndrome of sepsis-related myocardial dys-function includes reduced left and right ejectionfractions and elevated heart rate (Table 5).15 Thereis evidence of apoptotic damage to cardiac myo-fibres in the rodent model of sepsis.25 In patientssurviving sepsis there is no evidence of persistentcardiac defects attributable to such a process.Presumably, the dysfunction is cytokine driven andreversible.19 The autopsied heart shows prominentinterstitial mononuclear cells—this is not myocar-ditis but mainly enlargement of capillary endothe-lial cells, as part of the generalised endothelial up-regulation phenomenon.
Given the generally old age of patients admittedto ICU with sepsis, many have coronary arterydisease, with or without previous myocardialinfarction, at autopsy. The extent to which thiscontributes (if at all) to death needs to be carefullyconsidered in the context of the whole case. TheDavies scale of certainty for ischaemic heart
le 5 Cardiac pathologies encountered in ICU patient
Ischaemic necrosis(atonic fibres)
Contraction band n(hyper-contracted
ocardialarction
+ �
-perfusionury
+ +
tropes &aine
+ +
sis 7 �
ectiveocarditis
7 �
rdio-pulmonaryuscitation
+ +
disease death (although designed for suddencardiac death in the community) is a bench-markfrom which to work.26 Nothing irritates ICUclinicians more than to be told that the cause ofdeath was ‘ischaemic heart disease’ in a complexcase of multi-organ failure and sepsis. If the patientwas part of a therapeutic protocol trial, it is evenmore unfortunate, as the aspects of apparenttherapy failure will be mis-apportioned.
Heart examination
Given the subtle nature of cardiac lesions in sepsisand its treatment, there is an argument for properhistopathological examination of a complete hor-izontal slice, with a minimum of five blocks taken:two from the right ventricle in one block, and onefull-thickness section from each left ventricularquadrant.26
Brain
At the gross and standard microscopic level, thebrain is not directly affected by sepsis and septicshock. This matches the lack of imaging-detecteddamage despite the common clinical cognitive andperformance deficiencies,15 and is presumably atransient cytokine-based phenomenon. Certaincerebral pathologies are associated with sepsissyndromes for more tangible reasons, including:
�
s a
ecfib
cerebral infarction from thrombo-embolisation;
� hypoxic-ischaemic encephalopathy (HIE) follow-ing temporary cessation of blood and/or oxygensupply during a crisis;
� metastatic cerebral abscess and/or meningitisfrom a remote focus of sepsis;
� microinfarction from TMA affecting all areas ofthe brain.
nd sepsis syndromes.49,50
rosisres)
Interstitialinflammation
Myocarditis Interstitialhaemorrhage
� � +
� � +
� � �
+ 7 ++ + �
� � +

ARTICLE IN PRESS
The autopsy pathology of sepsis-related death 381
In the case of HIE, post-mortem pathology doesnot form part of the case definition, which is solelyclinical, neurophysiological and radiological. Themost sensitive zones of the brain for such damageare the cerebellar nuclei and the hippocampus,followed by the cerebral cortex in the watershedareas at the junctions of the cerebral artery supplyzones. It is useful to sample these to confirm HIE,and to be aware of artifacts.27
Lung
Lung dysfunction at the commencement of severesepsis is present in about 20% of such patients.15
The clinical diagnosis of acute lung injury is madewhen there arterial hypoxaemia (PaO2
=FiO2o300)
and bilateral chest pulmonary infiltrates on chestX-ray, in the absence of pneumonia or heart failure.It becomes acute respiratory distress syndrome(ARDS) when hypoxaemia is more severe(PaO2=FiO2o200). Ventilation/perfusion mismatch(effectively right-to-left shunting) of blood flowoccurs, exacerbating the hypoxaemia.
Pathologically, the process is diffuse alveolardamage (DAD). This is not specific to sepsissyndromes as it also occurs in inhalational injury(smoke, toxic gases, oxygen in high concentration),aspiration of gastric contents, and X-irradiationdamage; these represent direct damage to the lungtissue. DAD also follows from remote injury as partof SIRS, the pathogenesis being mediators in theblood stream; the causes include cytotoxic drugtherapy, pancreatitis, cardio-pulmonary bypass,blood transfusion reaction, fat embolism, paraquatpoisoning, and systemic shock from any cause.28
The cycle of injury and damage is indicated inFigure 3. DAD goes through stages termed the
SEPSIS
Systemic cytokine release
Endothelial & epithelialcell damage
Collapse, oedema,haemorrhage
Surfactantdeficiency Shear forces
Figure 3 Sequence of events that lead to—and mayperpetuate—lung damage in sepsis syndromes (adaptedfrom Corrin and Nicholson28 with permission).
exudative, regenerative, and repair phases. Theexudative phase lasts up to a week, and grossly thelungs are dark red and heavy. The early stagehistologically comprises:
�
Fighycyt
alveolar wall congestion and expansion;
� variable neutrophils in the interstitium (usuallynot);
� oedema and red cells in the alveolae; � Type 1 epithelial cell and alveolar capillaryendothelial cell damage (difficult to identify onlight microscopy).
The later exudative phase is the classic and,histologically, readily identifiable stage oftentermed ‘shock lung’ (Figure 4):
�
alveolar collapse, haemorrhage and oedema; � hyaline membrane formation on the epithelialsurface of respiratory bronchioles and alveolarducts: this comprises fibrin and necrotic epithe-lial cells;
� variable neutrophil accumulation in alveolarcapillaries.
The regenerative phase permits healing andrecovery of the lung to normal structure orprogresses to fibrosis via the repair phase. Type 2epithelial cells proliferate to replace the denudedepithelium; they may be large and elongated,resembling macrophages in the airways. Theepithelium may regrow beneath the hyaline mem-brane, which is sloughed off; or over the mem-brane, in which case it becomes incorporated intothe alveolar wall and is a mechanism for interstitialfibrosis. In capillaries, the endothelial repair may
ure 4 Lung. Early diffuse alveolar damage withaline membranes and hypertrophied type 2 pneumo-es. H&E.

ARTICLE IN PRESS
Figure 5 Lung. Organising post-DAD, with thickenedalveolar walls and intra-alveolar fibrosis. H&E.
Figure 6 Lung. Neutropaenic sepsis. Clusters of Gram-positive cocci, fibrin, haemorrhage in alveoli; no poly-morphs. H&E.
S. Lucas382
be accompanied by local thrombosis, organisationand local vascular remodelling.
The repair phase occurs in those whose DAD hasnot resolved through regeneration. As well as theprogressive interstitial thickening from incorpora-tion of hyaline membranes and the ingress offibroblasts into this tissue, the alveolar exudatesorganise. There are granulation tissue buds in thealveoli, as seen in organising pneumonias. Thisfibrosis can happen within weeks.
In practice, if patients survive long periods in ICUwith episodes of severe sepsis and infectivepneumonia and have been mechanically ventilatedfor long periods, the resulting lung tissue at autopsycan show a varied pattern with areas of nearlynormal tissue, organising pneumonia and intersti-tial fibrosis separately and combined: it can bedifficult if not impossible to ascribe specificaetio-pathogeneses to this end-stage lung fibrosis(Figure 5).
Why some patients with DAD in whom theinfecting agent is identified and treated promptlystill go on to the repair phase and die of pulmonaryfibrosis is unresolved. Patients presenting as ad-vanced HIV disease with Pneumocystis infection,and despite co-trimoxazole plus steroid cover,become progressively hypoxic; at autopsy the lungsshow combined intra-alveolar and interstitialfibrosis.
Ventilator-associated pneumonia (VAP)
VAP is an important entity in ICU, as the develop-ment of lung infection during respiratory supportdemands a change in therapy. Studies of thediagnostic criteria for VAP in vivo (microbiology
and cytopathology) and at autopsy (histopathol-ogy), have yielded unsettling results29:
�
There are no agreed criteria for diagnosingpneumonia in man by histology. � Pathologists do not agree amongst themselveswhether there is pneumonia or not.
� Quantitative pre-mortem bacteriology does notcorrelate with clinical symptoms or autopsyhistopathology.
� Bronchiolar lavage fluid with few neutrophilscorrelates with absence of histological pneumo-nia.
Evidently pathology is not yet serving clinicalscience optimally in this area.
Neutropaenic sepsis
This is a common terminal condition in patientswith treated cancer. Bacteria proliferate in manyorgans and blood vessels, and in the lung are visiblein the alveoli with fibrin and mononuclear cells(Figure 6).
Liver
The liver in septic shock has no specific features(Table 6). Clinically, there is cholestatic jaundice. Ifthe source of the sepsis is the biliary tract(cholangitis) there may be abscesses centred onportal tracts. Otherwise, the liver is usually heavierthan normal, bile stained, and soft. Histologically,autolysis with cell plate separation is often moreadvanced than expected from the time since death(perhaps due to high levels of TNFa). There is often

ARTICLE IN PRESS
Table 6 Liver histopathology in sepsis.
Liverabscess
Bacterialcholangitis
Bile ductobstruction
Severe sepsis patterns
Canalicularcholestasis
Ductular cholestasis &inflammation
Non-bacterialcholestasis
Perivenular cholestasis 7 � + + + �
Canal of hering &ductular cholestasis
� � � � + �
Ductular proliferation � + + � + +Ductular acuteinflammation
7 + 7 � + +
Parenchymal necrosis + + 7 � � �
Figure 7 Liver. E. coli sepsis: severe centriacinarnecrosis; canalicular cholestasis. H&E.
The autopsy pathology of sepsis-related death 383
fatty change, but usually little parenchymal in-flammation, although the sinusoid Kupffer cells andendothelial cells are prominent, and there may behaemophagocytosis. Centriacinar necrosis is oftenprominent (Figure 7).
Several patterns of bile duct histopathology aredescribed, although none are specific to sepsis30:
�
intracanalicular cholestasis in the perivenularareas; � ductular cholestasis, proliferating ductules, andsurrounding portal neutrophilic inflammation, inaddition to canalicular cholestasis;
� non-bacterial cholangitis, with proliferating bileductules; this is seen in the toxic shock syn-drome.
Kidney
Acute renal failure occurs in 20% of patientsbecoming septic, rising to 50% in septic shock.15,31
It is the commonest organ dysfunction, manifestingas oliguria and azotaemia. The pathogenesis of thedamage in sepsis includes systemic hypotension,renal vasoconstriction, toxic drugs (e.g. antibioticaminoglycosides), and inflammatory cytokines.
The pathological lesion is acute tubular injury(ATI) (formerly ‘acute tubular necrosis’).31 Grosslythe kidneys are enlarged (oedematous cortex) andtypically pale, with blurred cortico-medullaryjunctions. Focal pyaemic lesions, ascending acutepyelonephritis lines, and (where arterial thrombiare formed) regional cortical infarctive necrosismay also be seen.
ATI can only be reliably evaluated microscopi-cally. The glomeruli may be collapsed but other-wise show no damage. Tubular damage is concep-tually divided into ‘ischaemic’ and ‘toxic’,31 withmore extensive proximal tubule lesions, and moreevident cell death, in the latter. In septic shock,with the aetio-pathogenesis often multi-factorial,the distinction becomes blurred. Autopsy kidneysare notoriously autolysed unless analysedrapidly after death. The main features of ATI(Figure 8) are:
�
interstitial oedema with separation of tubules; � tubular cell swelling; � loss of nuclei of tubular cells or apoptosis; � shedding of tubule cells into the lumen; � attenuation of the tubular epithelium thickness; � regeneration of tubular cells: hyperchromaticenlarged nuclei, often adjacent; mitoses;
� insignificant interstitial inflammation; � accumulation of nucleated cells in the vasa rectain the outer medulla–lymphocytes, myeloidprecursors, and nucleated red cell precursors.
The time delay to autopsy often precludesconfirmation of these features. Microvesicularvacuolation of proximal tubules is not ATI, but the

ARTICLE IN PRESS
Figure 8 Kidney. Acute tubular injury: apoptotic tubularcells sloughed into the lumen; regenerating cells withhypertrophied nuclei; interstitial oedema. H&E.
Figure 9 Bone marrow haemophagocytosis. Numerousmacrophages engulfing red cells. H&E.
S. Lucas384
result of drugs and dextrose-containing plasmaexpanders.
Adrenal glands
The adrenals may show the following features:
�
lipid depletion and hyperplasia; � atrophy (due to prolonged steroid therapy); � parenchymal haemorrhages, small or large; � thromboses in small arterioles.Haemophagocytic syndromes (HPS)
There is a group of conditions termed HPS wherethe driving process is excessive phagocytosis offormed blood cells by macrophages in the marrow,spleen and lymph nodes (Figure 9). The clinicaloutcomes include:
�
high fever; � pancytopaenia; � liver dysfunction; � clotting abnormalities including raised fibrindegradation products and hypofibrinogenaemia;
� hepatosplenomegaly; � hyperferritinaemia.HPS overlaps clinically with septic shock by casedefinition.32 The mortality is high, up to 70%.33,34
Many patients that prove to have HPS presentacutely with SIRS, infection screens are negative,and the death occurs within a week, of multi-organfailure, despite intensive therapy.
The pathogenesis of HPS is considered to be anaberrant immunological over-reaction, the hyper-
stimulation of macrophages by cytokines (particu-larly TNFa, IL-6, IL-1 and IFNg) as result of T-cellactivation. In addition to a rare familial HPS, theaetiologies include infections, autoimmune disease(particularly SLE) and lymphoma (particularly T-celllymphoma, but also B-cell). The potential causativeinfections are legion32–34:
�
viral, e.g. EBV, HHV8, HIV, CMV, B19, rubella,viral hepatitis; � bacteria, e.g. pneumococcal, typhoid; � mycobacteria, e.g. tuberculosis; � fungi, e.g. histoplasmosis; � protozoa, e.g. leishmaniasis.Bone marrow haemophagocytosis is found in onethird of ICU non-survivors, associated positivelywith sepsis and blood transfusion, and negativelywith cardiovascular disease.35 The distinction be-tween a non-specific reactive process and asyndrome is currently blurred.
Thrombotic microangiopathy syndromes
Thombi, composed of fibrin and platelets in varyingproportions, are frequently encountered in smallvessels in sepsis and other conditions. There aretwo groups of conditions to consider: disseminatedintravascular coagulation (DIC) and TMA.
Disseminated intravascular coagulation36
The thrombi are predominantly composed of fibrinand it is accompanied by coagulopathy withdepletion of coagulation factors in the blood. DIC(as defined by laboratory criteria) occurs in up to

ARTICLE IN PRESS
Figure 10 Kidney. Fibrin thrombi in glomerular capil-laries (meningococcal sepsis). H&E.
The autopsy pathology of sepsis-related death 385
half of patients with severe sepsis. The pathogen-esis is not well understood but may be endothelialinjury, the expression of tissue factor on infectedmonocytes, and initiation of the clotting cascade.15
With the exception of meningococcal septicaemia,autopsy studies do not show a correlation of organdysfunction and deposition of microthrombi in DIC.When thrombi are seen, the renal glomeruli andlung alveolar capillaries are the commonest loca-tions (Figure 10).
N. meningitides infection causes a fulminantmeningococcaemia (often without meningitis).Here DIC is the norm, and bacteria may be foundwithin dermal vessels. Meningococci differ fromother Gram-negative bacilli as they shed membraneblebs that active complement and coagulationdirectly. Widespread skin and internal organ hae-morrhages are seen, associated with small vesselDIC, and the adrenal shows haemorrhages (thoughrarely a massive destructive haematoma).
The prototype TMA is thrombotic thrombocyto-paenic purpura (TTP) and the related haemolyticuraemic syndrome.37 Unlike DIC, the clottingfactors are not affected, and the thrombi arepredominantly platelets. Clinically TMA may simu-late septic shock. Immunocytochemistry to quanti-fy fibrin versus platelets (anti-fibrin and anti-CD61antibodies, respectively) and thus distinguish TMAfrom DIC is not always helpful: the stainingintensities may be similar in both conditions.
End-stage liver disease
The adverse impact of cirrhosis is well-attested inmany medical and surgical conditions. The Child–
Pugh liver score (a measure of hepatic and extra-
hepatic dysfunction based on combined biochem-ical markers and clinical signs) predicts non-survival in cirrhotic patients admitted to ICU.Overall, the 1-year mortality of such patients is69–74%, with median survival of 1 month.38,39
Cardiac operations are hazardous in cirrhoticpatients, with those on cardio-pulmonary bypassparticularly liable to die40 and—if they are Child–Pughclass C—approach a 100% mortality. Abdominaltrauma patients have ICU post-operative mortalityrates increasing from 15% to 63% as the severity liverfailure increases.41 In these patients a major causeof death is sepsis and septic shock. The abnormalblood circulation to cirrhotic liver tissue renders theKupffer cell macrophages less able to clear bacteriafrom the blood.
Cirrhosis is significantly under-diagnosed pre-mortem, and clinicians would like better methodsof identifying the patients who have cirrhosis.There are several implications. First, consider liverdisease carefully in ICU and sepsis deaths. Theeyeball—confident diagnosis of cirrhosis—or not—is not always possible. Secondly, in the formulationof cause of death in these cases, ‘cirrhosis’ shouldbe included as a contributor to mortality in thedeath certificate.
Liver biopsy is the only pre-autopsy definitivemarker of liver fibrosis and cirrhosis; but is invasiveand has a mortality rate. Imaging, standardbiochemical tests, serum markers of fibrosis, andmore specialised tests of liver function only identifya proportion of cirrhotic patients,42 and these non-invasive tests have not been validated for ‘normal’patients about to undergo cardiac surgery or thosealready in ICU for other reasons. Further researchinto better indicators of cirrhosis is urgentlyneeded.
Outcomes and co-morbidities
Mortality in patients with septic shock is highlyvariable, from 35% to 70% depending on manyvariables that include9:
�
age and sex; � co-morbidities-immunosuppression,6,43 chronicobstructive pulmonary disease, ischaemic heartdisease, end-stage liver disease;
� the combined total of failing organs, particularlylung and kidney;
� whether the infection is nosocomial or polymi-crobial;
� whether the infection is a fungus; � ethnicity and inherited variables.20
ARTICLE IN PRESS
S. Lucas386
The treatment of sepsis
3ICU treatment of patients in sepsis and shock hasfour main approaches:
�
Anti-microbial therapy of known or suspectedinfective agents. � Failing organ support, e.g. pulmonary, renal,hepatic, cardiac.
� Indirect immunomodulatory/anti-inflammatorytherapies aimed at the systemic inflammatoryresponse and its consequences.
� Surgical treatment—excision of septic foci andremoval of necrotic tissue (e.g. infarcted bowel,necrotising fasciitis).
Many trials of anti-inflammatory chemotherapyhave been held in septic shock, including against10:immune regulation, endotoxin, TNFa, NO, IL-1,oxidants, neutrophil activity, complement, andcoagulation. Only steroid therapy and activatedprotein C (APC) improve survival. Other therapeu-tic avenues have not proven successful because of:(a) non-homogeneity of the study populations, and(b) the ill-understood multifactorial complexity ofthe sepsis syndromes.
Steroid therapy has its known complications. APCacts as an anti-coagulant (important in DIC) andinhibits production of IL-1, IL-6 and TNFa. The sideeffects are intracerebral44 and pulmonary haemor-rhage (personal observations).
As well as inotropic and renal support, a majorfunction of ICU is ventilatory support. In DAD, thealveoli shut down on expiration and require ahigher pressure to re-open. Mechanical ventilationexerts stresses on the delicate lung tissue. Inconjunction with the high oxygen concentrationrequired to keep a reasonable blood PO2, this canfurther damage the lung (Figure 3).
The known increase in apoptosis in the lymphoidpopulation17 has prompted consideration of anti-apoptotic chemotherapy. However, the potential ofuncontrolled cell growth has to be evaluated first.
Statin therapy is associated with reduced rates ofsepsis and fatality from sepsis.45 Statins have manyother effects: anti-inflammatory, modulation ofcellular immunity, improvement of endothelial cellfunction, and increasing the bio-availability of NO.Apart from suggesting further strategies in sepsistherapy, this observation reminds pathologists tolook at the patient’s treatment history.
Conclusion
This review of septic shock autopsy pathology andits differential diagnosis has focussed on the major
conditions. There are less obvious pathologieswhose contribution to the disease and outcomeare uncertain, e.g. apoptosis of neurones and glialcells in the cardiovascular centres of the brain.Patients who died of septic shock showed more suchapoptosis in the amygdala and medullary auto-nomic nuclei than those dying of non-septic shockand sudden extra-cranial trauma. This was stronglyassociated with endothelial iNOS expression.46 Doesthis significantly contribute to outcome over andabove direct organ damage?
There is much still to be studied in the morbidanatomy of sepsis syndromes. If pathologists are tobe useful in sepsis research, careful documentationof autopsy organ pathology and microbiology, andthe correlation of outcome with clinical featuresand the various therapeutic modalities, is essential.
Practice points
A. The approach to the severe sepsisautopsy
� Read the medical records� Consult with the clinicians who know about
the case� Perform a complete autopsy� Accept that gross findings may be non-
specific� Obtain histopathology samples on all the
relevant organs, in particular:J HeartJ LungsJ LiverJ KidneyJ Bone marrow� Obtain appropriate samples for microbiolo-
gical evaluation� Liaise with microbiologists in the interpre-
tation of results� Think carefully when formulating the cause
of death in these complex cases:J Does the pathological evidence fulfil the
clinical case definition of a sepsis syn-drome?
J Use the term ‘bacteraemia’, not ‘septi-caemia’
� Encourage intensive care mortality meet-ings to discuss the results: both cliniciansand pathologists have much to learn
B. Differential diagnosis of septic shock
� Atherosclerosis� Haemophagocytic syndrome

ARTICLE IN PRESS
The autopsy pathology of sepsis-related death 387
� Thrombotic microangiopathy� Disseminated cancer—carcinoma and lym-
phoma� Adrenal and thyroid disease� Drug reactions (acute anaphylaxis)� Pancreatitis
References
1. Arismendi-Morrillo GJ, Briceno-Garcia AE, Romero-AmaroZR, et al. Acute non-specific splenitis as indicator ofsystemic infection. Assessment of 71 autopsy cases. InvestClin 2004;45:131–5.
2. Morris JA, Harrison LM, Partridge SM. Postmortem bacter-iology: a re-evaluation. J Clin Pathol 2006;59:9.
3. Dellinger P, Carlet JM, Masur H, et al. Surviving sepsiscampaign guidelines for management of severe sepsis andseptic shock. Crit Care Med 2004;32:858–78.
4. Roosen J, Frans E, Wilmer A, Knockaert DC, Bobbaers H.Comparison of premortem clinical diagnoses in critically illpatients and subsequent autopsy findings. Mayo Clin Proc2000;75:562–7.
5. Goldman L, Sayson R, Robbins S, Cohn LH, Bettman M,Weisberg M. The value of the autopsy in three medical eras.N Engl J Med 1983;308:1000–5.
6. Combes A, Mokhtari M, Couvelard A, et al. Clinical andautopsy diagnoses in the intensive care unit: a prospectivestudy. Arch Intern Med 2004;164:389–92.
7. Perkins GD, McAuley DF, Davies S, Gao F. Discrepanciesbetween clinical and postmortem diagnoses in critically illpatients: an observationsl study. Crit Care 2003;7:R129–32.
8. Blosser SA, Zimmerman HE, Stauffer JL. Do autopsies ofcritically ill patients reveal important findings that wereclinical undetected? Crit Care Med 1998;26:1332–6.
9. Annane D, Bellisant E, Cavaillon J-M. Septic shock. Lancet2005;365:63–78.
10. Riederman NC, Guo R-F, Ward PA. The enigma of sepsis.J Clin Invest 2003;112:460–7.
11. Danai P, Martin GS. Epidemiology of sepsis: recent advances.Curr Infect Dis Rep 2005;7:329–34.
12. Levy MM, et al. SCCM/ESICM/ACCP/ATS/SIS InternationalSepsis Definitions Conference. Crit Care Med 1992;31:1250–6.
13. Calandra T, Cohen J, et al. The International Sepsis ForumConsensus Conference on Definitions of Infection in theIntensive Care Unit. Crit Care Med 2005;33:1538–48.
14. Fowler A, Collins L, de Ruiter A, et al. MulticentricCastleman’s disease in a patient with HIV. Int J STD AIDS2006;17:63–4.
15. Munford RS. Sepsis, severe sepsis, and septic shock. In:Mandell GL, Bennet JE, Dolin R, editors. Mandell,Douglas and Bennett’s principles and practice of infectiousdiseases. Pennsylvania: Elsevier Churchill Livingstone; 2005.p. 906–25.
16. Mitchell RN. Hemodynamic disorders, thromboembolic dis-ease, and shock. In: Kumar V, Abbas AK, Fausto N, editors.Robbins and Contran pathologic basis of disease. Philadel-phia: Elsevier Saunders; 2005. p. 119–44.
17. Hotchkiss RS, Swanson PE, Freeman B, et al. Apoptotic celldeath in patients with sepsis, shock, and multiple organdysfunction. Crit Care Med 1999;27:1230–51.
18. Singer M, De Santis V, Vitale D, Jeffcoate W. Multiorganfailure is an adaptive, endocrine-mediated, metabolic
response to overwhelming systemic inflammation. Lancet2004;364:545–8.
19. Levy RJ, Piel DA, ACton PD, et al. Evidence of myocardialhibernation in the septis subject. Crit Care Med2005;33:2752–6.
20. Villar J, Maca-Meyer N, Perez-Mendez L, Flores C. Bench-to-bedside review: understanding genetic predisposition tosepsis. Crit Care 2004;8:180–9.
21. National Confidential Enquiry into Patient Outcome andDeath. The Coroner’s autopsy: do we deserve better? 2006/www.ncepod.org.ukS.
22. Tsokos M. Immunohistochemical detection of sepsis-inducedlung injury in human autopsy material. Legal Med 2003;5:73–86.
23. Zhu BL, Ishikawa T, Michiue T, Quan L, Maeda H. Postmortemserum endotoxin level in relation to the causes of death.Legal Med 2005;7:103–9.
24. Hirata K, Miyagi S, Tome M, et al. Cor pulmonale due totumour cell microemboli. Arch Intern Med 1988;148:2287–9.
25. Ha T, Grant D, Xia Y, et al. Glucan phosphate attenuatescardiac dysfunction and inhibits cardiac MIF expression andapoptosis in septic mice. Am J Physiol Heart Circ Physiol2006;291:H1910–8.
26. Royal College of Pathologists. Sudden death with likelycardiac pathology. /www.rcpath.orgS. Guidelines for Au-topsy Practice-best practice scenarios. 2005.
27. Whitwell H. Techniques. In: Whitwell H, editor. Forensicneuropathology. London: Hodder Arnold; 2005. p. 20–35.
28. Corrin B, Nicholson A. Diffuse alveolar damage. In:Pathology of the Lung, 2006. p. 131–49.
29. Corley DE, Kirtland SH, Winterbauer RH, et al. Reproduci-bility of the histologic diagnosis of pneumonia among a panelof four pathologists. Chest 1997;112:458–65.
30. Scheuer P, Lefkowitch JH. The liver in systemic disease andpregnancy. In: Liver biopsy interpretation. Elsevier Saun-ders; 1980. p. 331–2.
31. Racusen L, Kashgarian M. Ischemic and toxic acute tubulardamage and other ischemic renal injury. In: Jennette JC,Olson JL, Schwartz MM, Silva FG, editors. Heptinstall’spathology of the kidney. Philadelphia: Lippincott, Williams& Wilkins; 2007. p. 1139–86.
32. Fisman DN. Hemophagocytic syndromes and infection.Emerg Infect Dis 2000;6:601–8.
33. Takahashi N, Chubachi A, Kume M, et al. A clinical analysis of52 adult patients with hemophagocytic syndrome: theprognostic significance of the underlying diseases. Int JHaematol 2001;74:209–13.
34. Ningsanond V. Infection associated hemophagocytic syn-drome: a report of 50 children. J Med Assoc Thai 2000;83:1141–9.
35. Stauss R, Neureiter D, Westenburger B, et al. Multifactorialrisk analysis of bone marrow histiocytic hyperplasia withhemophagocytosis in critically ill medical patients—a post-mortem clinicopathologic analysis. Crit Care Med 2004;32:1316–21.
36. Toh CH, Dennis M. Disseminated intravascular coagulation:old disease, new hope. Br Med J 2003;327:974–7.
37. Hosler GA, Cusumano AM, Hutchins GM. Thrombotic throm-bocytopenia purpura and hemolytic uremic syndrome aredistinct pathologic entities. A review of 56 autopsy cases.Arch Pathol Lab Med 2003;127:834–9.
38. Gildea TR, Cook WC, Nelson DR, et al. Predictors of long-term mortality in patients with cirrhosis of the liveradmitted to a medical ICU. Chest 2004;126:1598–603.
39. Arabi Y, Ahmed QA, Haddad S, Aljumah A, Al-Shimemeri A.Outcome predictors of cirrhosis patients admitted to the

ARTICLE IN PRESS
S. Lucas388
intensive care unit. Eur J Gastroenterol Hepatol 2004;16:333–9.
40. Hayashida M, Shoujima T, Teshima H, et al. Clinical outcomeafter cardiac operations in patients with cirrhosis. AnnThorac Surg 2004;77:500–5.
41. Christmas AB, Wilson AK, Franklin GA, et al. Cirrhosis andtrauma: a deadly duo. Am Surg 2005;71:996–1000.
42. Rockey DC, Bissell M. Non-invasive measures of liver fibrosis.Hepatol 2006;43:S113–20.
43. Morris A, Masur H, Huang L. Current issues in criticalcare of the HIV-infected patient. Crit Care Med 2006;34:42–9.
44. Recombinant human Protein C Worldwide Evaluation inSevere Sepsis (PROWESS) study group. Efficacy and safetyof recombinant human activated protein C for severe sepsis.N Engl J Med 2001;344:699–709.
45. Hackam DG, Mamdani M, Li P, Redelmeier DA. Statins inpatients with cardiovascular disease: a population-basedcohort analysis. Lancet 2006;367:413–8.
46. Sharshar T, Gray F, de la Grandmaison GL, et al. Apoptosis ofneurons in cardiovascular autonomic centres triggered by
inducible nitric oxide after death from septic shock. Lancet2003;362:1799–805.
47. Moreillon P, Que Y-A, Glauser MP. Staphylococcus aureus(including staphylococcal toxic shock). In: Mandell GL,Bennet JE, Dolin R, editors. Mandell, Douglas, and Bennett’sprinciples and practice of infectious diseases. Philadelphia:Elsevier Churchill Livingstone; 2005. p. 2321–51.
48. Bisno AK, Stevens DL. Streptococcus pyogenes. In: MandellGL, Bennet JE, Dolin R, editors. Mandell, Douglas, andBennett’s principles and practice of infectious diseases.Philadelphia: Elsevier Churchill Livingstone; 2005.p. 2362–79.
49. Baroldi G. Basic pathophysiologic changes. In: Fineschi V,Baroldi G, Silver MD, editors. Pathology of the heart andsudden death in forensic medicine. Boca Raton, FL: CRCPress, Taylor & Francis Group; 2006. p. 31–76.
50. Nishida N, Chiba T, Ohtani K, Ikeda N, Katayama Y, YoshiokaN. Relationship between cardiopulmonary resuscitation andinjuries of the cardiac conduction system: pathologicalfeatures and pathogenesis of such injuries. Crit Care Med2006;34:363–7.