Embed Size (px)
Citation preview

1
The First 1000 days: The Importance of
Early Brain and Childhood Development
Colleen Kraft, M.D., F.A.A.P.
Professor of Pediatrics
Virginia Tech Carilion School of Medicine and Research Institute
Realizing the
Potential of
Pediatrics
Disclosures
• Senior Medical Officer for MajestaCare, a
Medicaid Managed Care ACO
• Merck Vaccines, speaker and Advisory Board
• Expert Panel, Text4Baby
Learning Objectives
• Understand the role of toxic stress in
the intergenerational transfer of
health disparities;
• Present an organizing, integrated,
ecobiodevelopmental framework;
• Discuss ways pediatricians might
advocate in translating science into
healthier life-courses

2
Critical Concept #1
Childhood Adversity has Lifelong Consequences.
Significant adversity in childhood is
strongly associated with
unhealthy lifestyles and
poor health decades later.
The Adverse Childhood
Experiences Study
(ACE Study)
“In my beginning is my end.”
T.S. Eliot, Four Quartets
ACE Study Findings
• Childhood experiences are powerful
determinants of who we become as adults
3
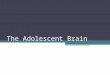
HMO Members in ACE Study
• 80% White,
including Hispanic
• 10% Black
• 10% Asian
• About 50% men,
50% women
• 74% had attended
college
• 62% age 50 or older
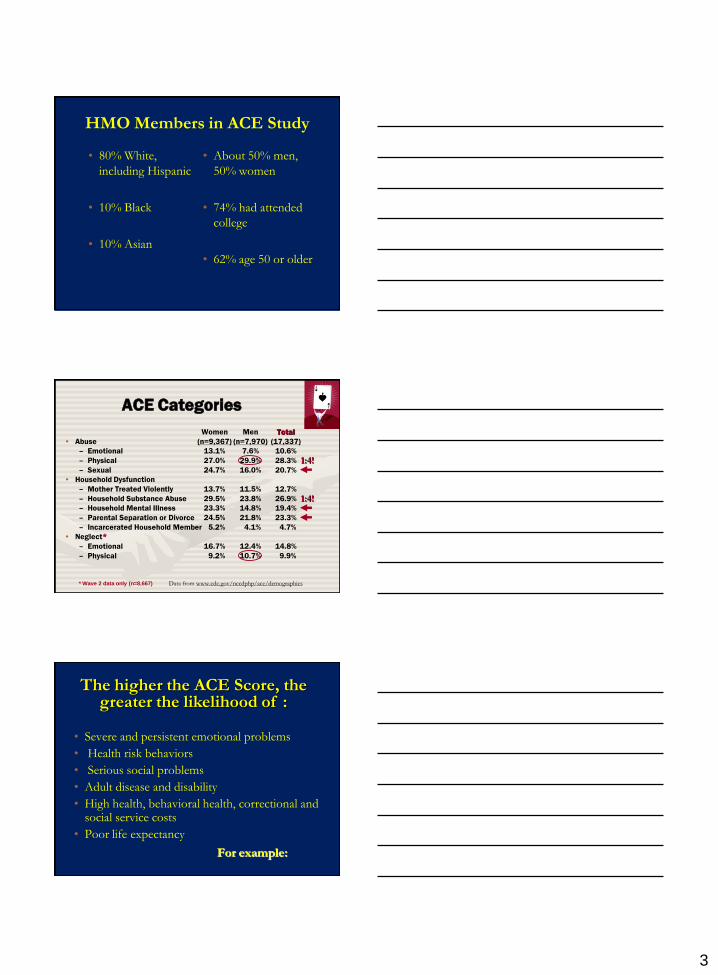
ACE Categories
Women Men Total
• Abuse (n=9,367) (n=7,970) (17,337)
– Emotional 13.1% 7.6% 10.6%
– Physical 27.0% 29.9% 28.3%
– Sexual 24.7% 16.0% 20.7%
• Household Dysfunction
– Mother Treated Violently 13.7% 11.5% 12.7%
– Household Substance Abuse 29.5% 23.8% 26.9%
– Household Mental Illness 23.3% 14.8% 19.4%
– Parental Separation or Divorce 24.5% 21.8% 23.3%
– Incarcerated Household Member 5.2% 4.1% 4.7%
• Neglect*
– Emotional 16.7% 12.4% 14.8%
– Physical 9.2% 10.7% 9.9%
* Wave 2 data only (n=8,667) Data from www.cdc.gov/nccdphp/ace/demographics
1:4!
1:4!
• Severe and persistent emotional problems
• Health risk behaviors
• Serious social problems
• Adult disease and disability
• High health, behavioral health, correctional and social service costs
• Poor life expectancy
For example:
The higher the ACE Score, the greater the likelihood of :
4
• Sexually Transmitted Disease
• Liver Disease
• COPD
• Ischemic Heart Disease
• Autoimmune Disease
• Lung Cancer
Higher ACE Score = significant rise in
chronic health conditions:
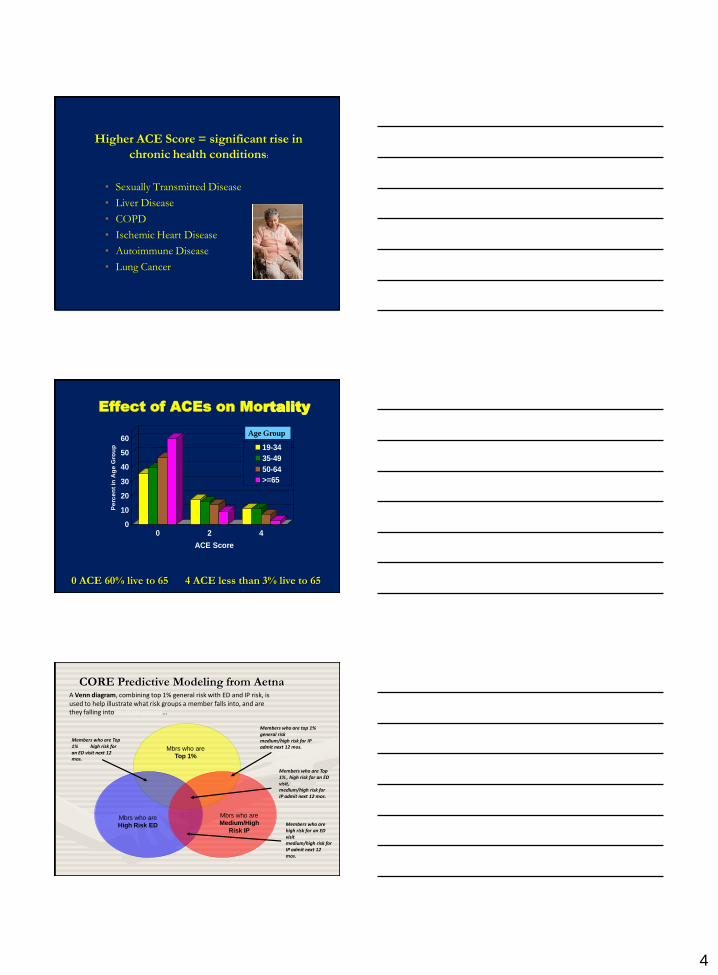
Effect of ACEs on Mortality
0
10
20
30
40
50
60
Pe
rce
nt
in A
ge
Gro
up
0 2 4
ACE Score
19-34
35-49
50-64
>=65
Age Group
0 ACE 60% live to 65 4 ACE less than 3% live to 65
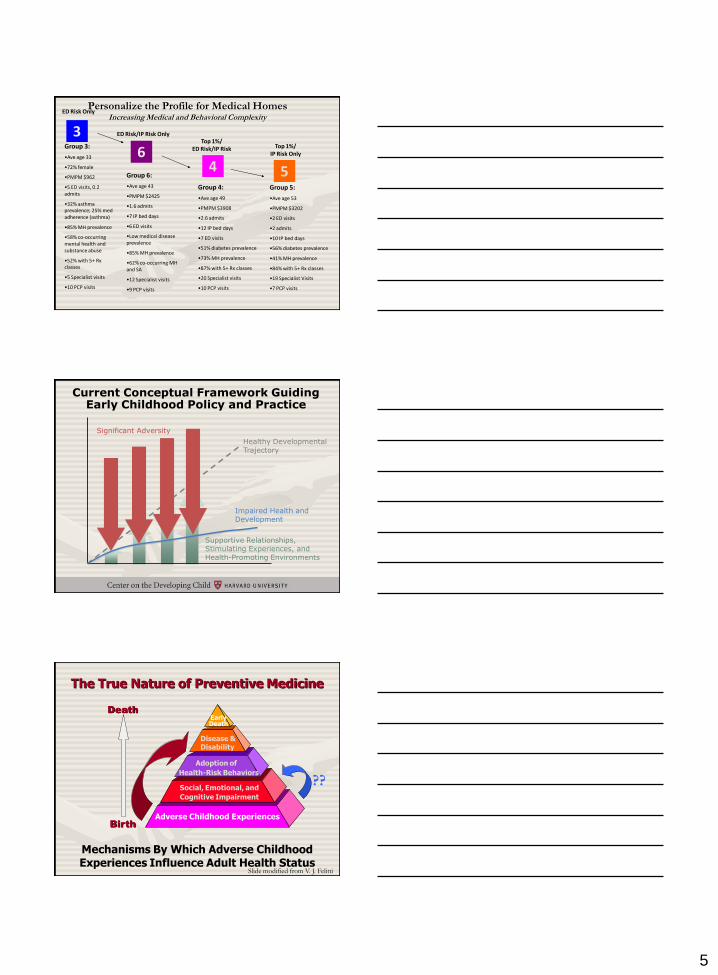
CORE Predictive Modeling from Aetna
Mbrs who are
Top 1%
Mbrs who are
High Risk ED
Mbrs who are
Medium/High
Risk IP
A Venn diagram, combining top 1% general risk with ED and IP risk, is used to help illustrate what risk groups a member falls into, and are they falling into multiple groups…
Members who are Top 1% AND high risk for an ED visit next 12 mos.
Members who are Top 1% , high risk for an ED visit, AND medium/high risk for IP admit next 12 mos.
Members who are top 1% general risk AND medium/high risk for IP admit next 12 mos.
Members who are high risk for an ED visit AND medium/high risk for IP admit next 12 mos.
5
Personalize the Profile for Medical Homes Increasing Medical and Behavioral Complexity
Group 3:
•Ave age 33
•72% female
•PMPM $962
•5 ED visits, 0.2 admits
•32% asthma prevalence; 25% med adherence (asthma)
•85% MH prevalence
•58% co-occurring mental health and substance abuse
•52% with 5+ Rx classes
•5 Specialist visits
•10 PCP visits
Group 4:
•Ave age 49
•PMPM $3908
•2.6 admits
•12 IP bed days
•7 ED visits
•51% diabetes prevalence
•73% MH prevalence
•87% with 5+ Rx classes
•20 Specialist visits
•10 PCP visits
Group 6:
•Ave age 43
•PMPM $2425
•1.6 admits
•7 IP bed days
•6 ED visits
•Low medical disease prevalence
•85% MH prevalence
•62% co-occurring MH and SA
•12 Specialist visits
•9 PCP visits
3
6 4
Group 5:
•Ave age 53
•PMPM $3202
•2 ED visits
•2 admits
•10 IP bed days
•56% diabetes prevalence
•41% MH prevalence
•84% with 5+ Rx classes
•19 Specialist Visits
•7 PCP visits
5
ED Risk Only
ED Risk/IP Risk Only Top 1%/
ED Risk/IP Risk Top 1%/ IP Risk Only
Significant Adversity
Supportive Relationships, Stimulating Experiences, and Health-Promoting Environments
Healthy Developmental Trajectory
Impaired Health and Development
Current Conceptual Framework Guiding Early Childhood Policy and Practice
Mechanisms By Which Adverse Childhood Experiences Influence Adult Health Status
Adverse Childhood Experiences
Social, Emotional, and
Cognitive Impairment
Adoption of
Health-Risk Behaviors
Disease & Disability
Early Death
Death
Birth
The True Nature of Preventive Medicine
Slide modified from V. J. Felitti
??

6
Developing a Model of
Human Health and Disease
Life Course Science
Early childhood ecology
strongly associates with
lifelong developmental outcomes
What are the
mechanisms
underlying these
well-established
associations?
How do you
begin to define
or measure the
ecology?
Defining Adversity or Stress
• How do you define/measure adversity?
• Huge individual variability
– Perception of adversity or stress (subjective)
– Reaction to adversity or stress (objective)
• National Scientific Council on the Developing Child (Dr. Jack Shonkoff and colleagues)
– Positive Stress
– Tolerable Stress
– Toxic Stress
Based on the REACTION
(objective physiologic responses)
• Positive Stress
– Brief, infrequent, mild to moderate intensity
– Most normative childhood stress
• Inability of the 15 month old to express their desires
• The 2 year old who stumbles while running
• Beginning school or daycare
• The big project in middle school
– Social-emotional buffers allow a return to baseline
(responding to non-verbal clues, consolation, reassurance, assistance in planning)
– Builds motivation and resiliency
– Positive Stress is NOT the ABSENCE of stress
Defining Adversity or Stress

7
• Toxic Stress
– Long lasting, frequent, or strong intensity
– More extreme precipitants of childhood stress (ACEs)
• Physical, sexual, emotional abuse
• Physical, emotional neglect
• Household dysfunction
– Insufficient social-emotional buffering (Deficient levels of emotion coaching, re-processing, reassurance and support)
– Potentially permanent changes and long-term effects
• Epigenetics (there are life long / intergenerational changes in how the genetic program is turned ON or OFF)
• Brain architecture (the mediators of stress impact upon the mechanisms of brain development / connectivity)
Defining Adversity or Stress
Critical Concept #2
Epigenetics:
• Which genes are turned on/off, when, and where
• Ecology (environment/experience) influences
how the genetic blueprint is read and utilized
• Ecological effects at the molecular level
• Stress-induced changes in epigenetic markers
Biology Physiologic Adaptations
and Disruptions
Life Course Science
Through epigenetic mechanisms,
the early childhood ecology becomes
biologically embedded, influencing how the genome is utilized
Developing a Model of
Human Health and Disease

8
Critical Concept #3
Developmental Neuroscience:
• Synapse and circuit formation are experience and
activity dependent
• Ecology (environment/experience) influences how
brain architecture is formed and remodeled
• Early childhood adversity -> vicious cycle of stress
• Diminishing cellular plasticity limits remediation
• Potentially permanent alterations in brain
architecture and functioning
Two Types of Plasticity
• Synaptic Plasticity –
– Variation in the STRENGTH of individual connections
– “from a whisper to a shout”
– Lifelong (how old dogs learn new tricks)
• Cellular Plasticity –
– Variations in the NUMBER (or COUNT) of connections
– “ from one person shouting to a stadium shouting”
– Declines dramatically with age (waning by age 5)
Brain Stem & Cranial Nerves:
Vital functions Swallowing
Cerebellum:
Smooth movements Coordination
Occipital Lobe:
Visual processing
Parietal Lobe:
Integration of sensory data and movement
Temporal lobe (outside):
Processing sound and language
Limbic System (inside):
Emotions and impulsivity
Frontal lobes:
Abstract thought, reasoning, judgment, planning, impulse and affect regulation, consequences
Brain Structure (and Function)
+ The Gas Pedal +
Amygdala
- The Brake – PFC (with some hippocampal help)
9
Impact of Early Stress
TOXIC STRESS
Chronic “fight or flight;” adrenaline / cortisol
Changes in Brain Architecture
Hyper-responsive stress response; calm/coping
CHILDHOOD STRESS
Development results from an on-
going, re-iterative, and cumulative
dance between nurture and nature
Brain Development
Alterations in Brain
Structure and Function
Experience
Protective and Personal
(versus Insecure and Impersonal)
Epigenetic Changes
Alterations in the Way the
Genetic Program is Read
Behavior
Adaptive or Healthy Coping Skills
(vs. Maladaptive or Unhealthy Coping Skills)
Biology Physiologic Adaptations
and Disruptions
Life Course Science
Declining plasticity in the developing brain results in potentially permanent
alterations in brain functioning and development
Developing a Model of
Human Health and Disease

10
Eco-Bio-Developmental
Model of Human Health and Disease
Biology Physiologic Adaptations
and Disruptions
Life Course Science
The Basic
Science of Pediatrics
Ecology
Becomes biology,
And together they drive development across the lifespan
Critical Concept #4
The Science of
Early Brain and
Child Development
Epigenetics Physiology of Stress Neuroscience
Education Health Economics
One Science – Many Implications
The critical challenge now is to translate
game-changing advances in developmental science
into effective policies and practices for families w/ children
to improve education, health and lifelong productivity
Childhood Adversity Poor Adult Outcomes
Toxic Stress
Epigenetic Modifications
Disruptions in Brain Architecture
Behavioral Allostasis
Linking Childhood Experiences and
Adult Outcomes

11
It’s
Health
Equity
It’s early
brain &
child dev
It’s epi-
genetics
It’s
foster
care It’s
mental
health
It’s
obesity
Toxic Stress
…it’s a little like the blindfolded man feeling the
elephant
The Problems of Children And Families that We Focus on: Are Parts of the Elephant
It’s problems
of immigrant
children
It’s food
insecurity
It’s low
immuniz.
rates
It’s poor
oral
health
It’s
poverty
The BIG Questions are…
3) What does this mean for pediatrics
– particularly for primary care?
Critical Concept
For young children,
parent/caregiver support is critical:
• Turns off physiologic stress response by addressing physiologic and safety
needs
• Turns off the physiologic stress response by promoting healthy relationships
and attachment
• Notes and encourages foundational coping skills as they emerge
Pediatricians are ideally placed to:
• Promote this sort of “Purposeful” Parenting
• Advocate for a public health approach to address toxic stress

12
• Primary / Universal Prevention – Proactive, universal interventions to make stress
positive, instead of tolerable or toxic
– Acknowledges that preventing all childhood adversity is impossible and even undesirable
– Actively building resiliency (“immunizing” through positive parenting, 7C’s of resilience, promoting optimism, formalized social-emotional learning)
– SE Buffers allow the physiologic stress response to return to baseline
•Parenting skills for younger children
•SEL skills for older children (www.casel.org)
Addressing Toxic Stress
Promoting the Five R’s of Early
Childhood Education
• READING together - daily
• RHYMING, playing and cuddling
• ROUTINES – help children know
what to expect of us - what is expected of them
• REWARDS for everyday successes – PRAISE is
a powerful reward
• RELATIONSHIPS, reciprocal and nurturing –
foundation of healthy child development
• Secondary / Targeted Preventions
– Focused, targeted interventions for those deemed to be
“at high risk”
– Visiting Nurse Programs (Nurse Family Partner.)
– Parenting Programs (Triple-P, Nurturing Parent.)
– More likely to be effective; minimize “damage”
– Requires screening
Addressing Toxic Stress

13
Addressing Toxic Stress
• Treatment of the consequences – TF-CBT and PCIT are evidence-based
– Reactive – some “damage” already done!
– Very COSTLY
– Efficacy linked to age and chronicity
•Declining brain plasticity?
– Insufficient number of / access to providers
– Persistent STIGMA
•“Character Flaws” vs “Biological Mal-adaptations”
Universal Primary Preventions
Bright Futures
Connected Kids
Circle of Security
Relationships as a “vital” sign
Basic EBCD Competencies
Targeted Interventions
Screening for risks
(assess the ecology)
Refer to/advocate for EBI
Collaborating/Developing EBI
Mid-level Competencies
Evidence-Based Treatments
Screening for diagnoses
Common factors approach
Refer for/advocate for EBT
Collaborating/Developing EBT
Advanced Competencies
WHAT are we DOING?!
New Protective Interventions
Building an Enhanced Theory of Change that Balances Enrichment and Protection
Significant Adversity
Healthy Developmental Trajectory
Supportive Relationships, Stimulating Experiences, and Health-Promoting Environments

14
Public Investment in Children
by Age
Quality Early Care and Education
Pays Off: Cost/Benefit Analyses
Show Positive Returns
41
$2
$6
$8
$4
$10
$3.23
Abecedarian Project (early care and
education aged 0-5)
$5.70
Nurse Family Partnership
(home visiting prenatal – age 2 for
high risk group)
Perry Preschool (early education age 3-4)
Total Return per $1 Invested
Data Sources: Heckman et al. (2009) Karoly et al. (2005)
Break-Even Point
0
$9.20
Graph Courtesy: Center on the Developing Child at Harvard University
State Network Business leader organizations in many states have
started supporting proven investments in early childhood. ReadyNation has sponsored business
leader summits and provided other types of assistance
to support business leader engagement in over half
the states. There are also many other business groups
in the states working in early childhood. Click on the map to find out more about business
organizations promoting early childhood policy in that
state.
Learn more about our National Network of business
organizations.
The States at a Glance Looking for data on your state that illustrates both the
status of children and the power of early investment? We recommend the following:
http://www.readynation.org/state-
network/

15
We’re in the “building
health and developmental
assurance” business…..
Physical health
Developmental health
Relational health
Key Drivers of EBCD
• Pediatricians carrying the urgent message
– Core Story of EBCD/ toxic stress
– “Building health for education readiness and our economic
future”
• Collaborative intentional partnerships with shared
vision at all levels – national, state and local
• Calling out Building Health in child health reform
• Calling for population health and outcome trajectory
data from health and EC investment
• Promoting innovation at the intersections of EC
communities and medical home
CONCLUSION:
It is easier to build strong children
than to repair broken men.
Frederick Douglass