Embed Size (px)
Citation preview

THE ANATOMY AND SURGICAL APPROACHOF THE FOREARM
PRORI FATWA NOOR

The ForearmTwo long bones :
The UlnaThe Radius
Articulate with: The Humerus The carpi

Ulna• Proximal : olecranon and
the coronoid processes.• Distal : a lateral head and
a medial styloid process.

Radius• Proximal : head , neck ,
proximal medial radial tuberosity.
• Distal : carpal articular surface, an ulnar notch, a dorsal tubercle (Lister’s tubercle) and a lateral styloid process.
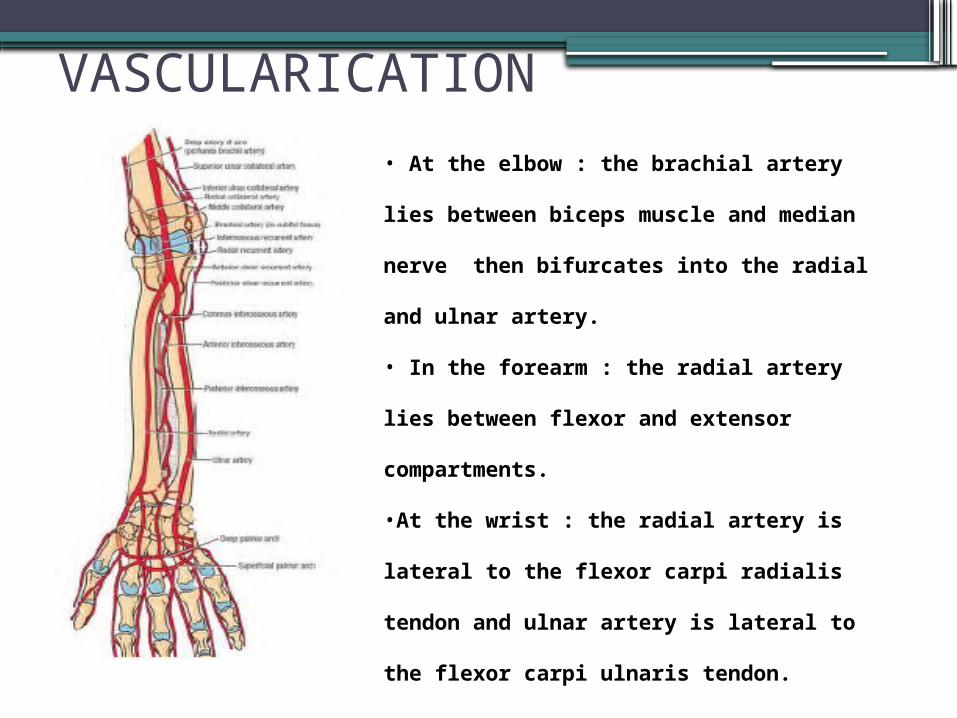
VASCULARICATION• At the elbow : the brachial artery lies
between biceps muscle and median nerve
then bifurcates into the radial and ulnar
artery.
• In the forearm : the radial artery lies
between flexor and extensor
compartments.
•At the wrist : the radial artery is lateral
to the flexor carpi radialis tendon and
ulnar artery is lateral to the flexor carpi
ulnaris tendon.

INNERVATIONRadial Nerve in Forearm
Posterior view

Ulnar nerve

Median nerve

Surgical Approach of the forearm• Proximal anterior / anterolateral for Radius
(Henry)• Posterolateral Approach for (Thompson)• The Posterior expose of the shaft Ulna

Anterior Approach for the Radius(Henry)• This approach is used for the following:
▫ Open reduction and internal fixation of fractures▫ Bone grafting and fixation of nonunion fracture▫ Radial osteotomy▫ Biopsy and treatment of bone tumors▫ Excision of sequestra in chronic osteomyelitis▫ Anterior exposure of the bicipital tuberosity
• Its advantages is an internervous approach with everything on the lateral side being radial nerve innervated and the other side being median nerve part. Also, it is easily allows proximal and distal extension.
• There is no major disadvantages to this approach except lack of surgeon familiarity with it.

the patient supine, the upper extremity being supported on the board or table with the
forearm supinated
Position of the Patient

Biceps tendonBrachioradialisStyloid process of the radius
Landmarks

Internervous plane
Distally, lies between brachioradialis muscle which is innervated by the radial nerve, just proximal to the elbow joint, and the flexor carpi radialis muscle, which is innervated by the median nerve. Proximally, lies between the brachioradialis muscle and the pronator teres.

DangersNerves• The posterior interosseous nerve is vulnerable as it winds
around the neck of the radius within the substance of the supinator muscle.Detach the insertion correctly.
• The superficial radial nerve runs down the forearm under the brachioradialis muscle and become vulnerable when the mobile wad of three muscles is mobilized and retracted laterally. Take care when retracting the nerve.
Vessels• The radial artery run down the middle of the forearm under
the brachioradialis muscle and become vulnerable during mobilization of this muscle and according to the proximal end of the wound as the artery passes to the medial side of the biceps tendon. Remember to remaining lateral to the tendon.
• The recurrent radial arteries aries from the radial artery below the elbow joint, which pass in front of and behind the superficial radial nerve. They must be ligated.

Posterolateral Approach(Thompson)• This approach is used primarily for plating of radius
fractures, that provides access to the proximal two-thirds of the radius. Also for the following :▫ ORIF of radial fractures (extensor side)▫ Treatment of delayed union or nonunion fractures of radius▫ Access to the posterior interosseous nerve such as for
decompression▫ Radial osteotomy▫ Treatment of the radial osteomyelitis▫ Biopsy and treatment of bone tumors
• Its advantages makes the patient positioning easy and the arm doesn’t need to be repositioned for the ulnar plate, when we used for plating both fractures of the forearm.
• Otherwise, this approach put the radial nerve at considerable risk

Position of the Patient
the patient supine with the shoulder abducted and internally rotated, the upper extremity being supported on the board or
table with the elbow flexed and the forearm pronated

•Lateral epicondyle of humery•Litter’s tubercle (the dorsoradial tubercle)
Landmarks

Internervous plane
Proximally, lies between the extensor carpi radialis brevis muscle (innervated by radial nerve) and the extensor digitorum communis muscle (innervated by posterior interosseus nerve).
Distally, lies between extensor carpi radialis brevis muscle (innervated by radial nerve) and the extensor policis longus muscle (innervated by posterior interosseus nerve)

DangersNerves• The posterior interosseous nerve.
Identifying and preserving the nerve in supinator muscle it’s the only means of ensuring that it will not be trapped beneath any plate that is applied for radial fracture.• Vigorous retraction on the brachioradialis
can also damage the sensory branch of the radial nerve.
The Exposure of the shaft Ulna•This approach is used for the following :
▫ORIF of ulnar fractures▫Treatment of delayed union or nonunion
fractures of ulnar▫Osteotomy of the ulnar▫Treatment of the ulnar osteomyelitis▫Treatment of the fibrous anlage of the ulna
in cases of ulnar clubhand▫Ulnar lengthening▫Ulnar shorthening
•It’s the simplest approach of the forearm, uncovering the entire length of the bone.

Position of the Patient
the patient supine with the upper extremity across the chest to expose the subcutaneous border of the ulna with the elbow flexed and the forearm pronated

•Olecranon•Subcutaneous border of the ulna•Styloid process of the ulna
Landmarks

Internervous planeInternervous plane lies between the extensor carpi ulnaris muscle (innervated by posterior interosseous nerve) and the flexor carpi ulnaris muscle (innervated by ulnar nerve).

DangersNerves• The ulnar nerve, travels down under the
flexor carpi ulnaris lies on the flexor digitorum profundus. Will safe as long as FCU is stripped off the ulna subperiosteally
Vessels•The Ulnar artery travels down with the
nerve, lying on the radial side. Will be vulnerable when dissection of the flexor carpi ulnaris is not carried out subperiosteally.

THANK YOU





























