Embed Size (px)
Citation preview

Termination of Ventricular Tachycardiaby an Increase in Cardiac Vagal Drive
MENASHE B. WAXMAN, M.D., AND ROBERT W. WALD, M.D.
SUMMARY Out of 12 patients in whom phenylephrine ter-minated ventricular tachycardia, four were selected for detailedstudies of its mechanism of action. Pretreatment withedrophonium (15-20 mg, i.v.) decreased, while atropine (2.4 mg, i.v.)increased by at least a factor of two, the dose of phenylephrine re-quired to break ventricular tachycardia. Carotid sinus massage
VENTRICULAR TACHYCARDIA (VT) is believed to beunresponsive to enhanced vagal traffic, while supraventric-ular tachycardias are slowed or converted to normalrhythm.' This time-honored method of clinical differentia-tion of supraventricular tachycardia with aberrant conduc-tion and VT has become the subject of renewed interest.4Recently, we reported that phenylephrine terminated sixcases of ventricular tachycardia (VT).8 A considerableamount of attention was directed at trying to relate thoseterminations to a vagal mechanism, but we could not make afirm conclusion on the evidence we had. Since that report,we have examined 12 cases of VT which could be terminatedby phenylephrine. Our observations in four of these casesaimed at elucidating the mechanism of phenylephrine's ac-tion are detailed in this report.
Materials and Methods
Thirteen patients with VT were selected for challenge withphenylephrine based on the following criteria: 1) The VTwas recurrent over five or more years. 2) The VT did not oc-cur as a result of or in the presence of acute myocardialischemia, acute myocardial infarction or severe left ventric-ular dysfunction of any etiology. 3) The VT producedminimal or no discernible adverse hemodynamic effects. 4)Pressor challenges with phenylephrine were deemed to besafe. In 12 of these 13 patients, phenylephrine terminatedVT and among these, four were selected for very detailed ex-amination of a possible vagal role in these terminations. Thesole reason for selecting these four particular cases is thatthey had had numerous episodes of stable VT. In any onecase comparisons could be made with either multiple spon-taneously occurring episodes of VT or episodes induced byexercise, rapid right atrial or ventricular pacing or timedpremature ventricular beats. Intracardiac electrograms wererecorded by standard techniques and recorded on an Elec-tronics for Medicine DR-12 recorder. Intracardiac stimula-tion was performed by means of a Grass S-88 stimulatorcoupled through stimulus isolation units. The drugs used inthese studies included edrophonium hydrochloride (10-20mg, i.v.), phenylephrine (0.1-3.0 mg, i.v.), atropine sulfate(1.8-2.4 mg, i.v.), isoproterenol (1-10 lAg, i.v.) andpropranolol (5 mg, i.v.).
From the Department of Medicine, Faculty of Medicine, University ofToronto and the Division of Cardiology, Toronto General Hospital, Toronto,Ontario, Canada.
Supported in part by the Ontario and Canadian Heart Foundations.Address for reprints: M. B. Waxman, M.D., Cardiovascular Unit, Toronto
General Hospital, 101 College Street, Toronto, Ontario, Canada M5G 1L7.Received December 3, 1976; revision accepted April 1, 1977.
following pretreatment with edrophonium in unusually high (15-20mg, i.v.) doses broke ventricular tachycardia in all four patients. Theevidence presented supports the assumption that a vagal mechanismcaused both instances of termination. These findings significantlyalter our interpretation of vagal interventions in the bedside clinicaldiagnosis of wide QRS complex tachycardias.
The protocol for study was as follows:A) The precise dose of phenylephrine needed to break two
consecutive episodes of VT was determined. This was doneby intravenous bolus injections of phenylephrine starting at adose of 0.1 mg and increasing this in steps of 0.1-0.2 mg. Theblood pressure was carefully monitored either continuouslythrough an intra-arterial line or by repeated cuff determina-tions. An interval of at least five minutes following the returnof the blood pressure to control was allowed to elapsebetween successive challenges.
B) During a third episode of VT, carotid sinus massage(CSM) was applied before and after pretreatment with 10, 15or 20 mg edrophonium HCI. In instances whereedrophonium was administered, right or left sided carotidsinus massage (CSM) was applied as soon as the patient feltsome of the muscarinic side effects" (about 30-40 secondslater).
C) During a fourth episode of VT (at least 30 min follow-ing step B), the patients were pretreated with a second doseof edrophonium identical to that which permitted VT ter-mination in conjunction with CSM. The dose ofphenylephrine needed to terminate VT was now redeter-mined by bolus injections similar to those used in (A).
D) During a fifth episode of VT (at least 30 minutesfollowing step C), the patients were pretreated with atropine2.4 mg, i.v. Conversion of VT with phenylephrine was nowattempted using bolus injections starting at a dose of 0.5 mgand increasing this in steps of 0.2 mg. The maximumchallenging dose was limited by not allowing the peaksystolic pressure to exceed 200 mm Hg.The nature and purpose of these studies was fully ex-
plained and informed verbal and written consent was ob-tained from each patient.
Results
Criteria for Ventricular Tachyeardia
In all cases the diagnosis of VT was established by thefollowing criteria:'0 1) The QRS complexes during thetachycardia were 120 msec or greater in duration and totallydifferent from the complexes during supraventricularrhythm (figs. 1-9). 2) Atrioventricular (A-V) dissociation(figs. 1-3, 6, 8) or V-A block (fig. 7) was present. 3) Intermit-tent fusion and normal capture beats occurred (figs. 1, 2). 4)Atrial pacing to rates in excess of the tachycardia did notproduce aberration (fig. 2). 5) There was no His bundlepotential preceding ventricular activation during thetachycardia. A His bundle potential preceded each QRScomplex with a normal H-V interval when sinus rhythm was
385
by guest on May 20, 2018
http://circ.ahajournals.org/D
ownloaded from
VOL 56, No 3, SEPTEMBER 1977
LI
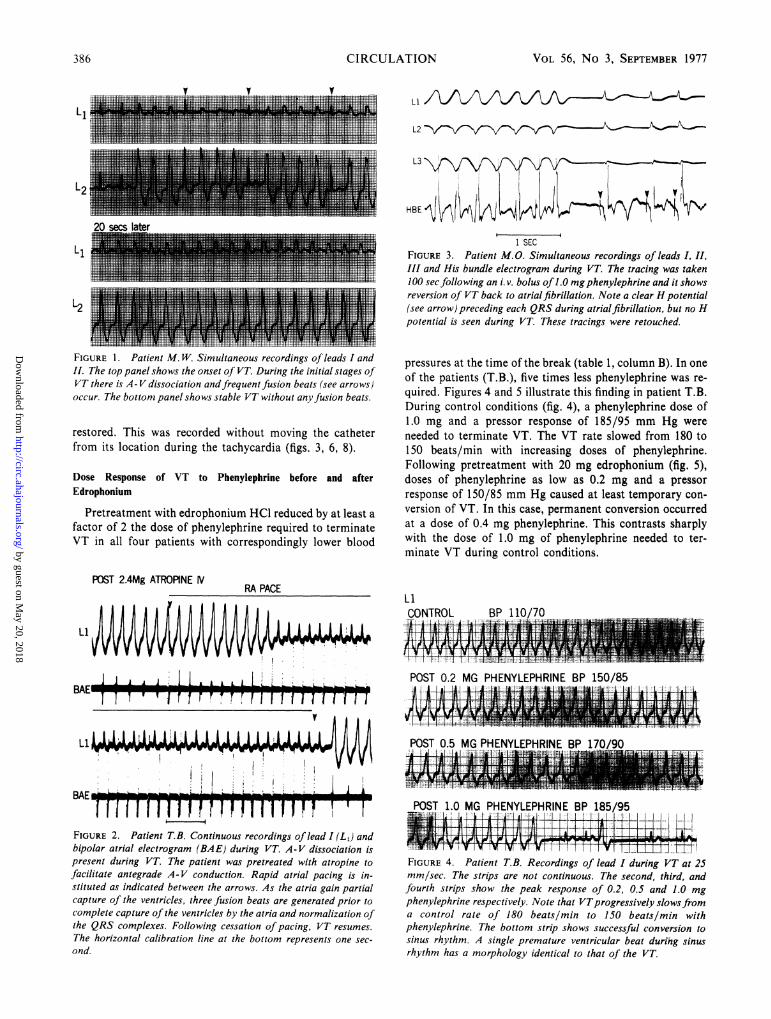
FIGURE 1. Patient M. W. Simultaneous recordings of leads I andIL The top panel shows the onset of VT. During the initial stages ofVT there is A- V dissociation andfrequent fusion beats (see arrows)occur. The bottom panel shows stable VT without anyfusion beats.
restored. This was recorded without moving the catheterfrom its location during the tachycardia (figs. 3, 6, 8).
Dose Response of VT to Phenylephrine before and afterEdrophonium
Pretreatment with edrophonium HCl reduced by at least afactor of 2 the dose of phenylephrine required to terminateVT in all four patients with correspondingly lower blood
POST 2.4Mg ATROPINE [V
L3
1 SECFIGURE 3. Patient M.O. Simultaneous recordings of leads I, II,III and His bundle electrogram during VT. The tracing was taken100 sec following an i.v. bolus of 1.0 mgphenylephrine and it showsreversion of VT back to atrial fibrillation. Note a clear H potential(see arrow) preceding each QRS during atrialfibrillation, but no Hpotential is seen during VT. These tracings were retouched.
pressures at the time of the break (table 1, column B). In oneof the patients (T.B.), five times less phenylephrine was re-quired. Figures 4 and 5 illustrate this finding in patient T.B.During control conditions (fig. 4), a phenylephrine dose of1.0 mg and a pressor response of 185/95 mm Hg wereneeded to terminate VT. The VT rate slowed from 180 to150 beats/min with increasing doses of phenylephrine.Following pretreatment with 20 mg edrophonium (fig. 5),doses of phenylephrine as low as 0.2 mg and a pressorresponse of 150/85 mm Hg caused at least temporary con-version of VT. In this case, permanent conversion occurredat a dose of 0.4 mg phenylephrine. This contrasts sharplywith the dose of 1.0 mg of phenylephrine needed to ter-minate VT during control conditions.
RA PACE
Li
LLL L LBAE A E i n mmmb-1 ' ITT r7Tr
-.
POST 0.2 MG PHENYLEPHRINE BP 150/851 AA.~4 .._&'1 II.. |.......*sW_El'i..*1-. i:
1t IIVVIi7
V
FIGURE 2. Patient T.B. Continuous recordings of lead I (L1) andbipolar atrial electrogram (BAE) during VT. A-V dissociation ispresent during VT. The patient was pretreated with atropine tofacilitate antegrade A-V conduction. Rapid atrial pacing is in-stituted as indicated between the arrows. As the atria gain partialcapture of the ventricles, three fusion beats are generated prior tocomplete capture of the ventricles by the atria and normalization ofthe QRS complexes. Following cessation of pacing, VT resumes.
The horizontal calibration line at the bottom represents one sec-
ond.
POST 1.0 MG PHENYLEPHRINE BP 185/95
FIGURE 4. Patient T.B. Recordings of lead I during VT at 25mm/sec. The strips are not continuous. The second, third, andfourth strips show the peak response of 0.2. 0.5 and 1.0 mgphenylephrine respectively. Note that VTprogressively slowsfroma control rate of 180 beats/min to 150 beats/min withphenylephrine. The bottom strip shows successful conversion tosinus rhythm. A single premature ventricular beat durtng sinusrhythm has a morphology identical to that of the VT.
IIII..II..-... IIUIIIIIIIII,III .............M llillli lllrT E il l;;4 rls lT r rll lrz_
386 CIRCULATION
by guest on May 20, 2018
http://circ.ahajournals.org/D
ownloaded from
V TACH AND VAGAL EFFECTS/Waxman, Wald
Li 20 MG EDROPHONIUM HCLCONTROLv
40 SEC LATER
POST 0.2 MG PHENYLEPHRINE BP 150/85
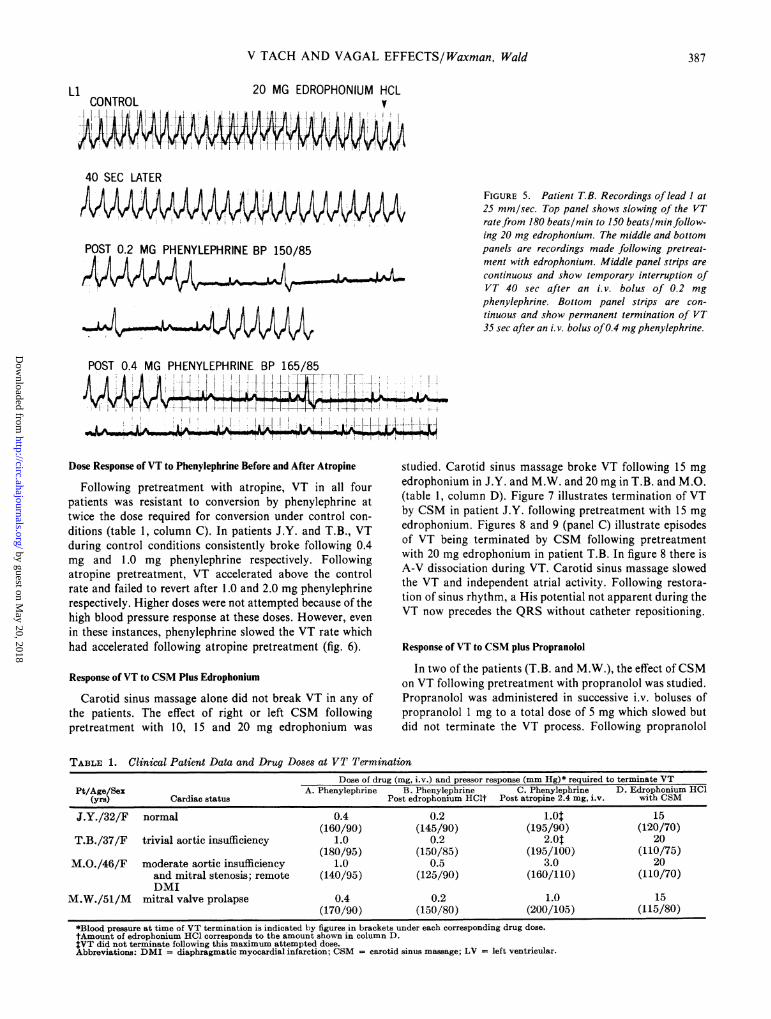
FIGURE 5. Patient TB. Recordings of lead I at
25 mm/sec. Top panel shows slowing of the VTratefrom 180 beats/min to 150 beats/min follow-ing 20 mg edrophonium. The middle and bottompanels are recordings made following pretreat-ment with edrophonium. Middle panel strips are
continuous and show temporary interruption ofVT 40 sec after an i.v. bolus of 0.2 mg
phenylephrine. Bottom panel strips are con-
tinuous and show permanent termination of VT35 sec after an i. v. bolus of0.4 mg phenylephrine.
POST 0.4 MG PHENYLEPHRINE BP 165/85
TfT--F-
Dose Response ofVT to Phenylephrine Before and After Atropine
Following pretreatment with atropine, VT in all fourpatients was resistant to conversion by phenylephrine attwice the dose required for conversion under control con-
ditions (table 1, column C). In patients J.Y. and T.B., VTduring control conditions consistently broke following 0.4mg and 1.0 mg phenylephrine respectively. Followingatropine pretreatment, VT accelerated above the controlrate and failed to revert after 1.0 and 2.0 mg phenylephrinerespectively. Higher doses were not attempted because of thehigh blood pressure response at these doses. However, even
in these instances, phenylephrine slowed the VT rate whichhad accelerated following atropine pretreatment (fig. 6).
Response of VT to CSM Plus Edrophonium
Carotid sinus massage alone did not break VT in any ofthe patients. The effect of right or left CSM followingpretreatment with 10, 15 and 20 mg edrophonium was
studied. Carotid sinus massage broke VT following 15 mgedrophonium in J.Y. and M.W. and 20 mg in T.B. and M.O.(table 1, column D). Figure 7 illustrates termination of VTby CSM in patient J.Y. following pretreatment with 15 mgedrophonium. Figures 8 and 9 (panel C) illustrate episodesof VT being terminated by CSM following pretreatmentwith 20 mg edrophonium in patient T.B. In figure 8 there isA-V dissociation during VT. Carotid sinus massage slowedthe VT and independent atrial activity. Following restora-tion of sinus rhythm, a His potential not apparent during theVT now precedes the QRS without catheter repositioning.
Response of VT to CSM plus Propranolol
In two of the patients (T.B. and M.W.), the effect ofCSMon VT following pretreatment with propranolol was studied.Propranolol was administered in successive i.v. boluses ofpropranolol 1 mg to a total dose of 5 mg which slowed butdid not terminate the VT process. Following propranolol
TABLE 1. Clinical Patient Data and Drug Doses at VT TerminationDose of drug (mg, i.v.) and pressor response (mm Hg)* required to terminate VT
Pt/Age/Sex A. Phenylephrine B. Phenylephrine C. Phenylephrine D. Edrophonium HCI(yrs) Cardiac status Post edrophonium HClt Post atropine 2.4 mg, i.v. with CSM
J.Y./32/F normal 0.4 0.2 1.01 15(160/90) (145/90) (195/90) (120/70)
T.B./37/F trivial aortic insufficiency 1.0 0.2 2.Ot 20(180/95) (150/85) (195/100) (110/75)
M.O./46/F moderate aortic insufficiency 1.0 0.5 3.0 20and mitral stenosis; remote (140/95) (125/90) (160/110) (110/70)DMI
M.W./51/M mitral valve prolapse 0.4 0.2 1.0 15(170/90) (150/80) (200/105) (115/80)
*Blood pressure at time of VT termination is indicated by figures in brackets under each corresponding drug dose.tAmount of edrophonium HCl corresponds to the amount shown in column D.$VT did not terminate following this maximum attempted dose.Abbreviations: DMI = diaphragmatic myocardial infarction; CSM = carotid sinus massage; LV = left ventricular.
387
by guest on May 20, 2018
http://circ.ahajournals.org/D
ownloaded from
VOL 56, No 3, SEPTEMBER 1977
Rest
Control
40 secs Post lmg Phenylephrine
HBE
200
100
Post
Rest
HBE 1BAE
100
0 Lt
40 secs Post 2mg Phenylephrine
-A i <1i
r I ---
I I I
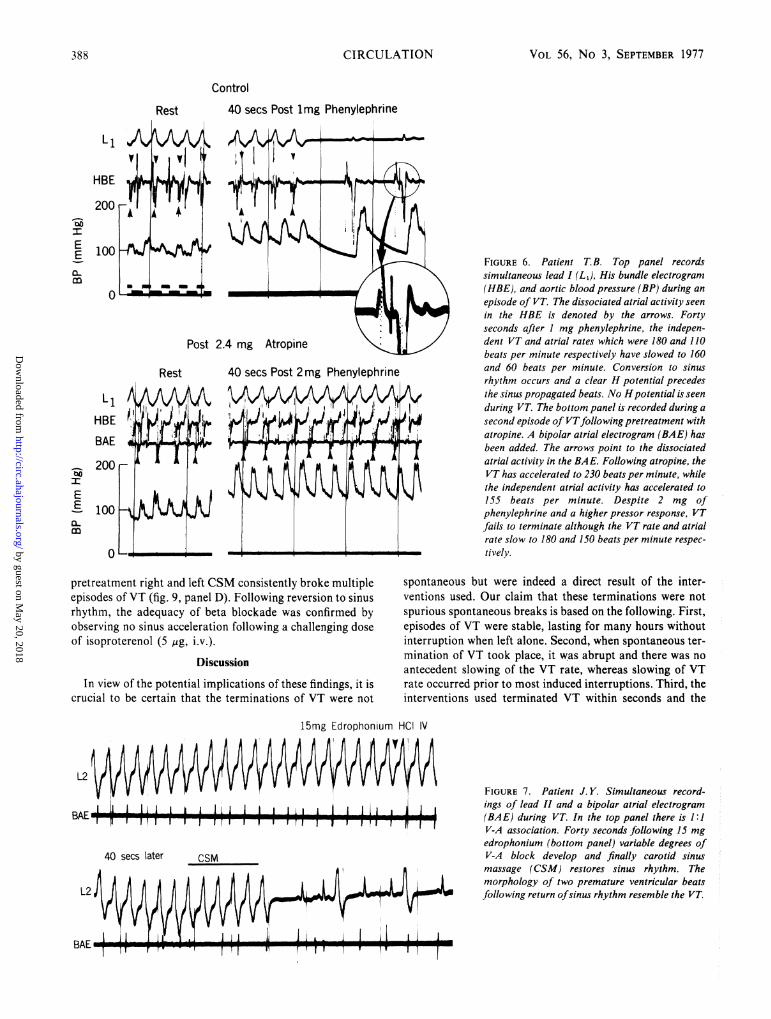
FIGURE 6. Patient T.B. Top panel recordssimultaneous lead I (L1), His bundle electrogram(HBE), and aortic blood pressure (BP) during anepisode of VT. The dissociated atrial activity seenin the HBE is denoted by the arrows. Fortyseconds after I mg phenylephrine, the indepen-dent VT and atrial rates which were 180 and 110beats per minute respectively have slowed to 160and 60 beats per minute. Conversion to sinusrhythm occurs and a clear H potential precedesthe sinus propagated beats. No Hpotential is seenduring VT. The bottom panel is recorded during asecond episode of VTfollowing pretreatment withatropine. A bipolar atrial electrogram (BAE) hasbeen added. The arrows point to the dissociatedatrial activity in the BAE. Following atropine, theVT has accelerated to 230 beats per minute, whilethe independent atrial activity has accelerated to155 beats per minute. Despite 2 mg ofphenylephrine and a higher pressor response, VTfails to terminate although the VT rate and atrialrate slow to 180 and 150 beats per minute respec-tively.
/V
i-I -
pretreatment right and left CSM consistently broke multipleepisodes of VT (fig. 9, panel D). Following reversion to sinusrhythm, the adequacy of beta blockade was confirmed byobserving no sinus acceleration following a challenging doseof isoproterenol (5 gtg, i.v.).
Discussion
In view of the potential implications of these findings, it iscrucial to be certain that the terminations of VT were not
spontaneous but were indeed a direct result of the inter-ventions used. Our claim that these terminations were notspurious spontaneous breaks is based on the following. First,episodes of VT were stable, lasting for many hours withoutinterruption when left alone. Second, when spontaneous ter-mination of VT took place, it was abrupt and there was no
antecedent slowing of the VT rate, whereas slowing of VTrate occurred prior to most induced interruptions. Third, theinterventions used terminated VT within seconds and the
15mg Edrophonium HCI IV
L2 IVVVVVVVVV V V V V VV V V
--I II IIII I I " II I I I I I II I I IbALI
40 secs later CSM
FIGURE 7. Patient J. Y. Simultaneous record-ings of lead II and a bipolar atrial electrogram(BAE) during VT. In the top panel there is 1:IV-A association. Forty seconds following 15 mgedrophonium (bottom panel) variable degrees ofV-A block develop and finally carotid sinusmassage (CSM) restores sinus rhythm. Themorphology of two premature ventricular beatsfollowing return ofsinus rhythm resemble the VT
Y-
EE
c0
EEE
m
CIRCULATION388
V.
by guest on May 20, 2018
http://circ.ahajournals.org/D
ownloaded from
V TACH AND VAGAL EFFECTS/Waxman, Wald
Post 20mg Edrophonium
It1 . I ii-, - I r r I !- I .1I r
I
HBEI^. I
VI I I I Icsm
m
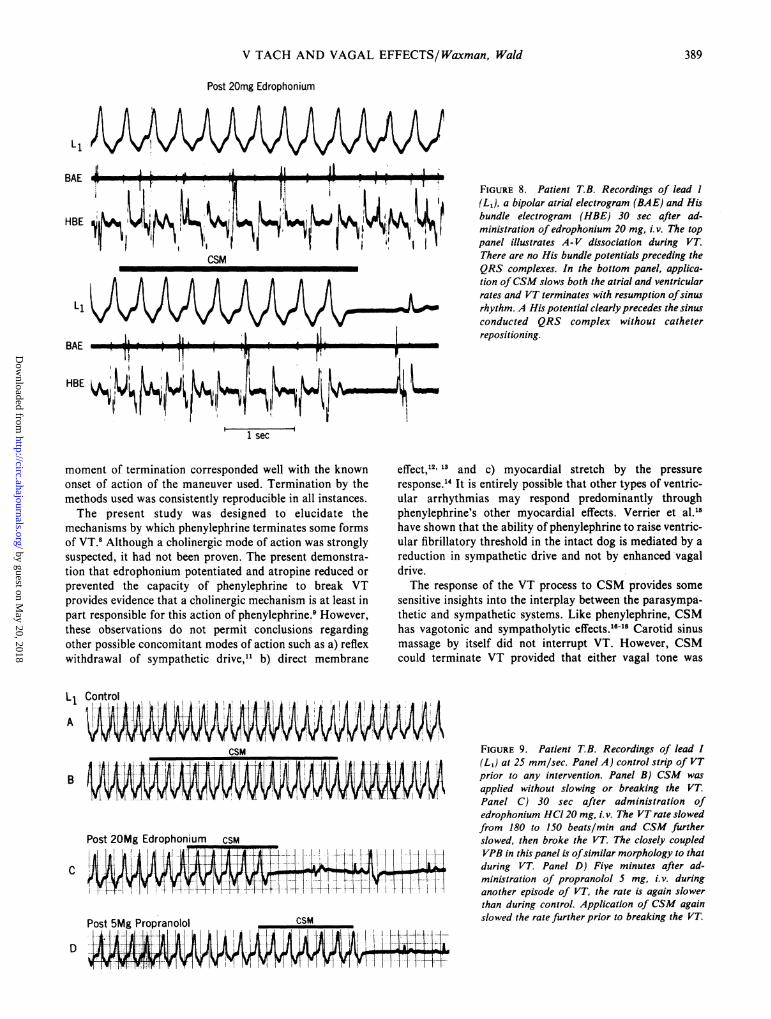
FIGURE 8. Patient T.B. Recordings of lead I
(Lj), a bipolar atrial electrogram (BAE) and Hisbundle electrogram (HBE) 30 sec after ad-ministration of edrophonium 20 mg, i.v. The toppanel illustrates A-V dissociation during VT.There are no His bundle potentials preceding theQRS complexes. In the bottom panel, applica-tion ofCSM slows both the atrial and ventricularrates and VT terminates with resumption ofsinusrhythm. A His potential clearly precedes the sinusconducted QRS complex without catheterrepositioning.
BAE
HBE
W! 1siE
i1 sec
moment of termination corresponded well with the knownonset of action of the maneuver used. Termination by themethods used was consistently reproducible in all instances.The present study was designed to elucidate the
mechanisms by which phenylephrine terminates some formsof VT.8 Although a cholinergic mode of action was stronglysuspected, it had not been proven. The present demonstra-tion that edrophonium potentiated and atropine reduced or
prevented the capacity of phenylephrine to break VTprovides evidence that a cholinergic mechanism is at least inpart responsible for this action of phenylephrine.9 However,these observations do not permit conclusions regardingother possible concomitant modes of action such as a) reflexwithdrawal of sympathetic drive,11 b) direct membrane
LlA
ControlII...; l.i-. -- iSM
B
Post 20Mg Edrophonium CSM
C
Post SMg Propranolol CSM
D #
effect,12' 13 and c) myocardial stretch by the pressure
response.' It is entirely possible that other types of ventric-ular arrhythmias may respond predominantly throughphenylephrine's other myocardial effects. Verrier et al.1'have shown that the ability of phenylephrine to raise ventric-ular fibrillatory threshold in the intact dog is mediated by a
reduction in sympathetic drive and not by enhanced vagaldrive.The response of the VT process to CSM provides some
sensitive insights into the interplay between the parasympa-thetic and sympathetic systems. Like phenylephrine, CSMhas vagotonic and sympatholytic effects.16 Carotid sinusmassage by itself did not interrupt VT. However, CSMcould terminate VT provided that either vagal tone was
AA
FIGURE 9. Patient TB. Recordings of lead I(L1) at 25 mm/sec. Panel A) control strip of VTprior to any intervention. Panel B) CSM was
applied slowing breaking VT.
Panel C) 30 sec after administration ofedrophonium HCI 20 mg, i. v. The VT rate slowedfrom 180 to 150 beats/min and CSM furtherslowed, then broke the VT. The closely coupled
L ---1 VPB in this panel is ofsimilar morphology to thatduring VT. Panel D) Fiye minutes after ad-
ministration of propranolol 5 mg, i. v. duringanother episode of VT, the rate is again slowerthan during control. Application of CSM againslowed the rate further prior to breaking the VT.
BAE I Ij1. I. . . .
T 1. F- I" p -T r I T -,
389
i . . -1,
by guest on May 20, 2018
http://circ.ahajournals.org/D
ownloaded from

VOL 56, No 3, SEPTEMBER 1977
enhanced by edrophonium pretreatment or sympathetic tonewas antagonized by propranolol pretreatment.
Inasmuch as both phenylephrine and CSM sharevagotonic and sympatholytic properties, the relative impor-tance of the two effects in the termination of VT remains un-resolved by our observations. It appears, however, that thetwo mechanisms may in fact be additive in the sense that anincrease in the intensity of either may dampen the require-ment for the other and it remains to be determined whether astrong enough pure vagal stimulus will by itself break VT atany level of sympathetic tone. A similar electrophysiologicinterplay between vagal and sympathetic influences hasrecently been shown by Kolman et al.'9 Using intact dogs,they showed that vagal stimulation could restore to normalthe ventricular fibrillatory threshold which had been loweredby prior sympathetic nerve stimulation.
There is mounting evidence from different sources whichsuggests that the vagus nerve may modulate the electricalproperties of ventricular tissues. Dressel and Sutter20 haveshown that stimulation of the distal cut vagus nerve in dogscan abolish premature ventricular beats which are inducedby cyclopropane-epinephrine mixtures. Bailey et al.2'demonstrated that automaticity in His bundle and proximalbundle branch cells is depressed by acetylcholine. Spear andMoore22 have shown that the ventricular pacemaker rate inexperimentally induced heart block may be reduced by vagalstimulation. Kent et al.5 have shown that cholinergic in-fluences raise the ventricular fibrillation threshold in dogswith experimental myocardial infarction while anti-cholinergic interventions reduce ventricular fibrillationthreshold.
In addition, since several groups of investigators haveidentified histologically the presence of vagal nerve fiberswithin the ventricular septum of dogs, cats and man,23-25 it isconceivable that any vagally sensitive VT process may in-volve this region in a crucial way.
It is not possible from our limited experience to date tospeculate how frequently or what type of VT is likely to ter-minate with the maneuvers herein described. The constraintsimposed by our selection criteria limited our observations towhat may be a homogeneous group of "idiopathic"recurrent VT. Because of the acute rises in blood pressurewhich result from phenylephrine administration, this formof testing or treatment will have to be used with great discre-tion in the more common cases of VT which occur in the set-tings of coronary artery disease or left ventricular dysfunc-tion of diverse causes. It is of interest that all four cases ofVT were easily started by exercise and the maneuverssuccessfully used to convert VT in these patients would tendto counter the autonomic effects of exercise. It is thus possi-ble that the relative balance between vagotonic and sym-patholytic requirements for conversion of a given VT mayparallel the balance between vagolytic and sympathetic in-fluences incurred during its induction. This possiblerelationship requires further investigation.
Termination of VT by vagal maneuvers has not to datebeen a clinically recognized entity. In view of the frequencywith which vagal maneuvers are used in the clinicaldiagnosis of tachyarrhythmias, the elusiveness of thedescribed findings is notable. This could be explained in twoways. First, since it is widely accepted that a wide QRS com-
plex tachycardia which breaks or slows with vagalmaneuvers is of supraventricular origin,' it is likely that atleast some episodes of VT might have been erroneouslylabelled to be supraventricular purely on the basis of theirresponse to vagal maneuvers. Second, it appears that thedegree of cardiac vagal drive required to end VT in our casesmay be very considerable. This is reflected in the high dosesof anticholinesterase employed in tandem with CSM as wellas the high vagal potency of the pressor agent used. In fact,our failure to break VT with CSM in conjunction withedrophonium in our previously described cases of phenyle-phrine terminated VT8 seems to have been related to the useof inadequate doses of edrophonium. This occurred despitethe use of doses (10 mg) which provided a clear vagal end-point in the form of selective slowing of the atrial rate. Thisunderscores the fact that enhanced vagal drive sufficient toaffect supraventricular structures may not be adequate toalso influence ventricular tissue.Our findings should in no way be construed as under-
mining the general usefulness of vagal interventions in theclinical differentiation of wide QRS complex tachycardias.However, when unusually potent vagal stimuli are requiredto break a wide QRS complex tachycardic process, the clini-cian should be alerted to the possibility of VT. Furthermore,in attempting to break VT with phenylephrine, the concomi-tant use of edrophonium should increase both the successrate and safety in terms of the maximal pressor responserequired.
References1. Bellet S: Clinical Disorders of the Heart Beat, ed 3. Philadelphia, Lea
and Febiger, 19712. Friedberg CK: Diseases of the Heart, ed 3. Philadelphia, WB Saunders,
19663. Levine HD: Vagal stimulation in the presence of supraventricular
mechanisms. In Mechanisms and Therapy of Cardiac Arrhythmias,edited by Dreifus LS, Likoff W. New York, Grune & Stratton, 1966
4. Corr PG, Gillis RA: Role of the vagus nerves in the cardiovascularchanges induced by coronary occlusion. Circulation 49: 86, 1973
5. Kent KM, Smith ER, Redwood DR, Epstein SE: Electrical stability ofacutely ischemic myocardium: Influences of heart rate and vagal stimu-lation. Circulation 47: 86, 1973
6. Myers RW, Pearlman AS, Hyman RA, Goldstein RA, Kent KM, Golds-tein FA, Epstein SE: Beneficial effects of vagal stimulation and bradycar-dia during experimental acute myocardial ischemia. Circulation 49: 943,1974
7. Olson HG, Miller RR, Dasilva 0, Amsterdam EA, Mason T: Vagalstimulation in patients with acute myocardial infarction: Antiarrhythmicand hemodynamic effects of edrophonium. (abstr) Circulation 49, 50:(suppl III): 111-33, 1974
8. Waxman MB, Downar E, Berman ND, Felderhof CH: Phenylephrine(neo-synephrine) terminated ventricular tachycardia. Circulation 50: 656,1974
9. Carrier 0 Jr: Pharmacology of the Peripheral Autonomic NervousSystem. Chicago, Year Book Medical Publishers, 1972
10. Peuch P, Grolleau R, Fijac E, Posner J: The diagnosis of supraventric-ular arrhythmias and the differentiation between supraventriculartachycardias with aberrant conduction and ventricular tachycardias. InSymposium on Cardiac Arrhythmias, edited by Sandoe E, Flensted-Jensen E, Elesen KH, Sodertalje, Sweden, AB Astra, 1970, p 199
11. Heymans C, Neil E: Reflexogenic Areas of the Cardiovascular System.London, J and A Churchill Ltd., 1958
12. Govier WC: Prolongation of the myocardial functional refractory periodby phenylephrine. Life Sci 6: 1367, 1967
13. Benfey BG, Varma DR: Interactions of sympathomimetic drugs,propranolol and phentolamine, in atrial refractory period and contrac-tility. Br J Pharmacol 30: 603, 1967
14. Monroe RD, Lafarge CG, Gamble WJ, Rosenthal A, Honda S: Left ven-tricular pressure volume relations and performance as affected by suddenincreases in developed pressure. Circ Res 22: 333, 1968
15. Verrier R, Calvert A, Lown B, Axelrod P: Effect of acute blood pressureelevation on the ventricular fibrillation threshold. Am J Physiol 226: 893,1974
CIRCULATION390
by guest on May 20, 2018
http://circ.ahajournals.org/D
ownloaded from
DETECTION OF LVH WITH RBBB/Holt, Barnard, Kramer
16. Eab HW, Green JH, Neil E: A comparison of the effects of pulsatile andnonpulsatile blood flow through the carotid sinus on the reflexogenic ac-tivity of the sinus baroreceptors in the cat. J Physiol 118: 509, 1952
17. Sarnoff SJ, Gilmore JP, Brockman SK, Mitchell JH, Linden RJ:Regulation of ventricular contraction by the carotid sinus: Its effect onatrial and ventricular dynamics. Circ Res 8: 1123, 1960
18. Berkowitz WD, Scherlag BJ, Stein E, Damato AN: Relative roles ofsympathetic and parasympathetic nervous systems in the carotid sinusreflex in dogs. Circ Res 24: 447, 1969
19. Kolman BS, Verrier RL, Lown B: The effect of vagus nerve stimulationupon vulnerability of the canine ventricle. Role of sympathetic-parasympathetic interaction. Circulation 52: 578, 1975
20. Dresel PE, Sutter MC: Factors modifying cyclopropane-epinephrine car-diac arrhythmias. Circ Res 9: 1284, 1961
21. Bailey J, Greenspan K, Elizari MV, Anderson GJ, Fisch C: The effects ofacetylcholine on automaticity and conduction within the proximal His-Purkinje specialized conduction system. Circ Res 20: 210, 1972
22. Spear JF, Moore EW: Influence of brief vagal and stellate nerve stimula-tion and pacemaker activity and conduction within the atrioventricularconduction system of the dog. Circ Res 32: 27, 1973
23. Joo F, Csillik B: Cholinesterase activity of intercalated discs in mam-malian heart muscle. Nature (London) 193: 1192, 1962
24. Jacobowitz D, Cooper T, Barner HB: Histochemical and chemicalstudies of the localization of adrenergic and cholinergic nerves in normaland denervated cat hearts. Circ Res 20: 289, 1967
25. Kent KM, Epstein SE, Cooper T, Jacobowitz DM: Cholinergic innerva-tion of the canine and human ventricular conducting system. Circulation50: 948, 1974
A Study of the Human Heartas a Multiple Dipole SourceIV. Left Ventricular Hypertrophy
in the Presence of Right Bundle Branch Block
JOHN H. HOLT, JR., M.D., ANTHONY C. L. BARNARD, D. SC.,
AND JOHN 0. KRAMER, JR., M.S.
SUMMARY This report concerns the task of electrocardio-graphic (ECG) diagnosis and quantitation of left ventricular hyper-trophy (LVH) in patients with right bundle branch block (RBBB). In36 patients with RBBB the left ventricular mass (LVM) of eachpatient was independently known from quantitative biplaneangiography. Two ECG techniques, standard 12-lead ECG and mul-tiple dipole electrocardiography (MDECG), were evaluated. Indiagnosing LVH, the best performance of the several standard ECGcriteria was sensitivity = 29%, specificity = 100%, and that of theMDECG was sensitivity = 94%, specificity = 96%. In quantitating
THE PRESENT REPORT deals with the continuingassessment of an advanced electrocardiographic (ECG)method referred to as multiple dipole ECG (MDECG).
In 1969 the present authors published a report' on theMDECG and its ability to detect and quantitate LVH. Theresults were established using a series of 72 patients withnormal conduction. A strong correlation (predicted theo-retically) was demonstrated experimentally between thedipole activity in the left ventricle and septal segments,which is a quantity derived from MDECG, and the left ven-tricular mass (LVM) derived from quantitative biplaneangiocardiography.2 The regression equation obtained fromthe correlation can now be used to predict LVM on the basisof MDECG measurements. A prospective study using a new
From the Departments of Medicine and Information Sciences, School ofMedicine, University of Alabama in Birmingham, and the Veterans Ad-ministration Hospital, Birmingham, Alabama.
This work was aided by research funds from the Veterans Administration,Research Grants HE-11310 and RR-00145 from the National Institutes ofHealth and a Grant-in-Aid from the Alabama Heart Association.
Address for reprints: John H. Holt, Jr., M.D., Veterans AdministrationHospital, 700 South 19th Street, Birmingham, Alabama 35233.
Received February 28, 1977; revision accepted April 12, 1977.
LVH, the standard ECG gave a correlation with LVM of r = 46%and a standard error of estimate of 98 g. The corresponding figuresfor the MDECG were r = 81% and the root mean square predictionerror = 64 g.
These results confirm other studies showing that the conventionalECG is of only marginal value in the task of diagnosing LVH in thepresence of RBBB. In contrast, the MDECG performs well both inthis task and that of quantitating LVH. The results provide furthersupport of the accuracy of the model of the cardiac electricalgenerator and volume conductor used in the MDECG method.
series of 113 patients with normal conduction has provedthat the prediction has a root mean square error of 66 g insuch patients.3The effectiveness of an ECG technique for determining
the presence or absence of some particular cardiac condi-tion, or combination of conditions, may be studied by trialson a series of patients. This series must be composed ofpatients for whom the presence or absence of the conditionsis independently and reliably known. Only then can the ac-curacy of the ECG predictions be assessed.The present paper reports results on a series of patients
with right bundle branch block (RBBB) and compares theability of the standard 12-lead ECG and the MDECG todetect and quantitate LVH in this situation. In addition, thisstudy provides further validation of the modeling assump-tions used in the MDECG method. The non-ECG methodused to determine the presence and degree of LVH wasquantitative biplane angiography.2
Materials and Methods
To date, 126-lead ECG data have been recorded on 1,234patients and normal subjects, as part of the MDECG
391
by guest on May 20, 2018
http://circ.ahajournals.org/D
ownloaded from

M B Waxman and R W WaldTermination of ventricular tachycardia by an increase in cardiac vagal drive.
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1977 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.56.3.385
1977;56:385-391Circulation.
http://circ.ahajournals.org/content/56/3/385the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on May 20, 2018
http://circ.ahajournals.org/D
ownloaded from





























