Embed Size (px)
Citation preview

Potential New Dimensions in Dermatology...pg. 34
Forum For osteopathic thought
Official Publication of the American Academy of Osteopathy ®
tradition shapes the Future Volume 23 number 4 december 2013
JOURNALThe AAO

The American Academy of Osteopathy® is your voice . . ....in teaching, advocating, and researching the science, art and philosophy of osteopathic medicine, emphasizing the integration of osteopathic principles, practices and manipulative treatment in patient care.
• AccesstothemembersonlysectionoftheAAOwebsite,whichwillbeenhancedinthecomingmonthstoincludenewfeaturessuchasresourcelinks,ajobbank,andmuchmore.
• DiscountsonadvertisinginAAOpublications,ontheWebsiteandattheAAO’sConvocation.
• TheAmericanOsteopathicBoardofNeuromusculoskeletalMedicine,theonlycertifyingboardformanualmedicineinthemedicalworldtoday,accepts,withoutchallenge,allcoursessponsoredbytheAAO.
• MaintenanceofanearnedFellowshipprogramtorecognizeexcellenceinthepracticeofosteopathicmanipulativemedicine.
• Promotionofresearchontheefficacyofosteopathicmedicine.
• SupportforthefutureoftheprofessionthroughtheStudentAmericanAcademyofOsteopathyonosteopathicmedicalschoolcampuses.
• Yourprofessionalduesaredeductibleasabusinessexpense.
Ifyouhaveanyquestionsregardingmembershipormembershiprenewal,pleasecontactSusanLightleat(317)879-1881orslightle@academyofosteopathy.org.ThankyouforsupportingtheAmericanAcademyofOsteopathy.
TheAAOMembershipCommitteeinvitesyoutojointheAmericanAcademyofOsteopathyasa2013-2014member.TheAAOisyourprofessionalorganization.ItfostersthecoreprinciplesthatledyoutochoosetobecomeaDoctorofOsteopathy.
Forjust$5.01aweek(lessthanalargespecialtycoffeeatyourfavoritecoffeeshop)orjust71centsaday(lessthanabottleofwater),youcanbecomeamemberoftheprofessionalspecialtyorganizationdedicatedtothecoreprinciplesofyourprofession!
Yourmembershipduesprovideyouwith:• Anationaladvocateforosteopathicmanipulative
medicine(includingappropriatereimbursementforOMMservices)withosteopathicandallopathicprofessionals,publicpolicymakers,themediaandthepublic.
• ReferralsofpatientsthroughtheSearchforaPhysiciantoolontheAAOwebsite,aswellascallstotheAAOoffice.
• DiscountsonqualityeducationalprogramsprovidedbyAAOatitsannualconvocationandweekendworkshops.
• Newonlinecourses.• Networkingopportunitieswithyourpeers.• DiscountsonpublicationsintheAAOBookstore.• Freesubscriptiontothe AAO Journalpublished
electronicallyfourtimesannually.• FreesubscriptiontotheonlineAAO Member Newsletter.
Potential New Dimensions in Dermatology...pg. ???
Forum For osteopathic thought
Official Publication of the American Academy of Osteopathy ®
tradition shapes the Future Volume 23 number 4 december 2013
JOURNALThe AAO
About the artist for the September AAOJ cover:
JordanBlumerisa19-year-oldaspiringartist.ShegraduatedfromCorvallisHighSchool(Corvallis,OR)in2012withbuttwovisualartsclassesunderherbeltandhasyettoentercollege.Havinggrownupwithdoctorsasparents,shepullsmuchinspirationfromthemedicalfield.Aftertheyleftananatomytextbooklyingaroundoneday,shestoleitawayanddiscoveredanewpassioninanatomicaldrawing.Althoughherfavoritemediumiscompressedcharcoal,shehasexploredeverythingfromjewelry-makingandmetalworktocreatingherpromdressoutofducttape.
Cover photo by Dr. Kate McCaffrey, Ashland, Oregon, ©2013.

JThe AAO Forum for Osteopathic Thought
Official Publication of the American Academy of Osteopathy
TRADITION SHAPES THE FUTURE • VOLUME 23 NUMBER 4 • DECEMBER 2013
The mission of the American Academy of Osteopathy® is to teach, advocate and research the science, art and philosophy of osteopathic medicine, emphasizing the integration of osteopathic principles, practices and manipulative treatment in patient care.
OURNAL
Vol. 23, No. 4, December 2013 • The American Academy of Osteopathy Journal Page 3
3500DePauwBoulevard,Ste.1080Indianapolis,IN46268
Phone:(317)879-1881•Fax:(317)879-0563www.academyofosteopathy.org
American Academy of Osteopathy®
DavidCoffey,DO,FAAO. . . . . . . . . . . . . . . . . . . . . . . . .PresidentKennethJ.Lossing,DO. . . . . . . . . . . . . . . . . . . . .President-ElectDianaL.Finley,CMP. . . . . . . . . . . . . . . . . . . ExecutiveDirector
Editorial Advisory BoardDeniseK.Burns,DO,FAAOEricJ.Dolgin,DOClaireM.Galin,DOWilliamJ.Garrity,DOStephenI.Goldman,DO,FAAOStefanL.J.Hagopian,DO,FAAORaymondJ.Hruby,DO,MS,FAAOBrianE.Kaufman,DOHollisH.King,DO,PhD,FAAODavidC.Mason,DOKateMcCaffrey,DOPaulR.Rennie,DO,FAAOHallieJ.Robbins,DOMarkE.Rosen,DOKatherineA.Worden,DO,MS
The AAO JournalKateMcCaffrey,DO. . . . . . . . . . . . . . . . . . . . . . . ScientificEditorKatherineA.Worden,DO,MS. . . . . . . . . . . . . .AssociateEditorDianaL.Finley,CMP. . . . . . . . . . . . . . . . . . . .SupervisingEditorLaurenGood. . . . . . . . . . . . . . . . . . . . . . . . . . . . ManagingEditor
The AAO Journal is the official publication of the AmericanAcademyofOsteopathy.® IssuesarepublishedinMarch,June,SeptemberandDecembereachyear.
The AAO Journalisnotresponsibleforstatementsmadebyanycontributor.Althoughalladvertisingisexpectedtoconformtoethicalmedicalstandards,acceptancedoesnotimplyendorsementbythisjournal.
OpinionsexpressedinThe AAO JournalarethoseoftheauthorsanddonotnecessarilyreflectviewpointsoftheeditorsorofficialpolicyoftheAmericanAcademyofOsteopathy®ortheinstitutionswithwhichtheauthorsareaffiliated,unlessspecified.
Pleasesendemailaddresschangesto:[email protected].
AdvertisingratesforTheAAO Journal, officialpublicationoftheAmericanAcademyofOsteopathy®(AAO).AAOandAmericanOsteopathicAssociationaffiliateorganizationsandmembersoftheAcademyareentitledtoa20percentdiscountonadvertisinginthisjournal.CalltheAAOat(317)879-1881formoreinformation.Subscriptions:$60.00peryear.
2014 Advertising Rates
Placed1time Placed2times
Placed4times
FullPage7.5”x10” $600 $570 $540
HalfPage7.5”x5” $400 $380 $360
ThirdPage7.5”x3.3” $300 $285 $270
QuarterPage3.75”x5” $200 $190 $180
Classified $1.00perword
In this Issue:
AAOCalendarofEvents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
CMECertificationofHomeStudyForms. . . . . . . . . . . . . . . . . . 13
The AAOJ2013Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .38
ComponentSocietyCalendarofEvents. . . . . . . . . . . . . . . . . . 44
Editorials:
ViewfromthePyramids:ItTakesanOsteopathicVillage . . . . . 4Kate McCaffrey, DO
LookingBackandLookingAhead . . . . . . . . . . . . . . . . . . . . . . . .5Katherine A. Worden, DO, MS
Original Contribution:
ATaleofTwoSisters:AnOsteopathicStory. . . . . . . . . . . . . . . . .7Lawrence Uhrig, DO
TheEffectoftheStudentAmericanAcademyofOsteopathySummerPreceptorshipProgramonStudents’PerceptionofOsteopathicManipulativeTreatment . . . . . . . . . . . . . . . . . . . . . 14
Kathleen M. Vazzana, OMS IV; Vivian Chan, OMS II; Charles Wenzel, JD, OMS IV; and Sheldon C. Yao, DO
TheApplicationoftheCranialConceptintheInvestigationofBafflingMedicalDisordersandTheirTreatment:ASynergopathicMedicalDiseaseModel. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .20
Krishnahari S. Pribadi, MD
PotentialNewDimensionsinDermatology:TheOsteopathicApproachtoCutaneousDisease . . . . . . . . . . . . . . . . . . . . . . . . . .34
Ana M. Michunovich, BS, OMS III; and Robert Stern, MD
Case Study:
UseofOMTtoTreatPatientwithRamsayHuntSyndromeandHIV:ACaseStudy. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Joshua P. Baker, DO, FAAFP

Page 4 The American Academy of Osteopathy Journal • Vol. 23, No. 4, December 2013
View from the Pyramids
It Takes an Osteopathic VillageKate McCaffrey, DO
CME QUIZ
The purpose of the quiz, found on page 13, is to provide a convenient means of self-assessment for your reading of the scientific content in “Use of OMT to Treat Patient with Ramsay Hunt Syndrome and HIV: A Case Study” by Joshua P. Baker, DO, FAAFP.
Please answer each question listed. The correct answers will be published in the March 2014 issue of the AAOJ.
To apply for Category 2-B CME credit, record your answers to the AAOJ CME quiz application form answer sheet on page 13. The AAO will note that you submitted the form, and forward your results to the AOA Division of CME for documentation. You must score a 70 percent or higher on the quiz in order to receive CME credit.
DearColleagues,
IwouldliketowelcometoourAAO JournalournewAssociateEditor,KatherineA.Worden,DO.Dr.WordenisanassociateprofessorintheOMMDepartmentatAZCOMandisfromMichigan.Wearefortunatetohaveatalentedandsageosteopathicphysicianjoinoureditorialstaff.IwouldalsoliketoacknowledgethemanydedicatedAAOPublicationCommitteeMembersfortheireditorialassistanceandguidance.ThankyoutoDr.BrianKaufman,Dr.ClaireGalinandDr.RayHrubyforrecruitingauthorsandeditingnumerousarticles.Iwouldliketoaskyou,mycolleagues,topleasecontinueyoureffortstorecruitandreferbothexperiencedandnewwritersandresearcherstosubmittheirworktotheAAOJ—wecanmakethisjournalsuccessfulwitheveryone’shelp!This is your journal and this is our history—let’s create this story together!
ThisDecember2013AAOJisinterestingandthoughtprovoking.Itincludesatouchingarticleaboutthebenefitsofregularosteopathicmanipulationandcareovertwolifetimes.ThroughDr.Uhrig’sarticle,A Tale of Two Sisters: An Osteopathic Story,Iamremindedofthehealththatregularosteopathicmedicalcareprovidesourpatients.
Dr.Baker’scasestudyre-engagesusonadeeperlevelwithneuroanatomyandtheinterconnectednessbetweenOsteopathyintheCranialField,HIVandtheRamsayHuntSyndrome.Heconcludeswithproposingresearchonthistopiconalargerscale.
Welcometoourosteopathicmedicalstudentcontributers!PleasereadStudentDoctorsKathleenM.Vazzana,OMSIV;VivianChan,OMSII;CharlesWenzel,JD,OMSIV;andtheirAttending,Dr.SheldonC.Yao’s,analysisofasummerSAAOProgram’simpactontheperceptionofOMT.KudostoAnaM.Michunovich,BS,OMSIII,andhermentor,Dr.RobertStern,forthereminderofhowabalancednervoussystemaidsinoverallhealth,decreasestheallostericloadanditscoetaneousmanifestation.Welldonestudents!Keepresearching!
Inhisusualandengagingstyle,Dr.Pribadicontinuestochallengeourprofessiontoexpanditsvisionofosteopathyandwhereitfitsintoothermodalitiesanddiseasessuchas“leakygut”syndrome,foodintolerancesandEasternMedicine.
Andfinally,IwouldliketodrawyourattentiontothenumerousCMEopportunitiescomingyourwaythisyearandnextinthebeautifulstateofColoradoandbeyond!
Respectfully,
KateM.

Vol. 23, No. 4, December 2013 • The American Academy of Osteopathy Journal Page 5
Hello!
Thisfallhasbeenabusyosteopathicseason.IamhonoredtohavejoinedtheteamhereattheAAO JournalwithDr.McCaffrey,LaurenGoodandthePublicationsCommittee.IwouldliketothankDr.SeffingerforthenudgetovolunteerfortheAAO Journal,andIamexcitedaboutitsfuture!
Iwanttosharewithyouasnapshotofmylasttwomonths…andavision.ThispastSeptemberItraveledtomy25threunionfromMSUCOMinEastLansing,MI,whereitwasgreattovisitoldfriends,swapadventures,and,ofcourse,towatchtheSpartanswin!IthoughtitwashightimewepresentedvisceraltreatmenttoMichigandoctorsandpresentedaworkshoponthetreatmentforthe“MichiganNose”thatwaswellreceived.OurAZCOMOMMDepartmentJournalClubmettodiscussthenew10-yearStrategicPlanforOsteopathicResearch.Wealsodiscussedthemulti-sitestudyonCounterstraintenderpointfrequencyinosteopathicmedicalstudentsheadedbytheKirksvilleteam.Kudostoall!WegraduatedourfirstNMMPlusOneResidentfromournewprogram,GregHeller,DO,whowonhisdivisionoftheAAOResearchPosterContestatConvointheSpring.
InearlyOctoberEdnaM.Lay,DO,FAAO,FCA,andtheSCTFfacultyvisitedAZCOMandpresentedanIntermediateCranialCourse.ThiswasDr.Lay’sfinalteachingventure,andweweregratefultoherforallofherteachingsovertheyears.WealsoconvenedacommitteetodevelopanOCA-approved40-hourBasicCranialCourseoncampusforstudents.
Inmid-OctoberIfinallymademyvisitto“theMothership,”A.T.StillUniversityinKirksville,MO.BrianL.Degenhardt,DO,andhisteammettocontinuetobuildaOsteopathicPhysician–BasedResearchNetwork(PBRN)whichyoumayhaveheardofasDO-Touch.Net.Thisnetworkwillallowourresearcherstodevelopclinicalstudieswithlargernumbersofsubjectsbycombiningdatafrommultiplesites.Thisforwardthinkinginvolvesbuildinganinfrastructureinourprofessionfromwhichbetterresearchmaybeaccomplished.Ifyouorothersyouknowareinterestedinjoiningthisnetwork,[email protected].
Looking Back and Looking Ahead Katherine A. Worden, DO, MS
WhatfuntodrivedownOsteopathyStreetinKirksville,haveyourpicturetakenwiththeStatueofthe“OldDoc”onthetownsquare,seethepreservedlogcabinandfirstschoolofOsteopathy,andgazeuponthewallsoftheroominwhichweweremeetingtoseeapictureofayoungLouisaBurns,DO,andtheoriginalportraitofW.G.Sutherland,DO—yesthatone!Thehighlightofthetrip,however,wassittinginthebackroomofthelocalwateringhole,theWoodenNickel,onSaturdaynightbeingenthralledbystoriesoftheearlydaysofOsteopathytoldbyJason,thecuratoroftheMuseumofOsteopathy.Recentdiscoverieshaveledtonewmysteries,suchasWhat did A.T. have inside those boots all those years and why?
InNovemberIwasoneofmanyDOsrecruitedtohelpadministertheNMM/OMMBoardExamstoalargeclassof50+whoareseekingBoardCertification.
WhydoIshareallthiswithyou?SothatyoumaytakeheartthatOsteopathyisaliveandwellandgrowing…inourtreatmentrooms,onourcampuses,inourresidencies,andinourpresentandfutureresearchendeavors.Dowecontinuetohaveuniquechallengesinthecurrentmedicalclimate?Absolutely.ButweareproducingthelargestandperhapsthebrightestgenerationofDOswhowillhelpustofindcreativewaystomeetthosechallenges.Itisourjobasmentorstokeeptheminspiredandengagedingrowingtheirosteopathichandsandhearts.Itistimeforosteopathicphysicianstocreatesteppingstonesratherthanroadblocksforthisnextgenerationtolearnoftheirrichheritage,developtheirosteopathicskillsandleadusintothefuture.
ItistheAAO Journal’scollectivevisiontofillaneededvoidindevelopingnewwritersandresearchers.Wewouldliketocontinuetorecordosteopathichistoryasithappens.Eachissuestrivestobeasnapshotofcurrenteventsaffectingourprofession.IfyouhaveideasabouthowtomakethisJournalevenbetterortosubmitanarticle,feelfreetocontacttheAAO [email protected].
Thanksforlistening…
KateW.

Page 6 The American Academy of Osteopathy Journal • Vol. 23, No. 4, December 2013
AAO Calendar of Events
Mark your calendar for these upcoming Academy meetings and educational courses.All times local.
2014
January 1 FAAOApplicationsDue
January 29 COFAAOWebConference,8:30pm
TBD MembershipCommitteeTeleconference
February 1-2 BoardofTrustees’StrategicPlanningMeeting—AAOOffices,Indianapolis,IN
February 7-8 EducationCommitteeMeeting—1:00pm,AAOOffices,Indianapolis,IN
February 14-16 Basic Percussion Course—RichardW.Koss,DO—TCOM,FortWorth,TX
March 15-18 New Approach to Osteo-Articular Manipulations Including the Superior and Inferior Limbs(Pre-Convo),Jean-PierreBarral,DO(France);KennethJ.Lossing,DO—TheBroadmoor,ColoradoSprings,CO
March 17-18 Osteopathic Approach to Common ENT Complaints of Childhood (Pre-Convo)—HeatherP.Ferrill,DO,TheBroadmoor,ColoradoSprings,CO
March 17-18 Fascial Distortion Model(Pre-Convo)—ToddA.Capistrant,DO,TheBroadmoor, ColoradoSprings,CO
March 18 COFAAOMeeting—TheBroadmoor,ColoradoSprings,CO
March 19 BoardofTrusteesMeeting—8:00am,TheBroadmoor,ColoradoSprings,CO
March 19 BoardofGovernorsMeeting—1:00pm,TheBroadmoor,ColoradoSprings,CO
March 19-23 AAOConvocation—Trauma: An Integrated Osteopathic Approach DeniseK.Burns,DO,FAAO,ProgramChair—TheBroadmoor,ColoradoSprings,CO
February 14–16, 2014 at TCOMCourse Description and Background:At Dr. Fulford’s last course in May of 1997, he expressed his desire to leave his ailing body after his scheduled presentation to the Cranial Academy in June. After demonstrating what he was going to present to the Cranial Academy, he asked Dr. Koss (Program Chair) and Dr. Rajiv L. Yadava to continue teaching his work to the Osteopathic profession. Dr. Fulford passed away four days after the Cranial Academy presentation.
This course has been restructured to provide the participant a more complete understanding and experience of Dr. Fulford’s contributions to Osteopathy. Although hand and percussion techniques are included, the course emphasizes increasing the clarity of one’s working knowledge. Based on the participant’s inclinations, there is freedom within the curriculum to change the direction of what information is relayed. Time needed to assimilate what is taught will also be respected.
Prerequisites:This Level III course is for DOs, MDs, dentists and students with a 40-hour approved Cranial course and/or prior training and experience
in Cranial Osteopathy or permission from the program chair.
Course Objectives:• One will recognize that many of Dr. Fulford’s
ideas are rooted in Dr. Still’s and Dr. Sutherland’s teachings;
• One will begin to see that the results realized from the use of the percussor is directly dependent on the osteopath’s understanding;
• One will see that the use of the percussor will save the physician time and energy; and
• One will appreciate that Dr. Fulford gave more to Osteopathy than a new technique.
CME:22 hours of AOA Category 1-A credit is anticipated
Course Location:Texas College of Osteopathic Medicine3500 Camp Bowie Blvd.Fort Worth, TX 76107(817) 735-2000
Richard W. Koss, DO
Robert C. Fulford, DO
Dr. Robert C. Fulford’s Basic Percussion Course
Click here to register
online.

Vol. 23, No. 4, December 2013 • The American Academy of Osteopathy Journal Page 7
A Tale of Two Sisters: An Osteopathic Story Lawrence M. Uhrig, DO
Hereisaniceanecdotalstoryoftwosisterswhohavewalkedthisearthfornearlytwocenturiesbetweenthetwoofthem.Dorothyhasbeenapatientinmypracticeforover55years,gettingregularosteopathictreatmentsand,rarely,medicaltreatmentforminorillnesses.Ihavetreatedherforthe23yearsthatIhavebeeninthisofficewithmytraditionalosteopathicpractice.IhavetreatedDorothywiththoroughosteopathicmanipulationonamonthlybasisformyentirecareer.
Dorothyisanelegant95-year-oldwomanwhoisveryactivewithchurchactivities,shopping,socializingandgoingouttoeatwithfriendsalmostdaily.Shewalksfullyupright,hasveryfewcomplaintsaboutarthritis,backachesorinternalproblemsbutdoescarryacaneincasesheneedsitinherdailyactivity.ShehasbeentreatedintheofficewhereIcurrentlyworksincethelate1950swhenHerbertC.Miller,DO,FCA,andWilliamRankin,Sr.,DO,workedhere.WilliamRankin,Jr.,DO,treatedherfollowinghisfather’sdeathin1965,andIstartedtreatingDorothyin1990whenIjoinedDr.Rankin,Jr.’s,practice.Dorothyisamodelpatient,neverforgettingherappointments,stilldrivingandlivingbyherself,alwaysverypleasanttotreatandthankfulforwhatOsteopathyhasdoneforherovertheyears.Shehasenjoyedatremendouslyhealthylifewithonlyrecentperiodicheartirregularityandanepisodeofshingles.Littleelsehasevertroubledher.
Dorothy’soldersister,Violet,is97yearsoldandalsoisaverypleasantwomantochatwithandvisit.
Violethasneverbeentreatedinourofficeand,otherthansomeregularfluvaccinations,hasneverbeentreatedbymeforanymedicalissues.Sheseesanotherprimarycarephysiciantohelpherdealwithanumberofmedicalandmusculoskeletalissues.Violethas,therefore,neverreceivedosteopathiccareduringhernearcenturyonearth.
OtherthanoccasionalvisitstochurchonSunday,Violetrarelyleavesherhouse.Shesitsinareclinermostofthedayandusesawalkertoambulatewhatlittlesheisableto.Shehasatypicalstoopedosteoporoticposturewithambulation.Sheisnotabletowalkfarorcarrymuchweightduetoherweakness,spinalcompressionandosteoarthritisrestrictions.
So,wehaveananecdotalcomparisonoftwosisterswhohavereceiveddifferentapproachestotheirhealthcareduringtheirlives.WeknowthatOsteopathywasfoundedontheprinciplesofA.T.Stilltomaintainhealthasmuchaspossiblebyworkingtoimprovecirculationandoptimizemobilityasclosetonormalaspossible.Certainlygeneticandenvironmentalforcescaninfluencehealthinmanywaysbutitisawonderfulconsiderationthat,atleastinDorothy’scase,Osteopathyhasprobablyallowedhertoenjoybetterhealthandmobilityandmaximizeherabilitytogetthemostoutofwhatlifehashadtooffer.DorothyandVioletarebothwonderfulpeopletoknow,andhopefully,bothhavemorehealthyyearsahead.
Thankyou,Dr.Still!
Above: Dorothy in the office. Right: Dorothy and Violet.

Page 8 The American Academy of Osteopathy Journal • Vol. 23, No. 4, December 2013
Figure 171. Pterygopalatine ganglion.Putz, Pabst: Atlas of Human Anatomy ©Elsevier GmbH, Urban & Fischer, Munich.
Abstract
A31-year-oldmalepresentswithaskinrashonafewlocationsonhisleftearandleftforehead.Apresumptivediagnosisofimpetigoismadeandtreatmentisinitiated.Severaldayslater,thesamepatientreturnswithfacialparalysisonthesideoftheskinlesions.AdiagnosisofRamsayHuntsyndromeismadeandthenconfirmedthroughtissuepathologicanalysisandPCRanalysis.RamsayHuntsyndrome,thereactivationofherpeszosterviruswithinthegeniculateganglionofthefacialnerve,presentswithavarietyoffacialnervepathologiesincludingskinrashandfacialparalysisasitdidinthiscase.Itcanpresentwithavarietyofothercranialnerveneuropathicpresentations,asitdidinthiscaseaswell.Adjuvanttreatmentwithosteopathicmanipulativetreatment(OMT)wasinitiatedattheonsetofthefacialpalsy.HIVpatientswithRamsayHuntsyndromehaveshowedtohaveapropensitytomoresevereneurologicsymptomsandcomplications.Inthiscase,thepatientresultedincompleteresolutionofallhissymptoms.
Use of OMT to Treat Patient with Ramsay Hunt Syndrome and HIV: A Case StudyJoshua P. Baker, DO, FAAFP
Presentation of a Case
A31-year-oldCaucasianmalepresentedFebruary2013ondaytwoofarashonhisleftforeheadandleftearthatbegansimultaneously.Bothlesionsappearedasscab-like,theearlesionasmildlypruriticinhisearcanalwitherythemaaroundthelesion,whiletheforeheadlesionwasasymptomatic.Thepatientdeniedburning,stinging,bleeding,pain,vertigo,dizziness,weakness,headache,fevers,chills,sweats,hearingloss,tinnitusandfacialparesthesias.Hefeltcompletelynormalexceptforthisnewrash.Healsopresentedondaytwoofasorethroatwithmildodynophagia,whichhestatedwascomparabletowhenhehadpreviouslybeendiagnosedwiththrush.Hisphysicalexamwasunremarkablewiththeexceptionofthethreebelowregions:
1. Leftforehead:scabbedoverpapule3mmx3mmwithtendernesstopalpation.Nofluctuance,surroundingredness,honey-crustedscale,discharge,hyperesthesia,purulence,vesicles.
2. LeftEar:tender,fluid-filled2mmx2mmpustuleonantihelixwithassociatedhoney-crustedplaqueinvolvingantihelixaroundthepustule
approximately1cmx1cmwithearrednessinthisregion.Thescalealsospreadfromtheantihelixtotheconchaandintothelateralone-fourthofthesuperioraspectoftheearcanal.Wherethecrustinghadbeenremovedintheearcanal(duetopruritus),therewasunderlyingerythema.Noinduration,fluctuance,warmth,edema,clearfluidfilledvesicles,hyperesthesia,

Vol. 23, No. 4, December 2013 • The American Academy of Osteopathy Journal Page 9
bleeding,discharge,tympanicmembraneabnormalities.
3. ENT:diffusebilateralpharyngealerythemawithscatteredwhiteplaques.
Thepatient’smedicalhistoryincludedadiagnosisofhumanimmunodeficiencyvirus(HIV)madeAugust2012withinitiationofhighlyactiveantiretroviraltreatment(HAART)atthattime.HispresentingillnessAugust2012wasanAIDS-definingillness:pneumocystisjirovecipneumonia.Theremainderofhismedical,surgical,allergy,alcohol,tobaccoandsocialhistorywasunremarkable.
ThepatientreportedthathismostrecentCD4countwasnormal.(Thoserecordsareunavailabletotheauthor.)CurrentmedicationsincludedReyataz(atazanavir)300mgPOoncedaily,Truvada(emtricitabine/temofovirdisproxil)200mg/300mgPOoncedaily,andBactrimDS(trimethoprim/sulfamethoxazole)160/800POoncedaily.
Theinitialshortlistassessmentofthisskinrashincludedimpetigo,varicella-zostervirus(VZV)andherpessimplexvirus(HSV).Thepharyngealabnormalitywasconsistentwithoropharyngealcandidiasisandlesslikelyesophagealcandidiasis.Theseskinlesionswerehighlyconsistentwithimpetigo.HelackedmultiplesymptomsthatareusuallypresentinVZVorHSV,namelyparesthesias,tingling,hyperesthesias,pain,burning,stingingandclearfluidfilledvesicles.Othermoreseveresymptomsmayhaveincludedfacialnervepalsy,tinnitus,hearingloss,vertigo,dizziness,conjunctivitis,photophobia,visionchanges,eyepainandothereyesymptoms.Additionally,thelocationofthelesiononhisforeheadwasinthedistributionofophthalmicdivisionofthetrigeminalnerve(V1),andtheearlesionwasonthemandibulardivisionofthetrigeminalnerve(V3)andpossiblymayhaveinvolvedthefacialnerve(CNVII)attheearcanal.ThiswouldmakeHSVunlikelyandwouldmakeVZVmultidermatomalinnature;whichisuncommon.
Thetreatmentplanincludedthefollowing:fluconazole(Diflucan)100mgPOoncedailyfor30days(firstdoseof200mgfollowedby100mgonsubsequentdays);Nystatin100,000units/mLsuspension5mlrinseandswallowfourtimesperdayfor10days;mupirocintopical(Bactoban)2%ointmentappliedtopicallytoaffectedareasthreetimesdailyfor14days.
Ondaynineoftheillness,thepatientreturnedtotheofficebecausehenoticedatwo-dayprogressivelyworseningleftfacialparalysiswhichincludedthe
inabilitytoclosetheeye,puffouthischeeks,smileandfrown.Thepharyngealpainhadcompletelyresolved.Theforeheadlesionwasstillscabbedoverandasymptomatic.Theearlesionhadresolutionoftheredness,resolutionofpruritus,significantdecreaseofscaling/crusting,andhewasotherwisefeelingwell.Hisreviewofsystemswasnegativeforvisionproblems,eyepain,redeye,photophobia,eyesymptomsofanykind,vertigo,tinnitus,dizziness,earpain,eardrainage,palatepain,tongueparesthesias,tasteproblems,facialparesthesias,headache,fevers,chills,andsweats.Hewasfeelingcompletelynormaldespitethisnewonsetfacialnerveparalysis.
ApresumptivediagnosisofRamsayHuntsyndrome(reactivationofvaricella-zosterviruswithinthegeniculateganglionoftheseventhcranialnerve)wasmade.EvaluationincludedlesionalswaboftheforeheadandearlesionsforHSVandVZV,moleculardetection,polymerasechainreaction(PCR),dermal,andcompleteexcisionoftheleftforeheadlesionsentforpathologicanalysis.Hisnewtreatmentincludedacyclovir(Zovirax)800mgPOfivetimesdailyforsevendays;Prednisone9-daytaper(50mgPOoncedailyforfivedays,40mgx1day,30mgx1day,20mgx1day,10mgx1day);Systanebrandophthalmiclubricantduetoinabilitytoclosehiseyelidcompletely;initiationofosteopathicmanipulativetreatment(OMT)anddiscontinuationoftopicalmupirocin(Bactroban).AdetaileddescriptionofsomaticdysfunctionsandOMTprovidedwillbeaddressedinthediscussionsectionofthisarticletofollow.
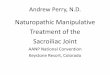
Figure 1181. Facial nerve VII; the facial canal and tympanic cavity have been opened; viewed from the right. Clinical term: cerebellopontine angle.Putz, Pabst: Atlas of Human Anatomy ©Elsevier GmbH, Urban & Fischer, Munich.

Page 10 The American Academy of Osteopathy Journal • Vol. 23, No. 4, December 2013
Onday11,theHSVandVZV,moleculardetection,PCR,dermaltestresultedinthedetectionofvaricella-zostervirusDNA.
Byday17(postoperativedayeight),thewoundonthepatient’sforeheadwaswellhealed,andsutureswereremoved.Theskinlesiononhisearwascompletelyresolved.Heneverusedtheophthalmiclubricant,ashewasabletofullyclosehiseyeinamatterofdaysafterhewasseenondaynineoftheillness.Hereportedhewasunabletonoticehisfacialpalsy.Hisphysicalexamwasconsistentwithanormalappearingforeheadandear.Hisfacialpalsywasnearlyresolvedbutstillperceptibletoadetailedexam.OMTwasperformed.
Onday18,thepathologyreportontheforeheadlesionrevealedabenignulcerwithnoevidenceofherpesviruscytopathiceffectseen,namelyviralinclusions.
Onday24,arecheckintheofficewasperformed,andhewasunabletoperceivethefacialpalsy.Uponexamduringhisnormalconversation,thepalsywasimperceptible.Detailedexaminationrevealedamildlyperceptiblefacialasymmetrywhenhesmiled,frownedandfurrowedhiseyebrowswithmaximalintensity.OMTwasperformed.
Onday31,arecheckintheofficerevealedacompleteresolutionofanyfacialasymmetryondetailedexam.OMTwasperformed.
Recheckswereagainperformedondays38and45toperformOMT.Onday45,resolutionofhiskeylesionwasnotedpriortoinitiationofOMT.Atthatpoint,nofurtherevaluationortreatmentwasrecommended.Atday45,hissymptomswerecompletelyresolved,hiskeysomaticdysfunctionwasnolongerpresent,andnofurtherfollowupwasrecommendedforthisproblem.
Clinical Discussion: Ramsay Hunt Syndrome
RamsayHuntsyndrome(RHS)isreactivationoftheherpeszostervirusoriginatingfromthegeniculatenucleusofthefacialnerve(CNVIII)thatislocatedwithinthefacialcanalwithinthetemporalbone.1
Typically,RHSpresentswithunilateralfacialparalysis,neuropathicpainanderuptionofherpeticvesicleswithinthedistributionofthesensoryinnervationsfromtheafferentfacialnervefibers.Othertypicalpresentationsincludetinnitus,vertigoandhearinglossduetothejuxtapositionofcranialnervesVIIandVIIIinthefacialcanal.Multiple,lesstypicalmanifestationsincludevariousneuropathiesofthefollowingnervespresentedindecreasingfrequency:vestibulocochlearnerve(CNVIII),glossopharyngealnerve(CNIX),trigeminalnerve(CNV),vagusnerve(CNX)andabducensnerve(CNVI).Additionally,thepresentationofRHSinpatientswithHIVisknownforitsmoresevereneurologicpathologyandisalsofoundtoresultingreaterneuropathicsequelae.1,2,3,4
brings to light a rich tradition of excellence in education and leadership. Currently, the Georgia Campus—Philadelphia College of Osteopathic Medicine, in the greater Atlanta area, has the following exciting positions available:
Full time faculty position in the Department of Osteopathic Manipulative Medicine. This individual will be expected to teach osteopathic medical students in both lecture and laboratory sessions in all four years of the curriculum, see patients and develop an outpatient clinic for M-3 month long rotation, plan and supervise OMM Inpatient Student Service, assist in preparation of OMM video clips and tutorials, participate in existing research and initiate new OMM research, assist in planning and production of new publications, and assist in planning and supervision of the OMM Residency. The successful applicant will have a D.O. degree and proficiency in osteopathic manipulative medicine. The candidate needs to have or be eligible for a license to practice Osteopathic Medicine in the State of Georgia. Board Certification or eligibility by the AOBNMM or AOBSPOMM is required. Additional Board Certification or eligibility by the AOBFM is desirable. The review of applications will begin immediately and continue until the position is filled. Salary for this position will be commensurate with experience and qualifications.
Seeking qualified Osteopathic Physician for a full-time Clinical Education Coordinator. This full time position reports to the Chair of Undergraduate Clinical Education. This individual will be responsible as the Director of the Advanced Clinical Skills Program. He/She will supervise the Clinical Adjunct Faculty’s participation in the didactic educational programs and assist the Chair in management of the Clinical Clerkship program. Minimum of five years in a clinical practice. Experience in clinical education as a Clerkship Director, Program Director, Didactic Educator, or similar activities. Must be Board Certified in a Primary Care specialty.
To apply for these positions, send via E-mail a personal statement describing interest in and qualifications for this position, a curriculum vitae, and names and addresses of three references, preferably from current or former supervisors.
All inquiries must include salary requirements and should be directed to:EOE
WWW.PCOM.EDU

Vol. 23, No. 4, December 2013 • The American Academy of Osteopathy Journal Page 11
InformationregardingRamsayHuntsyndromeinpatientswithHIVislimited.Theauthorlocatedatotalofeightothercasesintheliteraturethatreportedavarietyofsigns/symptomsaswellasvariedfinaloutcomes.Thereisonlyoneothercasereporttodateofapatientrecoveringwithcompleteresolutionandwithoutsequelae.5
ThestandardtreatmentforRamsayHuntsyndromeisearlyinitiationofsystemicantiviralsthataretypicallyusedforvaricella-zostervirussuchasacyclovir(Zovirax)inadditiontotheuseofsystemiccorticosteroids(suchasprednisone)inavarietyofdosingschedules.6,7
ThereisalackofrecommendationsforthetreatmentofafacialnervepalsyfromRHS,butthereareothertreatmentoptionsforidiopathicfacialnervepalsythatincludethefollowing:acupuncture,physicaltherapy,occupationaltherapy,biofeedback,osteopathicmanipulativetreatmentandneuromuscularre-education.Surgicalintervention,intheformofdecompression,isnotrecommendedinRHSduetothetypicalpresenceof“skip”regionsanddiffusesneuritisofthefacialnerve.8,9,10,11,12
Thepatientinthiscasestudyhadsigns/symptomsthatinvolvedmultiplenervedistributions
• Facialnerve(CNVII)
» skinlesionsintheearcanal
» facialpalsy
• Mandibulardivisionoftrigeminalnerve(V3)
» skinlesionsontheearantihelixandconcha
• OphthalmicdivisionoftrigeminalverveV(V1)
» skinlesionontheforehead
Thispatientreceiveddelayedinitiationofantiviralandsystemiccorticosteroidadministrationduetotheatypicalpresentationbutdidreceivethemnonetheless.Asidefromthedelayedinitiationofthosemedications,nodeviationfromstandardcarewasidentified.
Clinical Discussion: Use of OMT in Ramsay Hunt Syndrome
AdjuvanttherapywithOMTwasutilizedinthiscasestudy.Thispatientdemonstratedrepeatedipsilateraltemporalbonedysfunctions,whichwerethekeylesions.Therewasnopatterntothespecificdysfunction.Occasionally,itwasfoundinternallyrotatedandatothertimesitwasexternallyrotated.Therewasnomorespecificpatternnotedthantherepeatedipsilateraltemporalbonedysfunctionitself.
Intotal,hereceivedOMTonsixoccasions,days9,17,24,31,38and45oftheillness.
OMTwasperformedonmultiplebodyregionsduringeachtreatmentsession,utilizingmultipletreatmentmodalities,withafocusofOsteopathyintheCranialFieldmainlyontheheadandsacrum.Aspreviouslymentioned,theipsilateraltemporal
Figure 1411. Inner ear with the facial nerve and the vestibulocochlear nerve; projected onto the petrous part of the temporal bone; superior view. Putz, Pabst: Atlas of Human Anatomy ©Elsevier GmbH, Urban & Fischer, Munich.

Page 12 The American Academy of Osteopathy Journal • Vol. 23, No. 4, December 2013
bonedysfunctionappearedtobethekeylesionthroughoutthishealingprocess.Comparedtotheotherdysfunctionspresentineachtreatmentsession,thetemporalbonedysfunctionsweremoresevereandrequiredmoretimetotreatuntilresolution.Thesedifficultdysfunctionsalwaysrespondedtotreatmentduringeachtreatmentsession.Directandindirecttreatmentmodalities(withapersonalpreferencetowardindirectbytheprovider)wereutilized.Therewasnopatternnotedaboutwhattypesoftreatmentsweremoreeffective.Onsomeoccasions,directtreatmentsweremosteffectivewhileatothertimes,indirecttreatmentswereeffective.Onsomeoccasions,bothtypesoftreatmentswereneeded.
Uponreviewofthemedicalliterature,therearenocasereportsinvolvingtheuseofOMTforafacialnervepalsyinducedbyRamsayHuntsyndrome.ThereareotherpublicationsregardingtheuseofOMTinotherknowncausesaswellasinidiopathicfacialnervepalsy.Twoofthesepublicationsnoteipsilateraltemporalbonedysfunctionsbeingprevalent,similartothiscasereport.Oneotherpublicationnotestheabsenceofthisfindingaltogether.13,14,15
Conclusions
RHSmaypresentinavarietyofways,especiallyinHIV,thusrequiringtheosteopathicphysicianunderstandthecranialnerves’structureand
functions.Thiswillthenenablecorrectrecognitionofneuropathies.TheadditionofOMTasadjuvanttreatmentforRHSisbasedupontheprincipalsofosteopathicmedicine.Inparticular,OsteopathyintheCranialFieldhaspotentialforabeneficialoutcomeinpatientswhopresentinthismanner.Treatmentofthepatient’scranialdysfunctionscanassistinthenormalizationofsomaticcomplaints.
Thepatientinthisstudyhadamagnificentendresultwithcompleteresolutionofallhissymptomsfollowingallthetreatments;howeveritisnotscientifictoclaimthatOMTwasthereasonhehadsuchanastoundingoutcome.Thiscaseexemplifiesoneapproachandcouldprovideaframeworkforfurtherstudyinthehopesthatovertimepatternsandconsistenciesthatcanhelpguideosteopathicphysicianscanbeestablished.
Acknowledgements:TheauthorwouldliketoacknowledgeTonyNguyen,MLIS,forhisexpertiseinliteraturesearch.
References1. Chapter7.CranialnerveVII.In:JonesHR,SrinivasanJ,Allam
GJ,BakerRA,eds.Netter’s Neurology.2nded.Philadelphia,PA:Saunders-Elsevier;2012:98-108.www.ClinicalKey.com.Accessed09-17-2013.
2. GilchristJM.SeventhCranialNeuropathy.Seminars in Neurology.2009;29(1):5-13.
3. GlesbyMJ,MooreRD,ChaissonRE.Clinicalspectrumofherpeszosterinadultsinfectedwithhumanimmunodeficiencyvirus.Clinical Infectious Diseases.1995;21:370-375.
4. MeenstraJ,vanPraagR,KrolA,vanDillenP,WeigelHM,SchellekensP,LangeJ,CoutinhoR,vanderMeerJ.ComplicationsofvaricellazosterreactivationinHIV-infectedhomosexualmen.AIDS.1996;10:393-399.
5. GoldaniLZ,FerreiradeSilvaLF,DoraJM.RamsayHuntsyndromeinpatientsinfectedwithhumanimmunodeficiencyvirus.Clinical and Experimental Dermatology.2009;34:e552-e554
6. UscateguiT,DoreeC,ChamberlainIJ,BurtonMJ.CorticosteroidsasadjuvanttoantiviraltreatmentinRamsayHuntsyndrome(herpeszosteroticuswithfacialpalsy)inadults.Cochrane Database of Systematic Reviews.2008;3:CDC006852.
7. UscateguiT,DoreeC,ChamberlainIJ,BurtonMJ.AntiviraltherapyforRamsayHuntsyndrome(herpeszosteroticuswithfacialpalsy)inadults.Cochrane Database of Systematic Reviews.2008;4:CDC006851.pub2.
8. ManikandanN.Effectoffacialneuromuscularre-educationonfacialsymmetryinpatientswithBell’spalsy:arandomizedcontrolledtrial.Clinical Rehabilitation.2007;21:338-343.
9. ShafshakTS,Thetreatmentoffacialpalsyfromthepointofviewofphysicalandrehabilitationmedicine.Europa Medicophysica.2006;42(1):41-47.
Figure 1429. Facial nerve within the petrous part of the temporal bone; the petrous part of the temporal bone, as well as the facial canal and the tympanic cavity, have been partially opened; posterior view. Putz, Pabst: Atlas of Human Anatomy ©Elsevier GmbH, Urban & Fischer, Munich.
continued on page 17

Vol. 23, No. 4, December 2013 • The American Academy of Osteopathy Journal Page 13
September2013AAO Journal CMEquizanswers:
1. E2. A3. C4. C
AnswerstotheDecember2013AAOJCMEquizwillappearintheMarch2014issue.
CMECERTIFICATIONOFHOMESTUDYFORMThisistocertifythatI,___________________________ Pleaseprintname
READthefollowingarticleforAOACMEcredits.
Name of Article:UseofOMTtoTreatPatientwithRamsayHuntSyndromeandHIV:ACaseStudy
Authors: JoshuaP.Baker,DO,FAAFP
Publication: AAOJ,Volume23,No.4,Dec.2013,pp.8-12
Mailthispageto:AmericanAcademyofOsteopathy3500DePauwBlvd.Suite1080Indianapolis,IN46268
Category2-Bcreditmaybegrantedforthesearticles.00____________ AOANumberFullname:______________________________________ (Pleaseprint)
Streetaddress:___________________________________
City,state,zip:__________________________________
Signature:______________________________________
FOROFFICEUSEONLYCategory:2-B Credits:_________Date:____________
American Osteopathic Association Continuing Medical Education
ThisCMECertificationofHomeStudyFormisintendedtodocumentindividualreviewofarticlesintheAmerican Academy of Osteopathy JournalunderthecriteriadescribedforCategory2-BCMEcredit.
Completethequiztotherightbycirclingthecorrectanswer.MailyourcompletedanswersheettotheAAO.TheAAOwillforwardyourresultstotheAOA.Youmusthave70percentaccuracyinordertoreceiveCMEcredits.
1. RamsayHuntsyndromeisareactivationoftheherpeszosterviruswithinwhichnervebody?a. Geniculateganglionofthefacialnerve(cranial
nerveVII)b. Trigeminalganglionofthetrigeminalnerve
(cranialnerveV)c. C2Dorsalrootgangliond. Pterygopalatineganglion(alsoknownas
sphenopalatineganglion)ofthefacialnerve(cranialnerveVII)
2. RamsayHuntsyndromemaypresentwiththefollowingsymptomsexcept:a. Unilateralfacialmuscleparalysisb. Vesicularrashintheearcanalc. Vertigoandhearinglossd. Anosmia
3. WhichOsteopathicmanipulativetreatmentswouldbereasonabletoapplyonapatientwithRamsayHuntsyndromeandaunilateralfacialmuscleparalysiswhoalsopresentedwithanipsilateralinternallyrotatedtemporalbone?a. Directtreatmentaugmentingexternalrotation
ofthedysfunctionaltemporalboneb. Indirecttreatmentaugmentinginternal
rotationofthedysfunctionaltemporalbonec. Venoussinusdrainaged. Alloftheabove
4. PermanentneurologicsequalaeiscommoninRamsayHuntsyndrome.a. Trueb. False

Page 14 The American Academy of Osteopathy Journal • Vol. 23, No. 4, December 2013
The Effect of the Student American Academy of Osteopathy Summer Preceptorship Program on Students’ Perception of Osteopathic Manipulative Treatment
Kathleen M. Vazzana, OMS IV; Vivian Chan, OMS II; Charles H. Wenzel, JD, OMS IV;and Sheldon C. Yao, DO
Abstract
Context:Tomaintaintheidentityoftheosteopathiccommunity,itiscrucialtohaveprogramsthatencourageosteopathicmedicalstudentstoutilizeOMT.TheStudentAmericanAcademyofOsteopathy(SAAO)SummerPreceptorshipProgramisauniqueprogramthatfocusesongivingclinicalOMTexposuretosecond-yearstudents.
Objective:TodetermineifparticipationintheSAAOSummerPreceptorshipProgramaffectedstudents’perceptionsofOMTandlikelihoodofintegrationofOMTintostudents’futuremedicalpractice.
Design:Survey
Setting: NewYorkInstituteofTechnologyCollegeofOsteopathicMedicine(NYIT-COM)
Participants:Second-yearosteopathicmedicalstudents
Main Outcome Measure:WemeasuredtheinterpretationsofOMTusingLikertscalesreportedbytheparticipants.
Method: Fiftyparticipantswereadministeredapapersurveycontaining12multiple-choiceandfiveopen-endedquestionsregardingtheirperceptionsofOMTandexperienceswiththeprogram.
Results: Thirtystudentscompletedthesurvey.Twenty-ninestudentshadanimprovedconfidencelevelandunderstandingoftheclinicalapplicationwithusingOMT;onewasundecided.Twenty-ninestudentsweremorelikelytointegrateOMTintotheirfuturepractice;onewasundecided.Twenty-sevenstudentshadanexpandedawarenessofwhatconditionscanbetreatedwithOMT;threewereundecided.Twenty-ninestudentshadanoverallpositiveperceptionofOMT;onewasundecided.
Conclusions:TheSAAOSummerPreceptorshipProgramhadapositiveeffectonstudents’perceptionofOMTandlikelihoodofintegrationofOMTintotheir
futuremedicalpractice.Follow-upstudyiswarrantedtodetermineactualeffectsonfutureutilizationofOMTinclinicalpractice.
IRB: ApprovedbyNYITIRB.IRB#BHS970.(8/20/2013)
Introduction
Inmedicaleducation,thecurrentliteraturehasdeterminedthepositiveinfluenceofclinicalexperienceandrolemodelsonmedicalstudents’attitudestowardhealthprofessionsandcertaincareerspecialties.1-5AttheMayoMedicalSchool,exposuretoanoptionalweek-longpediatricsexperienceledtoanincreaseininterestandknowledgeinthefieldofpediatricsamongitsfirst-andsecond-yearmedicalstudents.Greaterthan25percentoftheschool’sfirst-andsecond-yearmedicalstudentsparticipatedinthisselectiveexperience,consistingofworkshopsandfacultyandresidentpaneldiscussions.6Otherstudieshavesimilarlydemonstratedthatexposingstudentstoparticularspecialtiesintheirpre-clinicalyearsincreasestheirpredilectiontowardschoosingthatspecialty.7,8
Practicingosteopathicmanipulativetreatment(OMT)ispartoftheuniqueidentityofdoctorsofosteopathicmedicine.However,ithasbeenutilizedlessfrequentlybyrecentosteopathicmedicalgraduates.9,10ChamberlainandYatesfoundthatpriortoenteringrotations,over70percentofsecond-yearosteopathicmedicalstudentsdecidedthattheywouldnotutilizeOMT.Withinthesamestudentpopulationupongraduation,thepercentageofstudentsthatweredisinclinedtowardOMTuseroseto90percent.11
Tomaintaintheidentityoftheosteopathiccommunity,itiscrucialtohaveprogramsthatencourageosteopathicmedicalstudentstoutilizeOMT.Teng,AK,etal.foundthattheadditionofamandatorythird-yearandfourth-yearclinicalosteopathicmanipulativetreatment(OMT)exposureledtoanimprovementinthestudents’reportedcomfortlevelwithOMT;however,students’overallattitudetoward

Vol. 23, No. 4, December 2013 • The American Academy of Osteopathy Journal Page 15
OMTusewasnotexamined.12TheeffectofprovidingOMTclinicalexperiencesduringthepre-clinicalmedicaleducationyearsmeritsfurtherstudy.
TheStudentAmericanAcademyofOsteopathy(SAAO)SummerPreceptorshipProgramisauniqueprogramofferedbyNYITCollegeofOsteopathicMedicine(NYIT-COM).ThisprogramprovidesOMTworkshopsandclinicalsessionstoincomingsecond-yearstudents.Thisstudyassessestheeffectivenessofthe2013SAAOSummerPreceptorshipProgramoninfluencingstudents’attitudesandprospectiveuseofOMT.
Description of SAAO Summer Preceptorship Program
Thisyear’sSAAOSummerPreceptorshipProgramranfromJune10toJuly26,2013.Fifty-tworisingsecond-yearmedicalstudentsparticipatedintheprogram;50studentscompletedtheprogram.Tocompletetheprogram,studentswererequiredtoattendatleast10outof14workshopsandcompletetwoshadowingsessionsofosteopathicphysiciansattheAcademicHealthCareCenteratNYIT-COM.The14workshopsincludedtopicsrangingfromcase-basedpresentationsutilizingOMTtoalternativemedicines.Mostworkshopsranforonehour,weretaughtbyosteopathicphysicians,andincludedtimeforstudentstopracticedemonstratedtechniquesononeanother.
Date Workshop Description
June10 IntroductiontotheProgramandBalancedLigamentousTension(BLT)workshop. Students were oriented to professionalism, HIPAA, and observation of OMT in the health center. Students then practiced BLT for the transverse carpal ligament, interosseous membrane, and rib cage after discussion of clinical cases in which they would be used (i.e., carpal tunnel syndrome and asthma).
June11 OsteopathicClinicalConsiderationsinTreatingIrritatedBowelSyndrome(IBS):Presentation on the nervous system’s role in IBS. Students practiced the following techniques: indirect myofascial on the thoracolumbar, sacroiliac articulation technique and sacral rocking, abdominal mesenteric lift, and suboccipital release.
June12 AlternativeApproachestoPatientEducation:Articles on alternative treatments were provided and discussed. Students practiced the Jacobson’s Muscle Relaxation Technique.
June18 TheStillTechnique:The Still Techniques for the first rib, cervical spine, and thoracic spine were demonstrated and practiced. Clinical correlations for treatment of these areas were discussed.
June24 Acupuncture:The origins and principles of acupuncture were presented. After the physician spoke about his own training and patients’ successes, he guided the students in how to use an acupuncture needle to alleviate their partners’ tense muscle.
June25 PainfromStudyingandtheEffectsofStressonVisceralOrgans:With guidance, students practiced the following stress-relieving techniques: condylar decompression, FPR on the trapezius and the first rib, thoracic outlet release.
July9 TaiChi:A Tai Chi instructor for NYIT’s Parkinson’s program led an outdoor Tai Chi session.
Date Workshop Description
July10 OMTinRotationsandPreparingforBoards:Academic scholars at NYIT-COM led small group sessions, sharing their experience with utilizing OMM and OMT in rotations, preparing for boards, and briefly presented on board topics, such as Chapman’s reflex points.
July17,3hrs
BiodynamicCranialOsteopathy:Biodynamic concepts were introduced. Students experienced a palpation workshop sensing their partner’s health through cranial, chest and lower extremity palpations.
July19,2hrs
Occipital-AtlantoJointandBiodynamics:A presentation on biodynamic concepts reviewed cranial dysfunctions and how to treat an anterior and posterior atlas. Students were also guided through palpation exercises.
July23 UsingYourOsteopathicHandsandMind:This was a discussion on the principles of osteopathic and alternative medicines, including traditional Chinese Medicine.
July23 UsingandExplainingOMTinClinicalSituations;OMTinResearch:Advice and insight to common patient encounters and osteopathic research were discussed. Research concepts and advances in the field of OMM were discussed.
July26 OutdoorTherapeuticYogaIntegratingOsteopathicPhilosophy:An academic scholar led an outdoors yoga session integrating osteopathic philosophy and concepts.
July27 OMTinPediatrics;ProgramClosingNotes:Faculty demonstrated and discussed OMT use on children with two volunteer children from the faculty. The workshop covered key considerations in treating the pediatric population.
Table 1. 2013 SAAO Summer Preceptorship Program Workshops. Unless otherwise specified, workshops were taught by osteopathic physicians and professors at NYIT-COM and ran for one hour. New York Institute of Technology College of Osteopathic Medicine. Old Westbury, NY. 2013.

Page 16 The American Academy of Osteopathy Journal • Vol. 23, No. 4, December 2013
Table 1showsthedates,duration,andtopicofeachworkshop.
Methods
ThisstudywasapprovedbytheNYITInstitutionalReviewBoardasanexemptstudy(NYIT-IRBBHS#970).FollowingcompletionoftheSAAOOMTSummerPreceptorshipProgram,studentswereprovidedwithabrief,hardcopy12-questionsurvey(seeAppendixA,page20).ThestudywasconductedatNYIT-COMinOldWestbury,NY.Responderswerenotprovidedwithanyincentivestocompletethesurvey.
Thesurveycontainedfivemultiple-choicequestionsregardingtheimpactofthepreceptorshiponthestudents’perceptionsofOMT.ThesurveyemployedthestatisticallyvalidatedLikertscaleformatforfiveofthesevenscaledquestions.Thefive-pointLikertscaleanswerselectionsrangedfrom“stronglyagree”to“stronglydisagree.”13Thesefirstfivequestionsassessedtheeffectoftheprogramontheparticipants’perceptionofOMTconfidencelevel,understandingofclinicalapplicationsofOMT,awarenessofthescope,anticipatedfutureuseofOMTandtheiroverallperceptionofOMT.TheoutcomesmeasuredweretheinterpretationsoftheperceptionLikertscalesreportedbytheparticipants.
Responders’confidencelevelwasassessedbythestatement,“IbelievethisprogramhelpedmetoimprovemyconfidencelevelwithusingOMT.”Theirunderstandingwasassessedbythestatement,“Ibelievethisprogramhelpedmeunderstandthe
clinicalapplicationofOMT.”Participants’intentiontouseOMTinthefuturewasassessedbythestatement,“IbelievethisprogrampositivelyinfluencedmetoconsiderintegratingofOMTinmyfuturepractice.”TheirawarenessofthescopeofOMTwasassessedbythestatement,“IbelievethisprogramhelpedtoexpandmyawarenessofwhatconditionscanbetreatedwithOMT.”Finally,participantsratedtheeffectoftheprogramontheiroverallperceptionofOMTviathefollowingstatement:“IbelievethatthisprogrampositivelyimprovedmyoverallperceptionofOMT.”
Toevaluaterespectivelytheclinicandworkshopportionsoftheprogram,participantswereaskedtwo-partquestions.Thefirstpartofquestionssixandsevenrespectivelyaskedhowmanysessionsofeachdidthestudentattend.WeutilizedamodifiedLikert-typelevelofqualityscaleforthesecondpartofquestionssixandseven.14Theansweroptionsforthisscalewere:(1)VeryPoor,(2)Poor,(3)Neutral,(4)Good,(5)Excellent.
Thelastfivequestionsofthesurveywereopenandfree-forminnaturetoallowforfeedbackregardingtheleast/mostbeneficialaspectsoftheprogram,recommendedimprovements,andwhatthestudentwoulddodifferentlyafterparticipatingintheprogram.
DataanalysiswasperformedusingIBM©SPSS©statisticalsoftwareversion21.Theresponseratewascalculated.Frequenciesandpercentageswerecalculatedforeachofthescaledresponses:boththeLikertscalequestionsandthemodifiedLikert-typelevelofqualityquestions.
0.00
5.00
10.00
15.00
20.00
25.00
Helped me to improve myconfidence level with using
OMT.
Helped me understand theclinical application of OMT.
Positively influenced me toconsider integrating OMT in
my future practice.
Helped to expand myawareness of what
conditions can be treatedwith OMT.
Positively improved myoverall perception of OMT.
Num
ber o
f Res
pond
ents
Self-Reported Effect of Preceptorship on Respondents
Strongly Agree Agree Neutral Disagree Strongly Disagree
Figure 1. Likert Scaled Responses to OMT Perception Questions. N=30. New York Institute of Technology College of Osteopathic Medicine. Old Westbury, NY. 2013.

Vol. 23, No. 4, December 2013 • The American Academy of Osteopathy Journal Page 17
Results
Ofthe50second-yearmedicalstudentswhocompletedtheSAAOPreceptorshipProgram,30studentscompletedthesurvey.Theoverallresponseratewas60percent.ParticipantsrespondedtofivequestionsregardingtheeffectoftheprogramontheirperceptionofOMTonthevalidatedLikertscale.Whenassessingconfidencelevel,20percent(n=6)responded“stronglyagree,”76.67percent(n=23)responded“agree,”and3.33percent(n=1)responded“undecided.”
Theassessmentofparticipants’understandingofclinicalapplicationfoundthat50percent(n=15)responded“stronglyagree,”46.67percent(n=14)responded“agree,”and3.33percent(n=1)responded“undecided”totheLikertscalestatement.Thiswasa96.67percentpositiveresponseofeither“stronglyagree”or“agree.”
Whenassessingtheintentionoffutureclinicaluse,40percentofparticipants(n=12)responded“stronglyagree,”56.67percent(n=17)responded“agree,”and3.33percent(n=1)responded“undecided.”Thiswasa96.67percentpositiveresponserate.Assessment
ofparticipants’awarenessofthescopeofOMTwasassessedand26.67percentofparticipants(n=8)responded“stronglyagree,”63.33percent(n=19)responded“agree,”and10percent(n=3)responded“undecided.”Thiswasa90percentpositiveresponserateforscope.
AssessmentoftheoveralleffectoftheSAAOprogramonparticipants’perceptionofOMTfoundthat50percent(n=15)responded“stronglyagree,”46.67percent(n=14)responded“agree,”and3.33percent(n=1)responded“undecided”tothestatement.Thiswasa96.67percentpositiveresponseratefortheeffectoftheprogramonparticipants’overallOMTperception.Noparticipantsresponded“disagree”or“stronglydisagree”toanyofthesurveyquestions.(Figure 1)
Ofthe30completedsurveys,participantsattendedanaverageof2.21clinicshadowingsessions.Fiftypercent(n=15)ofparticipantsscoredthequalityofthesesessionsas“excellent”onthequalityscale;46.67percent(n=14)scoredthequalityas“good;”and3.33percent(n=1)scoredthequalityas“neutral.”
Participantsattendedanaverageof10.29workshopsessions.Twentypercent(n=6)ofparticipantsratedthequalityoftheworkshopsessionsas“excellent;”73.33percent(n=22)ratedthemas“good;”3.33percent(n=1)ratedtheworkshopsas“neutral.”
Sutherland Cranial Teaching FoundationUpcoming Courses
SCTF Basic Course:Osteopathy in the Cranial FieldJune 6–10, 2014Portland, OregonCourse Director: Dr. Duncan Soule40 hrs 1A CME anticipated
At The Double Tree Hotel at the Lloyd Center1000 NE MultnomahPortland, Oregon
direct link from the airport to the hotel via the Max Light Rail Line
2 restaurants and a fitness center available
Visit our website for enrollment forms and course details: www.sctf.com Contact: Joy Cunningham 509-758-8090Email: [email protected]
10. HaltiwangerE,HuberT,ChangJC,Gonzales-StuartA.AcasestudyofBell’sPalsyapplyingcomplementarytreatmentwithinanoccupationaltherapymodel.OccupationalTherapyInternational.2009;16(1)71-81.
11. ChenN,ZhouM,HeL,ZhouD,LiN.AcupunctureforBell’spalsy.Cochrane Database of Systematic Reviews.2010(8):CDC002914.
12. TeixieraLJ,ValbuzaJS,PradoGF.PhysicalTherapyforBell’spalsyidiopathicfacialparalysis.Cochrane Database of Systematic Reviews.2011;7(12):CD006283.
13. GanzBJ,RedleafMI,PerryBP,GubbelsSP.Chapter28managementofBell’sPalsyandRamsayHuntsyndrome.In:BrackmannDE,SheltonC,ArriagaMA,eds.Otologic surgery.3rded.Philadelphia,PA:Saunders-Elsevier;2010:335-346.www.ClinicalKey.com.Accessed09-17-2013.
14. LancasterDG,CrowWT.Osetopathicmanipulativetreatmentofa26-year-oldwomanwithBell’sPalsy.Journal of the American Osteopathic Association.2006;106(5):285-289.
15. BakerJP,BakerCD.OsteopathicmanipulativetreatmentforLymedisease-inducedBell’sPalsy:acasereport.The AAO Journal.2013;23(1):12-15.
16. CarbonJR.Establishingacaseforcauseandeffect.Journal of the American Osteopathic Association.2006;106(8):443-444.
Accepted for publication: November2013
Address correspondence to:JoshuaP.Baker,DO,FAAFPWestForkFamilyMedicine,PC705ElmStreetEastRockwell,[email protected]
continued from page 12

Page 18 The American Academy of Osteopathy Journal • Vol. 23, No. 4, December 2013
axis. In collaboration with Alain Croibier, DO, Jean-Pierre Barral has also developed the modalities of Neural Manipulation and Global Joint Treatment based on their on-going clinical research. Dr. Barral holds the title of Curriculum Developer for the Barral Institute. Dr. Barral took the modalities and developed them into various manual therapy courses, which he taught since 1985. Dr. Barral has trained and certified a team of International Teachers who also instruct these courses around the world.Since 1999 he has maintained a private practice in Grenoble, France, and has served as Chairman of Department of Visceral Manipulation on the Faculty of Medicine Osteopathy, Grenoble, France; the Chairman of Department of Visceral Manipulation on Faculty of Medicine Paris du Nord; and Academic Director of International College of Osteopathy, St. Etienne, France.
Kenneth J. Lossing, DO, Program ChairDr. Lossing is a 1994 graduate of Kirksville College of Osteopathic Medicine. He completed internship and residency programs at Ohio University College of Osteopathic Medicine, and is certified in Neuromusculoskeletal Medicine/Osteopathic Manipulative Medicine and Family Practice. Dr. Lossing studied under French osteopath Jean-Pierre Barral, DO, and is known internationally as a lecturer on visceral manipulation. He is the AAO President-elect and a member of the AAO Board of Trustees.
New Approach to Osteo-articular Manipulations:Including the Superior and Inferior Limbs
Course Description: This course will present a new manner to check and to treat all the upper limb components, shoulders, elbows, wrists and hands.As well as offering an unique and original approach of the lower limbs including the hips, knees, ankles and feet. CME:The program anticipates being approved for 32 hours of AOA Category 1-A CME credit pending approval by the AOA CCME.
Course Location:The Broadmoor1 Lake Avenue, Colorado Springs, CO 80906Reservations: 7am to 9pm (MT), seven days a week.(800) 634-7711 (Mention AAO event.) https://resweb.passkey.com/go/aao14
Jean-Pierre Barral, DO, Featured SpeakerJean-Pierre is an Osteopath and Registered Physical Therapist who serves as Director (and Faculty) of the Department of Osteopathic Manipulation at the University of Paris School of Medicine in Paris, France. He earned his diploma in Osteopathic Medicine in 1974 from the European School of Osteopathy in Maidstone, England, and went on to teach spinal biomechanics at the institution from 1975-1982.He developed the modality of Visceral Manipulation based on his innovative theory that each internal organ rotates on a physiological
March 15–18, 2014 in Colorado Springs, CO
Register online at www.academyofosteopathy.org. For travel arrangements, contact Tina Callahan of Globally Yours Travel at (800) 274-5975 or [email protected].
Comment
TheSAAOSummerPreceptorshipProgramcombinesclinicalshadowingexperiencesandOMTworkshops,exposingstudentstoavarietyofosteopathicphysicians,providingmentorsinthefield,andhighlightingthemanyclinicalapplicationsofOMT.
TheresultsillustratethepositiveeffectsoftheSAAOSummerPreceptorshipprogramonsecond-yearmedicalstudents’perceptionsofandintentionstouseOMT.RespondentsreportedanoverallpositiveeffectontheirperceptionofOMT,whichcomprisedtheirOMTconfidencelevel,understandingofclinicalapplicationsofOMT,awarenessofthescopeofOMT,andanticipatedfutureuseofOMTinclinicalpractice.
Acomprehensivemedicaleducationprovidesstudentswithclinicalexperiencesandmentors.Ourresultscoincidewithcurrenthealthcareeducationalresearch.Niemanetal.observedthatparticipationintheTexasStatewideFamilyPracticePreceptorshipProgram(TSFPPP)wasassociatedwithanincreased
selectionoffamilypracticeresidency.TheTSFPPPincludeddirectandobservedinteractionswithpatientsininpatientandoutpatientfamilypracticesettings.Incontrasttonon-participants,significancewasfoundinstudentswhoparticipatedinthefirstandsecondyear(OR=1.62,95%CI:1.41-1.87);thirdandfourthyear(OR=2.31,95%CI=1.99-2.68);andthroughouttheirfouryearsofmedicalschool(OR=4.98,95%CI:3.75-6.68).15Likewise,researchersatStanfordUniversityMedicalCenterconductedastudyexaminingtheeffectsofan8-weekvascularsurgerysimulationelectivecourseon52preclinicalmedicalstudents.Priortotheelective,ninepercentofstudentswerehighlyinterestedinvascularsurgeryasaspecialty.Post-course,90percent(p=.03)oftheparticipantswereinterestedinpursuingvascularsurgery,andlong-termfollowup(onetothreeyears)revealedthat70percentremainedinterested.Mostrespondentsattributedtheircontinuedinterestinthespecialtytothesimulationpracticecourse(90percent)andfacultymentorship(70percent).16
Click here to register
online.

Vol. 23, No. 4, December 2013 • The American Academy of Osteopathy Journal Page 19
Future Studies
Thelong-termeffectsofthisprogramcanbeassessedinfuturestudies.ThiscanbeaccomplishedbysurveyingpastparticipantsoftheprogramontheiruseofOMTduringthird-andfourth-yearclinicalrotationsandinclinicalpracticeaftergraduation.ThisstudycouldalsobeusedtoguidealargerstudyexaminingtheeffectofthistypeofprogramonOMTuseandperception.
Limitations
Thelimitationsofourstudydeserveconsiderationandshouldbeaddressedinfuturesurveysonthistopic.Oursamplesizeof30participantswassmall.Thereisaselectionbiasinnatelypresentinthisstudy—studentsself-selectedtoparticipateintheSAAOSummerPreceptorshipProgram.Studyparticipantsfromthatself-selectedgroupthenvoluntarilyansweredthissurvey.Participantsmaynotbetrulyrepresentativeofthelargerpopulationofpreclinicalosteopathicstudents.Baselineassessmentofparticipants’OMTperceptionspriortothestartoftheprogramwasnotobtained.
Conclusion
The2013SAAOSummerPreceptorshipProgram’seffecthasbeenevaluatedby60percentofitsparticipants(n=30)aspositivelyaffectingtheirperceptionofOMT.Thispositiveevaluationsupportsthecontinuationandfurtherstudyofthisprogram.Tothebestofourknowledge,theimplementationofOMTclinicalexperiencesinthepre-clinicalmedicaleducationyearshasseldombeenassessed.Theeffectsofastructuredpre-clinicalexperienceonstudents’attitudes,knowledgeandpotentialbehaviorinregardstoOMTuseandapplication—andthepotentialbenefitsitcanhaveonthecontinuedusageofOMTintheosteopathicprofessionasawhole—meritsfurtherattentionandresearch.
Acknowledgements
TheauthorsofthispaperwouldliketothanktheOsteopathicManipulativeMedicinedepartmentatNYIT-COMforconductingtheSAAOSummerPreceptorshipprogramandtheparticipantsinthissurveyfortheircontributiontothisresearch.
References 1. ChangJC,OdrobinaMR,McIntyre-SeltmanK.Residents
asrolemodels:theeffectoftheobstetricsandgynecologyclerkshiponmedicalstudents’careerinterest.J Grad Med Educ.2010;2:341–345.Availableat:http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2951771/.AccessedOctober21,2013.
2. KutikovA,BonslaverJ,CaseyJT,DegradoJ,DusseaultBN,FoxJA,etal.Thegatekeeperdisparity:whydosomemedical
schoolssendmoremedicalstudentsintourology?J Urol.2011Feb;185(2):647-652.Availableat:http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3058515/.AccessedOctober21,2013.
3. StrausSE,StrausC,TzanetosK.Careerchoiceinacademicmedicine:Systematicreview.J Gen Intern Med.2006;21:1222–1229.Availableat:http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1924755/.AccessedOctober21,2013.
4. WrightS,WongA,NewillC.Theimpactofrolemodelsonmedicalstudents.J Gen Intern Med.1997;12:53-56.Availableat:http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1497058/pdf/jgi_09.pdf.AccessedOctober21,2013.
5. SternszusR,CruessS,CruessR,YoungM,SteinertY.Residentsasrolemodels:impactonundergraduatetrainees.Acad Med.2012Sep;87(9):1282-1287.
6. Keating,EM,O’DonnellEP,Starr,SR.“Howwecreatedapeer-designedspecialty-specificselectiveformedicalstudentcareerexploration”.Med Teach. 2013;35(2):91-94.doi:10.3109/0142159X.2012.731110.Epub2012Oct26.
7. JohnsonAL,SharmaJ,ChinchilliVM,EmerySE,McCollisterEC,Floyd,MW,etal.Whydomedicalstudentschooseorthopaedicsasacareer?J Bone Joint Surg Am.2012;94:e781–e789.
8. HauerKE,DurningSJ,KernanWN,FaganMJ,MintzM,O’SullivanPS,etal.Factorsassociatedwithmedicalstudents’careerchoicesregardinginternalmedicine.JAMA.2008;300:1154-1164.
9. JohnsonSM,KurtzME.Diminisheduseofosteopathicmanipulativetreatmentanditsimpactontheuniquenessoftheosteopathicprofession.Acad Med.2001;76:821–828.
10. ShannonSC,TeitelbaumHS.TheStatusandFutureofOsteopathicMedicalEducationintheUnitedStates.Acad Med.2009;84(6):707-711.
11. ChamberlainNR,YatesHA.“Aprospectivestudyofosteopathicmedicalstudents’attitudestowarduseofosteopathicmanipulativetreatmentincaringforpatients.”J Am Osteopath Assoc.2003Oct;103(10):470-478.Availableat:http://www.jaoa.org/content/103/10/470.long.AccessedOctober21,2013.
12. TengAY,TerryRR,BlueRJ.“IncorporatingaMandatoryOsteopathicManipulativeMedicine(OMM)curriculuminclinicalclerkships:impactonstudentattitudestowardusingOMM.”J Am Osteopath Assoc.2011Apr;111(4):219-224.Availableat:http://www.jaoa.org/content/111/4/219.long.AccessedatOctober21,2013.
13. Albaum,G.TheLikertscalerevisited:analternateversion.Journal of the Market Research Society.39.2(Apr.1997)p331.
14. Vagias,WadeM.Likert-typescaleresponseanchors.ClemsonInternationalInstituteforTourism&ResearchDevelopment,DepartmentofParks,RecreationandTourismManagement.ClemsonUniversity.2006.Availableat:http://www.jaoa.org/content/111/4/219.long.AccessedatOctober30,2013.
15. NiemanLZ,FoxhallLE,ChuangAZ,ChengL,PragerTC.EvaluatingtheTexasStatewideFamilyPracticePreceptorshipProgram,1992-2000.Acad Med.2004Jan;79(1):62-68.
Accepted for publication: November2013
Address correspondence to: SheldonC.Yao,DODepartmentofOsteopathicManipulativeMedicineNewYorkInstituteofTechnologyCollegeofOsteopathicMedicineRoom126NorthernBoulevardOldWestbury,[email protected]

Page 20 The American Academy of Osteopathy Journal • Vol. 23, No. 4, December 2013
Abstract
Despitecurrentprogressinmedicalresearchofdiseases,therearestillmanydiseasesthatareconsideredtobeenigmaticandbafflinginnature.Toinvestigatetheetiologiesandthenatureofmanybafflingdisorders,medicalresearchersdesigntrialstoexplorethepathwaysthatleadtoillnessandtosearchfornewwaystotreathumandisease.Therangeofavailablemodelsisextensive,rangingfromcomputermodelstosinglecellsandsimpleorganisms,suchasworms,tohighervertebratespecies.However,extrapolationintohumansubjectsremainsproblematic.Ideally,thebestdiseasemodelisthehumandiseasemodel,thereforeobviatingtheneedtoextrapolatetheresultsofresearchbasedonnon-
The Application of the Cranial Concept in the Investigation of Baffling Medical Disorders and Their Treatment: A Synergopathic Medical Disease ModelKrishnahari S. Pribadi, MD
humanmodels.However,manyinvestigativemethodsareintrusiveandmayintroduceunpredictablechangesandresponsesofthebodymechanisms.Thehumanorganismisverycomplexandmaynotberepresentedbyinanimateoranimalmodelslackinginmentalandspiritualdimension.
Byusinganon-invasivecranialpalpationmethodtodeterminethebioenergetic,spiritual,craniosacral,physicalmedical,meridian,acupuncture,endocrine,nutritional,foodintolerance,leakygut,circulation,specificpathologicalprofilesofanindividual,theauthorsuggeststhetechnicalprocedurestoevaluatetheclinicalcomprehensiveandholisticpictureofanindividualaffectedbyaspecificdiseaseprocess.Basedonthesefindings,wecandevelopthehypothesesof
APPENDIX A
SAAO Summer OMM Preceptorship Survey 2013
Pleasecircle/underlineorcompletethefollowingquestions:
1. IbelievethisprogramhelpedmetoimprovemyconfidencelevelwithusingOMT.
StronglyAgree/Agree/Undecided/Disagree/StronglyDisagree
2. IbelievethisprogramhelpedmeunderstandtheclinicalapplicationofOMT.
StronglyAgree/Agree/Undecided/Disagree/StronglyDisagree
3. IbelievethisprogrampositivelyinfluencedmetoconsiderintegratingofOMTinmyfuturepractice.
StronglyAgree/Agree/Undecided/Disagree/StronglyDisagree
4. IbelievethisprogramhelpedtoexpandmyawarenessofwhatconditionscanbetreatedwithOMT.
StronglyAgree/Agree/Undecided/Disagree/StronglyDisagree
5. IbelievethatthisprogrampositivelyimprovedmyoverallperceptionofOMT.
StronglyAgree/Agree/Undecided/Disagree/StronglyDisagree
6.a.Howmanysessionsdidyoushadowaclinicianinthisprogram?_________
b.Howwouldyouratetheoveralleducationalqualityoftheshadowingsession?VeryPoor/Poor/Neutral/Good/Excellent
7.a.Howmanyworkshopsessionsdidyouattendinthisprogram?_________
b.Howwouldyouratetheoveralleducationalqualityoftheworkshops?VeryPoor/Poor/Neutral/Good/Excellent
8. Whataspectsoftheprogramweremostbeneficial?
9. Whataspectsoftheprogramdidyoufindleastvaluable?
10. Whatimprovementswouldyourecommend?
11. Giveanexampleofonethingyouwilldodifferentlybecauseofthisprogram.
12. Pleasefeelfreetoshareanyadditionalcommentsandsuggestions.Andusethebackofthepagetocontinueifnecessary.(Youranswerswillbekeptconfidential.Thankyouforyour
assistancetocontinuetoimprovetheprogram!)

Vol. 23, No. 4, December 2013 • The American Academy of Osteopathy Journal Page 21
specificdiseaseswhichaffecttheindividuals.Thehypothesescanthenbetestedindesigntrialsusingvariousmodelsasappropriate.Varioustreatmentapproachescanbedevelopedandtestedout.TheSynergopathicDiseaseModelAssessmentFormhasbeendevisedbytheauthorandcanbeobtainedforfreeforclinicalandresearchpurposesbyemail.
Introduction
Despitecurrentprogressinmedicalresearchofdiseases,therearestillmanydiseasesthatareconsideredenigmaticandbafflinginnature.Koch’spostulates,developedinthe19thcentury,haveplayedanimportantroleinmicrobiology1asgeneralguidelinestoidentifyetiologiesofinfectiousdiseases.Theyhavebeensuccessfulinclarifyingthenatureofmanyinfectiousdiseaseprocessessuchascholera,smallpox,tuberculosis,poliomyelitisandmanyotherviralinfections. Recently,modernnucleicacid–basedmicrobialdetectionmethodshavemadeKoch’soriginalpostulateslessrelevant.Thesenucleicacid–basedmethodsmakeitpossibletoidentifymicrobesthatareassociatedwithadisease.2Yettherearestillmanybafflingdiseases,includingmanyautoimmunedisorders,degenerativediseases,fibromyalgia,chronicfatiguesyndrome,schizophrenia,autism,diabetesmellitustype1and2,Alzheimers’sdisease,Parkinson’sdisease,Guillain-Barresyndrome,leakygutsyndrome,polyneuropathy,allergicdiseases,variouscancersandmanyothers.Toinvestigatetheetiologiesandthenatureofthesebafflingdisorders,medicalresearchersdesigntrialstoexplorethepathwaysthatleadtoillnessandtosearchfornewwaystotreathumandisease.Thesescientistsusediseasemodelsintheirresearch,especiallytotestspecifichypothesesortoexploreunintendedreactions.Animalmodelsplayanintegralpartintranslationalresearch.Therangeofavailablemodelsisextensive,rangingfromcomputermodelstosinglecellsandsimpleorganismssuchasworms,tohighervertebratespecies.However,extrapolationintohumansubjectsremainsproblematic.3Thus,thetreatmentofbafflingdisordersremainshamperedbythelackofunderstandingofthediseaseprocessesandthelimitationsofconventionalmedicine,whichreliesheavilyonchemicalpharmacologicalinterventions,developedprimarilybasedonanimalmodelSandinvitrotesting.Ideally,thebestdiseasemodelisthehumandiseasemodel,thereforeobviatingtheneedtoextrapolatetheresultsofresearchbasedonnon-humanmodels.However,manyinvestigativemethodsareintrusiveandmayintroduceunpredictablechangesandresponsesofthebodymechanisms.Thehumanorganismisverycomplexandmaynotberepresented
byinanimateoranimalmodelslackinginmentalandspiritualdimension.Furthermore,thepowerofconventionalbedsidephysicalexaminationislimited.PsychiatricdisorderswereconsideredtohavenophysicalabnormalitiesbeforetheworkofWoods&Woods.Theirresearchdemonstratedthepresenceofabnormalcranialmechanisminschizophrenicpatientscharacterizedbymembranousrestriction,osteo-mastoidsuturalrestriction,sphenobasilarcompressionandslowandweakcranialimpulserhythm.4
Synergopathic Disease Model
WhatisSynergopathicmedicine?TheauthorcoinedthetermtodescribeasystemofmedicinecapableofintegratingvariousphilosophicalformsofmedicinewithinasingleframeworkbasedonsynergeticphilosophicalideasandconceptsaspromulgatedbyR.BuckminsterFuller.Synergyisastateofoptimalfunctioningofanintegratedsystemconsistingofpartsandcomponents.“Synergymeansbehaviorofintegral,aggregate,wholesystemsunpredictedbybehaviorsofanyoftheircomponentsorsubassembliesoftheircomponentstakenseparatelyfromthewhole.”5,6Disease is caused by a dis-synergic state of the systems and subsystems within an organism, caused by either internal or external factors or both.Synergopathicmedicinesynthesizesandintegratesallcurrentformsofmedicine—including,butnotlimitedto,allopathicmedicine,osteopathicmedicine,cranialosteopathy,homeopathy,naturalmedicine,chiropracticmedicine,acupuncture,herbalism,traditionalmedicine,bio-energeticmedicine,spiritualmedicine,etc.—withinasingleframeworkcapableofdissolvingalldifferencesandcontradictions,therebysynthesizingandintegratingallthecomponentsandsubassembliesoftheircomponentstoformasynergicstate.
Cranial Osteopathy is considered to be the core of Synergopathic medicine and is used to integrate all elements of various medicines since all forms of medicine affect the craniosacral system functioning as the highest regulatory system in the body. By evaluating, monitoring and manipulating therapeutically the craniosacral system, we synergetically apply any medical procedures capable of optimizing this system.Wenolongerdivideapatientintopartsandcomponentstobetreatedwithvariousformsofmedicine.Thus,wenolongertreatunilaterally—organswithvariouspharmacologicalmoietiesand/orsurgeries;themindwithmanipulationofthinking;emotionalpatternswithvariouspsychotherapeuticmodalitiesandinterventions;andthespiritwithpracticesofvariousbeliefsandmyths.Instead,weseeapatientasalivinghumanbeingconsistingofsystemsorganized

Page 22 The American Academy of Osteopathy Journal • Vol. 23, No. 4, December 2013
andintegratedbiologically,socially,mentally,cosmologicallyandspirituallytoformathinking,acting,willingbeingthathasfeelings,meaningandhopeaswellasphysicalcomponentsandspiritualexistence.Insteadofforcingapatientintooneformofmedicine,webringallformsofmedicinetothepatienttobeappliedsystematicallyandholistically.6
The Craniosacral Digital Diagnostic Method
Theauthor’sresearch,usingasurfacescanninglaserdisplacementmetertorecordmicro-pulsations,hasobjectivelyestablishedthepresenceofpulsations(withamaximumdeflectionof0.07mmandfrequenciesrangingfrom4to11cpm)atseveralacupuncturepoints,thecharacteristicsofwhichareidentifiedwiththecharacteristicsofthecranialrhythmicimpulse.7Thecranialrhythmicimpulse(CRI)reflectsthehomeostaticstatusofaperson.AbnormalCRIusuallyindicatesthereareproblemswithinthehomeostaticmechanismsofaperson.ThereareagentsandforcesthatcaninfluencetheCRIcharacteristics.The use of non-invasive and safe palpation, with “feeling, thinking, seeing and knowing fingers” is the cornerstone of the cranial diagnostic method as developed by William G. Sutherland, DO. MonitoringtheCRIwhileapplyingthecranialmanipulativeproceduresisanimportantaspectofthepalpationoftheCRI.Basedonthesefindings,theauthordevelopedtheCraniosacral Digital Diagnostic
Methodtoassessthecharacteristicsofpulsationsofspecificacupuncturepointstodeterminethemeridianprofileofanindividual.BypalpatingtheMUE49ofthehandfingersandtwoadditionalacupuncturepointsatthedorsalsurfaceofthemiddleknuckles,thetreatmentspecialistestablishesthecharacteristicsofthe12meridiansofanindividual.Thefollowingmethodsdevelopedbytheauthorcombinetocreateanindividual’sacupunctureprofile:
• CraniosacralAcupuncturePalpatoryMethod©isusedtolocateabnormalacupuncturepoints.
• CraniosacralNutritionalAssessmentMethod©determinesnutritionalrequirementsbypalpatingthenutritionalpointsforCRI.
• CraniosacralAllergyScreeningTest©canscreenfoods,substancesand/ordrugsforallergyorintolerance.
• CraniosacralTherapeuticSensitivityandDoseDetermination©determines individualtherapeuticsensitivitytotherapeuticagentsandtheirdoses.
• CraniosacralTele-DiagnosticMethod©canbeusedtodiagnose,aswellastreat,patientsfromgreatdistances.
• CraniosacralPathologicalProfileMethodisamethodtodeterminethenatureofthepathologicalprocessesofanindividual
GROWING FL PRACTICE SEEKS FP/DO/DERMATOLOGIST
ReliantFamilyPracticeinGainesville,FL,seeksspecialistinFamilyPractice/OMMand/orFamilyPractice/Dermatologyforitsgrowing,close-knit,supportivepracticeunderthedirectionofErikSchabert,DO.CallMikaHarris,OfficeManager,forfirstcontactat(352)[email protected].
NMM PLUS 1 POSITIONS AVAILABLE IN SUNNY
SOUTH FLORIDA
ResidencyprogramatLarkinHospital.ContactJoelD.Stein,DO,FAAO,at(954)[email protected].
NMM PLUS 1 RESIDENCY PROGRAM IN NEW YORK
NMMPlus1ResidencyatSouthamptonHospitalinbeautifulSouthampton,LongIsland.Applicationsarecurrentlybeingaccepted.Ifinterested,pleasecontactProgramDirectorDeniseK.Burns,DO,FAAO,atdrdenise@optonline.netorEducationDepartmentSecretaryKarenRobertsat(631)726-0409.
PRACTICE OSTEOPATHY IN BEAUTIFUL COLORADO
Successfulintegrativepracticeseeksaboard-certified/eligibleNMM/OMMphysicianforitsbusyDenveroffice.Preferablysomeonecomfortablewithabroadvarietyoftechniques.Verycompetitive
compensation.Friendlyandprofessionalatmosphere.Pleasecall(303)781-7862oremailCVtomgentile@cointegrative.com.Ourwebsiteiswww.cointegrative.com.
DO SOUGHT FORCONNECTICUT PRACTICE
PracticeavailableinHartford,CT.PrimarilyspecializesinOMT,prolotherapyandchronicpainmanagement.Incomefor2012was$700K,withnetincomeof$335K.Muchmoretoexplainregardingdemographicsofthecommunity,hospitalsintheareaandbeautifulnearbyresidentialareas.Ifinterested,pleasecontactGaryN.Wiessenat(631)[email protected].
CLASSIFIED ADVERTISEMENTS

Vol. 23, No. 4, December 2013 • The American Academy of Osteopathy Journal Page 23
(circulation,immunity,toxin,hormone,neoplastic,degeneration,nutritional,tissueoxygenation,spiritual).
Theauthoralsodevisedamethodtodeterminethespecificbloodbiochemicalvaluesofanindividualbypalpatingspecificpoints.AbnormalpointsareassociatedwiththeabsenceofPRMpulsationsofthespecificpoints(Upledger-Pribadi’ssign).Therearethreelevelsofpressuresused:light(0g),medium(5g)andhard(20g),representingsuccessivelythebioenergetic,chemicalandphysicaldimensionsofthediseaseprocessesbeingevaluated.8By determining the bioenergetic, spiritual, craniosacral, physical medical, meridian, acupuncture, endocrine, nutritional, food intolerance, leaky gut, circulation, specific pathological profiles of an individual, we can thus develop the clinical comprehensive and holistic picture of an individual affected by a specific disease process. Based on the findings, thus, we can develop the hypotheses of specific diseases which affect the individuals. The hypotheses can then be tested out in design trials using various models as appropriate. Various treatment approaches can then be developed and tested out. The Synergopathic Disease Model Assessment Form has been devised by the author.
Synergopathic Herbal Formulas
Theauthorintroducedthecranialosteopathic,homeopathicandacupuncturemedicineconceptsalongwiththephyto-pharmacologicalconceptinformulatingherbalformulasinadditiontoutilizingtraditionaldiscoveriesaswellasvastliteraturesintheuseofIndonesianherbalplantsformedicinalpurposes.Eachherbalplanthasaspecificmeridianspectralresponsewheningested.Theuseofalaserscanningmetertodetectandmeasurepulsationatacupuncturepointshasthepotentialtoobjectivelyevaluatethemeridianspectrumofeachherbalplant.Theauthorusesaclinicalpalpationmethodoftheacupuncturepointstoevaluatetheherbalmeridianspectrum.Fortunately,duetothebio-energeticpropertiesofherbalplants,bysimplytouchingthebodywithacertainherbalplant,wecanevaluateandmeasurethespecificeffectsofthatparticularherbalplantuponthecraniosacral,meridian,acupunctureandbioenergysystemofanindividualaffectedbyspecificdiseases;thuseachformulahastherapeuticeffectsuponthephysiologicalandregulatorymechanismsatthechemicallevel(phyto-pharmacologicaleffect),themeridiansystem(meridianeffect),thecraniosacralsystemasthehighestregulatorysystemwithinthebody(craniosacraleffect),thevitalenergysystem(homeopathiceffect)andtheprimitivebrainsystem(olfactoryoraromatherapeuticeffect).Thismodern
andrevolutionizedapproachtopreparingherbalplantsasremedieshasproventobeveryeconomical,effective,safeandpowerful.9
Leaky Gut Syndrome
Leakygutsyndrome,orincreasedintestinalpermeability,10iscausedbyincreasedpermeabilityofthegutwallresultingfromtoxins,poordiet,parasites,infectionormedications.11Thispermeabilitythenallowssubstancessuchastoxins,microbes,undigestedfood,wasteormacromoleculestoenterthecirculation.Intestinalinflammationcausedbyintestinaldysbiosisorothersourcesofirritation,widensthejunctionsbetweenthecellsoftheintestinallining,allowingendotoxinsandincompletelydigestedparticlestobepartiallyabsorbed.Thesearetargetedbyantibodies,formingimmunecomplexeswhichcauseasemi-infectiousstate,andcanbecarriedbythebloodstreamtodistantsiteswheretheymaystimulatethereleaseofcytokines.12Althoughleakygutsyndromeisnotanestablisheddiagnosis,thereareclinicaldiagnosticteststhatactuallymeasurepermeabilityofthegutwall.Cranialpalpationmethodcanbeusedtodetectleakygutsyndrome.Placetwohandssimultaneouslyonliver-epigastrum,liver-navelandliver-colonareas.TheabsenceofPRMpulsationsindicatesthepresenceofleakygutsyndrome.ProbesofCrEDTA,PEG400,lactulose,mannitolandrhamnose,havebeenusedtomeasureintestinalpermeabilitybylookingaturinaryrecovery.13Anothertestusedbyresearchersquantitativelyassessesthetranslocationoflipopolysaccharide(LPS)moleculesacrossthegutwall.14Lowgradefever,transientgutpain,andasenseofinabilitytoabsorbnutrientsaresomereportedsymptomsinotherwiseundiagnosedpatients.15Leakygutsyndromeisassociatedwithmanydisorderssuchasasthma,diabetes,autoimmunediseaseslikelupus,diseaseslikescleroderma,internalcolitis,long-termdisorderslikerheumatoidarthritis,severeillnesseslikemultiplesclerosisandchronicfatiguesyndromeandCrohn’sdisease.Severaldietarytreatments,includinggluten-freediets,casein-freediets,antifungaldiets,low-sugardiets,aswellassupplementsthatincludenystatin,B12andprobioticshavebeenintroduced.16
Case Investigation
Seetheaccompanyingtableonpage25.
Conclusion and Proposed Research Issues
ThecaseinvestigationusingtheSynergopathicdiseasemodelhasidentifiedcommonissuesinthepathwaysofvariousbafflingdisorders.Centralinthedevelopmentofdiseasesistheroleofviralinfection,whichtriggersautoimmunereactionsagainstmostcells

Page 24 The American Academy of Osteopathy Journal • Vol. 23, No. 4, December 2013
inthebody.Therefore,identifyingvirusesresponsibleforinitiatingthediseaseprocessiscrucial.ThePCRmethodisrelevant.Immunesystemabnormalityisparticularlypresent.Thestudyofimmunologycomponents,cellularandhumoralfactors,isessential.Thepresenceofnegativeenergyfieldandweakbioenergysystemsuggeststheroleofspiritualforces.ThesecanbestudiedbyusingKirlianphotography,surfacescanninglaserdisplacementmetertomeasureacupuncturepulsations,acupunctureelectronicmeasurementdevice,magneticsensordevice,etc.Abnormalcraniosacralmechanismcausedbystructuralboneandconnectivetissuechangesshouldbestudiedusingobjectivemeasurementmethods.Laboratorybiochemicalassaystodetermineabnormalmetabolismandassessmentofvitamins,mineralsandenzymedeficienciesshouldbeconducted.Specificbiologicalmarkersshouldbeidentifiedandlaboratoryproceduresdevisedtoassistinthediagnosis.Leakygutsyndromeshouldbediagnosedbylaboratorymethods,candidamicrobiologyanddigestivestoolexamination.Toxinsfromvirus,candida,heavymetals,toxicmetabolitesandchemicaldrugsshouldbeidentifiedandmeasured.Researchofvarioustreatmentmethodsaddressingalltheabnormalmechanismstoestablishanewbalanceandhomeostaticregulationpattern,cellular,tissueandorganrepairandregenerationandnutritionaldeficienciesshouldbedevisedandstudied.Treatmentproceduresthataffectthecraniosacralsystemnegativelyarenotconsideredeffective.Effectivetreatmentproceduresmustcorrectspecificabnormalitiesofthediseases.SynergopathicherbalformulasforspecificdiseaseshavebeendesignedtosupportandcorrecttheabnormaldiseaseprocessesandwillproducemoreorlessnormalSynergopathicdiseasemodelprofiles.By simply placing the specific formulas on the body, all the profiles as tested by the cranial palpation method will revert to normal.Itisunlikelythatonlypharmacologicalinterventioniseffective.Patientswiththesediseasesmaydevelopimmunologicalreactionstosyntheticdrugsandserioussideeffects.
References1. KochR.UntersuchungenüberBakterien:V.Die
ÄtiologiederMilzbrand-Krankheit,begründetaufdieEntwicklungsgeschichtedesBacillus anthracisInvestigationsintobacteria:V.Theetiologyofanthrax,basedontheontogenesisofBacillus anthracis.Cohns Beitrage zur Biologie der Pflanzen, Vol.2.1876:277–310.
2. BrockTD.(1999).Robert Koch: a Life in Medicine and Bacteriology.WashingtonDC:AmericanSocietyofMicrobiologyPress;1999.
3. ChangMC,GriederFB.Dis Model Mech.2008Sep-Oct;1(2-3):99–102.doi:10.1242/dmm.001354.PMCID:PMC2562189
4. PribadiK.Psychosynergisis:ASynthesisofOsteopathicMedicine,AcupunctureMedicineandHomeopathyinPsychiatry.Amer Academy Osteo J.Spring,1998.
5. FullerRB.Synergetics: Explorations in the Geometry of Thinking.NewYork:Macmillan,1975,p.3.
6. PribadiK.SynergopathicMedicineandthecranialconceptinthesuccessfultreatmentofapatientwithparalyticileus:acasereport.Amer Academy Osteo J.2012;22(3):pp.12-18.
7. PribadiK.TheDetectionandRecordingofCranialRhythmicImpulseinAcupuncturePointsusingSurfaceScanningLaserDisplacementMeteranditsSignificance.Amer Academy Osteo J.2008;18(4):p.20-28.
8. PribadiK.VariousmethodsofCRIpalpationofbodyparts,theirdiagnosticvaluesandinterpretationofthefindings.Amer Academy Osteo J.2010;20(3).
9. PribadiK.“NaturalMedicineandMedicinalHerbalism.”GuestLectureatUniversityofPancasila,Jakarta,Indonesia,PharmacyDepartment:2008.
10. MeadowsS.TheBoywithaThorninHisJoints.TheNew York Times.AccessedFeb.1,2013.
11. LiuZ,LiN,NeuJ.Tightjunctions,leakyintestines,andpediatricdiseases.Acta Paediatr.2005;94(4):386–93.doi:10.1111/j.1651-2227.2005.tb01904.x.PMID16092447.
12. KieferD,Ali-AkbarianL.Abriefevidence-basedreviewoftwogastrointestinalillnesses:irritablebowelandleakygutsyndromes.Altern Ther Health Med.2004;10(3):22–30;quiz31,92.PMID15154150.
13. Assessmentofthelactulose-mannitoltestinCrohn’sdisease.FANDREetal.,Gut,1988,29,511-515
14. EvidenceforTranslocationofMicrobialProductsinPatientswithIdiopathicCD4+Lymphocytopenia.Leeetal.JInfectDis2009June1;199(11):1664–1670
15. LeakyGutSyndromes:BreakingtheViciousCycles.GallandL.TownsendLetterforDoctors,August/September1995,p.63.
16. Pizzorno,JE,Murray,MT,(November2005)TextbookofNaturalMedicine,3rdedition,ChurchillLivingstone,pp167,584,1527ISBN0-443-07300-7
17. LevySE,MandellDS,SchultzRT.Autism.Lancet.2009;374(9701):1627–38.doi:10.1016/S0140-6736(09)61376-3.PMID19819542.
18. NewschafferCJ,CroenLA,DanielsJet al.TheepidemiologyofautismspectrumdisordersPDF.Annu Rev Public Health.2007;28:235–58.doi:10.1146/annurev.publhealth.28.021406.144007.PMID17367287
19. AshwoodP,WillsS,VandeWaterJ.Theimmuneresponseinautism:anewfrontierforautismresearch.J Leukoc Biol.2006;80(1):1–15.doi:10.1189/jlb.1205707.PMID16698940.
20. PicchioniMM,MurrayRM.Schizophrenia.BMJ.2007;335(7610):91–5.doi:10.1136/bmj.39227.616447.BE.PMID17626963.
21. McLarenJA,SilinsE,HutchinsonD,MattickRP,HallW.Assessingevidenceforacausallinkbetweencannabisandpsychosis:areviewofcohortstudies.Int. J. Drug Policy.2010;21(1):10–9.doi:10.1016/j.drugpo.2009.09.001.PMID19783132.
22. O’DonovanMC,CraddockNJ,OwenMJ.Geneticsofpsychosis;insightsfromviewsacrossthegenome.Hum. Genet.2009;126(1):3–12.doi:10.1007/s00439-009-0703-0.PMID19521722.
23. SeltenJP,Cantor-GraaeE,KahnRS.Migrationandschizophrenia.Current Opinion in Psychiatry.2007;20(2):111–115.doi:10.1097/YCO.0b013e328017f68e.PMID17278906.
continued on page 33

Vol. 23, No. 4, December 2013 • The American Academy of Osteopathy Journal Page 25
AU
TIS
M
Cas
e
FollowinganMRIvaccination,a4-year-oldboysuddenlyceasedhislanguagedevelopmentattheageof15months,accompaniedbytypicalautisticbehavior:pooreyecontact,socialavoidance,flapping,toe-walking,ritualcompulsivebehavior.Biomedicalinterventionsdidnotresultinsignificantimprovement.Historyincludesfebrileconvulsionandcesareandelivery.Nomedicalcomplicationsduringthefirsttwoyearsoflifeexceptforfebrileconvulsion.
Find
ings
ThisindividualshowspositiveUpledger-Pribadi’ssignattheCDAutism.AllCDsofpathologicprocessesrevealab-normalitiesindicatingthatthediseaseinvolvedallaspectsofhumanphysiology.However,thereisnoorganfailure.Automunnereactionsarepresentinmostorgans,notablybrain,nerves,thyroid,intrinsicfactor,gastrointestinesmostlikelytriggerredbymeaslesvirusfromvaccinationashedoesnothaveahistoryofchildhoodmeasles.MeaslesvirusispresentinthegeneticDNAandstemcells.Influenzavirusispresentinthenervoussystem,respiratory,GItract,immunesystem,musculoskeletalsystem,genitourinarysystem,etc.Mumpsvirusispresentintheparotidglandsandtestis.Leakygutsyndromeispresent,mostlikelycausedbyintestinalcandidainfectionandheavymetalspollution.Immunesystemisinefficientwithautoimmunecomponents.Allhormonesareaffected,notablytestosterone,steroid,pineal,thyroid,growthhormones.Neurotransmittersareabnormalwithhighdopamine,lowserotonin,acetylcholine,GABA.PolyneuropathymostlikelyduetodeficiencyofBcomplex,especiallyvitaminB12duetopoordigestionandabsorption.Notably,digestiveenzymesandbilesaltsarepoorlyproduced.NutritionaldeficienciesincludevitaminsA,Bcomplex,B12,C,E,bioflavonoid,chlorophyll,iodine,intrinsicfactor,calcium,magnesium,zinc.Heavymetalpoison-ingispresentnotably:aluminum,cadmium,mercury,arsenicum,lead.Toxinsarepresent.Mostmajoracupuncturepointsareabnormal,indicatingfailureofthebioenergysystem.Allchakras,auraarepoorlydeveloped.EMFshieldisweak,indicatingheiseasilyinfluencedbyenvironmentalEMF.Strongnegativeenergyandweakspiritualforcearedetected.Thehouseisfilledwithnegativeenergyfield.Thecraniosacralsystemislockedupandnotoperatingduetostresspatternsandweakenergysystem.Foodintoleranceincludes;gluten,casein,fryingvegetableoils,eggs,honey,sugar,tempeh,hotpepper,pepper,phenol-containingfruits,seafood,meat,chicken,fish,chocolate,coffee,additives,beans,nutswiththeexceptionofsoybeans.
Hyp
othe
sis
Centralinthedevelopmentofautismistheroleofviralinfection,whichtriggersneurodegenerationandautoimmunereactions,particularlytowardthebrainandnervecellularcomponents,intrinsicfactorandtissuewhichcauseabnormalneurotransmitterproductionandregulation.Immunesystemabnormalityisparticularlypresent.Abnormalcraniosacralmechanismcausedbyprenatal,natalornataltrauma,ispresent.Thickduralmembranes,SBScompression,medialcompressionaswellasbilateralosteomastoidrestrictionsandlumbosacralcompressionaredetected.Combinedwithpoorassimilationofneurovitaminsandantioxidantvitamins,thecentralandautonomicnervoussystemarejeopardized.Leakygutsyndrome,causedbyintestinalcandidainfection,sensitizestheimmunesystemtowardallergensandbodycomponents.Spiritualforcesplayintothedevelopmentofautismandthereforeshouldbeconsideredintreatingthisdisorder.Nutritionalapproachisessentialalongwithherbalandsupplementtreatment.Treatmentshouldbeholisticinnature,addressingalltheabnormalmechanismsandnutritionaldeficienciesandestablishinganewbalanceandhomeostaticregulationpattern.Leftandrightbrainintegration,audiovisualintegration,cerebralbrainstemintegrationarelacking.Autismisaneurodevelopmentaldisordercausedbymultiplefactorsinvolvingbody,mindandspiritualdimensions,includinggenemutations,heredity,viralinfection,autoimmuneresponsetovirus,leakygutsyndrome,neurotransmitterimbalance,nutritionaldeficienciesduetopoordigestionandassimilationofnutrition.Negativeen-ergyinterfereswiththebioenergeticregulatorysystematthecraniosacral,meridian-acupunctureandchakrasystem.
Curr
ent C
once
pts
&
Med
ical
Res
earc
h Fi
ndin
gs
Autismisadisorderofneuraldevelopmentcharacterizedbyimpairedsocialinteractionandcommunicationandbyrestrictedandrepetitivebehavior.Thegeneticsofautismarecomplex.Relationshavebeenfoundbetweenautismandschizophreniabasedonduplicationsanddeletionsofchromosomes.Evidencepointstosynapticdysfunctionasacauseofautism.17Environmentalfactorsthathavebeenclaimedtocontributeto,orexacerbate,autism,ormaybeimportantinfutureresearch,includecertainfoods,infectiousdisease,heavymetals,solvents,dieselexhaust,PCBs,phthalatesandphenolsusedinplasticproducts,pesticides,brominatedflameretardants,alcohol,smoking,illicitdrugs,vaccines18andprenatalstress.69Therelationshipofneurochemicalstoautismisnotwellunderstood;severalhavebeeninvestigated,withthemostevidencefortheroleofserotoninandofgeneticdifferencesinitstransport.3Aberrantimmuneactivityduringcriticalperiodsofneurodevelopmentispossible.
Syne
rgop
athi
c H
erba
l Fo
rmul
a
Extractsofabriprecatorius,centellaeasiatica,curcumaofficinalis,morindacitrifolia,panaxginseng,phylanthusuri-naria,stachytarphetamutabilis,sonchiarvensis,zingiberisofficinalis,aloevera,avocado,cantaloupe,pineapple,guava,passiflorafruits,probiotic,lactobacillusacidophilusinsorbitolandnaturalalcohol20%.
SCH
IZO
-P
HR
EN
IA
Cas
e
A38-year-oldmandiagnosedwithschizoaffectivedisorder,ahistoryofdrugabuse(marijuana,amphetamine,LSD,cocainebutnotheroine)andalcoholabusestartingatage16followingparentalseparation.Hehasbeenonantipsy-choticdrugsandvalproicacidforanumberofyears.Hehasengagedinaggressivebehaviortowardfamilymembers,criminalbehaviorsincludingtheftandrobbery,resultinginimprisonment.Symptomsincludemoodswings,auditoryhallucinations,persecutoryandgrandiosedelusionsandnegativesymptoms.
Table 1. Case Investigations

Page 26 The American Academy of Osteopathy Journal • Vol. 23, No. 4, December 2013
SCH
IZO
PH
RE
NIA
(con
t’d.)
Find
ings
ThisindividualshowspositiveUpledger-Pribadi’ssignattheCDSCHIZ.AllCDsofpathologicprocessesrevealabnor-malitiesindicatingthatthediseaseinvolvedallaspectsofhumanphysiology.However,thereisnoorganfailure.Autoim-munereactionsarepresentinmostorgans,notablybrain,nerves,thyroid,mostlikelytriggeredbymeaslesvirusfromvaccineashedoesnothaveahistoryofchildhoodmeaslesleadingtowardneurodegeneration.MeaslesvirusaswellasthegeneticDNAandstemcells.Influenzavirusispresentinthenervoussystem,respiratory,GItract,immunesystem,musculoskeletalsystem,genitourinarysystem,etc.Mumpsvirusispresentintheparotidglandsandtestis.Leakygutsyndromesispresent,mostlikelycausedbyintestinalcandidainfectionandheavymetalspollution.Immunesystemisinefficientwithautoimmunecomponents.Allhormonesareaffected,notablytestosterone,steroid,pineal,thyroid.Neurotransmittersareabnormalwithhighdopamine,lowserotonin,acetylcholine,GABA.PolyneuropathymostlikelyduetodeficiencyofBcomplex,especiallyvitaminB12duetopoordigestionandabsorption.Notably,digestiveenzymes,andbilesaltsarepoorlyproduced.Highuricacid,cholesterol,triglyceridesuggestabnormalmetabolism.Intrinsicfactorislacking.Mostmajoracupuncturepointsareabnormal,indicatingfailureofthebioenergysystem.Allchakras,auraarepoorlydeveloped.EMFshieldisweak,indicatingheiseasilyinfluencedbyenvironmentalEMF.Strongnega-tiveenergyandweakspiritualforcearedetected.Thecraniosacralsystemisnotoperatingduetostresspatternsandweakenergysystem.Thisyoungmanexperimentedwithaddictivedrugsattheageof16followingparentalseparation.Theseaddictivedrugsintroducedhimtotheworldofnegativeenergy;consequently,hehasbeeneasilyinfluencedbynegativespiritualforces,withpoorimpulsecontrolandlackofconscience.Hehasengagedinmanyantisocialbehav-iors,includingaggressivebehavior,robberyandtheft,andhasbeenimprisonedonseveraloccasions.Hewasunabletopursuehisgraduateeducationashisintellectualfunctioningdeterioratedquicklyandhewasunabletocontrolhisbehaviorandmotivation.Heshowsperiodicpsychoticdecompensationwithextrememoodswings.Deficiencyinmostvitamins,mineralsandaminoacidsduetopoordigestionresultsinabnormalmetabolismandineffectiveneurotrans-mitterproductionandregulation.
Hyp
othe
sis
Centralinthedevelopmentofschizophrenicillnessistheroleofviralinfection,whichtriggersneurodegenerationandautoimmunereactionsparticularlytowardthebrainandnervecellularcomponentsand/ortissue,whichcauseabnormalneurotransmitterproductionandregulation.Immunesystemabnormalityisparticularlypresent.Mentalstressinvitesnegativeenergyforces,andinthiscaseviatheuseofaddictivedrugsandlifestyle.Abnormalcraniosacralmechanismcausedbyprenatalornataltrauma, ispresentwithweakpotencyandenergyandSBScompressionaswellasbilateralosteomastoidrestrictionsandlumbosacralcompression.Combinedwithpoorassimilationofneuro-vitaminsandantioxidantvitamins,thecentralandautonomicnervoussystemSarejeopardized.Theperiodicnatureofthisillnessappearstoberelatedtocyclingduetoinefficienthomeostaticregulationandenvironmentalfactors.Deteriorationmayfollowprogressiveviralinfectionandautoimmunedestructiveprocess.Leakygutsyndromecausedby intestinalcandida infectionsensitizes the immunesystemtowardsallergensandbodycomponents.Hallucina-tionsanddelusionsareproducedbythecombinationofneurotransmitterfailure,bioenergeticdysregulationandviralinfectiontriggeredbymentalstressaswellasspiritualandtoxicfactors.Spiritualforcesplayintothedevelopmentofschizophrenicillnessandthereforeshouldbeconsideredintreatingthisdisorder.Nutritionalapproachisessentialalongwithherbalandsupplementtreatment.Treatmentshouldbeholistic innature,addressingalltheabnormalmechanismsandnutritionaldeficienciesandestablishinganewbalanceandhomeostaticregulationpattern.Theuseofaddictivedrugsisverydestructivetotheprogressionofillness.Schizophreniaisaneurodevelopmentaldisordercausedbymultiplefactorsinvolvingbody,mindandspiritualdimensionsincludinggenemutations,heredity,viralinfection,autoimmuneresponse,leakygutsyndrome,neurotransmitterimbalance,nutritionaldeficienciesduetopoordigestionandassimilationofnutrition.Negativeenergyinterfereswiththebioenergeticregulatorysystematthecraniosacral,meridian-acupunctureandchakrasystem.
Curr
ent C
once
pts
& M
edic
al R
esea
rch
Find
ings
Schizophreniaisamentaldisordercharacterizedbyabreakdownofthoughtprocessesandbyadeficitoftypicalemo-tionalresponses.Commonsymptomsincludeauditoryhallucinations,paranoidorbizarredelusions,ordisorganizedspeechandthinking,accompaniedbysignificantsocialoroccupationaldysfunction.Thegreatestriskfordevelopingschizophreniaishavingafirst-degreerelativewiththedisease(riskis6.5percent);morethan40percentofmonozygotictwinsofthosewithschizophreniaarealsoaffected.20Manypossiblecandidateshavebeenproposed,includingspecificcopynumbervariations,NOTCH4,andhistoneproteinloci.21Anumberofgenome-wideassociations,suchaszincfingerprotein804A,havealsobeenlinked.22Parentingstyleseemstohavenomajoreffect.Livinginanurbanenvironmentduringchildhoodorasanadulthasconsistentlybeenfoundtoincreasetheriskofschizophreniabyafactoroftwo.Otherfactorsthatplayanimportantroleincludesocialisolationandimmigrationrelatedtosocialadversity,racialdis-crimination,familydysfunction,unemploymentandpoorhousingconditions.23Abouthalfofthosewithschizophreniausedrugsoralcoholexcessively.24Evidencesupportsalinkbetweenearlieronsetofpsychoticillnessandcannabisuse.25Thereisevidencethatalcoholabuseviaakindlingmechanismcanoccasionallycausethedevelopmentofachronicsubstance-inducedpsychoticdisorder,e.g.,schizophrenia.Themoreoftencannabisisused,themorelikelyapersonistodevelopapsychoticillness,withfrequentusebeingcorrelatedwithtwicetheriskofpsychosisandschizophrenia.26Factorssuchashypoxiaandinfection,orstressandmalnutritioninthemotherduringfetaldevelopment,mayresultinaslightincreaseintheriskofschizophrenialaterinlife.Peoplediagnosedwithschizophreniaaremorelikelytohavebeenborninwinterorspring(atleastinthenorthernhemisphere),whichmaybearesultofincreasedratesofviralexposuresinutero.20StudiesusingneuropsychologicaltestsandbrainimagingtechnologiessuchasfMRIandPETtoexaminefunctionaldifferencesinbrainactivityhaveshownthatdifferencesseemtomostcommonlyoccurinthefrontallobes,hippocampusandtemporallobes.28Reductionsinbrainvolume,smallerthanthosefoundinAlzheimer’sdisease,havebeenreportedinareasofthefrontalcortexandtemporallobes.Particularattentionhasbeenpaidtothefunction

Vol. 23, No. 4, December 2013 • The American Academy of Osteopathy Journal Page 27
SCH
IZO
PH
RE
NIA
(con
t’d.)
ofdopamineinthemesolimbicpathwayofthebrain.TheinfluentialdopaminehypothesisofschizophreniaproposedthatexcessiveactivationofD2receptorswasthecauseof(thepositivesymptomsof)schizophrenia.Thedopaminehypothesis isnowthoughttobesimplistic,partlybecausenewerantipsychoticmedication(atypicalantipsychoticmedication)canbejustaseffectiveasoldermedication(typicalantipsychoticmedication),butalsoaffectsserotoninfunctionandmayhaveslightlylessofadopamineblockingeffect.29Lowlevelsofglutamatereceptorswerefoundinthepostmortembrainsofthosediagnosedwithschizophrenia.30
Syne
rgop
athi
c H
erba
l For
-m
ula
Extractsofhydrocotyleasiatica,panaxginseng,pinussylvestris,curcumaofficinalis,aeruginosa,xanthorriza,mangga,avocado,aloevera,apple,cantaloupe,nonifruit,passiflora,pineapple,guavainsorbitol.Propolisaspreservative.Con-tainsprobioticlactobacilusacidophilusbacteria.Containsnoalcoholorman-madechemicals.
MU
LTIP
LE S
CLE
RO
SIS
Cas
e A36-year-oldmansufferingfromweakness,legparalysis,attacksofunconsciousness,currentlywheelchair-bound.Hewasdiagnosedwithmultiplesclerosisbyaneurologist.ExaminationwasdonebyCraniosacralTelediagnosisashedidnotrespondtotheauthor’sinterestinexamininghimviaFacebookcommunication.
Find
ings
ThisindividualshowspositiveUpledger-Pribadi’ssignattheCDMS.AllCDsofpathologicprocesses(infection,degenera-tion,circulation,immunity,toxicity,hormones,neoplasticprocess,nutrition,spiritualdimension,tissueoxygenation)revealabnormalitiesattheenergetic,chemicalandphysicallevels,indicatingthatthediseaseinvolvedallaspectsofhumanorgans,tissues,cellsandphysiology.Mostmajoracupuncturepointsareabnormalatbioenergetic,chemicalandphysicallevels,indicatingfailureofthebioenergysystem.Allchakras,auraarepoorlydeveloped.EMFshieldisweak,indicatingheiseasilyinfluencedbyenvironmentalEMF.Strongnegativeenergyandweakspiritualforcearedetected.Thecraniosacralsystemisnotoperatingduetostresspatterns,SBScompression,bioccipitalmastoidrestrictions,OAand lumbosacralcompression.Allphysiologicalsystemsandorgansareaffectedatthebioenergetic,chemicalandstructurallevels.Autoimmunereactionsarestronglypresentinmostorgans,notablyimmunesystem,skin,internalorgans,brain,nerves,heart,arteries,veins,allendocrines.Enterovirusandinfluenzavirusesinfecttheimmunesystem,skin,allinternalorgans,tissuesandcellsaswellasthegeneticDNAandstemcells.Leakygutsyndromeispresent,mostlikelycausedbyviralinfection,intestinalcandidainfectionandheavymetalspollution.Toxinsarepresentinallstructuresofthebody.Immunesystemisinefficientwithautoimmunecomponents.Allhormonesareaffected,notablymalehormone,steroid,pineal,thyroid,insulin,growthhormone,etc.Neurotransmittersareabnormalwithnormaldopamine,lowserotonin,acetylcholine,GABA.PolyneuropathymostlikelyduetodeficiencyofBcomplex,especiallyvitaminB12,duetopoordigestionandabsorption.Notably,intrinsicfactor,digestiveenzymes,andbilesaltsarepoorlyproduced.Highuricacid,cholesterol,triglyceridesuggestabnormalmetabolism.Deficiencyinmostvitamins,mineralsandaminoacidsduetopoordigestionresultsinabnormalmetabolismandineffectiveneurotransmitterproductionandregulationaswellasosteoporoticchanges.Allnutritionalcomponentsarelow,notablyantioxidantvitamins,vitaminsBcomplex,C,D,K,bioflavonoids,calcium,magnesium,zinc,potassiumandnatriumarelow.Bloodsugarandcreatinineareslightlyelevated.Poorbloodcirculationandpoorcellularoxygenationarenoted.
Hyp
othe
sis
CentralinthedevelopmentofMSistheroleofviralinfection,nervoussheathandmutationofthegenes.Immunesystemabnormalityisparticularlypresent.Thepresenceofanegativeenergyfieldandweakbioenergysystemsuggesttheroleofspiritualforces.Abnormalcraniosacralmechanismcausedbystructuralboneandconnectivetissuechangesispresentwithweakpotencyandenergy.Combinedwithpoorassimilationofneurovitaminsandantioxidantvitamins,thecentralandautonomicnervoussystemarejeopardized.Thefailureofhomeostaticregulatorysystemisobvious.Remissionanddeteriorationmayfollowthewaxingandwaningofviralinfectionandautoimmunedestructiveprocess.Leakygutsyndrome,causedbyintestinalcandidaandviralinfection,sensitizestheimmunesystemtowardallergensandbodycomponents.Toxinsfromvirus,candida,heavymetals,toxicmetabolitesandchemicaldrugsmayaccumu-late.PoortissueandcellularoxygenationduetolowvitaminB12preventstissuerepair.Treatmentshouldbeholisticinnatureaddressingalltheabnormalmechanismsandestablishinganewbalanceandhomeostaticregulationpattern,cellular,tissueandorganrepairandregenerationandnutritionaldeficiencies.MSisanimmune-mediateddisordermediatedbyacomplexinteractionoftheindividual’sgeneticsandasyetunidentifiedenvironmentalinsults.4Possibletargetsoftheimmuneresponseincludemyelinbasicprotein(MBP)andproteolipidprotein(PLP).RecentdatasuggestaroleformyelinlipidsinMS.24Virusmayberesponsiblefortriggeringautoimmuneresponse.Strongspiritualfactorsarepresentinthiscasebutexternalinnature.
Curr
ent C
once
pts
&
Med
ical
Res
earc
h Fi
ndin
gs
Multiplesclerosis(MS)isaninflammatorydiseaseinwhichthefattymyelinsheathsaroundtheaxonsofthebrainandspinalcordaredamaged,leadingtodemyelinationandscarringaswellasabroadspectrumofsignsandsymptoms.31MostlikelyMSoccursasaresultofsomecombinationofgenetic,environmentalandinfectiousfactors.Anumberofgeneticvariationshavebeenshowntoincreasetheriskofdevelopingthedisease.32Possibletargetsoftheimmunere-sponseincludemyelinbasicprotein(MBP)andproteolipidprotein(PLP).RecentdatasuggestaroleformyelinlipidsinMS.33Diseaseactivationbiomarkersincludeinterleukin-6,nitricoxideandnitricoxidesynthase,osteopontinandfetuin-A.34Severestressmaybeariskfactoralthoughevidenceisweak.35Smokinghasalsobeenshowntobeaninde-pendentriskfactorfordevelopingMS.36Associationwithoccupationalexposuresandtoxins—mainlysolvents—hasbeenevaluated,butnoclearconclusionshavebeenreached.35Vaccinationswereinvestigatedascausalfactorsforthe

Page 28 The American Academy of Osteopathy Journal • Vol. 23, No. 4, December 2013
MU
LTIP
LE
SCLE
RO
SIS
(con
t’d.) disease;however,moststudiesshownoassociationbetweenMSandvaccines.35Evidenceforvirusesasacauseincludes
thepresenceofoligoclonalbandsinthebrainandcerebrospinalfluidofmostpeoplewithMS,humanherpesviruses,measles,mumpsandrubellahavealsobeenrelatedwithMS.31
Syne
rgop
athi
c H
erba
l Fo
rmul
a
Extractsofpanaxginseng,caselpiasappan,sonchusarvensis,stachytarpethamutabilis,isotomalongiflora,curcumaofficinalis,aeruginosa,xanthorriza,mangga,avocado,aloevera,pineappleinblackhoney,propolisasapreservative.Containsprobioticlactobacilusacidophilusbacteria.Containsnoalcoholorman-madechemicals.
SYST
EM
IC L
UP
US
ER
YT
HR
OM
AT
OSU
S (S
LE)
Cas
e A56-year-oldwoman,thefounderoftheIndonesianLupusAssociation,hasbeendiagnosedwithSLEforanumberyears.TheauthorperformedCraniosacralTelediagnosisbyviewingherpicturebroadcastviaTV.Theindividualisunknowntotheauthor.Sheappearstobehealthyandfunctional,beingabletoclimbupanddownmountains.
Find
ings
This individual showspositiveUpledger-Pribadi’s signat theCDSLE.AllCDsofpathologicprocesses (infection,degeneration, circulation, immunity, toxicity, hormones, neoplastic process, nutrition, spiritualdimension, tissueoxygenation)revealabnormalitiesattheenergetic,chemicalandphysicallevels,indicatingthatthediseasepermeatesallaspectsofhumanorgans,tissues,cellsandphysiology.Mostmajoracupuncturepointsareabnormalatbioenergetic,chemicalandphysicallevels,indicatingfailureofthebioenergysystem.Allchakras,auraarepoorlydeveloped.EMFshieldisweakindicatingsheiseasilyinfluencedbyenvironmentalEMF.Strongnegativeenergyandweakspiritualforcearedetected.Thecraniosacralsystemisnotoperatingduetostresspatterns,SBScompression,bioccipitalmastoidrestrictions,OAandlumbosacralcompression.Allphysiologicalsystemsandorgansareaffectedatthebioenergetic,chemicalandstructurallevels.Autoimmunereactionsarestronglypresentinmostorgans,notablyimmunesystem,kidneys,skin, internalorgans,brain,nerves,heart,arteries,veins, intrinsicfactor,allendocrines.Epstein-Barrandinfluenzavirusesinfecttheimmunesystem,skin,allinternalorgans,tissuesandcellsaswellasthegeneticDNAandstemcells.Leakygutsyndromeispresent,mostlikelycausedbyviralinfection,intestinalcandidainfectionandheavymetalspollution.Toxinsarepresentinallstructuresofthebody.Immunesystemisinefficientwithautoimmunecom-ponents.Allhormonesareaffected,notablyfemalehormone,steroid,pineal,thyroid,insulin,growthhormone,etc.Neurotransmittersareabnormalwithnormaldopamine,lowserotonin,acetylcholine,GABA.PolyneuropathymostlikelyduetodeficiencyofBcomplex,especiallyvitaminB12,duetopoordigestionandabsorption.Notably,intrinsicfactor,digestiveenzymes,andbilesaltsarepoorlyproduced.Highuricacid,cholesterol,triglyceridesuggestabnormalmetabolism.Deficiencyinmostvitamins,mineralsandaminoacidsduetopoordigestionresultsinabnormalme-tabolismandineffectiveneurotransmitterproductionandregulationaswellasosteoporoticchanges.Allnutritionalcomponentsarelow,notablyvitaminsA,Bcomplex,C,D,K,bioflavonoids,calcium,magnesium,zincarelow.Natriumishighandpotassiumislow.Poorbloodcirculationandpoorcellularoxygenationarenotedonallregions.Creatinine,bloodsugarandliverenzymesareslightlyelevated.
Hyp
othe
sis
CentralinthedevelopmentofSLEistheroleofviralinfection,whichtriggersautoimmunereactionsagainstmostcellsinthebody.Immunesystemabnormalityisparticularlypresent.Thepresenceofnegativeenergyfieldandweakbioenergysystemsuggeststheroleofspiritualforces.Abnormalcraniosacralmechanismcausedbystructuralboneandconnectivetissuechangesispresentwithweakpotencyandenergy.Combinedwithpoorassimilationofneurovita-minsandantioxidantvitamins,thecentralandautonomicnervoussystemarejeopardized.Thefailureofhomeostaticregulatorysystemisobvious.Remissionanddeteriorationmayfollowthewaxingandwaningofviralinfectionandautoimmunedestructiveprocess.Leakygutsyndrome,causedbyintestinalcandidaandviralinfection,sensitizestheimmunesystemtowardallergensandbodycomponents.Toxinsfromvirus,candida,heavymetals,toxicmetabolitesandchemicaldrugsmayaccumulate.PoortissueandcellularoxygenationduetolowvitaminB12preventstissuerepair.Treatmentshouldbeholisticinnature,addressingalltheabnormalmechanismsandestablishinganewbalanceandhomeostaticregulationpattern,cellular,tissueandorganrepairandregenerationandnutritionaldeficiencies.SLEisanimmune-mediateddisordermediatedbyacomplexinteractionoftheindividual’sgeneticsandasyetunidentifiedenvironmentalinsults.Virusmayberesponsiblefortriggeringautoimmuneresponse.Strongspiritualfactorsarepres-entinthiscasebutexternalinnature.
Curr
ent C
once
pts
& M
edic
al
Res
earc
h Fi
ndin
gs ConstitutiveoverexpressionofBAFFinBAFF-transgenicmiceleadstoexpandedB-cellpopulationsandpolyclonalhy-pergammaglobulinemia.37,38,39Increasedserumand/orplasmalevelsofBLyShavebeendocumentedinhumansystemicerythematosus(SLE),rheumatoidarthritis,Sjögren’ssyndromeandHIVinfection.40-43
Her
bal
For-
mul
a Extractsofpanaxginseng,sonchusarvensis,stachytarpethamutabilis,cinnamomumburmani,curcumaofficinalis,xanthorriza,mangga,avocado,aloevera,guava,pineappleinblackhoney,propolisasapreservative.Containsprobioticlactobacilusacidophilusbacteria.Containsnoalcoholorman-madechemicals.

Vol. 23, No. 4, December 2013 • The American Academy of Osteopathy Journal Page 29
Course DescriptionAn additional model used in the diagnosis and treatment of musculoskeletal pain. This course will cover the ankle, shoulder, and knee. FDM is a model of thinking that provides a framework to view the function of the body and the expres-sion of pain. Fascia can be viewed as the “wrapper” of our bones, muscles, and organs. Fascia is an integral part of the body’s nerve network. Dr. Still identified the importance of the fascial system when seeking health. Treatments in the FDM are directed at the fascia and restoring its function by focusing on correcting distortions in the fascial system and thereby eliminating pain. The FDM provides practitioners another model in which to view the body and another tool in the battle against musculoskeletal pain. FDM expands the capability of traditional Osteopathic modalities by specifically addressing the fascia and the distortions which are identified. Treatment of the fascial distortions can provide dramatic results by addressing the Biotensegrity of the body. The FDM is driven by a patient’s body language, verbal description, and the provider’s underlying understanding of the fascial distor-tions and their impact on the whole system. CME16 hours of AOA Category 1-A credit are anticipated.
Course TimesMonday and Tuesday: 8:00 am - 5:30 pmBreakfast and lunch on your own, coffee provided.Todd A. Capistrant, DO, MHA, Program ChairDr. Capistrant is a board-certified Family Medicine physician specializing in Osteopathic Manipulation. He has been with Tanana Val-ley Clinic in Fairbanks, AK, since 2006, where he first began attending to patients in their 1st Care Center. In June 2013 he was selected as the Medical Director of Tanana Valley Clinic and oversees the thirteen different departments that comprise the clinic. Dr. Capistrant received a B.S. in Biology from the University of Minnesota and a D.O. at Des Moines University in Iowa. In addition to his medical education, Dr. Capistrant received a master’s degree in Healthcare Administration from Des Moines University in Iowa. He is one of three physicians in the U.S. certified to teach seminars on the FDM model.Course LocationThe Broadmoor1 Lake Avenue, Colorado Springs, CO 80906Reservations: 7am to 9pm (MT), seven days a week. (800) 634-7711 (Mention AAO event.) https://resweb.passkey.com/go/aao14
An Introduction to the Fascial Distortion Model (FDM)March 17–18, 2014
Course DescriptionThis course is designed for participants with intermediate to advanced skills in OMM and those who have taken intermediate level Cranial courses. We will take an in-depth look at the anatomical and structural influences of the pediatric ENT patient, taking a close look at the cranial and facial anatomy and its influences on health and function of the middle ear, sinuses, and temporomandibular joint.CME16 hours of AOA Category 1-A credit are anticipated.Course TimesMonday and Tuesday: 8:00 am - 5:30 pmBreakfast and lunch on your own, coffee provided.Course LocationThe Broadmoor1 Lake Avenue, Colorado Springs, CO 80906Reservations: 7am to 9pm (MT), seven days a week.(800) 634-7711 (Mention AAO event.) https://resweb.passkey.com/go/aao14
Osteopathic Approach to Common ENT Complaints of Children
Heather P. Ferrill, DO, Program ChairDr. Ferrill, a 2000 Michigan State University College of Osteopathic Medicine graduate, is an Associate Professor of Osteopathic Manipulative Medicine (OMM) at the Rocky Vista University College of Osteopathic Medicine (RVUCOM). Board-certified in Family Practice and Neuromusculoskeletal Medicine/OMM, her practice emphasizes Osteopathic Manipulative Treatment in the pediatric population. She serves on the AAO Board of Governors and the Education Committee.
March 17–18, 2014
Register online at www.academyofosteopathy.org. For travel arrangements, Contact Tina Callahan of Globally Yours Travel at (800) 274-5975 or [email protected].
Click here to register
online.
Click here to register
online.

Page 30 The American Academy of Osteopathy Journal • Vol. 23, No. 4, December 2013
VIT
ILIG
O
Cas
e A55-year-oldmanwithprogressivevitiligoduringthelastsixyears.Nomedicaltreatmentsucceededinstoppingtheprogressionandimprovingpigmentation.Healsohashypertension,highuricacid,cholesterolandtriglycerideandobesity.Heworksasaphotographer.
Find
ings
ThisindividualshowspositiveUpledger-Pribadi’ssignattheCDVIT.AllCDsofpathologicprocesses(infection,degen-eration,circulation,immunity,toxicity,hormones,neoplasticprocess,nutrition,spiritualdimension,tissueoxygenation)revealabnormalitiesattheenergetic,chemicalandphysicallevels,indicatingthatthediseaseinvolvedallaspectsofhumanorgans,tissues,cellsandphysiology.Mostmajoracupuncturepointsareabnormalatbioenergetic,chemicalandphysicallevels,indicatingfailureofthebioenergysystem.Allchakras,auraarepoorlydeveloped.EMFshieldisweak,indicatingheiseasilyinfluencedbyenvironmentalEMF.Strongnegativeenergyandweakspiritualforcearedetected.Thecraniosacralsystemisnotoperatingduetostresspatternsandweakenergysystem.Allphysiologicalsystemsandorgansareaffectedatthebioenergetic,chemicalandstructurallevels,Autoimmunereactionsarestronglypresentinmostorgans,notablyimmunesystem,skin,internalorgans,brain,nerves,heart,arteries,veins,allendocrines.Unknownvirusandinfluenzavirusinfectstheimmunesystem,skin,allinternalorgans,tissuesandcellsaswellasthegeneticDNAandstemcells.Thedepigmentedareasare infectedwiththeunknownvirus.Leakygutsyndromeispresent,mostlikelycausedbyviralinfection,intestinalcandidainfectionandheavymetalspollution.Toxinsarepresentinallstructuresofthebody.Immunesystemisinefficientwithautoimmunecomponents.Allhormonesareaffected,notablymalehormone,steroid,pineal,thyroid,insulin,growthhormone,etc.Neurotransmittersareabnormalwithnormaldopamine,lowserotonin,acetylcholine,GABA.PolyneuropathymostlikelyduetodeficiencyofBcomplex,especiallyvitaminB12duetopoordigestionandabsorption.Notably,intrinsicfactor,digestiveenzymes,andbilesaltsarepoorlyproduced.Highuricacid,cholesterol,triglyceridesuggestabnormalmetabolism.Deficiencyinmostvitamins,mineralsandaminoacidsduetopoordigestionresultsinabnormalmetabolismandineffectiveneurotransmitterproductionandregulationaswellasosteoporoticchanges.Tissueuricacidisestimatedat8.5,Cholesterol230,triglyceride280,bloodsugar130,creatinine0.9,SGOT40.Allnutritionalcomponentsarelow,notablyantioxidants,vitaminsBcomplex,DandK,calcium,magnesium,zinc,potassium,natriumarelow.Poorbloodcirculationandpoorcellularoxygenationarenoted.Asitturnedout,anegativeenergyfieldemanatingfromanoldgravebehindthehousewasdetected.Elimina-tionofthisnegativeenergyfieldbyenergytechniqueandspiritual-religousmethodresultedinthedisappearanceofnegativeenergyinthebodybioenergysystem.
Hyp
othe
sis
Centralinthedevelopmentofvitiligoistheroleofviralinfectionofanunknownidentity,whichtriggerscellularde-generation,especiallytheskinmelanocytesandautoimmunereactions.Immunesystemabnormalityisparticularlypresent.Thepresenceofanegativeenergyfieldandweakbioenergysystemsuggesttheroleofspiritualforces.AbnormalcraniosacralmechanismcausedbystructuralboneandconnectivetissuechangesispresentwithweakpotencyandenergyandSBScompressionandlumbosacralcompression.Combinedwithpoorassimilationofneurovitaminsandantioxidantvitamins,thecentralandautonomicnervoussystemarejeopardized.Thefailureofhomeostaticregulatorysystemisobvious.Remissionanddeteriorationmayfollowthewaxingandwaningofviralinfectionandautoimmunedestructiveprocess.Leakygutsyndromecausedbyintestinalcandidaandviralinfectionsensitizestheimmunesystemtowardsallergensandbodycomponents.Toxinsfromvirus,candida,heavymetals,toxicmetabolitesandchemicaldrugsmayaccumulate.Nutritionalapproachisessentialalongwithherbalandsupplementtreatment.PoortissueandcellularoxygenationduetolowvitaminB12preventspigmentationandtissuerepair.Treatmentshouldbeholisticinnature,addressingalltheabnormalmechanismandestablishinganewbalanceandhomeostaticregulationpattern,cellular,tissueandorganrepairandregenerationandnutritionaldeficiencies.Vitiligoisasystemicdiseasecausedbyautoimmunereactionsagainstbodycomponents,particularlytheskinmelanocytes.Strongspiritualfactorsarepresentinthiscasebutexternalinnature.
Curr
ent C
once
pts
& M
edic
al
Res
earc
h Fi
ndin
gs Agenome-wideassociationstudyfound10independentsusceptibilitylociforgeneralizedvitiligo,responsiblefor7.4percentofthegeneticrisk.TYRencodestyrosinase,whichisnotacomponentoftheimmunesystem,butisanenzymeofthemelanocytethatcatalyzesmelaninbiosynthesis,andamajorautoantigeningeneralizedvitiligo.44Astudycomparing656peoplewithandwithoutvitiligoin114familiesfoundseveralmutations(single-nucleotidepolymorphisms)intheNALP1gene.TheNALP1gene,whichisonchromosome17locatedat17p13,isonacascadethatregulatesinflammationandcelldeath,includingmyeloidandlymphoidcells,whicharewhitecellsthatarepartoftheimmuneresponse.45
Syne
rgop
athi
c H
erba
l Fo
rmul
a
Extractsofalpinagalanga,aloevera,caselpiasappan,curcumaofficinalis,aeruginosa,xanthorriza,mangga,avocado,aloevera,pineapple,guavainsorbitol,propolisaspreservativeandnaturalalcohol4%inglycerin.Useasalocalherbalformulatoapplyonthedepigmentedareas.

Vol. 23, No. 4, December 2013 • The American Academy of Osteopathy Journal Page 31
IDIO
PAT
HIC
TH
RO
MB
OC
YT
OP
EN
IC P
UR
PU
RA
(IT
P)
Cas
e A52-year-oldmanexperiencinglassitude,paleness,palpitationandpetechialrashoftwomonthsduration.Recentplateletcountrevealed15.000,necessitatingaplatelettransfusion.Upondischargefromthehospital,hewasprescribedasteroiddrug,anantibioticandmultivitamins.
Find
ings
ThisindividualshowspositiveUpledger-Pribadi’ssignattheCDITP.AllCDsofpathologicprocessesrevealabnormali-tiesattheenergetic,chemicalandphysicallevels,indicatingthatthediseaseinvolvedallaspectsofhumanorgansandphysiology.Mostmajoracupuncturepointsareabnormalatbioenergetic,chemicalandphysicallevels,indicatingfailureofthebioenergysystem.Allchakras,auraarepoorlydeveloped.EMFshieldisweak,indicatingheiseasilyinfluencedbyenvironmentalEMF.Strongnegativeenergyandweakspiritualforcearedetected.Thecraniosacralsystemisnotoperatingduetostresspatternsandweakenergysystem.Allphysiologicalsystemsandorgansareaffectedatthebio-energetic,chemicalandstructurallevels.Autoimmunereactionsarestronglypresentinmostorgans,notablyimmunesystem,bonemarrow,bloodcells(particularlythrombocytes),bloodstemcells,skin,internalorgans,brain,nerves,heart,arteries,veins,allendocrinesandtheintrinsicfactor.Epstein-Barr,fluvirusinfectstheimmunesystem,skin,allinternalorgans,tissuesandcellsaswellasthegeneticDNAandstemcells.Leakygutsyndromeispresent,mostlikelycausedbyviralinfection,intestinalcandidainfectionandheavymetalspollution.Toxinsarepresentinallstructuresofthebody.Immunesystemisinefficientwithautoimmunecomponents.Allhormonesareaffected,echovirusnotablymalehormone,steroid,pineal,thyroid,insulin,growthhormone,etc.Neurotransmittersareabnormalwithnormaldopamine,lowserotonin,acetylcholine,GABA.PolyneuropathymostlikelyduetodeficiencyofBcomplex,especiallyvitaminB12,duetopoordigestionandabsorption.Notably,intrinsicfactor,digestiveenzymes,andbilesaltsarepoorlyproduced.Highuricacid,cholesterol,triglyceridesuggestabnormalmetabolism.Deficiencyinmostvitamins,mineralsandaminoacidsduetopoordigestionresultsinabnormalmetabolismandineffectiveneurotransmitterproductionandregulationaswellasosteoporoticchanges.Tissueuricacidisestimatedat10.5,Cholesterol230,triglyceride2560,bloodsugar130,creatinine0.9,SGOT20.Allnutritionalcomponentsarelow,notablyantioxidants,vitaminsBcomplex,DandK,calcium,magnesium,zinc,potassiumandnatriumarelow.Poorbloodcirculationandpoorcellularoxygenationarenoted.Asitturnedout,anegativeenergyfieldemanatingfromanoldtreeinfrontofthehousewasdetected.Labresult:thrombocytewaslow,anemic,leukopenia.
Hyp
othe
sis
CentralinthedevelopmentofITPistheroleofviralinfection,probablyEpstein-Barr,whichtriggerscellulardegenera-tionandautoimmunereactions,particularlytowardthebloodcells,especiallythrombocytes,skin,connectivetissues,skin,brainandnervecellularcomponentsandmanyorgans.Immunesystemabnormalityisparticularlypresent.Thepresenceofnegativeenergyfieldandweakbioenergysystemsuggeststheroleofspiritualforces.Abnormalcraniosa-cralmechanismcausedbystructuralboneandconnectivetissuechangesispresentwithweakpotencyandenergyandSBScompressionandlumbosacralcompression.Combinedwithpoorassimilationofneurovitaminsandantioxidantvitamins,thecentralandautonomicnervoussystemarejeopardized.Thefailureofhomeostaticregulatorysystemisobvious.Remissionanddeteriorationmayfollowthewaxingandwaningofviralinfectionandautoimmunedestructiveprocess.Leakygutsyndrome,causedbyintestinalcandidaandviralinfection,sensitizestheimmunesystemtowardallergensandbodycomponents.Toxinsfromvirus,candida,heavymetals,toxicmetabolitesandchemicaldrugsmayaccumulate.Nutritionalapproachisessentialalongwithherbalandsupplementtreatment.Treatmentshouldbeholisticinnatureaddressingalltheabnormalmechanismandestablishinganewbalanceandhomeostaticregulationpattern,cellular,tissueandorganrepairandregeneration.ITPisasystemicdiseasecausedbyautoimmunereactionsagainstbodycomponents,particularlythrombocytes,megakaryocytes,bloodstemcells,bonemarrow.Strongspiritualfactorsarepresentinthiscasebutexternalinnature.
Curr
ent C
once
pts
&
Med
ical
Res
earc
h Fi
ndin
gs
Idiopathicthrombocytopenicpurpura(ITP)ischaracterizedbypetechialrashassociatedwithanabnormallylowplateletcountofunknowncause.Averylowplateletcountcarriesanincreasedriskofbleedingandpurpura.ITPisdiagnosedbyalowplateletcountinacompletebloodcount(acommonbloodtest).Additionalinvestigations(suchasabonemarrowbiopsy)maybenecessaryinsomecases.Inapproximately60percentofcases,antibodiesagainstplateletscanbedetected.46MostoftentheseantibodiesareagainstplateletmembraneglycoproteinsIIb-IIIaorIb-IX,andareoftheimmunoglobulinG(IgG)typeandsomerenownedresearchestablishedtheimmunepathogenesisofITP.47Thecoat-ingofplateletswithIgGmakesthemsusceptibletoopsonizationandphagocytosisbysplenicmacrophages,aswellasbyKupffercellsintheliver.TheIgGautoantibodiesarealsothoughttodamagemegakaryocytes.47Recentresearchindicatesthatimpairedproductionoftheglycoproteinhormonethromboprotein,whichisthestimulantforplateletproduction,maybeacontributingfactor..
Syne
rgop
athi
c H
erba
l Fo
rmul
a
Extractsofpanaxginseng,caselpiasappan,cameliasinensis,sonchusarvensis,stachytarpethamutabilis,pinussylves-tris,curcumaofficinalis,aeruginosa,xanthorriza,mangga,avocado,aloevera,pineapple,guavainsorbitol,propolisaspreservative.Containsprobioticlactobacilusacidophilusbacteria.Containsnoalcoholorman-madechemicals.

Page 32 The American Academy of Osteopathy Journal • Vol. 23, No. 4, December 2013
DIA
BE
TE
S M
ELI
TU
S T
YP
E 2
Cas
e
A63-year-oldmansufferingfromdiabetesmelitustype2duringthelast15years.ThereisafamilyhistoryofhypertensionandDM,type2.Hehasahistoryofhighuricacid,cholesterol,LDLandtrigylcerides.Herecentlyunderwentcardiacsurgeryforthreeringsplacement.Heismaintainedonshortterminsulinandlongterminsulintokeephisbloodsugarlevelnormal.InthepasthealsoreceivedOADSandacholesterol-reducingdrug.
Find
ings
ThisindividualshowspositiveUpledger-Pribadi’ssignattheCDDMtype2andCDHYT.AllCDsofpathologicpro-cesses (infection, degeneration, circulation, immunity, toxicity, hormones, neoplastic process, nutrition, spiritualdimension,tissueoxygenation)revealabnormalitiesattheenergetic,chemicalandphysicallevels,indicatingthatthediseaseinvolvedallaspectsofhumanorgans,tissues,cellsandphysiology.Mostmajoracupuncturepointsareabnormalatbioenergetic,chemicalandphysicallevels,indicatingfailureofthebioenergysystem.Allchakras,auraarepoorlydeveloped.EMFshieldisweak,indicatingheiseasilyinfluencedbyenvironmentalEMF.Strongnegativeenergyandweakspiritualforcearedetected.Thecraniosacralsystemisnotoperatingduetostresspatterns,SBScompression,OAandlumbosacralcompression.Allphysiologicalsystemsandorgansareaffectedatthebioenergetic,chemicalandstructurallevels.Autoimmunereactionsarestronglypresentinmostorgans,notablyimmunesystem,pancrea,in-trinsicfactor,eyes,skin,internalorgans,brain,nerves,heart,arteries,veins,allendocrines.Enterovirusandinfluenzavirusesinfectpancreasandtheimmunesystem,skin,allinternalorgans,tissuesandcellsaswellasthegeneticDNAandstemcells.Leakygutsyndromeispresent,mostlikelycausedbyviralinfection,intestinalcandidainfectionandheavymetalspollution.Toxinsarepresentinallstructuresofthebody.Immunesystemisinefficientwithautoimmunecomponents.Allhormonesareaffected,notablymalehormone,steroid,pineal,thyroid,insulin,growthhormone,etc.Neurotransmittersareabnormalwithnormaldopamine,lowserotonin,acetylcholine,GABA.PolyneuropathymostlikelyduetodeficiencyofBcomplex,especiallyvitaminB12,duetopoordigestionandabsorption.Notably,intrinsicfactor,digestiveenzymesandbilesaltsarepoorlyproduced.Normaluricacid,cholesterol,triglyceridewithmedica-tions.Deficiencyinmostvitamins,mineralsandaminoacidsduetopoordigestionresultsinabnormalmetabolismandineffectiveneurotransmitterproductionandregulationaswellasosteoporoticchanges.Allnutritionalcomponentsarelow,notablyvitaminsA,Bcomplex,C,D,E,K,bioflavonoids,calcium,magnesium,zinc,potassiumarelow.Natriumishigh.Lowcardiacbloodcirculationandcellularoxygenationarenoted,otherwisenormal.Cellularinsulinsensitivityispoor,endogenousproduction:60percent.Langerhansactivity:60percent.Creatinineisnormal.
Hyp
othe
sis
Theroleofviralinfectioninthepancreascannotbeignored.Influenzavirusispresentinmostpartsofthebody.Im-munityislow.Autoimmuneresponsetomostorgans,tissue,cells(especiallyLangerhanscells),intrinsicfactor,retinaisnoted.Leakygutsyndrome,causedbyintestinalcandidaandviralinfection,sensitizestheimmunesystemtowardallergensandbodycomponents.Toxinsfromvirus,candida,heavymetals,toxicmetabolitesandchemicaldrugsmayaccumulate.Thepresenceofanegativeenergyfieldandweakbioenergysystemsuggeststheroleofspiritualforces.AbnormalcraniosacralmechanismcausedbystructuralboneandconnectivetissuechangesispresentwithweakpotencyandenergyandSBScompressionandlumbosacralcompression.Combinedwithpoorassimilationofneurovitaminsandantioxidantvitamins,thecentralandautonomicnervoussystemarejeopardized.ThefailureofhomeostaticregulatoryDMtype2isprobablyanimmune-mediateddisorderaffectingthepancreaticisletcellsmediatedbyacomplexinterac-tionoftheindividual’sgeneticsandlifestylefactors.Virusmayberesponsiblefortriggeringautoimmuneresponse.Strongspiritualfactorsarepresentinthiscasebutexternalinnature.
Curr
ent C
once
pts
& M
edic
al
Res
earc
h Fi
ndin
gs Diabetesmellitusisagroupofmetabolicdiseasesinwhichapersonhashighbloodsugar,eitherbecausethepancreasdoesnotproduceenoughinsulin,orbecausecellsdonotrespondtotheinsulinthatisproduced.48Type1diabetesmel-litusischaracterizedbylossoftheinsulin-producingbetacellsoftheisletsofLangerhanswhichisaT-cell-mediatedautoimmuneattackinthepancreas.Type1diabetesispartlyinherited,andthentriggeredbycertaininfections,withsomeevidencepointingatCoxsackieB4virus.AgeneticelementinindividualsusceptibilitytosomeofthesetriggershasbeentracedtoparticularHLAgenotypes.Type2diabetesmellitusischaracterizedbyinsulinresistance,whichmaybecombinedwithrelativelyreducedinsulinsecretion.2Type2diabetesisdueprimarilytolifestylefactorsandgenetics.49
Syne
rgop
athi
c H
erba
l Fo
rmul
a
Extracts of panax ginseng, caselpia sappan, cataranthus rosea, camelia sinensis, sonchus arvensis, stachytarpethamutabilis,tinosporacrispa,tribulusterestris,isotomalongiflora,curcumaofficinalis,xanthorrhiza,mangga,avocado,aloevera,pineapple,avocadoinblackhoneywithroyaljelly,propolisasapreservative.Containsprobioticlactobacilusacidophilusbacteria.

Vol. 23, No. 4, December 2013 • The American Academy of Osteopathy Journal Page 33
24. GreggL,BarrowcloughC,HaddockG.Reasonsforincreasedsubstanceuseinpsychosis.Clin Psychol Rev.2007;27(4):494–510.doi:10.1016/j.cpr.2006.09.004.PMID17240501.
25. LargeM,SharmaS,ComptonMT,SladeT,NielssenO.Cannabisuseandearlieronsetofpsychosis:asystematicmeta-analysis.Arch. Gen. Psychiatry.2011;68(6):555–61.doi:10.1001/archgenpsychiatry.2011.5.PMID21300939.
26. SewellRA,RanganathanM,D’SouzaDC.Cannabinoidsandpsychosis.International review of psychiatry (Abingdon, England).2009Apr;21(2):152–62.doi:10.1080/09540260902782802.PMID19367509.
27. BenAmarM,PotvinS.Cannabisandpsychosis:whatisthelink?Journal of Psychoactive Drugs.2007Jun;39(2):131–42.doi:10.1080/02791072.2007.10399871.PMID17703707.
28. Kircher,TiloandRenateThienel.The Boundaries of Consciousness.Amsterdam:Elsevier;2006.ISBN0-444-52876-8.Functionalbrainimagingofsymptomsandcognitioninschizophrenia.p.302.
29. JonesHM,PilowskyLS.Dopamineandantipsychoticdrugactionrevisited.British Journal of Psychiatry.2002;181:271–275.doi:10.1192/bjp.181.4.271.PMID12356650.
30. KonradiC,HeckersS.Molecularaspectsofglutamatedysregulation:implicationsforschizophreniaanditstreatment.Pharmacology and Therapeutics.2003;97(2):153–79.doi:10.1016/S0163-7258(02)00328-5.PMID12559388.
31. CompstonA,ColesA(October2008).Multiplesclerosis.Lancet372(9648):1502–17.doi:10.1016/S0140-6736(08)61620-7.PMID18970977.
32. DymentDA,EbersGC,SadovnickAD(February2004).Geneticsofmultiplesclerosis.Lancet Neurol3(92):104–10.doi:10.1016/S1474-4422(03)00663-X.PMID14747002.
33. HoPP,KanterJL,JohnsonAM,SrinageshHK,ChangEJ,PurdyTM,etal.(2012).Identificationofnaturallyoccurringfattyacidsofthemyelinsheaththatresolveneuroinflammation.Science Translational Medicine4(137):137–73.doi:10.1126/scitranslmed.3003831.PMID22674551.
34. HarrisVK,SadiqSA(2009).Diseasebiomarkersinmultiplesclerosis:potentialforuseintherapeuticdecisionmaking.Mol Diagn Ther13(4):225–44.doi:10.2165/11313470-000000000-00000.PMID19712003.
35. MarrieRA(December2004).Environmentalriskfactorsinmultiplesclerosisaetiology.Lancet Neurol3(12):709–18.doi:10.1016/S1474-4422(04)00933-0.PMID15556803.
36. GhadirianP,JainM,DucicS,ShatensteinB,MorissetR(1998).Nutritionalfactorsintheaetiologyofmultiplesclerosis:acase-controlstudyinMontreal,Canada.Int J Epidemiol.27(5):845–52.doi:10.1093/ije/27.5.845.PMID9839742.(primarysource)
37. GrossJA,JohnstonJ,MudriS,EnselmanR,DillonSR,MaddenK,XuW,Parrish-NovakJ,FosterD,Lofton-DayC,MooreM,LittauA,GrossmanA,HaugenH,FoleyK,BlumbergH,HarrisonK,KindsvogelW,CleggCH.TACIandBCMAarereceptorsforaTNFhomologueimplicatedinB-cellautoimmunedisease.Nature.2000;404:995–999.doi:10.1038/35010115.PubMedCrossRef
38. MackayF,WoodcockSA,LawtonP,AmbroseC,BaetscherM,SchneiderP,TschoppJ,BrowningJL.MicetransgenicforBAFFdeveloplymphocyticdisordersalongwithautoimmune
manifestations.J Exp Med.1999;190:1697–1710.doi:10.1084/jem.190.11.1697.PMCfreearticlePubMedCrossRef9
39. KhareSD,SarosiI,XiaX-Z,McCabeS,MinerK,SolovyevI,HawkinsN,KelleyM,ChangD,VanG,RossL,DelaneyJ,WangL,LaceyD,BoyleWJ,HsuH.SevereBcellhyperplasiaandautoimmunediseaseinTALL-1transgenicmice.Proc Natl Acad Sci USA.2000;97:3370–3375.doi:10.1073/pnas.050580697.PMCfreearticlePubMedCrossRef
40. ZhangJ,RoschkeV,BakerKP,WangZ,AlarcónGS,FesslerBJ,BastianH,KimberlyRP,ZhouT.Cuttingedge:aroleforBlymphocytestimulatorinsystemiclupuserythematosus.J Immunol.2001;166:6–10.PubMed
41. CheemaGS,RoschkeV,HilbertDM,StohlW.ElevatedserumBlymphocytestimulatorlevelsinpatientswithsystemicimmune-basedrheumaticdiseases.Arthritis Rheum.2001;44:1313–1319.doi:10.1002/1529-0131(200106)44:6<1313::AID-ART223>3.0.CO;2-S.PubMedCrossRef
42. GroomJ,KalledSL,CutlerAH,OlsonC,WoodcockSA,SchneiderP,TschoppJ,CacheroTG,BattenM,WhewayJ,MauriD,CavillD,GordonTP,MackayCR,MackayF.AssociationofBAFF/BLySoverexpressionandalteredBcelldifferentiationwithSjögren’ssyndrome.J Clin Invest.2002;109:59–68.doi:10.1172/JCI200214121.PMCfreearticlePubMedCrossRef
43. StohlW,CheemaGS,BriggsW,XuD,SosnovtsevaS,RoschkeV,FerraraDE,LabatK,SattlerFR,PierangeliSS,HilbertDM.Blymphocytestimulatorprotein-associatedincreaseincirculatingautoantibodylevelsmayrequireCD4+Tcells:lessonsfromHIV-infectedpatients.Clin Immunol.2002;104:115–122.doi:10.1006/clim.2002.5238.PubMedCrossRef
44. JinY,BirleaSA,FainPR,etal.(2010).VariantofTYRandAutoimmunitySusceptibilityLociinGeneralizedVitiligo.N Engl J Med.362(18):1686–97.doi:10.1056/NEJMoa0908547.PMC2891985.PMID20410501.
45. MashaghiA,etal.(2010).PossibleassociationoftheCD4genepolymorphismwithvitiligo.Clin Exp Dermatol.35(5):521–4.doi:10.1111/j.1365-2230.2009.03667.x.
46. CoopamahM,GarveyM,FreedmanJ,SempleJ(2003).Cellularimmunemechanismsinautoimmunethrombocytopenicpurpura:Anupdate.Transfus Med Rev.17(1):69–80.doi:10.1053/tmrv.2003.50004.PMID12522773.
47. SchwartzRS(2007).Immunethrombocytopenicpurpura--fromagonytoagonist.N. Engl. J. Med.357(22):2299–301.doi:10.1056/NEJMe0707126.PMID18046034.
48. Shoback,editedbyDavidG.Gardner,Dolores(2011).Greenspan’s Basic & Clinical Endocrinology(9thed.).NewYork:McGraw-HillMedical.pp.Chapter17.ISBN0-07-162243-8.
Accepted for publication:October2013
FormoreinformationortorequestafreecopyofThe Synergopathic Disease Model Assessment Form forresearchandclinicalpurposes,contact:KrishnahariS.Pribadi,MDJalanBorneoRaya,DepokTimur,WestJava,IndonesiaEmailaddress:[email protected]
continued from page 24

Page 34 The American Academy of Osteopathy Journal • Vol. 23, No. 4, December 2013
Abstract
Cutaneousdisorderssuchasacne,psoriasis,chronicwounds,hyperhidrosis,atopicdermatitisandsclerodermaareoftendifficulttotreatbecauseofcomplexpathologicalmechanisms.Currenttheorieslinkthesedisorderstophysiologicaldisturbancessuchaslocalizedtissuecongestion,stress-inducedinflammationandimbalanceoftheautonomicnervoussystem.Osteopathicmanipulativemedicine(OMM)hasalwayshadahomeintheprimarycaresector,butgrowingresearchonthephysiologiceffectsofosteopathicmanipulativetherapyonthebodyhasnowopenedthedoorforitsuseinmanyotherfieldsofmedicine,includingdermatology.Applicationofosteopathicmanipulativetreatment(OMT),suchasmyofascialrelease,ribraising,lymphaticdrainage,andcranialosteopathicmanipulativetechniquesaimtorestorebalanceandtoaidinlong-termmanagementofdermatologicaldisorders.Osteopathicmanipulativetreatmentwillbemostusefulwhencombinedwithcurrentconventionaltherapeuticoptions.However,randomized,well-controlledstudiesarenecessarytoconfirmsuchtherapeuticbenefits.
Contrarytocurrentconcepts,dermatologydoesnotcompromiseosteopathicprincipals,butratherhasthepotentialtoexemplifythoseideals.
Introduction
Osteopathicmanipulativemedicine(OMM)haslongbeenassociatedwiththesectorofprimarycareandhas,overtheyears,showntobeextremelybeneficialinthetreatmentofmusculoskeletaldisorderssuchassomaticdysfunctionsofthecervical,thoracicorlumbarspine,radialorfibularheads,andcarpaltunnelsyndrome.However,asosteopathicphysicianscontinuetogrowinnumberandfindtheirwayintootherspecialtiesoutsideofthefamilypracticeandprimarycarespectra,itisimportanttocontinuetoexploretherolethatOsteopathicmanipulativetreatment(OMT),acornerstoneofosteopathicmedicine,couldhaveinthistransition.Campbelletal.1demonstratehowOMTcanbeusedinthetreatmentofnotalgiaparesthetica,brachioradialispruritis,trigeminalneuralgia,elephantiasisnostrasverrucosaandstasisdermatitis.Inthisarticle,theauthorsaimtodemonstratehow
Potential New Dimensions in Dermatology: The Osteopathic Approach to Cutaneous DiseaseAna M. Michunovich, BS, OMS III; and Robert Stern, MD
similartechniquescanbeappliedtootherdermatologicdiseasesthatmayimprovepatientmanagement.Finally,itaimstodemonstratethatdermatologyisaspecialtythatexemplifiesmanyaspectsofosteopathicmedicalpractice.Theeffectivenessofmanyofthesetreatmentmodalitiesremainstobedemonstratedinclinicaltrials.Butthesubtexthereisthatadditionally,allopathicphysiciansshouldbeencouragedtoincorporatethemintotheirpractices.
Osteopathic Manipulative Medicine and Dermatologic Disease
Manydermatologicdisorderspresentwithamyriadoftreatmentchallengesthatcanbefrustratingforbothphysiciansandpatients.Themajorityofcurrenttreatmentmodalitiesfocusoneithertopicalorsystemicpharmaceuticalagents,mostofwhichcomewithahostofsideeffectsanddelayedbenefits.Topicalointments,creamsandlotionsoftenleavepatientswithdryskin,photosensitivity,skinatrophy,etc.,whileoralmedicationscanresultingastrointestinaldiscomfort,Cushingoidappearance,livertoxicityoraweakenedimmunesystem.Therecurrentlyisalackofresearchconcerningtheuseofosteopathicmanipulationsinthetreatmentofdermatologicaldisorders.However,emergingbreakthroughsinthepathologyofcutaneousdiseasesalongwithclinicalevidencesupportingtheuseofOMMindisorderswithsimilarmechanismssetthestageforrefreshingandcutting-edgetreatmentplans.AsummaryoftheapplicationofOMTtoanumberofdermatologicdiseasesispresentedinTable 1.
Acne. Acnevulgarisisoneofthemostcommonskindisorders,affectingadolescentsandadultsalike.2Itisaninflammatorydisordercharacterizedbyareasofskinwithseborrhea,comedones,papules,pustulesandnodulesandcanpotentiallyresultinhyperpigmentationandpermanentscarring.2Inadditiontophysicalblemishes,prolongedstruggleswithacnehavebeencommonlylinkedtopsychologicaldisturbances.2Tidman2findsthatcomplicationsofacnevulgariscanincludebothphysicalandemotionalscarring.Disfigurementfrominflammation,aswellaspigmentationchangesandscarringoftencauseembarrassment,canundermineconfidenceandlowerself-esteem.Acnecaninducemoreseriouspsychologicaldistress,resultinginanxiety,depression,

Vol. 23, No. 4, December 2013 • The American Academy of Osteopathy Journal Page 35
andsocialwithdrawal.Thepathogenesisofthisdisorderisacomplexinteractionofmultiplefactors,bothinternalandexternaltothepilosebaceousunit,includinginfectionwiththeGrampositivebacteriaPropionibacterium acnes,excessandrogensecretion,highglycemicloaddiets,andpolymorphisminTNF-α(tumornecrosisfactor-alpha),IL-1(interleukin-1),andCYP1A1(CytochromeP450,family1,subfamilyA,polypeptide1)expression.3-6Acnevulgarismayfurthermorebeexacerbatedbystress,2,3,7-9bygreasytopicalpreparationsthatencourageblockageofthepores,bytraumaorahumidclimate.2
Currenttreatmentmethodsincludetopicalretinoids,oralisotretinoin,topicalandoralantibiotics,oralcontraceptivesandlaserorlighttherapy.However,
giventhestrongcorrelationbetweentheworseningofacneandincreasedstresshormonelevels,itcanbeinferredthatOMTtechniquesthatdecreasesympatheticnervoussystemresponsesandrelaxthemindandbodywouldbebeneficialadditivestothesetreatmentprotocols.Assuch,myofascialrelease,ribraisingatT1-4orcranialosteopathicmanipulativemedicinewouldbebeneficial,aswouldbetechniquesthatdecreaseinflammationsuchasfacialeffleurage.Theuseofribraisingtechniquesdecreasessomaticdysfunctioninthatareaofthesympatheticchainganglion,andthusnormalizeexcessautonomicoutput.10,11
Compressionofthefourthventricle(CV-4),acranialOMTmaneuver,alsorestoresproperautonomic
Table 1. Summary of Dermatological Diseases and Applications of OMT
Disease Clinical Features Pathophysiology Suggested Treatment RationaleA
cne
Seborrhea,comedones,papules,pustulesandnodules
P. acnes,excessandrogens,stress,dietandgenetics
Myofascialrelease,ribraising,cranialosteopath-icmanipulativemedicineandfacialeffleurage
Normalizeautonomicnervoussystemoutputandnormalizelymphaticflowtoreduceinflamma-tion
Psor
iasi
s
Sharplydemarcated,erythematous,raisedlesionscoveredwithasilverywhitescale,com-monlyaffectingtheexten-sorsurfacesoftheknees,elbows,trunkandscalp
Stress,genetics Ribraisingandcranialosteopathicmanipulativemedicine
Normalizeautonomicnervoussystemoutput
Chr
onic
w
ound
s Woundsthatfailtohealorhealthenreappear
Lymphaticandvenousinsufficiency
Lymphatictechniques(pedalpump,thoracicpump,effleurageandpectorallift)
Removalofblockageoflymphaticandvenousflow
Hyp
erhi
-dr
osis
Excessivesweatingatthepalms,maxillaeandsoles
Heritablehyperfunction-ingofsudomotorsweatcontrolsystem
Cranialosteopathicmanipulativemedicineandribraising
Normalizeexcessivesympatheticoutputtosudomotorsweatcontrolsystem
Ato
pic
der-
mat
its
Xerosis,lichenification,andeczematouslesions.Excoriationsandcrustingarecommon.
Geneticlossoffunctionmutationinfilaggrin,infectionwithS. aureus,andautonomicnervoussystemdysfunction
Cervicalmyofascialre-lease,cranialosteopathicmanipulativemedicineandribraising
Normalizetheexcessivesympatheticandparasympathetictone
Scle
rode
rma
Damagetothecellsliningthewallsofsmallarter-ies,dilationoflymphaticvessels,destructionoflymphaticvessels,andanabnormalbuildupofscartissueeitherlocallyorsystemically
Autoimmunityandgeneticmutations
Lymphatictechniques(pedalpump,thoracicpump,effleurageandpectorallift)
Increasedclearanceoflymphaticfluid

Page 36 The American Academy of Osteopathy Journal • Vol. 23, No. 4, December 2013
responsebymeansofmanipulationoftheskullsutures,aswellasenhancingfluidexchange.12Furthermore,alymphatictechnique,facialeffleurage,mayhelptocalmsomeoftheinflammationseeninacnepatients.Suchlymphatictechniqueshavebeenlinkedtothemobilizationofinflammatorymediatorsintothecirculation.13
Psoriasis. Psoriasisisamultisystem,chronic,inflammatorydisorderinwhichpatientsexperiencerepeatedboutsofred,pruritic,scalypatchesofskin.Themostcommonformofpsoriasis,plaquepsoriasis,ischaracterizedbysharplydemarcated,erythematous,raisedlesionscoveredwithsilverywhitescalesthatcommonlyaffectstheextensorsurfacesofknees,elbows,trunk,andscalp.Thepathogenesisofpsoriasisinvolvesgeneticandenvironmentalfactors.Amongtheseinfluences,emotionalstressisconsideredtoplayanespeciallyimportantroleinitsonsetandexacerbation.14IthasbeenproposedthatactivatedTH1cellsarerecruitedintotheskinandsecreteinflammatoryIFNΥ(interferongamma)whichinturninduceslocalantigen-presentingcellstosecreteIL-1andIL-23topromotetheexpansionofIL-17expressingCD(clusterofdifferentiation)4+andCD8+Tcells.15Thepathogenesisofpsoriasis,similartoatopicdermatitis,hasbeenlinkedtoabluntedHPA(hypothalamus-pituitary-adrenal)axisinpsoriaticssensitivetopsychologicalstressors.16Currenttreatmentmodalitiesincludetopicalcorticosteroids,VitaminDanalogues,Anthralin,topicalretinoids,oralmethotrexate,oralcyclosporine,calcineurininhibitors,salicylicacid,coaltarandmoisturizers.However,similaritytotherolethatthedisruptionoftheautonomicnervoussystemplaysintheexacerbationofbothacnevulgarisandpsoriasis,suggestsOMTtreatmentmodalitiespreviouslystatedforacnevulgariswouldalsohelppsoriaticpatients.Thesetreatmentsincluderibraisingandcraniosacraltechniques.
Chronic Wounds.Chronicwoundsareclassifiedasthosethatfailtoproceedthroughthehealingprocessinanorderlymannerandthatlastforextendedperiodsoftimeoroccurrepetitively.17,18Thesewoundsareduetoanumberoffactors,butaremostcommonlylinkedtoatherosclerosis,diabetesmellitus,hypertensionandvenousinsufficiency,withincidenceincreasingwithageandobesity.17-19Properwoundhealing,arebuildingofdisruptedanatomicarchitecture,isinitiatedbyplatelet-inducedinflammationandcarriedoutbycellularinfiltrationwithneutrophils,macrophages,Tlymphocytes,fibroblastsandendothelialcells.
Problemsarisewhensuchmediatorscannotreachsitesofinflammation.Chronicvenousinsufficiency
andlymphaticinsufficiencyareassociatedwithchroniculcers.Abreakdowninthelymphaticsystempredisposestoinfectionandcompromiseswoundhealing.20-23Furthermore,MacdonaldandMayrovitz22findthatmanaginglymphedemaatawoundsiteenhancesthewound-healingprocessinindividualswithandwithoutvenousinsufficiency,furtherstrengtheningthelinkbetweenproperlymphaticflowandwoundhealing.
Currenttreatmentprotocolsforchronicwoundsincludehyperbaricoxygentherapy,infectiousdiseasemanagement,nutrition,painmanagement,surgeryandeducation.However,duetotheimportantrelationshipbetweenproperlymphaticflow,bloodflowandwoundhealing,itcanbehypothesizedthatOMTaimedatimprovinglymphaticflowwillhelpinthepreventionofchronicwounds.24,25Thesetechniquesincludethepedalpump,thoracicpump,effleurageandpectorallift.
Hyperhidrosis and atopic dermatitis. Hyperhidrosisisacommondisorderthatcauseshyperfunctioningofthesudomotorsweatcontrolsystem.Thisresultsinincreasedsweatsecretionatthepalms,axillaeandsoles.26Primaryhyperhidrosisappearsinadolescenceandisthoughttobeanautonomicdominantdisorder.27Secondaryhyperhidrosis,however,iscausedbyothermedicalconditions.Theexactpathophysiologyofhyperhidrosisisunderinvestigation.However,alackofsweatingatnightsuggestsastrongemotionalcomponent.28Additionalresearchpointstolocalizedhyper-functioningofsympatheticfiberspassingthroughtheT2andT3ganglia.29Atopicdermatitisisadermatologicconditioncharacterizedbyxerosis,lichenification,andeczematouslesions.30Thepathogenesisofthediseasehasbeenlinkedtoageneticloss-of-functionmutationinfilaggrin,infectionwithS. aureus,andmostrecently,anautonomicnervoussystemdysfunction.31Anotherstudyfindsthatatopicsubjectsexhibitanoveractivesympatheticresponsetoitchingandscratching,whiletheparasympathetictoneispersistentlyandrigidlyelevated,indicatingalackofadaptabilityinresponsetostress.31
Currenttreatmentforhyperhidrosisincludesprescriptionandover-the-counterantiperspirants,iontophoresis,oralmedicationsandbotulinumtoxininjections.Thoseforatopicdermatitisareequallyvariedandincludetopicalcorticosteroidcreams,antibiotics,oralantihistamines,phototherapyandimmunomodulators.However,OMTtechniquessuchascraniosacralandribraising,whichtargettheautonomicnervoussystem,mayaidintreatingthesepatients.

Vol. 23, No. 4, December 2013 • The American Academy of Osteopathy Journal Page 37
Sympatheticnervefibersemergefromthoracolumbarvertebrae,andtheirganglialieintheparavertebralregion.Duetotheproximityofthesympatheticganglion,OMTdirectedtowardthevertebralbodiesandribsprotrudingfromthemmaynormalizesympatheticoutputattheleveloftheganglion.Occipitalrelease,aformofmyofascialrelease,mayalsobeuseful,asitaugmentstheoutputoftheparasympatheticnervoussystemandmayhelptorestorebalance.Finally,cranialmanipulationmayalsohaveeffectsontheoutputofsympatheticactivity.1
Scleroderma. Sclerodermaisararediseasemarkedbydamagetothecellsliningthewallsofsmallarteriesandanabnormalbuildupofscartissue.32Thisdisordercanbelocalizedtothehandsandfaceorcausesystemicsclerosisandbeassociatedwithcalcinosis,Raynaud’sphenomenon,esophagealmotilitydysfunction,sclerodactylyandtelangiectasia.Thepathogenesisofsclerodermaisnotknownbuthasbeenattributedtoautoimmunitywithageneticabnormalitytriggeredbypossibleenvironmentalfactors.33Currentresearchhasalsonotedthatscleroticcutaneouslesionsshowselectivedilationofsomelymphaticvesselsanddestructionofothers.33Whilethereasonforthisselectivityisnotknown,astrongcorrelationexistsbetweenthesefindingsandtheedematousphaseandsubsequentfibrosis.32-34
Ithasbeenpostulatedthatdilationoftheselymphaticvesselsoverloadsthelymphaticsviaeitheranincreaseininterstitialfluidduetothepathologicprocessand/ortheoverallreducedcapacityoflymphdrainagecausedbythedecreasednumberoflymphvessels.33Assuch,itcanbepostulatedthattheuseofOMTtechniques,suchasthepedalpump,pectorallift,effleurageandthoracicpumpcouldaidintheclearanceoflymphaticfluidandthusdelaytheprogressionofdisease.
Conclusion
Asthefieldofosteopathicmedicinecontinuestogrowandexpand,itisonlynaturalthatosteopathicphysicianswillcontinuetoenterotherspecialtiesandbringwiththemuniquetreatmentmodalitiestophysiologicaldiseases.Asdiscussed,onesuchfieldofmedicineinwhichtheosteopathicapproachhasthepotentialtobeextremelyusefulisdermatology.
Theauthorsmaintainthatcommondermatologicconditionssuchasacnevulgaris,psoriasisandatopicdermatitis,aswellasotherdisorders,includingchronicwounds,hyperhidrosis,andscleroderma,canbetreatedaseffectivelyifnotmoreeffectivelythroughthisintegrationofOMTintodermatology,ascommonly
practiced.Thoughtheauthorshavenothaddirectexperiencewithpatientswithdermatologicdisorders,theybelievethatthroughthisunion,physicianswillbeabletoprovidetheultimateincomprehensivepatientcare.FurtherstudiesconcerningtheapplicationofOMTinthetreatmentofdermatologicdisordersareneededinordertoconfirmsuchbenefits.
Finally,itmustbeemphasizedthatdermatologyisaclinicalspecialtythatexemplifiesthebestaspectsoftheosteopathicmedicalprofession.35Infact,allopathicphysiciansshouldbeencouragedtoincorporatesuchapproachesintheirowntreatmentpractices.Theymaybemissingmajoreffectivemodalitiesintheirusualapproachtodermatologicdisorders.
References1. CampbellSM,WinkelmannRR,WalkowskiS.Osteopathic
manipulativetreatment:novelapplicationtodermatologicaldisease.J Clin Aesthet Dermatol. 2012;5(10):24-32.
2. TidmanMJ.Prompttreatmentofacneimprovesqualityoflife.Practitioner. Jun2012;256(1752):15-17,12.
3. TaylorM,GonzalezM,PorterR.Pathwaystoinflammation:acnepathophysiology.Eur. J. Dermatol. 2011;21(3):323-333.
4. SmithRN,MannNJ,BraueA,MakelainenH,VarigosGA.Theeffectofahigh-protein,lowglycemic-loaddietversusaconventional,highglycemic-loaddietonbiochemicalparametersassociatedwithacnevulgaris:arandomized,investigator-masked,controlledtrial.J. Am. Acad. Dermatol. 2007;57(2):247-256.
5. FerdowsianHR,LevinS.Doesdietreallyaffectacne?Skin Therapy Letter. 2010;15(3):1-2,5.
6. SpencerEH,FerdowsianHR,BarnardND.Dietandacne:areviewoftheevidence.Int. J. Dermatol. 2009;48(4):339-347.
7. PalatsiR,ReinilaM,KivinenS.PituitaryfunctionandDHEA-SinmaleacneandDHEA-S,prolactinandcortisolbeforeandafteroralcontraceptivetreatmentinfemaleacne.Acta Derm. Venereol. 1986;66(3):225-230.
8. FischerH.SkinandtheAutonomicNervousSystem.Arch. Phys. Ther. (Leipz.). 1963;15:137-152.
9. PetersEM,LiezmannC,KlappBF,KruseJ.Theneuroimmuneconnectioninterfereswithtissueregenerationandchronicinflammatorydiseaseintheskin.Ann. N. Y. Acad. Sci. 2012;1262:118-126.
10. EhrenfeuchterW.Softtissue/ArticulatoryApproach.Foundations of Osteopathic Medicine.3ed.Philadelphia,Pennsylvania:LippincottWilliams&Wilkins;2011:763-785.
11. KorotkovK,ShelkovO,ShevtsovA,etal.StressreductionwithosteopathyassessedwithGDVelectrophotonicimaging:effectsofosteopathytreatment.J. Altern. Complement. Med. 2012;18(3):251-257.
12. ChaitowL.OsseousandSoftTissueApproaches.Cranial Manipulation Theory and Practice.London,England:ChurchillLivingstone;1999:116.
13. SchanderA,DowneyHF,HodgeLM.Lymphaticpumpmanipulationmobilizesinflammatorymediatorsintolymphaticcirculation.Exp Biol Med (Maywood). 2012;237(1):58-63.
14. HellerMM,LeeES,KooJY.Stressasaninfluencingfactorinpsoriasis.Skin Therapy Letter. 2011;16(5):1-4.
continued on page 42

Page 38 The American Academy of Osteopathy Journal • Vol. 23, No. 4, December 2013
Archer, Jamie B. DOInthehandsofanangel.Vol.23,No.2,June2013,pp.19-22
Baker, Charity D. DOOsteopathicmanipulativetreatmentforLymedisease-inducedBell’spalsy:acasestudy.Vol.23,No.1,March2013,pp.12-15
Baker, Joshua P. DO, FAAFPTreatment of a posterior rib utilizinga multimodal sequence of osteopathicmanipulativetreatments.Vol.23,No.2,June2013,pp.10-13
UseofOMTtotreatpatientwithRamsayHunt syndromeandHIV:a case study.Vol.23,No.4,Dec.2013,pp.8-12
OsteopathicmanipulativetreatmentforLymedisease-inducedBell’spalsy:acasestudy.Vol.23,No.1,March2013,pp.12-15
Berkowitz, Murray R. DO, MA, MS, MPHRef lections on our recent past andthoughtsaboutour future.Vol. 23,No.2,June2013,pp.4,7
View from the Pyramids: New gradu-ate medical education opportunitiesfound—andlost.Vol.23,Issue1,March2013,pp.4,7
Bertucci, W. PhDStabilometric platform as a diagnosissupport for pain? Example of chroniclowbackpain.Vol.23,No.1,March2013,pp.44-45
Blumer, Janice U. DODistance learningandosteopathicma-nipulativemedicine.Vol.23,No.2,June2013,p.9
The extinction of manipulative medi-cine?Vol.23,No.3,Sept.2013,p.5
Burns, Denise K. DO, FAAOOsteopathic management of a familywithinheritedcervicaldystonia.Vol.23,No.3,Sept.2013,pp.30-37
Byrnes, Jr., Thomas DOBook Review—Charlotte Weaver: Pio-neer in Cranial Osteopathy, Edited byMargaretSorrell,DO.Vol.23,No.3,Sept.2013,pp.12-13
Capalbo, Gina OMS IVOsteopathic manipulative treatmentofpesanserinebursitisusingthetripletechnique:acasereport.Vol. 23,No. 1,March2013,pp.34-38
Chan, Vivian OMS IITheeffectoftheStudentAmericanAcad-emyofOsteopathy summerpreceptor-ship program on students’ perceptionofosteopathicmanipulative treatment.Vol.23,No.4,Dec.2013,pp.14-20
Channell, Millicent King DO, FAAOEvaluatingteachingmethodsandassess-menttoolsofhighvelocitylowamplitudetechniques for undergraduate osteo-pathic manipulative treatment of thespine.Vol.23,No.1,March2013,pp.24-32
Chmielewski, Richard MS, DO, FA-CEPOsteopathic manipulative treatmentofpesanserinebursitisusingthetripletechnique:acasereport.Vol. 23,No. 1,March2013,pp.34-38
Cloud, John BS, MS IVFractureasaresultofvolcanoboarding.Vol.23,No.3,Sept.2013,pp.15-20
Covington, J. Daren OMS IVReliefofpersistentjawpainwiththeuseof osteopathic manipulative medicine.Vol.23,No.2,June2013,pp.15-17
Crow, Wm. Thomas DO, FAAOSensoryintegrationsyndromeordevel-opmentalcoordinationdisorder:acasereport. Vol. 23, No. 1, March 2013, pp.8-10,15
Cymet, Tyler DOFractureasaresultofvolcanoboarding.Vol.23,No.3,Sept.2013,pp.15-20
Davidson, Ross BS, OMS IIFractureasaresultofvolcanoboarding.Vol.23,No.3,Sept.2013,pp.15-20
Deason, J. ScB, MS, PhG, DOFromtheArchives:StructureandFunc-tion.Vol.23,No.3,Sept.2013,pp.22-24
Ely, Rachel MHA, OMS IIITreatment of a posterior rib utilizinga multimodal sequence of osteopathicmanipulativetreatments.Vol.23,No.2,June2013,pp.10-13
Flaum, Theodore B. DOUsefulnessof video learning forosteo-pathic manipulative medicine (OMM)techniquesintheeducationalandclini-calsetting.Vol.23,No.3,Sept.2013,pp.24-30
Huard, Yannick DO, ScMStabilometric platform as a diagnosissupport for pain? Example of chroniclowbackpainVol.23,No.1,March2013,pp.44-45
Jung, Min-Kyung PhDUsefulnessof video learning forosteo-pathic manipulative medicine (OMM)techniquesintheeducationalandclini-calsetting.Vol.23,No.3,Sept.2013,pp.24-30
Kravchenko, Tamara I. PhD, DOThe liquorodynamic model of the pri-maryrespiratorymechanism.Vol.23,No.2,June2013,pp.24-29
Lipton, James A. DO, CSPOMM, FAAO, FAAPMR, DAOBPMRTheuseoforthoticsinthereductionofself-reported pain scores in a VeteransAffairspopulation:aretrospectivestudy.Vol.23,No.3,Sept.2013,pp.9-12
Reliefofpersistentjawpainwiththeuseof osteopathic manipulative medicine.Vol.23,No.2,June2013,pp.15-17
Litman, Randy G. DO, FAAONormalization of thoraco-abdominalfascialandautonomictone:acasestudyforthediagnosisandtreatmentofatypi-calchestpain.Vol.23,No.1,March2013,pp.20-22
Sequelae of traumatic closed-head in-jury:acasereportofa71-year-oldmaleseen40yearslater.Vol.23,No.1,March2013,pp.17-18,22
Mancini, Jayme D. DO, PhD, FAWMOsteopathic management of a familywithinheritedcervicaldystonia.Vol.23,No.3,Sept.2013,pp.30-37
Marberry, Kevin MDFractureasaresultofvolcanoboarding.Vol.23,No.3,Sept.2013,pp.15-20
McCaffrey, Kate DOMillenialTimes:Womeninosteopathicmedicine.Vol.23,No.1,March2013,pp.5,7
ViewfromthePyramids:Inyourhandsnow!Volume23,Issue3,September2013,p.4
View from the Pyramids: It takes anosteopathicvillage.Vol.23,No.4,Dec.2013,p.4
View from the Pyramids: Osteopathicmedicineandspirituality.Vol.23,No.2,June2013,p.7
Meghpara, Melissa K. OMS IIIUsefulnessof video learning forosteo-pathic manipulative medicine (OMM)techniquesintheeducationalandclini-calsetting.Vol.23,No.3,Sept.2013,pp.24-30
The AAO Journal 2013 IndexBY AUTHOR

Vol. 23, No. 4, December 2013 • The American Academy of Osteopathy Journal Page 39
Michunovich, Ana M. BS, OMS IIIPotentialnewdimensions indermatol-ogy: theosteopathic approach to cuta-neousdisease.Vol.23,No.4,Dec.2013,pp.34-37
Moskalenko, Yuri E. DSc, DO (Hon.)The liquorodynamic model of the pri-maryrespiratorymechanism.Vol.23,No.2,June2013,pp.24-29
Palmer, Tiffany R. BS, MS IVFractureasaresultofvolcanoboarding.Vol.23,No.3,Sept.2013,pp.15-20
Pena, Nicole OMS IVOsteopathic manipulative treatmentofpesanserinebursitisusingthetripletechnique:acasereport.Vol. 23,No. 1,March2013,pp.34-38
Pribadi, Krishnahari S. MDThe application of the cranial conceptin the investigationofbafflingmedicaldisordersand their treatment:a syner-gopathicmedicaldiseasemodel.Vol.23,No.4,Dec.2013,pp.20-33
Stern, Robert MDPotentialnewdimensions indermatol-ogy: theosteopathic approach to cuta-neousdisease.Vol.23,No.4,Dec.2013,pp.34-37
Terzella, Michael J. DOUsefulnessof video learning forosteo-pathic manipulative medicine (OMM)techniquesintheeducationalandclini-calsetting.Vol.23,No.3,Sept.2013,pp.24-30
Uhrig, Lawrence DOAtaleoftwosisters:anosteopathicstory.Vol.23,No.4,Dec.2013,p.7
Vardy, Terence C. DOThe liquorodynamic model of the pri-maryrespiratorymechanism.Vol.23,No.2,June2013,pp.24-29
Vazzana, Kathleen M. OMS IVTheeffectoftheStudentAmericanAcad-emyofOsteopathy summerpreceptor-ship program on students’ perceptionofosteopathicmanipulative treatment.Vol.23,No.4,Dec.2013,pp.14-20
Weinstein, Gustav B. PhDThe liquorodynamic model of the pri-maryrespiratorymechanism.Vol.23,No.2,June2013,pp.24-29
Wenzel, Charles JD, OMS IVTheeffectoftheStudentAmericanAcad-emyofOsteopathy summerpreceptor-ship program on students’ perceptionofosteopathicmanipulative treatment.Vol.23,No.4,Dec.2013,pp.14-20
Worden, Katherine A. DO, MSLookingbackandlookingahead.Vol.23,No.4,Dec.2013,p.5
Yao, Sheldon C. DOTheeffectoftheStudentAmericanAcad-emyofOsteopathy summerpreceptor-ship program on students’ perceptionofosteopathicmanipulative treatment.Vol.23,No.4,Dec.2013,pp.14-20
Usefulnessof video learning forosteo-pathic manipulative medicine (OMM)techniquesintheeducationalandclini-calsetting.Vol.23,No.3,Sept.2013,pp.24-30
AcnePotentialnewdimensions indermatol-ogy: theosteopathic approach to cuta-neousdisease;Michunovich,AnaM.BS,OMSIII;RobertStern,MDVol.23,No.4,Dec.2013,pp.34-37;
Alzheimers’s diseaseThe application of the cranial conceptin the investigationofbafflingmedicaldisordersand their treatment:a syner-gopathicmedicaldiseasemodel;Pribadi,KrishnahariS.MD;Vol.23,No.4,Dec.2013,pp.20-33;
Angel’s RestInthehandsofanangel;Archer,JamieB.DO;Vol.23,No.2,June2013,pp.19-22;
Atopic dermatitisPotentialnewdimensions indermatol-ogy: theosteopathic approach to cuta-neousdisease;Michunovich,AnaM.BS,OMSIII;RobertStern,MDVol.23,No.4,Dec.2013,pp.34-37;
A.T. Still UniversityLookingBackandLookingAhead;Wor-den,KatherineA.DO,MS;Vol.23,No.4,Dec.2013,p.5;
Book reviewBook Review—Charlotte Weaver: Pio-neer in Cranial Osteopathy, Edited byMargaretSorrell,DO;Byrnes,Jr.,ThomasDO;Vol.23,No.3,Sept.2013,pp.12-13;
Case studyNormalization of thoraco-abdominalfascialandautonomictone:acasestudyforthediagnosisandtreatmentofatypi-cal chest pain; Litman, Randy G. DO,FAAO; Vol. 23, No. 1, March 2013, pp.20-22;
Osteopathic management of a familywithinheritedcervicaldystonia;Burns,DeniseK.DO,FAAO;JaymeD.Mancini,
DO, PhD, FAWMVol. 23, No. 3, Sept.2013,pp.30-37;
OsteopathicmanipulativetreatmentforLymedisease-inducedBell’spalsy:acasestudy; Baker, CharityD.DO; Joshua P.Baker,DO, FAAPVol. 23,No. 1,March2013,pp.12-15;
Osteopathic manipulative treatmentofpesanserinebursitisusingthetripletechnique:acasereport;Capalbo,GinaOMSIV;RichardChmielewski,MS,DO,FACEP;NicolePena,OMSIVVol.23,No.1,March2013,pp.34-38;
Sensoryintegrationsyndromeordevel-opmentalcoordinationdisorder:acasereport;Crow,Wm.ThomasDO,FAAO;Vol.23,No.1,March2013,pp.8-10,15;
Sequelae of traumatic closed-head in-jury:acasereportofa71-year-oldmaleseen 40 years later; Litman, Randy G.DO, FAAO;Vol. 23, No. 1,March 2013,pp.17-18,22;
Cell theoryFromtheArchives:StructureandFunc-tion;Deason,J.ScB,MS,PhG,DO;Vol.23,No.3,Sept.2013,pp.22-24;
Cerro Negro, NicaraguaFractureasaresultofvolcanoboarding;Cloud,JohnBS,MSIV;TiffanyR.Palmer,BS,MSIV;RossDavidson,BS,OMSII;TylerCymet,DO;KevinMarberry,MDVol.23,No.3,Sept.2013,pp.15-20;
Charlotte WeaverBook Review—Charlotte Weaver: Pio-neer in Cranial Osteopathy, Edited byMargaretSorrell,DO;Byrnes,Jr.,ThomasDO;Vol.23,No.3,Sept.2013,pp.12-13;
Chest painNormalization of thoraco-abdominalfascialandautonomictone:acasestudyforthediagnosisandtreatmentofatypi-cal chest pain; Litman, Randy G. DO,FAAO; Vol. 23, No. 1, March 2013, pp.20-22;
Chronic woundsPotentialnewdimensions indermatol-ogy: theosteopathic approach to cuta-neousdisease;Michunovich,AnaM.BS,OMSIII;RobertStern,MDVol.23,No.4,Dec.2013,pp.35-39;
Clinical ExposureTheeffectoftheStudentAmericanAcad-emyofOsteopathySummerpreceptor-ship program on students’ perceptionofosteopathicmanipulative treatment;Vazzana, KathleenM. OMS IV; VivianChan,OMSII;CharlesWenzel,JD,OMSIV;andSheldonC.Yao,DOVol.23,No.4,Dec.2013,pp.14-20;
BY SUBJECT

Page 40 The American Academy of Osteopathy Journal • Vol. 23, No. 4, December 2013
Closed-head injurySequelae of traumatic closed-head in-jury:Acasereportofa71-year-oldmaleseen 40 years later; Litman, Randy G.DO, FAAO;Vol. 23, No. 1,March 2013,pp.17-18,22;
Cranial osteopathyBook Review—Charlotte Weaver: Pio-neer in Cranial Osteopathy, Edited byMargaretSorrell,DO;Byrnes,Jr.,ThomasDO;Vol.23,No.3,Sept.2013,pp.12-13;
Craniosacral Acupuncture Palpatory MethodThe application of the cranial conceptin the investigationofbafflingmedicaldisordersand their treatment:a syner-gopathicmedicaldiseasemodel;Pribadi,KrishnahariS.MD;Vol.23,No.4,Dec.2013,pp.20-33;
Craniosacral Allergy Screening TestThe application of the cranial conceptin the investigationofbafflingmedicaldisordersand their treatment:a syner-gopathicmedicaldiseasemodel;Pribadi,KrishnahariS.MD;Vol.23,No.4,Dec.2013,pp.20-33;
Craniosacral Digital Diagnostic MethodThe application of the cranial conceptin the investigationofbafflingmedicaldisordersand their treatment:a syner-gopathicmedicaldiseasemodel;Pribadi,KrishnahariS.MD;Vol.23,No.4,Dec.2013,pp.20-33;
Craniosacral Nutritional Assessment MethodThe application of the cranial conceptin the investigationofbafflingmedicaldisordersand their treatment:a syner-gopathicmedicaldiseasemodel;Pribadi,KrishnahariS.MD;Vol.23,No.4,Dec.2013,pp.20-33;
Craniosacral Pathological ProfileThe application of the cranial conceptin the investigationofbafflingmedicaldisordersand their treatment:a syner-gopathicmedicaldiseasemodel;Pribadi,KrishnahariS.MD;Vol.23,No.4,Dec.2013,pp.20-33;
Craniosacral Tele-Diagnostic MethodThe application of the cranial conceptin the investigationofbafflingmedicaldisordersand their treatment:a syner-gopathicmedicaldiseasemodel;Pribadi,KrishnahariS.MD;Vol.23,No.4,Dec.2013,pp.20-33;
DermatologyPotentialnewdimensions indermatol-ogy: theosteopathic approach to cuta-neousdisease;Michunovich,AnaM.BS,
OMSIII;RobertStern,MDVol.23,No.4,Dec.2013,pp.34-37;
Developmental coordination disor-derSensoryintegrationsyndromeordevel-opmentalcoordinationdisorder:acasereport;Crow,Wm.ThomasDO,FAAO;Vol.23,No.1,March2013,pp.8-10,15;
DiagnosisStabilometric platform as a diagnosissupport for pain? Example of chroniclowbackpain;Bertucci,W.PhD;YannickHuard, DO, ScMVol. 23, No. 1,March2013,pp.44-45;
Normalization of thoraco-abdominalfascialandautonomictone:acasestudyforthediagnosisandtreatmentofatypi-cal chest pain; Litman, Randy G. DO,FAAO; Vol. 23, No. 1, March 2013, pp.20-22;
Distance learningDistance learningandosteopathicma-nipulative medicine; Blumer, Janice U.DO;Vol.23,No.2,June2013,p.9;
Edna LayLookingBackandLookingAhead;Wor-den,KatherineA.DO,MS;Vol.23,No.4,Dec.2013,p.5;
Extinction of manipulative medicineThe extinction of manipulative medi-cine?;Blumer,JaniceU.DO;Vol.23,No.3,Sept.2013,p.5;
From the archivesFromtheArchives:StructureandFunc-tion;Deason,J.ScB,MS,PhG,DO;Vol.23,No.3,Sept.2013,pp.22-24;
Guillain-Barre syndromeThe application of the cranial conceptin the investigationofbafflingmedicaldisordersand their treatment:a syner-gopathicmedicaldiseasemodel;Pribadi,KrishnahariS.MD;Vol.23,No.4,Dec.2013,pp.20-33;
HeadacheInthehandsofanangel;Archer,JamieB.DO;Vol.23,No.2,June2013,pp.19-22;
High velocity low amplitude tech-niquesEvaluating teaching methods and as-sessment tools of high velocity lowamplitude techniques for undergradu-ateosteopathicmanipulativetreatmentof the spine; Channell, Millicent KingDO, FAAO;Vol. 23, No. 1,March 2013,pp.24-32;
HIVUseofOMTtoTreatPatientwithRamsayHuntSyndromeandHIV:ACaseStudy;
Baker,JoshuaP.DO,FAAFP;Vol.23,No.4,Dec.2013,pp.8-12;
HyperhidrosisPotentialnewdimensions indermatol-ogy: theosteopathic approach to cuta-neousdisease;Michunovich,AnaM.BS,OMSIII;RobertStern,MDVol.23,No.4,Dec.2013,pp.34-37;
Inherited cervical dystoniaOsteopathic management of a familywithinheritedcervicaldystonia;Burns,DeniseK.DO,FAAO;JaymeD.Mancini,DO, PhD, FAWMVol. 23, No. 3, Sept.2013,pp.30-37;
Jaw painReliefofpersistentjawpainwiththeuseof osteopathic manipulative medicine;Covington, J. DarenOMS IV; JamesA.Lipton,DO,FAAO,FAAPMRVol.23,No.2,June2013,pp.15-17;
Koch’s postulatesThe application of the cranial conceptin the investigationofbafflingmedicaldisordersand their treatment:a syner-gopathicmedicaldiseasemodel;Pribadi,KrishnahariS.MD;Vol.23,No.4,Dec.2013,pp.20-33;
Leaky gut syndromeThe application of the cranial conceptin the investigationofbafflingmedicaldisordersand their treatment:a syner-gopathicmedicaldiseasemodel;Pribadi,KrishnahariS.MD;Vol.23,No.4,Dec.2013,pp.20-33;
Liquordynamic modelTheliquorodynamicmodeloftheprima-ryrespiratorymechanism;Kravchenko,TamaraI.PhD,DO;YuriE.Moskalenko,DSc, DO (Hon.); Gustav B.Weinstein,PhD;TerenceC.Vardy,DOVol.23,No.2,June2013,pp.24-29;
Long-term care benefitsAtaleoftwosisters:anosteopathicstory;Uhrig,LawrenceDO;Vol.23,No.4,Dec.2013,p.7;
Low back painStabilometric platform as a diagnosissupport for pain? Example of chroniclowbackpain;Bertucci,W.PhD;YannickHuard, DO, ScMVol. 23, No. 1,March2013,pp.44-45;
Lyme disease-induced Bell’s palsyOsteopathicmanipulativetreatmentforLymedisease-inducedBell’spalsy:acasestudy; Baker, CharityD.DO; Joshua P.Baker,DO, FAAPVol. 23,No. 1,March2013,pp.12-15;

Vol. 23, No. 4, December 2013 • The American Academy of Osteopathy Journal Page 41
Margaret SorrellBook Review—Charlotte Weaver: Pio-neer in Cranial Osteopathy, Edited byMargaretSorrell,DO;Byrnes,Jr.,ThomasDO;Vol.23,No.3,Sept.2013,pp.12-13;
Medical EducationTheeffectoftheStudentAmericanAcad-emyofOsteopathySummerpreceptor-ship program on students’ perceptionofosteopathicmanipulative treatment;Vazzana, KathleenM. OMS IV; VivianChan,OMSII;CharlesWenzel,JD,OMSIV;andSheldonC.Yao,DOVol.23,No.4,Dec.2013,pp.14-20;
View From the Pyramids: New gradu-ate medical education opportunitiesfound—and lost; Berkowitz,MurrayR.Do,MA,MS,MPH;Vol.23,Issue1,March2013,pp.4,7;
Millenial TimesMillenialTimes:Womeninosteopathicmedicine;McCaffrey,KateDO;Vol.23,No.1,March2013,pp.5,7;
Multimodal sequenceTreatment of a posterior rib utilizinga multimodal sequence of osteopathicmanipulative treatments;Baker, JoshuaP.DO,FAAFP;RachelEly,MHA,OMSIIIVol.23,No.2,June2013,pp.10-13;
NYIT-COMTheeffectoftheStudentAmericanAcad-emyofOsteopathySummerpreceptor-ship program on students’ perceptionofosteopathicmanipulative treatment;Vazzana, KathleenM. OMS IV; VivianChan,OMSII;CharlesWenzel,JD,OMSIV;andSheldonC.Yao,DOVol.23,No.4,Dec.2013,pp.14-20;
Usefulnessof video learning forosteo-pathic manipulative medicine (OMM)techniques in the educational andclinicalsetting;Flaum,TheodoreB.DO;MelissaK.Meghpara,OMSIII;MichaelJ.Terzella,DO;Min-Kyung Jung, PhD;SheldonC.Yao,DOVol.23,No.3,Sept.2013,pp.24-30;
OrthoticsTheuseoforthoticsinthereductionofself-reported pain scores in a VeteransAffairspopulation:aretrospectivestudy;Lipton,JamesA.DO,CSPOMM,FAAO,FAAPMR, DAOBPMR; Vol. 23, No. 3,Sept.2013,pp.9-12;
Osteopathic Manipulative TreatmentTheeffectoftheStudentAmericanAcad-emyofOsteopathySummerpreceptor-ship program on students’ perceptionofosteopathicmanipulative treatment;Vazzana, KathleenM. OMS IV; VivianChan,OMSII;CharlesWenzel,JD,OMS
IV;andSheldonC.Yao,DOVol.23,No.4,Dec.2013,pp.14-20;
Parkinson’s diseaseThe application of the cranial conceptin the investigationofbafflingmedicaldisordersand their treatment:a syner-gopathicmedicaldiseasemodel;Pribadi,KrishnahariS.MD;Vol.23,No.4,Dec.2013,pp.22-34;
Pes anserine bursitisOsteopathic manipulative treatmentofpesanserinebursitisusingthetripletechnique:Acasereport;Capalbo,GinaOMSIV;RichardChmielewski,MS,DO,FACEP;NicolePena,OMSIVVol.23,No.1,March2013,pp.34-38;
Posterior ribTreatment of a posterior rib utilizinga multimodal sequence of osteopathicmanipulative treatments;Baker, JoshuaP.DO,FAAFP;RachelEly,MHA,OMSIIIVol.23,No.2,June2013,pp.10-13;
PreclinicalTheeffectoftheStudentAmericanAcad-emyofOsteopathySummerpreceptor-ship program on students’ perceptionofosteopathicmanipulative treatment;Vazzana, KathleenM. OMS IV; VivianChan,OMSII;CharlesWenzel,JD,OMSIV;andSheldonC.Yao,DOVol.23,No.4,Dec.2013,pp.14-20;
Primary respiratory mechanism (PRM)Theliquorodynamicmodeloftheprima-ryrespiratorymechanism;Kravchenko,TamaraI.PhD,DO;YuriE.Moskalenko,DSc, DO (Hon.); Gustav B.Weinstein,PhD;TerenceC.Vardy,DOVol.23,No.2,June2013,pp.24-29;
PsoriasisPotentialnewdimensions indermatol-ogy: theosteopathic approach to cuta-neousdisease;Michunovich,AnaM.BS,OMSIII;RobertStern,MDVol.23,No.4,Dec.2013,pp.35-39;
Ramsay Hunt SyndromeUseofOMTtoTreatPatientwithRamsayHuntSyndromeandHIV:ACaseStudy;Baker,JoshuaP.DO,FAAFP;Vol.23,No.4,Dec.2013,pp.8-12;
ReflectionsLookingBackandLookingAhead;Wor-den,KatherineA.DO,MS;Vol.23,No.4,Dec.2013,p.5;
Ref lections on our recent past andthoughts about our future; Berkowitz,MurrayR.DO,MA,MS,MPH;Vol. 23,No.2,June2013,pp.4,7;
Saint’s RestInthehandsofanangel;Archer,JamieB.DO;Vol.23,No.2,June2013,pp.19-22;
SclerodermaPotentialnewdimensions indermatol-ogy: theosteopathic approach to cuta-neousdisease;Michunovich,AnaM.BS,OMSIII;RobertStern,MDVol.23,No.4,Dec.2013,pp.35-39;
Self-reported pain scoresTheuseoforthoticsinthereductionofself-reported pain scores in a VeteransAffairspopulation:aretrospectivestudy;Lipton,JamesA.DO,CSPOMM,FAAO,FAAPMR, DAOBPMR; Vol. 23, No. 3,Sept.2013,pp.9-12;
Sensory integration syndromeSensoryintegrationsyndromeordevel-opmentalcoordinationdisorder:Acasereport;Crow,Wm.ThomasDO,FAAO;Vol.23,No.1,March2013,pp.8-10,15;
SpiritualityView from the Pyramids: Osteopathicmedicine and sprituality; McCaffrey,KateDO;Vol.23,No.2,June2013,p.7;
StabilometricStabilometric platform as a diagnosissupport for pain? Example of chroniclowbackpain;Bertucci,W.PhD;YannickHuard, DO, ScMVol. 23, No. 1,March2013,pp.44-45;
Still, A.T.Inthehandsofanangel;Archer,JamieB.DO;Vol.23,No.2,June2013,pp.19-22;
Structure and functionFromtheArchives:StructureandFunc-tion;Deason,J.ScB,MS,PhG,DO;Vol.23,No.3,Sept.2013,pp.22-24;
SwingInthehandsofanangel;Archer,JamieB.DO;Vol.23,No.2,June2013,pp.19-22;
Synergopathic Herbal FormulasThe application of the cranial conceptin the investigationofbafflingmedicaldisordersand their treatment:a syner-gopathicmedicaldiseasemodel;Pribadi,KrishnahariS.MD;Vol.23,No.4,Dec.2013,pp.20-33;
Teaching methodsEvaluating teaching methods and as-sessment tools of high velocity lowamplitude techniques for undergradu-ateosteopathicmanipulativetreatmentof the spine; Channell, Millicent KingDO, FAAO;Vol. 23, No. 1,March 2013,pp.24-32;

Page 42 The American Academy of Osteopathy Journal • Vol. 23, No. 4, December 2013
Thoraco-abdominal fascial and auto-nomic toneNormalization of thoraco-abdominalfascialandautonomictone:Acasestudyforthediagnosisandtreatmentofatypi-cal chest pain; Litman, Randy G. DO,FAAO; Vol. 23, No. 1, March 2013, pp.20-22;
Triple techniqueOsteopathic manipulative treatmentofpesanserinebursitisusingthetripletechnique:Acasereport;Capalbo,GinaOMSIV;RichardChmielewski,MS,DO,FACEP;NicolePena,OMSIVVol.23,No.1,March2013,pp.34-38;
Upledger-Pribadi’s signThe application of the cranial conceptin the investigationofbafflingmedicaldisordersand their treatment:a syner-gopathicmedicaldiseasemodel;Pribadi,KrishnahariS.MD;Vol.23,No.4,Dec.2013,pp.20-33;
Veterans AffairsTheuseoforthoticsinthereductionofself-reported pain scores in a VeteransAffairspopulation:aretrospectivestudy;Lipton,JamesA.DO,CSPOMM,FAAO,FAAPMR, DAOBPMR; Vol. 23, No. 3,Sept.2013,pp.9-12;
Video learningUsefulnessof video learning forosteo-pathic manipulative medicine (OMM)techniques in the educational andclinicalsetting;Flaum,TheodoreB.DO;MelissaK.Meghpara,OMSIII;MichaelJ.Terzella,DO;Min-Kyung Jung, PhD;SheldonC.Yao,DOVol.23,No.3,Sept.2013,pp.24-30;
View from the PyramidsViewfromthePyramids:Ittakesanos-teopathic village; McCaffrey, Kate DO;Vol.23,No.4,Dec.2013,p.4;
ViewfromthePyramids:Inyourhandsnow!;McCaffrey, KateDO;Volume 23,Issue3,September2013,p.4;
View From the Pyramids: New gradu-ate medical education opportunitiesfound—and lost; Berkowitz,MurrayR.Do,MA,MS,MPH;Vol.23,Issue1,March2013,pp.4,7;
Volcano boardingFractureasaresultofvolcanoboarding;Cloud,JohnBS,MSIV;TiffanyR.Palmer,BS,MSIV;RossDavidson,BS,OMSII;TylerCymet,DO;KevinMarberry,MDVol.23,No.3,Sept.2013,pp.15-20;
Women in osteopathic medicineMillenialTimes:Womeninosteopathicmedicine;McCaffrey,KateDO;Vol.23,No.1,March2013,pp.5,7;
15. KryczekI,BruceAT,GudjonssonJE,etal.InductionofIL-17+TcelltraffickinganddevelopmentbyIFN-gamma:mechanismandpathologicalrelevanceinpsoriasis.J. Immunol. 2008;181(7):4733-4741.
16. Buske-KirschbaumA,EbrechtM,KernS,HellhammerDH.EndocrinestressresponsesinTH1-mediatedchronicinflammatoryskindisease(psoriasisvulgaris)--dotheyparallelstress-inducedendocrinechangesinTH2-mediatedinflammatorydermatoses(atopicdermatitis)?Psychoneuroendocrinology. 2006;31(4):439-446.
17. SenCK,GordilloGM,RoyS,etal.Humanskinwounds:amajorandsnowballingthreattopublichealthandtheeconomy.Wound Repair Regen. Nov-2009;17(6):763-771.
18. FonderMA,LazarusGS,CowanDA,Aronson-CookB,KohliAR,MamelakAJ.Treatingthechronicwound:Apracticalapproachtothecareofnonhealingwoundsandwoundcaredressings.J. Am. Acad. Dermatol. 2008;58(2):185-206.
19. CaseyG.Chronicwoundhealing:legulcers.Nurs. N. Z. 2011;17(11):24-29.
20. MortimerPS.Evaluationoflymphaticfunction:abnormallymphdrainageinvenousdisease.Int. Angiol. 1995;14(3Suppl1):32-35.
21. MoutaC,HeroultM.Inflammatorytriggersoflymphangiogenesis.Lymphat. Res. Biol. 2003;1(3):201-218.
22. MacdonaldJM,SimsN,MayrovitzHN.Lymphedema,lipedema,andtheopenwound:theroleofcompressiontherapy.Surg. Clin. North Am.2003;83(3):639-658.
23. TabibiazarR,CheungL,HanJ,etal.Inflammatorymanifestationsofexperimentallymphaticinsufficiency.PLoS Med. 2006;3(7):e254.
24. NelsonKE,SergueefN,GlonekT.Theeffectofanalternativemedicalprocedureuponlow-frequencyoscillationsincutaneousbloodflowvelocity.J. Manipulative Physiol. Ther. 2006;29(8):626-636.
25. AnglundDC,ChannellMK.Contributionofosteopathicmedicinetocareofpatientswithchronicwounds.J. Am. Osteopath. Assoc. 2011;111(9):538-542.
26. VorkampT,FooFJ,KhanS,SchmittoJD,WilsonP.Hyperhidrosis:evolvingconceptsandacomprehensivereview.Surgeon. 2010;8(5):287-292.
27. RoKM,CantorRM,LangeKL,AhnSS.Palmarhyperhidrosis:evidenceofgenetictransmission.J. Vasc. Surg. 2002;35(2):382-386.
28. EisenachJH,AtkinsonJL,FealeyRD.Hyperhidrosis:evolvingtherapiesforawell-establishedphenomenon.Mayo Clin. Proc. 2005;80(5):657-666.
29. ShihCJ,WuJJ,LinMT.Autonomicdysfunctioninpalmarhyperhidrosis.J. Auton. Nerv. Syst. 1983;8(1):33-43.
30. RybojadM.Atopicdermatitis.Arch. Pediatr. 2012;19(8):882-885.31. TranBW,PapoiuAD,RussonielloCV,etal.Effectofitch,
scratchingandmentalstressonautonomicnervoussystemfunctioninatopicdermatitis.Acta Derm. Venereol. 2010;90(4):354-361.
32. MonroeJR.Isthisedemaandfirmingoftheskinaseveresign?Scleroderma.JAAPA. 2011;24(10):27.
33. RossiA,SozioF,SestiniP,etal.Lymphaticandbloodvesselsinsclerodermaskin,amorphometricanalysis.Hum. Pathol. 2010;41(3):366-374.
34. LongPR,MillerOF,3rd.Linearscleroderma.Reportofacasepresentingaspersistentunilateraleyelidedema.J. Am. Acad. Dermatol. 1982;7(4):541-544.
35. CampbellSM,SammonsDL,Sarsama-NixonRM,HolsingerJM,StephensonS,WalkowskiS.Dermatology:aspecialtythatexemplifiestheosteopathicmedicalprofession.J. Am. Osteopath. Assoc.2011;111(5):335-338.
Accepted for publication: November2013
Address correspondence to:RobertStern,MDDepartmentofBasicBiomedicalSciencesTouro-HarlemCollegeofOsteopathicMedicine230West-125thStreetNewYork,[email protected]
continued from page 37

Vol. 23, No. 4, December 2013 • The American Academy of Osteopathy Journal Page 43
AAOJ Submission ChecklistManuscript Submission
☐ SubmissionemailedtoAAOJ [email protected] ManagingEditor,AmericanAcademyofOsteopathy,3500DePauwBoulevard,Suite1080,Indianapolis,IN46268
☐ ManuscriptformattedinMicrosoftWordforWindows(.doc),textdocumentformat(.txt)orrichtextformat(.rtf)
Manuscript Components
☐ CoverletteraddressedtotheAAOJ ScientificEditor,KateMcCaffrey,DO,withanyspecialrequests(e.g.,rapidreview)notedandjustified
☐ Titlepage,includingtheauthors’fullnamesandfinancialorotheraffiliations,aswellasdisclosureofthefinancialsupportrelatedtooriginalresearchdescribedinthemanuscript
☐ “Abstract”(see“Abstract”sectionin“AAOJ InstructionsforContributors”foradditionalinformation)
☐ “Methods”section
• thenameofthepublicregistryinwhichthetrialislisted,ifapplicable
• ethicalstandards,therapeuticagentsordevices,andstatisticalmethodsdefined
☐ Fourmultiple-choicequestionsforthecontinuingmedicaleducationquizandbriefdiscussionsofthecorrectanswers
☐ Editorialconventionsadheredto
• unitsofmeasuregivenwithalllaboratoryvalues
• onfirstmention,allabbreviationsotherthanmeasurementsplacedinparenthesesafterthefullnamesoftheterms,asin“AmericanAcademyofOsteopathy(AAO)”
☐ Numberedreferences,tablesandfigurescitedsequentiallyinthetext
• journalarticlesandothermaterialcitedinthe“References”sectionfollowtheguidelinesdescribedinthemostcurrenteditionoftheAMA Manual of Style: A Guide for Authors and Editors.
• referencesincludedirect,open-accessURLstoposted,full-textversionsofthedocuments
• photocopiesprovidedforreferenceddocumentsnotaccessiblethroughURLs
☐ “Acknowledgements”sectionwithaconcise,comprehensivelistofthecontributionsmadeby
individualswhodonotmeritauthorshipcreditandpermissionfromeachindividualtobenamedinprint
☐ Formanuscriptsbasedonsurveydata,acopyoftheoriginalvalidatedsurveyandcoverletter
Graphic Elements
☐ Graphicsshouldbeformattedasspecifiedinthe“GraphicElements”sectionof“AAOJ InstructionsforContributors”
☐ Graphicsshouldnotbeincludedwithtextbutsentasseparategraphicfiles(e.g.jpg,tiff,pdf)
☐ Eachgraphicelementcitedinnumericalorder(e.g.,Table 1,Table 2,andFigure 1,Figure 2)withcorrespondingnumericalcaptionsinthemanuscript
☐ Forreprintedoradaptedtables,figuresandillustrations,afullbibliographiccitationgiven,providingappropriateattribution
Required Legal Documentation
☐ Forreprintedoradaptedtables,figuresandillustrations,permissiontoreprintfromthepublisherintheAAOJ printandonlineversionsaccompaniedbyphotocopiesoftheoriginalwork
☐ Forphotographsinwhichpatientsarefeatured,signedanddated“Patient-ModelRelease”formssubmitted
☐ Fornamedsourcesofunpublisheddataandindividualslistedinthe“Acknowledgments”section,permissiontopublishtheirnamesintheAAOJ obtained.
☐ ForauthorsservingintheU.S.military,thearmedforces’approvalofthemanuscriptandinstitutionalormilitarydisclaimerssubmitted
Financial Disclosure and Conflict of Interest
Authorsarerequiredtodiscloseallfinancialandnon-financialrelationshipsrelatedtothesubmission’ssubjectmatter.Alldisclosuresshouldbeincludedinthemanuscript’stitlepage.Seethe“Titlepage”sectionof“AAOJInstructionstoContributors”forexamplesofrelationshipsandaffiliationsthatmustbedisclosed.Thoseauthorswhohavenofinancialorotherrelationshipstodisclosemustindicatethatonthemanuscript’stitlepage(e.g.,“DrJoneshasnoconflictofinterestorfinancialdisclosurerelevanttothetopicofthesubmittedmanuscript”).
Publication in JAOA
PleaseincludepermissiontoforwardallmanuscriptstotheJournal of the American Osteopathic AssociationiftheEditordeemsamanuscriptnotsuitedtothecurrentneedsoftheAAOJ.
Questions? Contact Dr. Kate McCaffrey, Scientific Editor, at [email protected].

Component Societies and Affiliated Organizations Calendar of Upcoming Events
December 14, 2013Gentle Techniques for the Upper Body:
Head, Neck, and ThoraxCourse Director: R. Paul Lee, DO, FAAO, FCA
Rocky Vista UniversityCollege of Osteopathic Medicine, Parker, COCME: 4 Category 1-A AOA credits anticipated
Website: 2dockanze.wix.com/rockymtnaao#!events/crrl
February 15-19, 2014Midwinter Introductory Course in Osteopathy in the
Cranial FieldCourse Director: Zina Pelkey, DOHoliday Inn, Lake Buena Vista, FL
CME: 40 Category 1-A AOA credits anticipatedPhone: (317) 581-0411 Fax: (317) 580-9299
Email: [email protected]: www.cranialacademy.org
February 21-23, 2014Key Elements in Effective Osteopathic Practice
Course Director: Rachel Brooks, MDHoliday Inn, Lake Buena Vista, FL
Phone: (317) 581-0411 Fax: (317) 580-9299Email: [email protected]
Website: www.cranialacademy.org
April 10-13, 2014Orthopedic Neurology
Course Director: Maurice Bensoussan, MD, DO, FCAAssociate Director: R. Paul Lee, DO, FAAO, FCA
Holiday Inn, Lake Buena Vista, FLPhone: (317) 581-0411 Fax: (317) 580-9299
Email: [email protected]: www.cranialacademy.org
June 14-18, 2014June Introductory Course in Osteopathy in the Cranial Field
Course Director: Eric J. Dolgin, DO, FCASheraton Indianapolis City Centre, Indianapolis, IN
Phone: (317) 581-0411 Fax: (317) 580-9299Email: [email protected]
Website: www.cranialacademy.org
June 19-22, 2014Osteopathic Cranial Academy Annual Conference: Beyond
Sutherland’s Minnow: Anatomy, Perception and TreatmentConference Director: Melvin R. Friedman, DO
Sheraton Indianapolis City Centre, Indianapolis, INPhone: (317) 581-0411 Fax: (317) 580-9299
Email: [email protected]: www.cranialacademy.org