Embed Size (px)
Citation preview

Deborah L O’Connor PhD
The Art and Science of Keeping
Infants With Cancer Well-Nourished

Disclosures
I serve as Co-Chair on the Advisory Board of the
Rogers Hixon Ontario Human Donor Milk Bank
Lead a Canadian Institutes of Health Research
program with the aim to optimize use of human
milk for preterm infants

Objectives
Participants will be:
1. Able to describe current recommendations for
feeding healthy infants during the first year of
life including the introduction of solids and the
need for vitamin and mineral drops
2. Knowledgeable about reliable resources to
support families in adhering to feeding
guidelines

Important Definition for this
Presentation
While benefits of feeding at the breast are
acknowledged:
Breastfeeding = feeding human milk (fresh or
frozen) at the breast, by bottle, feeding tube
or supplemental nursing system
***Promote skin-to-skin contact for infants not fed at
the breast

Exclusive Breastfeeding to 6
Months
“….exclusive breastfeeding
for 6 months is the optimal
way of feeding infants.
Thereafter infants should
receive complementary foods
with continued breastfeeding up
to 2 years of age or beyond.”
World Health Organization. 2001. Global Strategies for Infant and Young Child Feeding. Resolution
Passed at: Fifty-fourth World Health Assembly; May 9, 2001
https://www.canada.ca/en/health-canada/services/food-nutrition/healthy-eating/infant-feeding.html

Benefits of Breast Milk: Short
Term Outcomes
• Uniquely meets the Nutritional Requirement
of Infants
• Is Well Tolerated

• Association between breastfeeding and
outcomes assessed from 28 systematic
reviews and meta-analyses, of which 22 were
commissioned for this paper

Benefits of Breast Milk: Short
Term Outcomes
• Uniquely meets the nutritional requirement of
infants
• Is well tolerated
• Decreases incidence of malocclusion
• Mortality
• Decreases incidence of infectious diseaseo Diarrhea**
o Respiratory tract infection
o Otitis media
Victora C et al Lancet 2016 475-90

Relative Risk (95%CI) of Diarrhea
Morbidity in Children < 6months
http://apps.who.int/iris/bitstream/10665/95585/1/9789241506120_eng.pdf?ua=1
Relative Risk of diarrhea with breastfeeding
0.37 (0.27-0.50) compared to formula feeding

Relative Risk (95%CI) of Hospitalization Due to
Respiratory Infection, Lower Respiratory Tract
Infection or Pneumonia in Children < 5 Years
http://apps.who.int/iris/bitstream/10665/95585/1/9789241506120_eng.pdf?ua=1
Relative Risk of with breastfeeding
0.43 (0.33-0.55) compared to formula feeding

Evidence of Breastfeeding
Improving Long-term Health
Outcomes ?
Benefits of Breast Milk: Long
Term Outcomes
Most studies were conducted in high income
countries
Probable reduction in:
• Overweight and obesity
• Diabetes
Victora C et al Lancet 2016 475-90
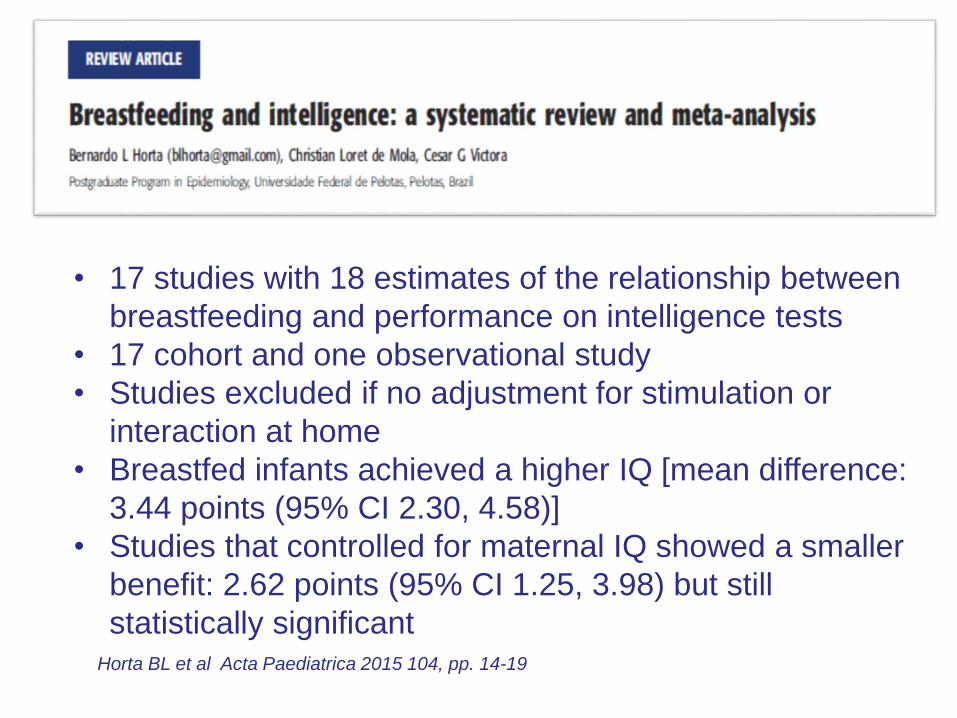
Horta BL et al Acta Paediatrica 2015 104, pp. 14-19
• 17 studies with 18 estimates of the relationship between
breastfeeding and performance on intelligence tests
• 17 cohort and one observational study
• Studies excluded if no adjustment for stimulation or
interaction at home
• Breastfed infants achieved a higher IQ [mean difference:
3.44 points (95% CI 2.30, 4.58)]
• Studies that controlled for maternal IQ showed a smaller
benefit: 2.62 points (95% CI 1.25, 3.98) but still
statistically significant
Benefits of Breastfeeding:
To the Mother• Birth spacing - predominant breastfeeding
associated with longer periods of
amenorrhea
• Reduced risk of breast cancer (exposure
lifetime breastfeeding duration)
• Reduced risk of ovarian cancer with longer
duration of breastfeeding (probable)
• Reduced risk of type 2 diabetes (probable)
Victora C et al Lancet 2016 475-90

Introduction of Iron Rich or Iron-Fortified
Complementary Foods at 6 Months
Nutrition for Healthy
Term InfantsJoint Statement of Health Canada,
CPS, Dietitians of Canada and
Breastfeeding Committee for Canada
• Birth to six months
• 6 months to 24
months
Iron stores laid down in
pregnancy depleted by six
months
Iron naturally low in breast
milk
Deficiency can lead to
anemia and is associated
with irreversible decrease
in cognitive function
https://www.canada.ca/en/health-canada/services/food-nutrition/healthy-eating/infant-feeding.html

Strategies to Prevent Iron
Deficiency
Iron rich foods• meat, poultry, or fish
• fortified cereals
Tip: homemade pureed foods work great (don’t add salt or sugar)
Tip: can transition from infant cereals to ready-to-eat breakfast cereals
Delay introduction of cow’s milk to 12 months as
also low in iron; use iron-fortified cow’s milk-based
formula if weaning
Once cow’s milk introduced limit volume to 3 cups
per day; will limit displacement of iron-rich foods
Iron drops
https://www.canada.ca/en/health-canada/services/food-nutrition/healthy-eating/infant-feeding.html
Other Consideration in
Introducing Solids: Allergy
• When introducing a food that is among the list of
common food allergens, suggest avoid offering >
one of these per day and wait two days before
introducing another of the common food allergens
• Once a potential food allergen has been introduced
successfully, continue to offer the food regularly in
order to maintain the child's tolerance
• Begin introduction of solids while
still breastfeeding
• The order that solid foods are
introduced does not affect the risk
of developing food allergy

Common Food Allergens
• Eggs
• Milk
• Mustard
• Peanuts
• Crustaceans and molluscs
• Fish
• Sesame Seeds
• Soy
• Sulphites
• Tree Nuts
• Wheat and Triticale

Other Consideration in
Introducing Solids
• Encourage parents to be responsive to
their infant’s hunger cues
• Gradually increase number of times/day
complementary foods are offered while
continuing to breastfeed
• Ensure lumpy textures are offered no later
than nine months. Encourage progress
toward a variety of textures, modified from
family foods (limited salt and sugar) by
one year of age

Do Infants Need Vitamin Drops?

Vitamin D Drops
• Vitamin D is low in breast milk
• Vitamin D is an essential nutrient for development of
strong bones and teeth
• Humans can synthesize vitamin D in their skin but
infants should not be exposed to direct sunlight due
to risk of skin cancer
• All breastfed infants should receive a supplement of
400 IU/day
• Vitamin D is added to all cow’s milk and infant
formulas in Canada (it is the law)
• Vitamin D can be added to plant-based beverages
but it is voluntary (need to read labels)

My Child Doesn’t Like
Vegetables

Prevalence of Inadequacy of Vitamins A,
C and Folate from Diet Alone among
Canadian Children - Supplement Users
Age Vitamin A Vitamin C Folate
1-3 years 0 0 0
4-8 years <5 0 0
Males: 9-13 years 16 <5 <5
Females: 9-13 years 14 <5 <5
Shakur Y et al Journal of Nutrition 142(3):534-40, 2012.

Intakes of Vitamins A, C and Folic Acid
Among Canadian Children Above the
Tolerable Upper Level - Supplement Users
Shakur Y et al Journal of Nutrition 142(3):534-40, 2012.
Age Vitamin A Vitamin C Folic acid
1-3 years 88 10 7
4-8 years 67 <5 5
9-13 years 18 <5 <5

Prevalence of Low Blood Levels of
Vitamin A and C in American Children
6 to 11 Years Old
Blood value Sample size Prevalence
Serum vitamin C, <11.4 umol/L 1,703 <1%
Serum vitamin A*, <20 ug/dl 860 1%
CDC. 2nd National Report on Biochemical Indicators of Diet and Nutrition in the U.S. Population, 2012

Resources to Support Parents
https:/www.ontario.ca/page/breastfeeding
Bilingual On-Line Ontario Breastfeeding Services on-line lactation consultant
locations of clinics, peer support locally
Introduction of Solids to your baby
Sample Meals for babies 6-12 months
Homemade baby foods
https://www.eatrightontario.ca/en/default.aspx
www.canada.ca/en/health-canada/services/food-nutrition/
healthy-eating/infant-feeding.html

Resources for Professionals/Parents
for the More Nutritionally Complex
Breastfeeding Program Videos:
The Hospital for Sick Children Toronto
http://www.sickkids.ca/breastfeeding-
program/videos/index.html

The Society of Obstetricians and
Gynecologists: Clinical Practice
GuidelineNo. 333, June 2016
Canadian Consensus on Female Nutrition:
Adolescence, Reproduction, Menopause, and
Beyond
J Obstet Gynaecol Can 2016;38(6):508-554

Concluding Thoughts
• Breastfeed exclusively for the first 6 months,
with introduction of solids at this time and
continued breastfeeding
• First solids should include iron-rich foods
• Breastfed infants require a vitamin D
supplement
• If weaning from the breast before 12 months
use an iron-fortified cow’s milk formula

Nourishing an infant with Cancer
Laura Collins, RD

Overview
• the significance of malnutrition
• the role of the Registered Dietitian
• components of a nutrition assessment
• the nutrition complications
• strategies to optimize nutrition
• future opportunities
• case study

Why is good nutrition important?
• promote growth and development
• improve QOL
• improve treatment tolerance
• decrease infection rate
• decreased LOS
• improve survival

Why is malnutrition in infants with cancerso significant?
• rapid wt gain/growth/development
• limited body reserves
• ability to play and interact
• brain development

What are the causes of malnutrition?
• increased needs: Cancer is a catabolic state
• increased losses: vomiting, diarrhea, malabsorption
• decreased intake: anorexia, nausea, taste changes, mucositis
• Host/Disease/Treatment factors

What are the challenges
in preventing malnutrition?
• poor intake and weight loss
• continuation of breastfeeding and supply
• healthy food choices
• feeding skills/aversions/food battles
• acceptance/tolerance to feeds
• frequent NG re-insertions
• weaning tube feed and transition to oral

The Registered Dietitian

Who is seen by the RD?
All infants with cancer
• weight loss• large tumour burden• HR cancers• intensive treatment protocols• receiving nutrition support

The RD role in pediatric oncology
1. nutrition assessment 2. develop nutrition care plan (NCP)3. provide nutrition education
4. discharge planning for NS
5. ongoing follow-up
6. Interdisciplinary team involvement

Common Goals with Team members
OT/PT: rehab/participation
OT: feeding/swallowing
PharmD: improved tolerance to EN
MD/RN: allies to promote NCP

Case Study: NBLDiagnosis:
• 11mth old female with intermediate risk NBL with a
significant suprarenal mass.
HPI:
• 2 mth history of poor growth and decreased intake of
solids and increased demand for breastfeeding
Clinical:
• appears very pale and thin
Social:
• lives with both parents, no siblings, ++anxious parents

Nutrition Assessment

ABCDE’s of Nutrition Assessment
• Anthropometrics
• Biochemical indices
• Clinical
• Diet/feeding history
• Estimate nutritional requirements

Categories of Nutritional Status
Measure Underweight
Weight for length <10th%ile
-1.32 z score
BMI
(> 2yrs)
<5th%ile
-1.70 z score
Arm
Anthropometry
MUAC (FFM)
< 5th%ile
IBW Severe <70%
Moderate 70-80%
Mild 80-90%
Weight loss > 5-10% in a month
GROWTH FAILURE: crosses over 2 growth channels
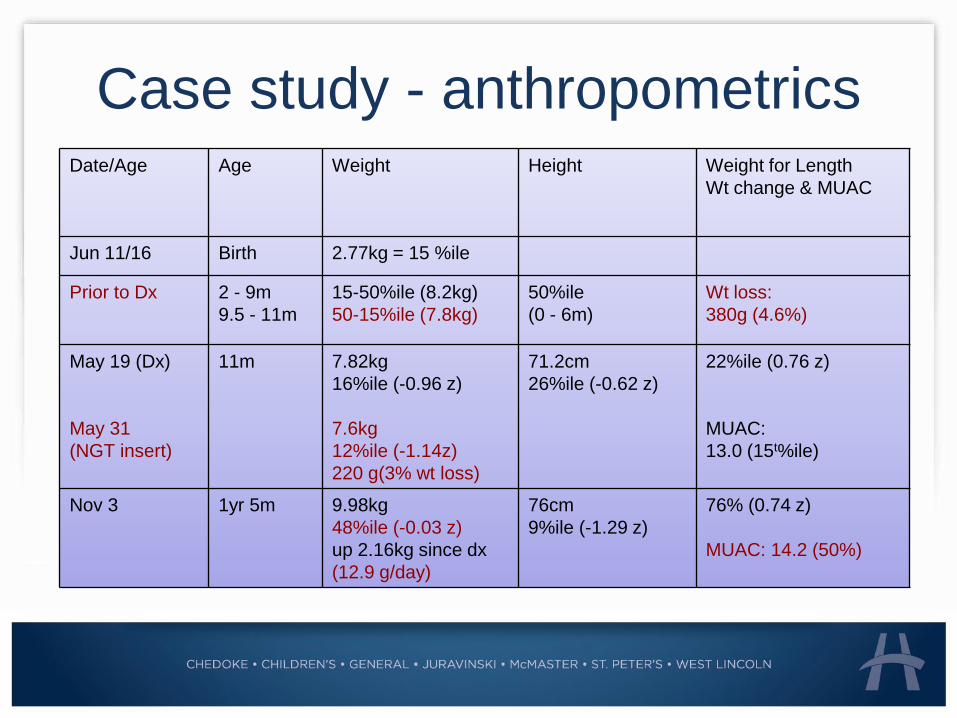
Case study - anthropometricsDate/Age Age Weight Height Weight for Length
Wt change & MUAC
Jun 11/16 Birth 2.77kg = 15 %ile
Prior to Dx 2 - 9m
9.5 - 11m
15-50%ile (8.2kg)
50-15%ile (7.8kg)
50%ile
(0 - 6m)
Wt loss:
380g (4.6%)
May 19 (Dx)
May 31
(NGT insert)
11m 7.82kg
16%ile (-0.96 z)
7.6kg
12%ile (-1.14z)
220 g(3% wt loss)
71.2cm
26%ile (-0.62 z)
22%ile (0.76 z)
MUAC:
13.0 (15t%ile)
Nov 3 1yr 5m 9.98kg
48%ile (-0.03 z)
up 2.16kg since dx
(12.9 g/day)
76cm
9%ile (-1.29 z)
76% (0.74 z)
MUAC: 14.2 (50%)

Case study - anthropometrics

Case study - anthropometrics

Case study - anthropometrics

Growth Velocity
AGE WEIGHT
(g/day)
LENGTH
(cm/mth)
<3 mo 25-35 2.6-3.5
3-6 mo 15-21 1.6-2.5
6-12 mo 10-15 1.2-1.7
1-3 yr 4-10 0.7-1.1
Diet History
• fluid intake (Br.Milk, formula, milk, juice)
• introduction to solids
• changes in intake
• nutritional adequacy of diet
• food/feeding aversions
• allergies and intolerances
• 3 day food record or 24hr recall
• current intake
Case study – diet assessment
Prior to Dx:
• increase in BF demand (ad lib q 3-5 hrs)
• taking some EBM via sippy cup,
• no homo milk or formula being used.
• exclusively breastfed until 5-6mths
• intro to solids was limited (texture sensitive)
• purees often with limited variety of solid
• feed self with finger foods

5
2
Estimating Nutritional Requirements

Calculating nutrition requirements
Fluids: 4:2:1 rule
Calories: 95-100 kcal/kg
Protein: 2g/kg
Carbs: ~ 25-35% of kcals
Fat: ~ 60% of kcals
vit/mins: use DRIs
https://www.nal.usda.gov/fnic/interactiveDRI/
Nutrition Interventions

Nutrition Support Options
• nutrition counseling/education
• dietary modifications and oral suppl’s
• enteral nutrition
• parenteral nutrition

Enteral Nutrition (EN)
• provision of nutrients via tube feeding
• functional GI tract• NG, NJ, GT, GJ
• partial supplementation vs sole source
• proactive EN is encouraged (team/family)
• EBM or formula (concentrated or diluted)
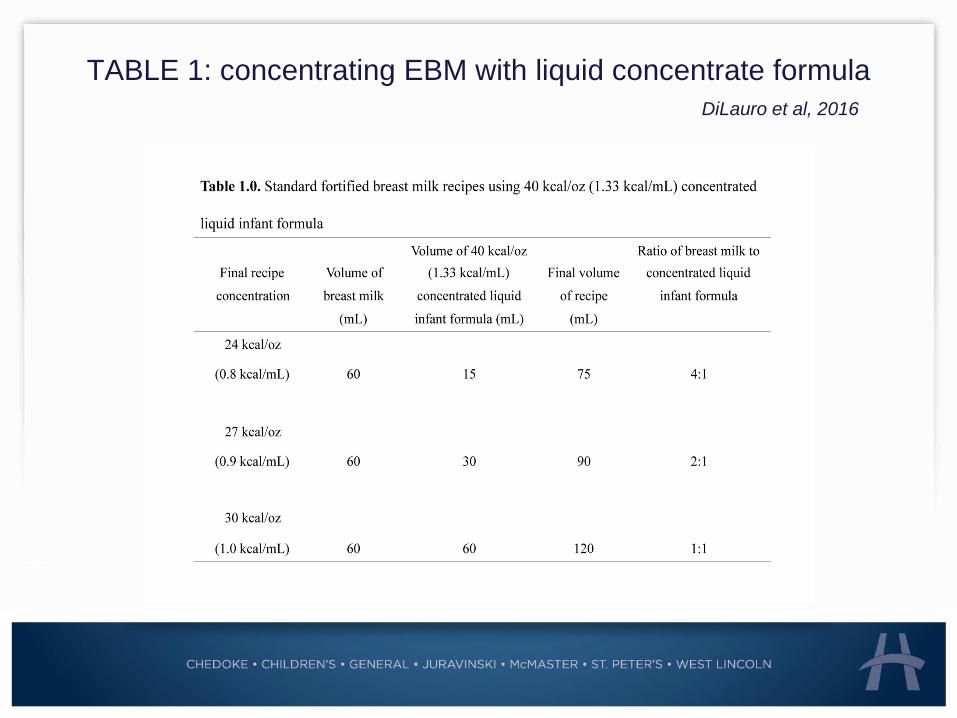
TABLE 1: concentrating EBM with liquid concentrate formula
DiLauro et al, 2016

Breastmilk/Infant Formula
• EBM
• Enfamil A+
• Similac Advance
• Goodstart
• specialized formulas
• standard dilution (0.67kcal/ml)
• Use liquid concentrate (powder used as per
family request) to concentrate formula

Pediatric Formula Choices for >1yr
Type Name/Brand
Standard Polymeric Pediasure
Pediasure Plus
Semi-elemental Peptamen Jr
Peptamen Jr 1.5
Pediasure peptide
Hydrolyzed Vivonex pediatric
Blenderized Tube Feed
(BTF)
Compleat Pediatric
Homemade

Case study – NCP for EN
• concentrated EBM (bottle/cup) & encouraged solids
• NG tube inserted (may 26)
• continuous to intermittent feeds (4 hrs on and 2 hrs off QID)
• concentrated EBM or concentrated Goodstart (up to
30kcal/oz)
• 1:1 ratio of concentrated EBM and Goodstart (due to supply)
• transition to pediatric formula (semi-elemental then
hypercaloric)
• oral intake remains very low with limited variety and textures
• unable to wean off NG feeds due to feeding aversions
• now 3 BOLUS FEEDS: 80% of est needs
6
1
Nutrition Monitoring

Monitoring and adjusting NCP
ORAL: breastfeeding, food intolerances/aversions
EN: tolerance of feed and schedule, adjustments with
chemo oral intake and optimized meds
TPN: not required throughout her treatment
GROWTH: changes (% and z scores) or no growth
nutrition assessment is only as good as the monitoring
ADJUST THE CARE PLAN TO IMPROVE NUTRITION STATUS

Ongoing and Future Projects
• SCAN – implementing screening tool
• Arm anthropometry measurements – serial measures and
consistent use
• Education Tool to help wean/transition from EN to oral
“Helping your child eat while on a tube feed”
• Healthy Eating interventions
Validated Nutrition screening tool for
childhood cancer
SCAN (reference article)
• identifies children with cancer at risk of malnutrition
• 6 simple questions
• Total Score ≥ 3 (“at risk of malnutrition”)
Murphy AJ, et al.

SCANa validated Nutrition Screening tool
1. Does the patient have a high risk cancer?
2. Is the patient currently undergoing intensive treatment?
3. Does the patient have any symptoms relating to the GI
tract?
4. Has the patient had poor oral intake over the past
week?
5. Has the patient had any weight loss over the past
month?
6. Does the patient show signs of undernutrition?

References1. DiLauro S, Unger S, Stone D, O’Connor D. Human milk for ill and
medically compromised infants: Strategies and ongoing innovation.
JPEN. 2016;40(6) 768-782.
2. Ladas, E.D., Sacks, N., Brophy, P., Rogers, P.C. Standards of nutritional
care in pediatric oncology.Pediatr Blood Cancer. 2006;46:339–344.
3. Murphy AJ, et al., Evaluation of the nutrition screening tool for
childhood cancer (SCAN). Clinical Nutrition. 2016;35(1):219-224.
4. Barron M, Pencharz P. Nutritional issues in infants with cancer.
Pediatr Blood Cancer. 2007;49:1093-1096
5. Gaynor EPT, Sullivan PB. Nutritional status and nutritional
management in children with cancer. Arch Dis Child.2015;100:1169-
1172
6. Rogers P. Importance of nutrition in pediatric oncology. Indian J
Cancer. 2015;52:176
7. World Health Organization. The WHO child growth standards.
www.whogrowthcharts.ca

THANK [email protected]















![WELCOME [ct1.medstarhealth.org] · 2016-05-05 · •Cancer is a complex disease •Some risk factors we cannot change •Many risk factors can be reduced •The more you know about](https://img.dokumen.tips/doc/110x75/5f0ea7bc7e708231d4404937/welcome-ct1-2016-05-05-acancer-is-a-complex-disease-asome-risk-factors.jpg)
![Nutrition & Prostate Cancer · 5 • Generally, higher blood levels of lycopene have been associated with a reduced risk of prostate cancer [32, 67-70]. • In one study, plasma levels](https://img.dokumen.tips/doc/110x75/5e1ee022f9e677137e788d28/nutrition-prostate-cancer-5-a-generally-higher-blood-levels-of-lycopene.jpg)