Embed Size (px)
Citation preview

THE AMERICANJOURNAL OF CANCER
A Continuation of The Journal of Cancer Research
VOLUME XXVI I I NOVEMBER, 1936
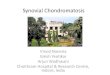
SYNOVIAL SARCOMA
LEILA CHARLTON KNOX, M.D.
NUMBER 3
(From the Pathological Laboratory, St. Luke's Hospital, Dr. Francis Carter Wood, Director)
INTRODUCTION
Among the malignant tumors of the extremities a relatively small grouptake their origin from the specialized connective-tissue cells which form thesynovial linings as well as from the deeper layers of fibrocytes in the walls ofbursae, tendon sheaths, and the articular surfaces of the joints. That thesestructures may give rise to tumors in which the morphology is often highlycharacteristic is not always appreciated. A certain number of them differgreatly from the spindle-cell type of neoplasm derived from nerves or fascia,and may possess pseudo-glandular or other cell relationships by which anorigin from the synovial layer may be suspected. On the other hand, not alltumors of bursae or joint capsules produce these clefts and tubules, some beinguniformly fibrous, with limited but diffusely distributed collagenous or myxomatous material which makes it impossible in some cases to distinguish themfrom spindle-cell sarcoma of bone. Not only are the synovial groups and thefibrosarcomata of the joints less frequent than the osteogenic tumors, but muchless attention has been paid to their structure, diagnostic features, and clinicalcourse, presumably because of their rarity.
The foreign literature, especially the French, has greatly exceeded ourown in the number of excellent papers dealing with the diagnosis and morphology of synovial tumors. But the subject is by no means exhausted. Theactual number of such tumors is very small, and for this reason only scantyinformation regarding them is available in the medical literature. Clinicallyit may be difficult to distinguish such a tumor from an inflammatory lesion,especially if it involves the articular surfaces alone; but since amputationmay be thought advisable, a recognition of the histopathology of these raregrowths is imperative. For these reasons, the histories of three personsoperated upon at Saint Luke's Hospital, New York, are here given, two ofthem followed to a fatal outcome, the third living and suffering from probable
461

462 LEILA CHARLTON KNOX
pulmonary metastases more than three years after amputation of the involvedextremity.'
CASE REPURTS
CASE I: C. D., a woman twenty-two years of age, entered Saint Luke's Hospital onAug. 25, 1921, with a large cyanotic swelling involving the entire elbow region of the rightarm. Three years earlier the patient had become conscious of slight pain with tenderness.beginning on the ulnar side of the forearm, just below the elbow. This gradually grewworse, and a mass appeared. About eighteen months prior to admission the tumor had beenremoved locally. No radiation or other treatment had been given. The growth had recurred after fifteen months, and the edges of the original wound had separated. Since thattime it had grown rapidly in size, until on admission to the Hospital it measured 7 inches indiameter, and was so heavy that the arm had constantly to be supported upon a pillow(Fig. 1). It was painful and throbbing. Softened and hemorrhagic areas alternated withothers which were very hard.
FIG. 1. CASE I: SYNOVIAL SARCOMA OF THE ELBOW
Roentgenograms 'showed no involvement of the bone and no evidence of metastases tothe chest. A small portion of the tumor was then excised for diagnosis, and it was notedat operation that this fragment appeared to be a part of the wall of a cavity, the lining ofwhich was smooth, glistening, and bluish in appearance. Microscopically this fragment wasdiagnosed a sarcoma, probably derived from the fascia.
The patient, being totally incapacitated by this huge ulcerated lesion, consented to anamputation in the proximal half of the upper arm. Upon dissection it was found that thetumor, cellular, soft, and yellowish, contained many large vascular sinuses and interstitialhemorrhages, and had replaced the fatty and fascial structures, invaded both flexor and extensor tendons and both condyles of the humerus. The head of the radius also showedslight softening. The microscopic picture varied considerably, sheets of spindle cells predominating, but a curious differentiation of these cells was present, to such an extent thatone questioned whether or not they were all connective tissue. Some were polygonal incross-section and suggested epithelium, such as appears in some teratoid tumors (Figs. 2and 3), while more of them resembled embryonic connective tissue with a slight tendencytoward a mucoid groundwork (Fig. 4) and with only a few hyaline connective-tissue fibrils(Fig. 5). Mitotic figures were present in both types of cell, but pyknotic nuclei in small
1 For their courtesy regarding the use of the clinical records and for follow-up data, I beg tothank Dr. J. J. Westermann, Jr., Dr. F. W. Solley, Dr. Mather Cleveland, and Dr, Wm. F.MacFee.

FIGS. 2 AND 3. CASE I: SECTIONS FROM SYNOVIAL SARCOMA OF THE ELBOW SnOWING CELL NESTS
St:GGESTING EPITHELIUM. X 300
463

FIGs. 4 AND 5. CASE I: SECTIOSS SnOWING RESEMBLANCE TO EMBRYONIC CONNECTIVE TISSUE WITH
SLIGHT TENDENCY TOWARD A MUCOID GROUNDWORK (FIG. 4, X 300) AND WITH ONLY A
FEW HYALINE CONNECTIVE-TISSUE FIBRILS (FIG. 5, X 240)
464

SYNOVIAL SARCOMA 465
cells with acidophile cytoplasm were also present (Fig. 6). The diagnosis of spindle-cellsarcoma was again made.
The patient recovered uneventfully and left the Hospital in three weeks. She was observed from time to time and remained in good health until early in 1928, when pain beganin the right chest and a swelling appeared in the shoulder. She reentered the Hospital onApril 12, 1928, over seven years after amputation of the arm, suffering from cough, weakness, and anorexia, as well as the large, hard, tender mass in the shoulder. This was situatedmedial to the upper end of the spine of the scapula apparently under the trapezius muscle.The right chest revealed no fluid, but a small amount of blood, indicating that the pleuralcavity probably contained tumor. A small amount of tissue was excised from the posteriortriangle of the right side of the neck, but the growth was very extensive and it was impossible to remove more than a small fraction of the mass. Sections of this material showedit to have the same morphology as the original growth in the arm. The patient was discharged from the Hospital on May 14, 1928, and died at home a short time later, ten years
FIG. 6. CASE I: SECTION SHOWING SARCOMA-LIKE AREA OF TUMOR. X 300
after the first appearance of symptoms and seven and a half years after an amputationwhich, when performed, had been regarded as an operation from which only temporary reliefcould be expected.
CASE II: W. B., a man thirty-three years of age, entered the Hospital on June 11, 1929,with a mass about 6 X 5 X 3 em. in the subcutaneous layers of the skin and fixed to thedeeper tissues in the right popliteal space. It had been present for six months. At firstno symptoms were associated with the growth, but as it gradually increased in size it interfered with flexion and with complete extension of the knee. and the patient walked with alimp. There was slight pain in the medial aspect of the knee, accentuated by walking, butnot radiating. The tumor was firm, non-movable, non-tender, without pulsation or bruit.Roentgenograms showed the bones to be normal in outline and density. A biopsy was made.
When exposed at operation, the mass was bluish in color, incompletely encapsulated,and cystic. Aspiration produced blood which was apparently enclosed within the largesinuses, as the tissue itself was pinkish or yellowish and resembled brain in color and consistency. Microscopic examination showed a cellular fibrous growth composed of spindleshaped cells of the connective-tissue group, and throughout this mass were large numbers of

FIG. 7. CASE II: SECTION OF SYNOVIAL SARCOMA OF TIlE RIGHT POPLITEAL SPACE,
SHOWING DILATED SINUSES. X ISO
FIG. 8. CASE II: SECTlOS OF TUMOR SHOWING Two TYPES OF CELLS WITH MITOSES
IN BOTH TYPES. X 240
466

SYNOVIAL SARCOMA 467
dilated sinuses (Fig. i). Many of these were lined with flattened cells, others with morecuboidal or polygonal cells, some of which appeared to surround large clefts and spacesresembling glands. Some of these cells were so tall and so arranged as to resemble columnarepithelium, but it was decided that they were either the swollen endothelial cells liningobstructed lymphatics, cells from the synovial surface of the bursa surrounded by the growthof tumor cells, or cells of the neoplasm which were reproducing in form the synovial cellsfrom which they had arisen. Mitoses were present in both types of cells (Fig. 8). Muchof the tumor was composed of compact masses of these cells, globular in outline, the cytoplasm swollen and appearing largely as clear mucoid material, and the nucleus eccentric.They did not resemble fat, nor did they stain with Sudan III. The cell membranes werepreserved to a variable degree. The tumor was diagnosed by the writer as a fibrosarcomaof synovial origin (see Fig. 9).
FIG. 9. CASE II: ANOTHER SECTION OF THE TUMOR, SHOWING GLOBULAR CELLS. X 320
A mid-thigh amputation of the leg was performed on June 24, 1929, and the patientwas discharged eleven days later. Dissection of the amputated leg revealed the wide extentof the tumor tissue in the popliteal space, where it formed a nodular mass about 7 em. indiameter, not encapsulated, firmly adherent to the periosteum of the condyle of the femur.The large vessels and nerves were not infiltrated but seemed rather to be pushed aside bythe growth. The joint cavity was entirely free. The vessels were not thrombosed. Microscopic examination of the tissue from several areas showed the morphology to be the sameas that of the fragment previously removed for diagnosis.
The patient returned to the Hospital on Nov. 27, 1931, a year and five months later,because of shortness of breath of ten days' duration. He had been very well most of thetime since discharge until the onset of dyspnea with fatigue and general loss of strength.In the three months before this admission he had lost only three pounds in weight. Theright pleural cavity was found to contain sero-sanguineous fluid and after removal of thisan x-ray of the chest showed a spherical mass in the right lung believed to be a metastatictumor. A course of x-ray treatments was given over this area but with no especial clinical

LEILA CHARLTON KNOX
improvement. The patient went home on Jan. 12, 1932, and died not long afterward. Noautopsy was permitted.
CASE III: A man, M. N., twenty-four years of age, was admitted to Saint Luke'sHospital on July 17, 1932. complaining of pain and swelling in the left foot beginning twoand a half years earlier. About that time the patient had struck his foot on a curb, but nodetails as to the position, extent, or severity of this trauma could be elicited. Soon afterthis he began to experience tenderness on the medial side of the foot with slight swelling.The symptoms became gradually worse, but were never severe enough to be incapacitating.After two months the pain became very severe whenever the toes were hyperflexed orextended.
There was a fluctuating, non-tender swelling 2 inches in diameter on the under surfaceof the foot over the first metatarsal bone, but without involvement of the skin. A roent-
Fro, 10. CASE Ill: SYNOVIAL SARCOMA INVOLVING THE PLANTAR SUR~'ACt: m' THE FOOT. X 65
The tumor cells follow the edge of the synovial sheath.
genogram showed no abnormality, and the condition was thought to be probably a tenosynovitis but of sufficient seriousness to necessitate exploration.
On July 18, 1932, the tumor was partially removed at operation through an incisionover the first metatarsal. It was bluish in color, gave the impression of a thin-walled sacabout 3.5 em. in diameter, and contained dark fluid. It was densely adherent to the surrounding structures and to the flexor hallucis tendon and the first metatarsal. Thesestructures were inseparable, and a single site of origin could not be clearly ascertained.The tumor was thought to be either hemangioma or sarcoma.
Microscopic examination showed an infiltrating tumor composed of small spindle-shapedcells with slight myxomatous degeneration throughout and many areas of necrosis. Thecells varied greatly in size and arrangement, being flat, small,elongated, and firmly cementedtogether where they lined a free surface, presumably a tendon sheath (Fig. 10), but elsewhere forming a compact reticular tissue, with polygonal or globular cells and vesicularnuclei. Mitotic figures were present but not numerous. Collagen was very scarce but a

FIG. 11. CASE III: SECTION Q}' TUMOR SHOWIl>G DISTENDED CELLS CONTAINING PRODUCTS OF
MUCOID DEGENERATION. X 540
FIG. 12. CASE III: SECTION OF TUMOR SHOWING PERITHELIAL ARRANGEMENT OF CELLS. X 225
469

470 LEILA CHARLTON KNOX
mucoid degeneration product was present in many distended cells (Fig. 11). The bloodsupply was very abundant. A diagnosis of fibrosarcoma of the tendon sheath was made.
Amputation was performed on Aug. 6. 1932. through the middle of the leg. Examination of the specimen disclosed a vascular growth of yellowish gelatinous tissue intimatelyconnected with the fascia around the muscles in the sole of the foot. the sheath of the posterior tibial tendon, and the plantar fat. It was adherent at the astragalo-tibial articulationbut had not destroyed the bones. Microscopically the tumor resembled that which hadbeen previously removed. Of special interest in the sections was the definite sheath oftumor cells forming a narrow band around many small capillaries, but with intervening degeneration (Fig. 12).
The patient made an uneventful recovery and remained well until June 1936. nearly fouryears after amputation, when hemorrhagic pleurisy developed. Pulmonary metastases arepresumably present.
SUMMARY OF CASES
Morphologically the three tumors here described are clearly from thesame source, although not identical in appearance. The first occurred in awoman of twenty-two, grew slowly around the tendons of the right elbowfor three years before it necessitated amputation, but was the cause of deathseven years later. The neoplasm was composed of a richly cellular fibroustissue with many rounded or polygonal cell nests resembling epithelial acini,and occasional small pseudo-glands. The second, in a man of thirty-three,involved the tendon sheaths and possibly the bursae in the right poplitealspace, grew rather rapidly for six months, when it had penetrated the softtissues widely. The leg was amputated, but the tumor had probably metastasized at that time and was undoubtedly the cause of death a year and ahalf later. The large cystic spaces and epithelial-like cells were even morefully developed here. The third tumor was in a man of twenty-six, began inthe tendon sheaths on the plantar surface of the left foot, and grew for twoyears and a half before an amputation was performed. The patient remainedwell until four years later, when evidence of pulmonary metastases appeared.The structure of the tissues closely resembled that of a tendon sheath and itis possible that the lesion as it appeared in some portions of the growth wasthat of an approximately normal structure invaded by the neoplasm, butpseudo-glandular acini seen in the two preceding examples were not prominent.All three tumors were extremely vascular, but all consisted essentially ofgrayish yellow, soft, hemorrhagic, cystic or homogeneous tissue. Grosslyalso all contained clefts and cystic spaces, some of which were filled with blood,while others contained only serum.
The most outstanding feature in the microscopic picture was the differentiation which had taken place among the connective-tissue cells, so thata large number of them appeared polygonal, elongated or cuboidal, and seemedto be projecting into free open spaces, while others adjacent to them in thesame field were definitely small, flat, and spindle-shaped, closely knit togetheror separated by a mucoid groundwork. The larger polygonal cells frequentlysurrounded central cavities, in this way suggesting the epithelium of aglandular acinus, except that no basement membrane could be demonstrated;in fact, the absence of any such structure was apparent as the two types ofcells merged into each other. That both these types of cells were actively

SYNOVIAL SARCOMA 471
growing and were an essential part of the tumor is shown by the fact thatmitotic figures were present in considerable numbers, both in the polygonaland in the spindle-shaped cells, and there was often a direct transition fromthe one type to the other. A considerable amount of degeneration was alsotaking place, and pyknotic nuclei alternated with the mitotic figures in thecells of the pseudo-glandular structures. The spindle-shaped cells oftenformed complex imbricated masses and at the same time underwent mucoiddegeneration, although no true mucus was found. The swollen cells producedin this way form one of the most characteristic features of these tumors andled to the early designation of sarcoma [usocellulaire and globocellulaire.Collagenous material was extremely infrequent, but is to be seen in smallamounts in the sections stained with eosin, while in those stained with thetrichrome stain, the corresponding areas were more distinct and intensely bluein color (Fig. 5). In the growth from the foot, the tumor cells were found inclose contact with the blood vessels, a fact which has led some writers to usethe term perithelioma, but which in the present case is understood to be onlyan indication that the nutrition of the cells, which was much better near theblood vessels, had facilitated their growth there.
LITERATURE
The early reports of malignant tumors involving the joints include severalimportant cases, possibly primary synovial sarcoma, especially those of Carre,Marsh, Weir, Turner, Lockwood, and even more particularly for its graphicdetails that of Salter and Hardie, who described the clinical and pathologicalappearance of a joint tumor found in the knee of a man twenty-five years ofage. This case has long been quoted, but the absence of illustrations makingclear its histopathology prevents us from certainly diagnosing it as a synovioma.
Among primary tumors of the joints and tendon sheaths, giant-cell tumorsor xanthomata are the most frequent. These, however, are excluded heresince their origin, metabolic relationships, and morphology place them in aseparate group. In addition they show an entirely different clinical course,for while they may recur, they do not in general exhibit malignant characteristics. Tumors of this group which are often included by earlier writerswith the sarcomata are those described by Julliard and Descoeudres, Moser,Spiess, Ziillig, Janik, Albertini, Gonzales-Aguilar, Faulkner, and many others.
Another group of neoplasms occurring in bursae and other articular structures so closely resemble periosteal spindle-cell sarcoma, both in their appearance and clinical course, that it is doubtful whether the attempt toseparate them has any real value or significance. The joint capsules arenotably poor in cells, and it would seem that many of the slowly growingfibrous tumors, both intra- and extra-articular, may have taken their originfrom these structures. They usually remain encapsulated, nodular, or lobu
-lated, but are prone to late recurrence and eventual metastasis. Such a tumorwas described by Martina in 1906 in the posterior Achilles bursa, and thecompilation of Adrian includes two similar cases, one from the prepatellar andone from the subdeltoid bursa. Tourneux in 1913 published abstracts of 93cases of joint tumors including all of these types, thus surveying the literature

472 LEILA CHARLTON KNOX
since 1852. Razemon and Bizard tabulated records of 45 benign and 29malignant tumors of the joints, the latter including myxoma, fibrosarcoma,chondroma, and others, as well as some of those clearly synovial in origin.
A fibrosarcoma of the knee capsule in a man forty-six years of age wasremoved at operation and reported by Burckhardt in 1909. More recentlyWagner described two cases, one of which also involved the knee joint, in aman of thirty-five who had had pain for ten years befort' a tumor was foundattached to the capsule posterior to the patella. This tumor recurred in oneyear, was again removed locally, and afterward treated with x-rays up to thelimit of skin tolerance, but a further recurrence took place and a year lateramputation was necessary. The patient died nine years after this, presumably with metastasis to the chest, as a large nodule was demonstrable in theroentgenogram. There was pleurisy with effusion and clinical cachexia suchas is seen in connection with malignant tumors. No autopsy was permitted.
Wagner's second case, an intra-capsular tumor of the ankle joint in a girlof fifteen, was also a fibrosarcoma, containing rather small spindle-shapedcells with blunt or triangular appearing nuclei such as are seen in the outerlayers of periosteal fibrous tissue. The outcome of the case is not positivelyknown, but a local recurrence was believed to be present a year later.
Van Neck in 1933 described a periosteal fibrosarcoma of the neck of theastragalus which recurred four years after a local excision. The foot wasamputated six months later, and the patient was well three years afterward.Hohenthal also described a tumor which originated in the knee but whichmetastasized widely and caused death after eight years.
Still another sarcoma of the knee joint was reported by Coley, who founda small tumor 3 X 2 X 0.8 em. attached by a slender stalk to the lining ofthe joint. This tumor apparently consisted largely of undifferentiated fibroustissue, but a diagnosis of synovioma was finally made.
Synovial Sarcoma
More precise knowledge of the synovial group of tumors began in 1906,when v. Ruediger Rydygier described a tumor of the left knee joint in a girlof twenty which caused much swelling, exudation of fluid and blood into thejoint, and the involvement of the entire lining of the cavity with long fingeror bean-like processes which entirely filled it. This material was resectedand diagnosed as a microglobulocellular sarcoma, which graphically describesa tumor of the malignant synovial group. The patient was well eleven monthsafterwards.
Hannemiiller in 1909 reported a sarcoma of the ankle joint in a man fortyfour years of age and was the first to illustrate his paper by a drawing whichshows the two types of cells characteristic of synovial tumor. A biopsy wasperformed followed by a local resection.
The earliest compilation of true synovial tumors, however, is to be foundin the paper of Lejars and Rubens-Duval, who in 1910 reported a single casewith excellent illustrations and clear interpretation of the histopathology.Their patient was a man aged twenty-two who had suffered with severe painin the left knee, worse at night, and in the flexed position. The joint had been

SYNOVIAL SARCOMA 473
observed for three years and treated for rheumatism. Eventually the jointenlarged and a small hard tumor was removed from the intra-articular surface.After this, extension into the soft parts took place rapidly, the skin ulcerated,the bones remaining normal. Amputation was performed shortly afterward.The further history of the patient is not known. The illustrations and description of the morphology show the special features which we now regardas most characteristic of synovial sarcoma.
Chenot and Tzanck described in 1912 a tumor arising from the inner aspect of the left foot at the astragalo-scaphoid articulation in a woman thirtyeight years of age. It had been growing for eight months and caused considerable pain. The skin was not ulcerated and the tumor was somewhatmobile. It was removed locally, was not encapsulated, was bluish or pinkishin color, and composed of stroma containing cylindrical cells which were believed to be endothelial cells from the synovia. The similarity of these structures to intestinal or endometrial mucosa was noted. Following the nomenclature of Lejars and Rubens-Duval, the authors diagnosed this a sarcoma[usocellulaire with cylindrical cells.
Faccini in 1923 published with excellent illustrations in color a report ofa sarcoma of the knee joint in a man thirty-eight years of age. Faccini usedthe term sarcomatous perithelioma because of the grouping of the cells aroundthe blood vessels, with necrotic zones between. The mucoid degenerationand the globular, sheath-like structure are well shown. Unquestionably thistumor is the same as Case III in our series.
Smith in 1927 reported three cases. One occurred on the inner aspectof the thigh, near Hunter's canal, an encapsulated tumor probably associatedwith the tendon sheaths or bursa, death having taken place six months afteroperation, but with no other clinical data available. Probably pulmonarymetastases were present. This tumor was characterized by anastomosingclefts lined with low-cuboidal epithelial-like cells and separated by compactgroups of spindle cells with intercellular fibrils. The second case was in awoman twenty-four years of age who had pain for eight months on the inneraspect of her left thigh, extending to the ankle. A hard mass occupied thespace above Poupart's ligament, extended into the pelvis, around the rectum,and was covered by the adductor muscles. It was very vascular, containedmany cysts with cords of tumor and empty clefts between them. X-ray treatment was given but without much benefit. The patient died with metastases in 1925. Smith's third tumor was in a man thirty-five years of age.Swelling on the inside of the knee had been present for five months, withoutpain. The mass was semi-fluctuating in some areas, and in others very hard.The tumor recurred after local excision, and an amputation was performedfifteen months later, when the entire joint cavity was found to be filled withtumor. Both types of cells, the columnar and the spindle-shaped, werepresent. Metastases eventually took place.
Wegelin in 1928 described with illustrations a synovial sarcoma whichappeared in a man twenty-eight years of age as a small nodule outside of thelower end of the left patella with no history of injury. The clinical appearance was of a joint mouse with intermittent hydrops. The tumor was5 X 4 X 1.5 em., grayish yellow, semi-transparent, with clefts and holes

474 LEILA CHARLTON KNOX
throughout. There was no bleeding, and the growth was covered by a smoothgray membrane. The patient was well five months later.
Tavernier described a woman twenty-three years of age treated for yearsfor periostitis of the left knee, when a small white homogeneous tumor wasremoved from inside the joint capsule. Microscopically it contained longopen spaces lined with endothelium. It recurred in one year, when the entiresynovial membrane was involved and the joint resected. Amputation wasrefused.
Diez, with a good summary of the literature to 1931, included ten caseswhich he believed to be of the synovial type, and added one which he designates an articular endothelioma. The patient was a woman who had sustainedan injury to the knee five years before and had noticed a small tumor sincethat time. It had recently been growing more rapidly, and when exploredwas found to be both intra- and extra-synovial, and was removed locally,amputation being refused. The later history is not given. Microscopicallythe tumor contained many clear spaces with variable types of cells, some beingapparently secretory and resembling epithelium, while the rest were mostlyclosely packed oval or spindle-shaped. There were a few mitotic figures.The article contains photomicrographs which serve to place the tumor in thisgroup.
Cooperman in 1932 reported a tumor in a girl of twenty-one who hadpreviously fallen three feet from a ladder but with only slight injury. Thistumor originated from the outer sheath of the tendon of the flexor brevis andsurrounded but did not involve the tendon. It was diffuse, soft, elastic, andsemi-gelatinous, and was diagnosed a spindle-cell sarcoma of moderate malignancy. After a local operation the patient was well eight months later.
Prym uses the term synovial sarcoendothelioma to describe a tumor ofthe knee joint. A woman sixty-six years of age had had pain in the rightknee for seven years, and a clinical diagnosis of tuberculous arthritis wasmade. A local operation was performed in 1923 and again in January 1924,but amputation became necessary in October of the same year. Extensioninto the pelvis was present a year later, and the patient died in April 1925.No autopsy was performed. The excellent illustrations in this paper indicatethat the long clefts and papillary arrangement may be seen inside a jointcavity as well as in the extra-articular tissues and so are an indication of theorigin of the growth rather than artefacts due to external mechanical influences.
Bonne and Collet have recently reported upon another instance of synovioma which occurred outside of the left knee joint of a woman twenty-fiveyears of age. This probably originated in a bursa. It was partially solid, butwith cystic areas containing gelatinous fluid, and in ten months had grown toa mass 20 em. in diameter. The tumor contained sarcomatous pseudoepithelial cysts, fat, and myxomatous tissue.
Sabrazes and his associates in a series of papers have discussed in considerable detail the pathological conditions occurring in joints and have madea noteworthy contribution to this subject. The malignant tumors observedin such structures are illustrated with a clinical description of one patientwhose history was first reported in 1932 and was brought to a conclusionin 1934 by the fatal termination of the case. The patient was a girl eighteen

SYNOVIAL SARCOMA 475
years of age who was first seen on Sept. 4, 1929, with a tumor of the leftknee on the postero-external aspect, which was at first thought to be apopliteal cyst or an abscess. It had begun insidiously five years before when,although the patient was in full health, the knee had become painful afterwalking, but without swelling. Three years later hydrarthrosis appearedafter bicycling, with tenderness on direct pressure and when the weight wasput on the foot. A mass about 4 X 3 X 3 em. was present in the poplitealspace, painful on pressure, the surface regular and soft. There was limitationof extension. The tumor showed in the roentgenogram as a mass projectingover the head of the peroneus and the head of the tibia. A diagnosis oftuberculous arthritis was made. Operation, however, disclosed a tumor believed to be a sarcoma, although encapsulated. The patient remained wellafter removal until May 1932, when a recurrence in the joint was detected anda series of radiotherapeutic treatments was given between May and July 1932,apparently with some benefit. In October 1933, however, amputation wasperformed but in June 1934 a hemorrhagic pleurisy was present and the patient died with general cachexia in the following month, nearly five years aftershe was first seen, but ten years after the appearance of symptoms.
A malignant synovioma primary in the knee joint has also been reportedby Hodgson and Bishop. The patient was a man twenty-eight years of agewho gave an indefinite history of an injury to the left knee about a yearbefore he was first admitted to the hospital. There was an onset of swellingand pain occurring simultaneously in December 1933, and an enlarged lymphnode was already present in the left inguinal region. Biopsy of this nodeshowed a fibrosarcoma. Heavy x-ray therapy was given to the knee, thighand inguinal region but without affecting either the size of the knee or causingalleviation of the pain. Fluid rapidly accumulated within the joint cavityafter aspiration, and metastases appeared in the skin of the thigh. Death occurred in June 1934, seven months after the apparent onset. No autopsy waspermitted. The photomicrographs which accompany this paper show a somewhat alveolar arrangement of globular cells, but the spindle or fibroblasticcells are not present. Undoubtedly this tumor is properly grouped as asynovioma.
The latest comprehensive paper on this subject is by Zwahlen, who described two malignant tumors of the synovia, one of the tendon sheath of theforearm in a woman twenty-two years of age, the first symptom being painin the hand which appeared early in 1926 and was thought to be due to atuberculous synovitis. X-ray treatment was without effect. In 1928 a biopsywas performed and was diagnosed by Professor Albertini as a relativelybenign unusual type of spindle-cell sarcoma. Two years later pain reappeared and was followed by a large fungating mass of tumor. The arm wasamputated in 1932 but the patient died in 1934 with metastases to the pleura.
Zwahlen's second case was in a young man sixteen years of age seen latein 1929 with a small tumor over the external malleolus, tender, elastic, semifluctuating, but movable on the deeper structures and not involving the skin.This was operated upon and found to infiltrate between the tendons, but notto involve the joint or bone. It recurred and amputation was finally consented to in March 1933, at which time an enormous fungating and ulcerated

476 LEILA (' HARLTON KNOX
tumor was present. Metastases to the pleura and lung followed, and deathtook place in June 1933. At '!1J.1Opsy no other organs were found to be involved. Both of these tum"'-/ ...re unquestionably synovial in type and showthe characteristic microscopic structure.
Fievez demonstrated a tumor of the left ankle joint. The patient was awoman fifty-nine years of age, first observed in 1925, when the tumor was already large and involved the astragalo-tibial articulation and the tendonsheaths, but not the bone. The ankle joint had been somewhat injured bybeing stepped upon by a cow in 1918, but there was no limitation of motion,and the joint became painful only after seven years, when a small mass appeared. A biopsy was advised, but not until 1935, ten years later, did thepatient consent to an operation. Amputation was then performed. Themicroscopic examination showed a malignant fibrous tumor, diagnosed anatypical endothelioma, and believed to be derived from the synovial structures. Epithelial-like cells were found, as well as spindle-shaped ones. Thelater clinical history. is not recorded.
CLINICAL ApPEARANCES
Of the reported cases of synovial sarcoma, 22 in number, 11 have occurredin women, 10 in men, and in one case the sex is not given. About half of thepatients were in their third decade, 3 being under twenty, 9 between twentyand twenty-nine, 4 between thirty and thirty-nine, 1 in the fourth, 1 in thefifth, and 2 in the seventh decade.
Nine of the tumors occurred in the knee joint, while 3, those of Sabrazes,Bonne and Collet, and Knox (Case II), have involved the soft tissues lateralor posterior to the joint, and in these three it is impossible to be certainwhether the tendon sheaths or a bursa of the popliteal space was the exactsite of origin. The cases of Hannemiiller, Chenot and Tzanck, Cooperman,Fievez, Zwahlen (Case II ), and Knox (Case II I) occurred in the ankle jointor one of the tendon sheaths around it.
Only two of the tumors, those reported by Zwahlen (Case I) and Knox(Case I), took their origin from the tendon sheaths of the right forearm, theformer in the mid portion of the extensor surface, the latter around the ulnarside of the cubital space. In two cases, those of Smith (Cases I and II), thetumor appeared in the upper thigh ami pelvis, the latter so diffuse and deeplylocated that the exact site of origin was never determined. In the other casethe tumor appeared in the fascia of Hunter's canal. Prym questions thesynovial origin of these two growths, and suggests that they may have hadsome intra-abdominal source. This negative criticism, however, is weakenedby the fact that there are a large number of bursae beneath the muscles inthe upper part of the thigh.
The duration of symptoms before seeking medical aid was less than ayear in 7 or 32 per cent of the cases, while in 11 other cases, or 50 per cent,this period was longer, from one to seven years. Not often did these tumorsarise in joints which had been the seat of chronic arthritis, unless we acceptthe two cases in which the period was very long-six to seven years-in whichit may be assumed that some inflammatory or benign process had been present.

SYNOVIAL SARCOMA 477
In the case of Lejars and Duval the interval was six years, and the patientonly twenty-two years of age, while in Pryrn's patient, aged sixty-six, theinterval was seven years.
The first symptom in 10 cases was pain, followed shortly afterward inseveral instances by the appearance of a tender mass. In a smaller numberof cases a small growth appeared before any other symptom. Swelling of ajoint with some tenderness was the first symptom in 12 patients. Whetherin a joint or in the tendon sheaths, pain on both flexion and extension has beennoticed.
Trauma as a predisposing or exciting cause has not as yet been shown tohave been effective. In fact, most of the records specify that there had beenno knowledge of injury. The case of Fievez is an exception, as the patientappears to have had some disability for seven years after a local injury at thesite of the tumor. In Case III of Knox there was also a history of trauma,though the details were not clear.
PROGNOSIS AND TREATMENT
The prognosis in this group of tumors is unfavorable. Omitting nearlyall of the earlier cases which were reported without a subsequent statement asto the outcome, there remain 10 cases in which a fatal termination has takenplace, or in which it was highly probable at the time of the final report. Theinterval between the time these patients were first treated and the time oftheir terminal illness has varied from seven months to seven and a half years.Sabrazes' patient survived four years after a local operation, but succumbedeight months after amputation. In the three cases here reported, however,with amputation performed relatively early in two, the patients remained ingood health for one and four years, while in the first case amputation evenat an advanced stage kept the patient in good health for seven and a half years.
It is unlikely that radiotherapy will prove effective. The patients ofZwahlen, of Hodgson and Bishop, and of Smith, whose tumors were in theextremities and could be subjected to a large amount of radiation, were notmaterially benefited. Adair has recently stated that the three recurrent casesunder treatment at the Memorial Hospital have received some benefit fromx-ray, but that these tumors were not being influenced sufficiently to justifyexpectation of ultimate improvement. In this respect these synovial tumorsapparently behave much the same as the fibrosarcomata, and although morecellular and with numerous mitoses, they are apparently resistant to radiotherapy.
SURGICAL PATHOLOGY
At operation the appearance of these tumors when in a joint cavity ischaracterized by the soft vascular or fleshy villous processes which may beseen to arise from all portions of the lining of the joint. This, however, doesnot distinguish them from certain inflammatory states, and it is more by thesoft, cellular quality of the tumor that their malignancy may be distinguishedfrom the more fibrous hypertrophic masses occasionally seen in inflammatory

478 LEILA CHARLTON KNOX
states. If the tumor arises in the soft tissues around the tendon sheaths ornear a bursa, it may usually be distinguished by the presence of bluish, cysticspaces, and a slightly gelatinous ground substance which is recognized onsection. Between these spaces and clefts the cellular tissue may be gray,yellowish, or pinkish in color. A partial capsule is often found to be present,and is sometimes a deceiving factor in judging of the malignancy of the growth.The tumor of Hodgson and Bishop metastasized to the inguinal nodes, butthis has not been generally observed as an early phenomenon. Autopsies havebeen performed only in the cases of Zwahlen, but several patients have diedwith hemorrhagic pleurisy, undoubtedly due to metastases.
In the popliteal space or other region where this type of growth has beenmost frequent, it can probably usually be distinguished from a neurogenic sarcoma by its cystic and vascular structure, while the neurogenic tumor growseither as a diffuse fibrous mass or shows tortuous coils of glistening tissueresembling a nerve trunk. The nodular neoplasms which are orange-brownin color and found in the vicinity of tendon sheaths or within a joint arealmost invariably of the giant-cell type, and are relatively benign.
The variations in microscopic morphology of joint tumors are well illustrated in the three cases here reported. The synovial layer of the joint,tendon sheath, or bursa is reproduced or modified in varying degrees. Insynovioma there are large, rounded or elliptical cells which tend to arrangethemselves perpendicular to the fibrous layer and thus simulate the twolayers of the synovial membrane, and demonstrate a characteristic whichseems as much a part of their nature as is the arrangement of the cells of anosteo- or chondrosarcoma. In the latter, distinguishing structural arrangements are constantly seen by every pathologist, and it is only because of theinfrequency of this group of tumors that their histogenesis is not alwaysrecognized, and their origin determined. It has been stated that the pseudoglandular arrangement is an artefact and has no histogenetic significance.Such pictures, however, are not seen except in structures from synovial membranes. The case of Prym, in which the identical morphology of a synoviomaarising in the soft tissues was reproduced by a growth which was wholly intraarticular, indicates also that the morphology of the tumor is dependent uponits synovial origin rather than upon the position in which it grows.
Neither the gross nor the microscopic diagnosis of joint tumors is necessarily simple. Certain varieties, as the giant-cell tumors of tendon sheaths,are recognizable under almost all conditions, but the synoviomata can scarcelybe distinguished from other sarcomata unless the sections happen to containsome of the special morphological structures in which cysts or pseudo-glandsor cell nests are to be found, or, in the fibrous portion, rounded, globular cellswith intracellular mucoid accumulations and perivascular grouping of theselarge, globular, or polygonal cells. Other less cellular tumors will show onlythe morphology of a spindle-cell sarcoma, in which the synovia may not shareto any appreciable extent, even though the growth is intra-articular or intracapsular. Special stains have so far failed to disclose the cytoplasmic projections characteristic of the lining cells of the large articulations, but it ispossible that some method of staining these may eventually be found.
The nomenclature of these tumors has been a matter of considerable dis-

SYNOVIAL SARCOMA 479
cussion, even among those who admit that they arise from the synovial tissues.They have been variously designated as myxosarcoma, sarcoma fuso-globocellulaire, villous angiofibroma, perithelioma, synovial sarco-endothelioma,and by other descriptive terms. Recently the name synovioma has come intomore general use, and this term, which emphasizes the histogenesis, is convenient because of its anatomical significance, and is as suitable as many ofthe other similar descriptive terms in general use, as hepatoma or meningioma.Moreover, since synovial· cells are at present recognized as a special modification of connective tissue, and not endothelium, it would seem that the termendothelioma should not be continued. The biological sciences have alwaysto be revised in their nomenclature, as well as in their fundamental concepts,and for the purposes of surgical diagnosis, the anatomical names are greatlyto be preferred.
CONCLUSIONS
Synovial sarcoma is a rare form of malignant tumor of the extremities.Abstracts of nineteen such cases from the literature are here included, andthree new cases are reported. Malignant tumors of the joints, bursae, andtendons may usually be separated into one of two groups, fibrosarcoma orsynovial sarcoma. The latter are recognized microscopically by the epitheliallike cells lining tubules, pseudo-glands or clefts, outside of which exists a densefeltwork of connective tissue. Synovial sarcoma is apparently resistant toradiation, nor have any permanent cures by amputation been recorded.
BIBLIOGRAPHY
ADAIR, F. E.: Ann. Surg. 101: 810, 1935.ADRIAN, C.: Beitr. z. klin. Chir. 38: 459, 1903.AGRIFOGLIO, M.: Ann. ital. di ehir. 7: 1220, 1928.v. ALBERTINI, A.: Gutartige Riesenzellgeschwulste, Leipzig, Thieme, 1928.BONNE, C., AND COLLET, A. M.: Geneesk, tijdsehr. v. Nederl-Indie 75: 1384, 1935.BURCKHARDT, H.: Deutsche Ztschr. f. Chir. 101: 467, 1909.CHENOT AND TZANCK: Bull. et memo Soc. anat. de Paris 87: 293,1912.COLEY, W. B.: Ann. Surg. 101: 805, 1935.COOPERMAN, M. B.: ]. Bone & Joint Surg. 14: 173, 1932.DIEZ, J.: Prensa med. argent. 18: 487, 1931.ENDERLEN: Med. Klin. 16: 721, 1920.FACCINI, D.: Arch. ital. di chir. 7: 481, 1923.FAULKNER, D. M.: Surg., Gynec. & Obst. 53: 189, 1931.FIEVEZ: Bull. et memo Soc. nat. de ehir. 61: 1034, 1935.GARRE, C.: Beitr. z. klin. Chir. 7:232, 1891.GESCHICKTER, C. F., AND COPELAND, M. M.: Tumors of Bone, published by Am. ]. Cancer,
N. v., 2nd Edition. 1936.GONZALES-AGUILAR,].: ]. Bone & Joint Surg. 12: 280, 1930.HANNEMULLER: Beitr. Z. klin. Chir. 63: 307, 1909.HODGSON, F. G., AND BISHOP, E. L.: J. Bone & Joint Surg. 17: 184, 1935.HOHENTHAL, T.: Finska lak-sallsk. hand!. 76: 458, 1934.JANIK, A.: Ann. Surg. 85: 897, 1927.JULLIARD, C., AND DESCOEUDRES, F.: Arch. internat. de chir. 1: 537, 1904.LEJARS AND RUBENS-DUVAL: Rev. de chir. 41: 751, 1910.LOCKWOOD, C. B.: Trans. Clin. Soc. London 35: 139, 1902.LOUBAT, E., AND MAGENDIE,].: Gaz. hebd. d. sci. med. de Bordeaux 53: 760,1932.

480 LEILA CHARLTON KNOX
MARQUaRT, W.: Zur Histologie der Synovialmembran, Freiburg Thesis, 1930.MARSH, H.: Lancet 2: 1330, 1898.MARTINA, A.: Deutsche Ztschr. f. Chir. 83: 317, 1906.MAXIMOW, A. A., A:-.ID BLOOM, W.: Text-book of Histology, W. B. Saunders Co., Phila-
delphia, 1930.MOSER, E.: Deutsche Zlschr. f. Chir. 9S: 306. !liOl) .
PRVM, P.: Virchows Arch. f. path. Anal. 271) : 71, 1930.RAZEMON, P., AND BIlARD, G.: Rev. de chir. so: 229, 1931.V. RUEDIGER RVDVGIER, A. R.: Deutsche Ztschr. f. Chir. 82: 211, IlJ06.SABRAZES, J., AND DE GRAILLV, R.: Gaz. hebd. sci. med, de Bordeaux 53: 449, 1932.SABRAZES, J., LOUBAT, E., DE GRAILLV, R., AND MAGENDlE, ].: Gaz. hebd. sci. rned de
Bordeaux 53: 481, 513, 1932; 55: 754,1934.SABRAZES. J.. MO:-.lTPELI.IER. J" DUBOUCHER, D., A:-.ID DE GRAILLV, R.: Gaz. hebd. sci. rned.
de Bordeaux 53: 769, 1932.SALTER AND HARDIE: Lancet 1: 1619, 1894.SAVARIAUD: Bull. et memo Soc. anal. de Paris 80: 890, 1905.SMITH, L. W.: Am.]. Path. 3: 355,1927.SPIESS, P.: Frankfurt. Ztschr. f. Path. 13: 1, 1913.TAVERNIER: Lyon chir. 27: 522, 1930.TOURNEUX,]. P.: Rev. de chir. 47: 817, 1913.TURNER, G. R.: Trans. Clin. Soc. London 35: 137,1902.VAN NECK: Scalpel 86: 1141, 1933.\·ILLARD. P. V.: Contribution a l'etude des sarcomes primitifs de la synoviale du genou,
These de Paris, 1929.\VAGNER, L. c.. Ann. Surg. 92: 421, 1930.WEGELIN, c.: Schweiz. med. Wchnschr. 9: 722,1928.WEIR, R. F.: New York M. ]. & Rec. 29: 725, 1886.ZULLIG, J.: Cor.-Blatt f. Schweizer Aerzte 47: 1368,1917.ZWAHLEN, P.: Bull. de l'Assoc. franc, p. l'etude du cancer 24: 682, 1935.