Embed Size (px)
Citation preview

04 (2007) 377–380www.elsevier.com/locate/ygyno
Gynecologic Oncology 1
Tertiary cytoreductive surgery in recurrent ovarian cancer:Selection criteria and survival outcome
Amer K. Karam a, Antonio Santillan b, Robert E. Bristow b, Robert Giuntoli II b,Ginger J. Gardner b, Ilana Cass a, Beth Y. Karlan a, Andrew J. Li a,⁎
a Department of Obstetrics and Gynecology, Division of Gynecologic Oncology, Cedars Sinai Medical Center, 8700 Beverly Blvd., Los Angeles, CA 90048, USAb The Kelly Gynecologic Oncology Service, Department of Gynecology and Obstetrics, The Johns Hopkins Medical Institutions, Baltimore, Maryland, USA
Received 10 July 2006Available online 2 October 2006
Abstract
Objectives. Studies of tertiary cytoreductive surgery (TCS) in recurrent epithelial ovarian cancer are limited, and appropriate patient selectionremains a clinical challenge. We sought to evaluate the impact of TCS on survival and to determine predictors of optimal tertiary resection.
Methods. Between January 1997 and July 2004, 47 women with recurrent epithelial ovarian cancer underwent TCS at two institutions. Allpatients received initial platinum and taxane-based chemotherapy following primary cytoreductive surgery. Clinico-pathologic factors and survivalwere retrospectively abstracted from medical records. Optimal TCS was defined as microscopic residual disease.
Results. Thirty of 47 (64%) patients underwent optimal TCS. Size of tumor implants <5 cm on preoperative imaging was the only significantpredictor of achieving optimal TCS. Overall survival after TCS was statistically longer in patients with microscopic versus macroscopic residualdisease (24 versus 16 months, p=0.03). After controlling for age, time to progression and optimal TCS, only the presence of diffuse disease attertiary exploration remained a significant poor predictor of survival. However, in a cohort of patients with limited disease implants, multivariateanalysis indicated that optimal TCS retained prognostic significance as a positive predictor of survival. Twelve patients (26%) experiencedsevere postoperative complications, including six with pulmonary embolism, four with fistulae and two with postoperative myocardialinfarctions.
Conclusions. Size of disease implants on preoperative imaging may guide the selection of candidates for TCS. In those patients with limiteddisease implants at laparotomy, optimal TCS is associated with improved survival.© 2006 Elsevier Inc. All rights reserved.
Keywords: Epithelial ovarian cancer; Cytoreductive surgery; Recurrent disease
Introduction
Most women diagnosed with epithelial ovarian cancerpresent with advanced stage disease. While complete clinicalremission can be achieved in up to 80% of these patients withcytoreductive surgery and combination chemotherapy, thetypical clinical course of their disease is characterized bymultiple recurrences [1–3]. Optimal management is less welldefined in recurrent disease, and treatment is typicallyindividualized based on factors such as progression-freeinterval, residual disease and quality of life. Management ofrecurrent disease may involve salvage chemotherapy, secondary
⁎ Corresponding author.E-mail address: [email protected] (A.J. Li).
0090-8258/$ - see front matter © 2006 Elsevier Inc. All rights reserved.doi:10.1016/j.ygyno.2006.08.037
tumor resection and/or radiation [4–13]. Several studies haveexamined secondary cytoreduction in the setting of recurrentovarian cancer. In a review of the existing published data onsalvage surgery in recurrent ovarian cancer, Munkarah andColeman reported on the technical feasibility of furtherresection, with 67% of 631 patients undergoing “optimal”secondary cytoreduction (with the definition of “optimal”ranging from <0.5 cm to <2 cm in the 10 studies reviewed)[6]. Operative times, transfusion requirements and overallcomplication rates are comparable to those associated withprimary surgery, indicating that these patients may undergosecondary tumor resection with acceptable morbidity [6,7]. Themajority of these data also demonstrate a survival advantage forwomen in whom optimal secondary cytoreduction is achieved[6,12].

Table 1
378 A.K. Karam et al. / Gynecologic Oncology 104 (2007) 377–380
Patients who enter a second remission following their initialrecurrence will eventually relapse. Data examining the clinicalbenefit of additional cytoreductive procedures in this setting arelimited, and there are no established guidelines to determinewhich patients may benefit from tertiary cytoreductive surgery(TCS). We hypothesized that in patients with a second diseaserecurrence, optimal tertiary surgical cytoreduction extendsoverall survival. Our objectives were to determine the feasibilityand morbidity of TCS and examine the impact of optimal TCSon survival.
Patients and methods
The records of all patients with recurrent epithelial ovarian cancer or primaryperitoneal carcinoma who underwent surgical procedures at Cedars-Sinai MedicalCenter and Johns Hopkins Hospital between January 1997 and July 2004 werereviewed under an IRB-approved protocol. All patients underwent secondarycytoreductive surgery at their first recurrence, followed by tertiary surgicalexploration at their first suspected second recurrence of disease. Patientswere takento the operating room with the intent to perform complete resection of allmacroscopic disease. Patients undergoing surgery for a primary diagnosis of bowelobstruction were excluded from review. While the clinicians at our institutions donot follow explicit criteria to select patients for tertiary cytoreduction, in generalTCS is offered to patients with an extended disease-free interval after remissionfrom secondary recurrence greater than 6 months, limited disease on imagingstudies to less than 3 tumor sites, and performance status of 0 to 1.
Data were abstracted from medical records regarding preoperative clinicalfactors, such as age at time of second recurrence, performance status, initialtreatment-free interval and treatment interval before tertiary cytoreductivesurgery. Preoperative imaging details were also abstracted, including the numberand size of disease sites. “Diffuse disease” was arbitrarily defined as ≥10disease sites at exploratory laparotomy. Operative details such as blood loss,extent of cytoreductive surgery and size of the largest tumor nodule were alsonoted. The amount of residual tumor was considered microscopic when novisible disease remained at the conclusion of surgery, and more or less than 1 cmdepending on the size of the remaining tumor nodules. We defined optimal TCSas microscopic residual disease. The postoperative course including length ofhospital stay and complications within 30 days of surgery was recorded.
The stage at initial diagnosis was based on the system developed by theInternational Federation of Gynecology and Obstetrics (FIGO). The number,timing and type of chemotherapeutic regimens were abstracted in order tocalculate the initial disease-free interval as well as the treatment interval beforethe TCS. Overall disease-specific survival (OS) was calculated from the time ofthe TCS until disease-related death.
Multivariate logistic regression was used to determine preoperative variablesrelated to optimal TCS. Survival curves were estimated using the Kaplan–Meiermethod. The log rank test was used to compare survival curves across groups.Variables related to the hazard (risk) of death were assessed using Coxproportional hazards models. Hazard ratios and 95% confidence intervals werecalculated for the significant predictor variables. A significance level of 0.05was used throughout. Statistical calculations were performed using the softwarepackage SAS version 9.1 (SAS Institute, Cary, NC).
Multiple logistic regression analysis of preoperative factors on ability to achieveoptimal cytoreduction at tertiary exploration
Variable OR 95% CI p
Age at TCS a 1.02 0.96–1.08 n.s.Initial treatment-free interval ≥12 months b 2.48 0.42–14.64 n.s.Ascites c 1.00 0.18–5.64 n.s.Number of lesions <4 d 1.36 0.30–6.13 n.s.Size of largest tumor <5 cm e 7.42 1.66–33.27 0.009a Analyzed as a continuous variable.b 36 patients had an initial treatment free interval >12 months.c 9 patients had ascites.d 21 patients had number of lesions <4.e 21 patients had size of their largest tumor <5 cm.
Results
Forty-seven patients who underwent TCS were identified. Themedian age at the time of the TCS was 58 (range, 28–77 years),and 92% (43/47) of patients had stage III or IV disease at initialdiagnosis. The median time from secondary cytoreductivesurgery (SCS) to TCS was 17 months (range, 6–66 months),with a median progression-free interval (PFI) before TCS of11 months (range, 1–66 months). Computed tomography was thepreoperative imaging modality of choice and was employed in
87% (41/47) of cases. The median number of disease sitesidentified on preoperative imaging was 4 (range, 1–diffuse).
A variety of cytoreductive surgical procedures were utilizedduring TCS, including small and large bowel resections, lymphnode dissections, partial liver resections, splenectomies andgenitourinary surgery. The median size of the largest tumormass was 5 cm (range, 1–11). The median amount of blood losswas 250 cc (range, 5–1100). 64% (30/47) of patients underwentTCS to microscopic residual disease and 81% (38/47) had<1 cm of residual disease after TCS. The median hospital staywas 7 days (range 2–27).
To determine potential preoperative predictors of optimal TCS,multivariate logistic regression analysis was performed. Aftercontrolling for presence of ascites, initial disease-free interval, ageat TCS and limited number of disease sites on preoperativeimaging (less than 4), only size of tumor (less than 5 cm) remainedas a statistically significant predictor of successfully resectingtumor at TCS to microscopic residual disease (p=0.02 andp=0.03, respectively; Table 1). The cutoff values for size of tumorand number of disease sites on preoperative imaging were chosenbased upon the median values reported above.
To identify pre- and intraoperative findings that mayinfluence survival after TCS, we performed both univariateand multivariate analyses. Univariate analysis identified that thepresence of diffuse disease at laparotomy (defined as >10disease sites) and suboptimal TCS were statistically significantnegative predictors of survival (p=0.008 and 0.03, respective-ly). Age at TCS, time to progression, optimal cytoreduction attime of SCS and tumor size were not predictive of survival. Inmultivariate analysis, only the presence of diffuse diseaseremained significantly associated with a poorer outcome(p=0.008, HR=2.78, 95% CI=1.3–6.1; Table 2).
Thirty-four patients had <10 disease sites at tertiaryexploration and were considered to have limited disease. Toexplore the impact of TCS on these patients, we examined asubset of patients with <10 disease sites at laparotomy. In thisanalysis of 34 patients, surgical resection of tumor implants tomicroscopic residual disease conferred a survival advantageboth on univariate (p=0.02) and multivariate analysis (p=0.02,HR=0.3, 95% CI=0.11–0.85; Table 3).
Associations between extent of TCS and survival werefurther examined with Kaplan–Meier survival analyses. In

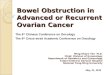
Fig. 1. Of all patients in the cohort, those undergoing tertiary cytoreductivesurgery to microscopic residual disease (dashed line) demonstrated longerdisease-specific overall survival when compared to those with macroscopicresidual disease (solid line; 24 versus 16 months, p=0.03).
Table 2Univariate and multivariate analysis of clinical factors on overall survival for 47patients undergoing tertiary cytoreductive surgery
Variable Univariateresults
Multivariate results
p value p value HR 95% CI
Presence of diffuse disease a 0.008 0.008 2.78 1.27–6.08Microscopic residual disease b 0.03 0.10 – –Initial treatment-free interval c 0.13 0.29 – –Age at TCS c 0.51 0.23 – –Treatment interval before TCSc 0.74 0.91 – –Tumor size c 0.90 0.92 – –
–, Not calculated.a 13 patients had diffuse disease at laparotomy.b 30 patients had microscopic residual disease after tertiary cytoreductive
surgery.c Analyzed as a continuous variable.
379A.K. Karam et al. / Gynecologic Oncology 104 (2007) 377–380
patients optimally cytoreduced to microscopic residual diseasefollowing TCS, median survival was 24 months, compared to16 months for those with macroscopic residual disease (p=0.03;Fig. 1). As reported above, optimal cytoreduction only retainedsignificance on multivariate analysis in the subcohort of patientswith limited disease at exploration. Given that the impact ofaggressive TCS appears to be most relevant in this group, weagain examined this subset of patients with less than 10 diseasesites at laparotomy. Here, Kaplan–Meier analyses indicate thatthose with microscopic residual disease survived a median of37 months, compared to 16 months for those with macroscopicresidual disease (p=0.02; Fig. 2).
Twelve patients (26%) developed postoperative complica-tions. Six patients (12.8%) were diagnosed with a pulmonaryembolism. Two patients developed an enterocutaneous fistula; athird patient developed a rectovaginal fistula and a fourthpatient a vesicovaginal fistula. Two patients (4.3%) werediagnosed with a postoperative myocardial infarction. Nopostoperative deaths were identified in our cohort.
Discussion
Our data suggest that in patients with limited disease atexploration, optimal TCS at second recurrence significantly
Table 3Univariate and multivariate analysis of clinical factors on overall survival for 34patients with limited disease (<10 tumor sites) undergoing tertiary cytoreductivesurgery
Variable Univariate results Multivariate results
p value p value HR 95% CI
Microscopic residual disease a 0.02 0.02 0.30 0.11–0.85Initial treatment-free interval b 0.21 0.40 – –Tumor size b 0.72 0.78 – –Age at TCS b 0.79 0.67 – –Treatment interval before TCS b 0.83 0.95 – –
–, Not calculated.a 24 patients had microscopic residual disease after tertiary cytoreductive
surgery.b Analyzed as a continuous variable.
extends overall survival. We identified size of tumor implantson preoperative imaging as a significant predictor of surgicaloutcome and found that the survival impact of optimal TCS ismost significant in those patients who have limited disease atsurgical exploration. It is also important to note that 26% ofwomen in this cohort developed severe postoperative complica-tions, but no postoperative deaths were identified.
The examination of TCS in recurrent epithelial ovariancancer remains limited. In the only other study of this kind,Leitao and colleagues reported on a cohort of 26 women andfound an 18-month gain in survival for patients with less than0.5 cm of residual disease after TCS versus those left with morethan 0.5 cm [14]. Our findings similarly define a survivaladvantage for those women who are able to undergo completeTCS. However, our data indicate that the survival advantageafforded by optimal TCS is limited to those patients with limiteddisease. While this finding may be influenced by delay indiagnosis, with attendant progression of disease, or surgeonbias, we hypothesize that our data suggest that tumor biology
Fig. 2. In patients with limited disease at tertiary exploration (defined as <10disease sites), those undergoing cytoreductive surgery to microscopic residualdisease (dashed line) demonstrate longer disease-specific overall survival whencompared to those with macroscopic residual disease (solid line; 37 versus16 months, p=0.02).

380 A.K. Karam et al. / Gynecologic Oncology 104 (2007) 377–380
remains a dominant factor on the clinical course of ovariancancer.
Despite these findings, cytoreductive surgery remains acontroversial therapeutic modality in the treatment of recurrentovarian cancer. Studies of secondary surgical cytoreductiondemonstrate technical feasibility of further resection, and thepreponderance of data suggest that aggressive tumor resectionin this setting confers a survival advantage in well-selectedpatients [6–12]. In an analysis of ten publications of SCS,Munkarah and Coleman found that complete resection of thetumor recurrence was one of the most powerful determinantsof prolonged survival [6]. However, these data continue to belimited by retrospective bias and the variety of patientselection criteria utilized in each report. Furthermore, to datethere are no randomized controlled trials that have examinedfurther cytoreductive surgery as a treatment modality inrecurrent ovarian cancer.
Our study is similarly limited by the small size of our cohortand its retrospective nature. Our data may be further constrainedby a lack of uniform criteria used to select patients to undergoTCS. Despite these limitations, TCS appears to extend survivalin those patients with limited disease sites at time of exploration.While we report an 8.5% postoperative fistula rate, we can onlyspeculate that prior surgical explorations and recurrent tumorvolume may contribute to this complication. Given thisrelatively high morbidity, we suggest that TCS should beconsidered only in patients with small tumor size onpreoperative imaging. Laparoscopy may be also consideredbefore laparotomy to evaluate disease burden before attemptingaggressive cytoreductive procedures. Further study is warrantedto fully evaluate the use of this treatment modality in themanagement of recurrent ovarian cancer.
Acknowledgment
The authors would like to acknowledge James Mirocha, Ph.D.(C), of the Cedars-Sinai Research Institute Biostatistics Corefor statistical assistance.
References
[1] Eisenkop SM, Friedman RL, Wang HJ. Complete cytoreductive surgeryis feasible and maximizes survival in patients with advanced epithelialovarian cancer: a prospective study. Gynecol Oncol 1998;69: 103–8.
[2] Vasey PA, Jayson GC, Gordon A, et al. Phase III randomized trial ofdocetaxel–carboplatin versus paclitaxel–carboplatin as first-line chemo-therapy for ovarian carcinoma. J Natl Cancer Inst 2004;96: 1682–91.
[3] Ozols RF, Bundy BN, Greer BE, et al. Gynecologic oncology group. phaseIII trial of carboplatin and paclitaxel compared with cisplatin and paclitaxelin patients with optimally resected stage III ovarian cancer: a gynecologiconcology group study. J Clin Oncol 2003;21:3194–200.
[4] Gordon AN, Tonda M, Sun S, et al. Long-term survival advantage forwomen treated with pegylated liposomal doxorubicin compared withtopotecan in a phase 3 randomized study of recurrent and refractoryepithelial ovarian cancer. Gynecol Oncol 2004;95:1–8.
[5] Parmar MK, Ledermann JA, Colombo N, et al. Paclitaxel plus platinum-based chemotherapy versus conventional platinum-based chemotherapy inwomen with relapsed ovarian cancer: the ICON4/AGO-OVAR-2.2 trial.Lancet 2003;361:2099–106.
[6] Munkarah AR, Coleman RL. Critical evaluation of secondary cytoreduc-tion in recurrent ovarian cancer. Gynecol Oncol 2004;95:273–80.
[7] Bristow RE, Tomacruz RS, Armstrong DK, et al. Survival effect ofmaximal cytoreductive surgery for advanced ovarian carcinoma during theplatinum era: a meta-analysis. J Clin Oncol 2002;20:1248–59.
[8] Segna RA, Dottino PR, Mandeli JP, et al. Secondary cytoreduction forovarian cancer following cisplatin therapy. J Clin Oncol 1993;11: 434–9.
[9] Eisenkop SM, Friedman RL, Spirtos NM. The role of secondarycytoreductive surgery in the treatment of patients with recurrent epithelialovarian carcinoma. Cancer 2000;88:144–53.
[10] Zang RY, Li ZT, Tang J, et al. Secondary cytoreductive surgery for patientswith relapsed epithelial ovarian carcinoma: who benefits? Cancer2004;100:1152–61.
[11] Morris M, Gershenson DM, Wharton JT, et al. Secondary cytoreductivesurgery for recurrent epithelial ovarian cancer. Gynecol Oncol 1989;34:334–8.
[12] Gadducci A, Iacconi P, Cosio S, et al. Complete salvage surgicalcytoreduction improves further survival of patients with late recurrentovarian cancer. Gynecol Oncol 2000;79:344–9.
[13] Gelblum D, Mychalczak B, Almadrones L, et al. Palliative benefit ofexternal-beam radiation in the management of platinum refractoryepithelial ovarian carcinoma. Gynecol Oncol 1998;69:36–41.
[14] Leitao Jr MM, Kardos S, Barakat RR, et al. Tertiary cytoreduction inpatients with recurrent ovarian carcinoma. Gynecol Oncol 2004;95:181–8.