Embed Size (px)
Citation preview

The Atrioventricular Block in pediatric cardiology
Coordinator:
Dr. GOZAR LILIANA
Author:
BENTZ OANA

AVB = atrioventricular blockAVB = atrioventricular block ECG = electrocardiogramECG = electrocardiogram ASD = arterial septal defectASD = arterial septal defect TGA = transposition of the great arteriasTGA = transposition of the great arterias VSD = ventricular septal defect VSD = ventricular septal defect CHD = congenital heart defectCHD = congenital heart defect
LegendLegend

ObjectivesObjectives
I. IntroductionI. Introduction
II. Material and methodsII. Material and methods
III. ResultsIII. Results
IV. DiscussionsIV. Discussions
V. ConclusionsV. Conclusions

AV block refers to a conduction delay or AV block refers to a conduction delay or interruption of the impulses generated in the interruption of the impulses generated in the atrium before they reach the ventricles. AV atrium before they reach the ventricles. AV block may be transient or permanent.block may be transient or permanent.
I. IntroductionI. Introduction


Classification of AVBClassification of AVB
congenital AVBcongenital AVB
post-surgery AVBpost-surgery AVB

Patients in the study have Patients in the study have received:received:
Clinical examination
Laboratory investigations:
History
ECG Fetal echocardiographyHolter

Laboratory investigations:
Echocardiography Exercise tolerance test

Treatment for AVB II and III degreeTreatment for AVB II and III degree temporary (pacing)temporary (pacing) permanent (permanent pacemaker).permanent (permanent pacemaker).

Permanent Permanent pacing is pacing is
definitely useful definitely useful and necessaryand necessary
Permanent pacing may be Permanent pacing may be indicated indicated
Class II A option is in favor Class II A option is in favor of efficacy of efficacy
Class II B in which efficacy Class II B in which efficacy is less well establishedis less well established
Permanent Permanent pacing is not pacing is not useful it can useful it can be harm full be harm full
Classes of pacemaker
I II III

at infants and children: pacemaker with epicardial electrodes

Aim of the workAim of the work
The goal is to analyze retrospective and The goal is to analyze retrospective and prospective major disorders of driving from prospective major disorders of driving from etiological point of view, therapeutic, evolutionarily.etiological point of view, therapeutic, evolutionarily.

II. Material and methodsII. Material and methods
The study group: 91 children The study group: 91 children average: age of 5 years and 5 months (between 2 average: age of 5 years and 5 months (between 2
days and 18 years) days and 18 years) period: 2008-2013 period: 2008-2013 The II Cardiology Clinic of children in Tg. MuresThe II Cardiology Clinic of children in Tg. Mures
Type of study: Type of study:
prospectiveprospectiveretrospectiveretrospective
2008 - 20122008 - 2012
andand
20132013

We had 17 cases (18.68%) of congenital AVB II We had 17 cases (18.68%) of congenital AVB II and III degree; 74 cases (81.32%) of post-surgery and III degree; 74 cases (81.32%) of post-surgery AVB II and III degree.AVB II and III degree.
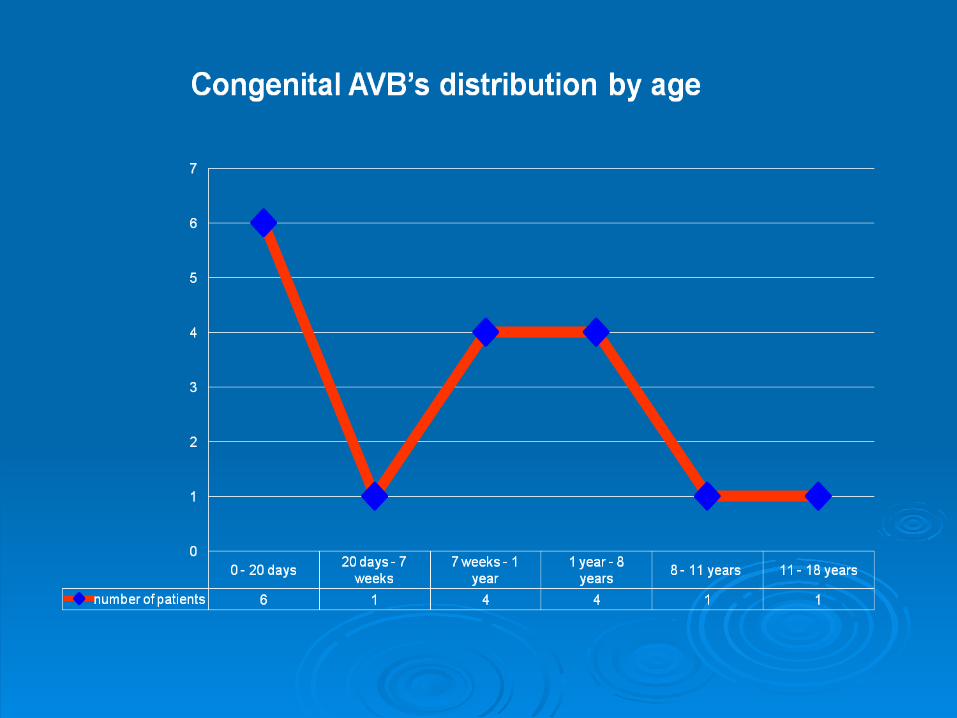
Congenital AVB may become manifest in: Congenital AVB may become manifest in:
The clinical suggestive element is reduced heart The clinical suggestive element is reduced heart rate.rate.
intrauterine (2 cases) newborn period (9 cases) early childhood (2 cases)
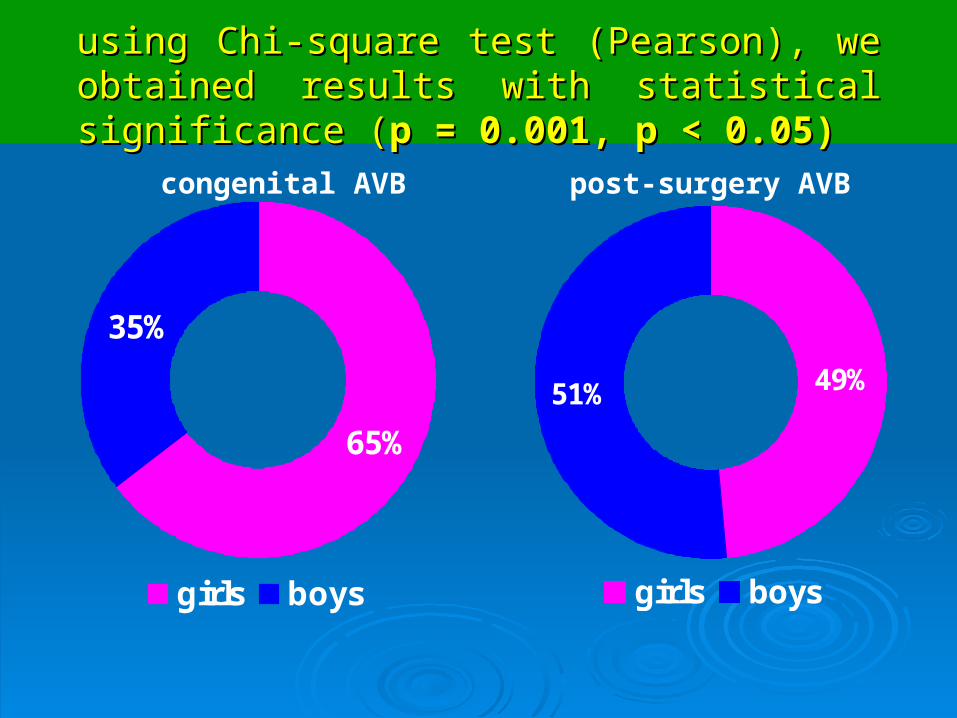
using Chi-square test (Pearson), we obtained results using Chi-square test (Pearson), we obtained results with statistical significance with statistical significance ((p = 0.001, p < 0.05)p = 0.001, p < 0.05)
65%
35%
girls boys
49%51%
girls boys
congenital AVB post-surgery AVB

analyzing environmental proportions of originanalyzing environmental proportions of origin
((p=0.001, p < 0.05p=0.001, p < 0.05))
53%47%
urban rural
34%
66%
urban rural
congenital AVB post-surgery AVB

0
5
10
15
20
25
30
35
40
1
4
34 post-surgery AVB > 7 days
post-surgery AVB < 7 days

0 2 4 6 8
6-18 years
1-5 years
0-1 year
ag
enumber of patients
0 10 20 30
6-18 years
1-5 years
0-1 year
ag
e
number of patients
post-surgery II AVB
post-surgery III AVB

III. ResultsIII. Results
Analyzing associated pathology in children, we have Analyzing associated pathology in children, we have found that the delay of the atrioventricular and found that the delay of the atrioventricular and intraventricular conduction is frequently observed intraventricular conduction is frequently observed after complex surgeries for congenital heart defects after complex surgeries for congenital heart defects and some of them presenting also heart failure.and some of them presenting also heart failure.

ASSOCIATED PATHOLOGIESASSOCIATED PATHOLOGIES
post-surgery II AVBpost-surgery II AVB
Cardiac Cases Percentages Extra-cardiac Cases Percentages
ASD 4 28.58%Gallbladder
malformation2 100%
TGA 4 28.58%
VSD 2 14.28%
Mitral insuf.
2 14.28%
Aortic insuf.
2 14.28%


ASSOCIATED PATHOLOGIESASSOCIATED PATHOLOGIESpost-surgery III AVBpost-surgery III AVB
Cardiac Cases Percentages Extra-cardiac Cases Percentages
VSD 24 45.28%Down
Syndrome1 25%
TGA 14 26.42%Gallbladder
malformation3 75%
ASD 10 18.87%
Mitral insuf. 3 5.66%
Aortic insuf. 2 3.77%



Exercise tolerance testExercise tolerance test
5 exercise tolerance test cases (29 %)5 exercise tolerance test cases (29 %) 12 cases without exercise tolerance test (71 %)12 cases without exercise tolerance test (71 %)

pacemaker 11 cases;
pacemaker 6 cases
pacemaker 43 cases;
pacemaker 31 cases.

IV. DiscussionsIV. Discussions
Most cases of:Most cases of:
AVB II degree high type has a risk to progress to a complete block.

In postoperative pathology predominates AVB III degree compared to AVB II degree, p = 0.03,
p < 0.05.

V. ConclusionsV. Conclusions
1
2
3
4
Congenital AVB is a major rhythm disorder Congenital AVB is a major rhythm disorder that requires cardiology dispensary.that requires cardiology dispensary.
Over 50% of patients require pacemaker Over 50% of patients require pacemaker implantation. implantation.
AVB is one of the complications of AVB is one of the complications of
surgical treatment of CHD.surgical treatment of CHD.
Some of these patients have evolved with Some of these patients have evolved with the recovery of atrioventricular the recovery of atrioventricular
conduction.conduction.

BibliographyBibliography
1. Kastor: Arrhythmias, Second Edition.1. Kastor: Arrhythmias, Second Edition.
2. Edward P. Walsh, J. Philip Saul, John K. 2. Edward P. Walsh, J. Philip Saul, John K. Triedman: Cardiac arrhythmias in children and Triedman: Cardiac arrhythmias in children and young adults with congenital heart disease.young adults with congenital heart disease.
3. John R. Hampton: The ECG made easy, 3. John R. Hampton: The ECG made easy, Seventh Edition. Seventh Edition.






























