Embed Size (px)
Citation preview

TENOFOVIR DFTENOFOVIR DF
DIVISION OF ANTIVIRAL DRUG DIVISION OF ANTIVIRAL DRUG PRODUCTS’ ADVISORY COMMITTEEPRODUCTS’ ADVISORY COMMITTEE
OCTOBER 3, 2001OCTOBER 3, 2001

Advisory Committee IssuesAdvisory Committee Issues
• Treatment indicationTreatment indication
• Nonclinical and clinical Nonclinical and clinical assessment of the effects of assessment of the effects of Tenofovir DF on boneTenofovir DF on bone
• Analysis of resistance dataAnalysis of resistance data
• Design ofDesign of trials for traditional trials for traditional approvalapproval

Advisory Committee IssuesAdvisory Committee Issues
Proposed treatment indication:Proposed treatment indication:
VIREADVIREADTMTM , in combination with other antiretroviral agents, , in combination with other antiretroviral agents, is indicated for the treatment of HIV-infected adults. This is indicated for the treatment of HIV-infected adults. This indication is based on analyses of plasma HIV-1 RNA indication is based on analyses of plasma HIV-1 RNA levels and CD4 counts in two controlled trials of VIREADlevels and CD4 counts in two controlled trials of VIREADTMTM of 24 and 48 weeks duration in treatment experienced of 24 and 48 weeks duration in treatment experienced adults with evidence of HIV-1 replication despite ongoing adults with evidence of HIV-1 replication despite ongoing antiretroviral therapy. At present, there are no results antiretroviral therapy. At present, there are no results from controlled trials evaluating the effect of tenofovir on from controlled trials evaluating the effect of tenofovir on clinical progression of HIV.clinical progression of HIV.

Advisory Committee IssuesAdvisory Committee Issues
• Treatment indicationTreatment indication– Pivotal studies 902 and 907 were conducted in a Pivotal studies 902 and 907 were conducted in a
treatment experienced adult populationtreatment experienced adult population• on stable ARV therapy for at least 8 weekson stable ARV therapy for at least 8 weeks• median duration of therapy of ~ 4 - 5 yearsmedian duration of therapy of ~ 4 - 5 years
• mean baseline viral load = 3.4 logmean baseline viral load = 3.4 log1010
• mean baseline CD4 counts = 410 cells/mmmean baseline CD4 counts = 410 cells/mm33 • baseline resistance mutations - NRTI(94%), PI(58%), baseline resistance mutations - NRTI(94%), PI(58%),
NNRTI(~40%)NNRTI(~40%)
– Requesting AC input regarding labeled indicationRequesting AC input regarding labeled indication
Advisory Committee IssuesAdvisory Committee Issues
• Bone EffectsBone Effects– BMD reductions/osteomalacia were observed BMD reductions/osteomalacia were observed
in 3 speciesin 3 species– Mechanism not fully definedMechanism not fully defined– Clinical trial data limited for BMDClinical trial data limited for BMD– Seeking advice regarding:Seeking advice regarding:
• implications of nonclinical and clinical bone dataimplications of nonclinical and clinical bone data• recommendations for additional studiesrecommendations for additional studies• monitoring plansmonitoring plans

Advisory Committee IssuesAdvisory Committee Issues
• Virology dataVirology data– VIREADVIREADTMTM NDA contains more virology data NDA contains more virology data
than other NDAthan other NDA– Many analyses evaluating HIV RNA Many analyses evaluating HIV RNA
response by baseline phenotype and response by baseline phenotype and genotypegenotype
– Seeking AC comments on:Seeking AC comments on:• clinical resistance analysesclinical resistance analyses• inclusion in product labelinginclusion in product labeling

VIREADVIREADTMTM NDA NDA
• Submitted in May 2001Submitted in May 2001– submitted under submitted under accelerated approvalaccelerated approval
regulations regulations • for serious and life-threatening conditionsfor serious and life-threatening conditions• provide meaningful therapeutic benefit over existing provide meaningful therapeutic benefit over existing
therapiestherapies• drug has an effect on a surrogate endpoint that is drug has an effect on a surrogate endpoint that is
reasonably likely to predict clinical benefit or on a reasonably likely to predict clinical benefit or on a clinical endpoint other than survival or irreversible clinical endpoint other than survival or irreversible morbiditymorbidity
• DAVDP requires 2 adequate and well-controlled trials DAVDP requires 2 adequate and well-controlled trials of 24 weeks durationof 24 weeks duration

Advisory Committee IssuesAdvisory Committee Issues
• Traditional approval plansTraditional approval plans– Continued marketing is subject to the need to Continued marketing is subject to the need to
confirm findings to establish clinical benefitconfirm findings to establish clinical benefit– DAVDP requires 2 studies of 48 weeks duration to DAVDP requires 2 studies of 48 weeks duration to
support traditional approvalsupport traditional approval• Study 903 is being conducted in naïve subjects and is Study 903 is being conducted in naïve subjects and is
fully enrolledfully enrolled• Compares tenofovir DF to stavudine on a background Compares tenofovir DF to stavudine on a background
of lamivudine and efavirenzof lamivudine and efavirenz
– Seeking AC advice regarding design of second Seeking AC advice regarding design of second study in pediatric populationstudy in pediatric population

Advisory Committee AgendaAdvisory Committee Agenda• 9:00 a.m.9:00 a.m. Gilead PresentationGilead Presentation
• 9:45 a.m.9:45 a.m. FDA PresentationFDA Presentation
• 10:30 a.m.10:30 a.m. BreakBreak
• 10:45 a.m.10:45 a.m. DiscussionDiscussion
• 12:00 p.m.12:00 p.m. LunchLunch
• 1:00 p.m. 1:00 p.m. Open Public HearingOpen Public Hearing
• 2:00 p.m.2:00 p.m. Continue Discussion and Questions to the Continue Discussion and Questions to the CommitteeCommittee
• 5:00 p.m.5:00 p.m. AdjournAdjourn

NDA 21-356NDA 21-356Tenofovir Disoproxil FumarateTenofovir Disoproxil Fumarate
Kimberly Struble, PharmDKimberly Struble, PharmD
Senior Regulatory Review OfficerSenior Regulatory Review Officer
Division of Antiviral Drug ProductsDivision of Antiviral Drug Products

Presentation OutlinePresentation Outline
• NDA Submission OverviewNDA Submission Overview• Efficacy SummaryEfficacy Summary• Clinical Virology ResultsClinical Virology Results• Nonclinical Assessment of Bone Abnormalities Nonclinical Assessment of Bone Abnormalities
- Jim Farrelly, Ph.D.- Jim Farrelly, Ph.D.• Clinical Assessment of Bone AbnormalitiesClinical Assessment of Bone Abnormalities• Second Study for Traditional ApprovalSecond Study for Traditional Approval• Summary of Regulatory IssuesSummary of Regulatory Issues

NDA OverviewNDA Overview
• Submission Date: May 1, 2001Submission Date: May 1, 2001
• Proposed Dosage: Tenofovir DF 300 Proposed Dosage: Tenofovir DF 300 mg once dailymg once daily
• Indication Sought: Treatment of HIV Indication Sought: Treatment of HIV infectioninfection

NDA Submission:NDA Submission:Four Clinical StudiesFour Clinical Studies
• Supportive:Supportive:– 901: Phase 2 dose finding (35 days)901: Phase 2 dose finding (35 days)– 908: Compassionate Use Safety908: Compassionate Use Safety
• PrincipalPrincipal– 902 and 907: Randomized, Double-blind 902 and 907: Randomized, Double-blind
Placebo Controlled (24 weeks)Placebo Controlled (24 weeks)

Principal Studies: 902 and 907Principal Studies: 902 and 907
• Similar Study DesignsSimilar Study Designs– Safety and Efficacy of TNV vs PBO when Safety and Efficacy of TNV vs PBO when
added to stable ARV regimen in treatment added to stable ARV regimen in treatment experienced patientsexperienced patients
• Similar baseline characteristicsSimilar baseline characteristics
• Differences in baseline HIV RNADifferences in baseline HIV RNA– 902: Baseline HIV RNA 400-100,000 902: Baseline HIV RNA 400-100,000
copies/mLcopies/mL– 907: Baseline HIV RNA 400-10,000 copies/mL907: Baseline HIV RNA 400-10,000 copies/mL

Primary Efficacy EndpointPrimary Efficacy Endpoint
• Primary endpoint = Time weighted change Primary endpoint = Time weighted change in login log10 10 HIV RNA over 24 weeks (DAVGHIV RNA over 24 weeks (DAVG2424))
• DAVG is an acceptable endpoint for DAVG is an acceptable endpoint for evaluating virologic responses in evaluating virologic responses in treatment experienced patients, such as treatment experienced patients, such as those enrolled in 902 and 907those enrolled in 902 and 907
• Secondary endpoints = Proportion < 400 Secondary endpoints = Proportion < 400 and 50 copies/mLand 50 copies/mL

HIV RNA Results:HIV RNA Results:Placebo vs Tenofovir 300 mgPlacebo vs Tenofovir 300 mg

Mean Change From Mean Change From Baseline: HIV RNABaseline: HIV RNA
-0.8
-0.6
-0.4
-0.2
0
0.2
TNF: 907PBO: 907TNF: 902PBO: 902
2 4 8 12 24
WEEKS
16 20 0
DAVG24= - 0.58
DAVG24= - 0.61

Proportion < 400 and Proportion < 400 and < 50< 50 copies/mL copies/mL
0
20
40
60
80
100
0 2 4 8 12 16 20 24
TNF < 400TNF < 50PBO < 400PBO < 50
0
20
40
60
80
100
0 2 4 8 12 16 20 24
TNF < 400TNF < 50PBO < 400PBO < 50
Study 902 Study 907
Weeks Weeks
CD4 Cell Count Results:CD4 Cell Count Results:Placebo vs Tenofovir 300 mgPlacebo vs Tenofovir 300 mg

CD4 Response: Study 902CD4 Response: Study 902
-20
-10
0
10
20
30
TNF PBO
4 8 12 24Weeks
DAVG24= -3.6
DAVG24= -10.5

CD4 Response: Study 907CD4 Response: Study 907
-20
-10
0
10
20
30
TNF: 907 PBO: 907
4 8 12 16 20 24Weeks
DAVG24= +12.6
DAVG24= -10.6

CD4 Response by Baseline CD4 Response by Baseline CD4: Studies 902 and 907CD4: Studies 902 and 907
BASELINECD4
PBO(N=210)
TNF(N=422)
NET TXEFFECT
DIFF.
< 200 -6.5 +20 +26.5
> 200 -10 +7.9 +17.9+8.6
P=0.65

Efficacy SummaryEfficacy Summary
• Mean viral load reductions similar for Mean viral load reductions similar for 902 and 907 (Mean DAVG 0.5 - 0.6)902 and 907 (Mean DAVG 0.5 - 0.6)
• < 400 and < 50 copies/mL< 400 and < 50 copies/mL– numerical differences: 902numerical differences: 902– statistically significant differences: 907statistically significant differences: 907
• Modest CD4 increases in study 907Modest CD4 increases in study 907• No differences for CD4 in study 902 No differences for CD4 in study 902
over 24 weeksover 24 weeks
Efficacy Summary (cont.)Efficacy Summary (cont.)
• Study population in 902 and 907 may not Study population in 902 and 907 may not be optimal for observing large increases be optimal for observing large increases in CD4, given only one new drug added in CD4, given only one new drug added to stable regimento stable regimen
• Addition of one new agent did not Addition of one new agent did not produce substantial increases in CD4 produce substantial increases in CD4 over timeover time
• Further evaluations of CD4 in studies Further evaluations of CD4 in studies with different designs are neededwith different designs are needed

Clinical Virology ResultsClinical Virology Results

Clinical VirologyClinical Virology
• Applicant: HIV RNA response by Applicant: HIV RNA response by prospectively defined baseline mutation prospectively defined baseline mutation subgroupssubgroups
• FDA: Exploratory analyses to further FDA: Exploratory analyses to further investigate HIV RNA response according to investigate HIV RNA response according to presence or absence of specific NRTI presence or absence of specific NRTI mutationsmutations– Determine if specific mutations or mutational Determine if specific mutations or mutational
patterns affected responsepatterns affected response to tenofovirto tenofovir

Clinical Virology: Clinical Virology: Limitations of FDA AnalysesLimitations of FDA Analyses
• Large number of potential comparisons limits Large number of potential comparisons limits ability to test for statistical significanceability to test for statistical significance
• Limited # of patients for some primary NRTI Limited # of patients for some primary NRTI and multi-drug resistant mutations to and multi-drug resistant mutations to determine clinical significancedetermine clinical significance
• Given these limitations FDA is soliciting Given these limitations FDA is soliciting feedback on the types of exploratory analyses feedback on the types of exploratory analyses conducted and recommendations for labelingconducted and recommendations for labeling

Genotypic ResultsGenotypic Results

Genotypic ResultsGenotypic Results• HIV RNA response by presence or absence HIV RNA response by presence or absence
of thymidine analogue mutations (TAMs)of thymidine analogue mutations (TAMs)• TAMs are defined as TAMs are defined as
– M41LM41L– D67ND67N– K70RK70R– L210WL210W– T215Y/FT215Y/F– K219Q/E/NK219Q/E/N

-0.9 -0.7 -0.5 -0.3 -0.1 0.1 0.3
67 +
67 -
70 +
70 -
219 +
219 -
HIV RNA Response by Baseline TAMs
Mean DAVG24 (N)
-0.53 (79)
-0.62 (143)
-0.71 (67)
-0.54 (155)
-0.60 (57)
-0.58 (165)

-1 -0.8 -0.6 -0.4 -0.2 0 0.2
Mean DAVG24 (N)
-0.80 (116)
-0.35 (106)
-0.70 (176)
-0.17 (46)
-0.78 (141)
-0.26 (81)
215 -
215 +
210 -
210 +
41 -
41 +
HIV RNA Response by Baseline TAMs

-1.1 -0.9 -0.7 -0.5 -0.3 -0.1 0.1 0.3 0.5
No 41 or 210
41 or 210
215 -
Impact of Impact of 215 Mutation215 Mutation on HIV on HIV RNA ResponseRNA Response
Mean DAVG24 (N)
-0.25 (82)
-0.70 (25)
-0.80 (116)

-1 -0.8 -0.6 -0.4 -0.2 0 0.2 0.4
No 41 or 210
41 or 210
Mean DAVG24 (N)
-0.79 (139)
-0.26 (93)
Impact of Impact of 41 or 210 Mutation41 or 210 Mutation on HIV RNA Responseon HIV RNA Response
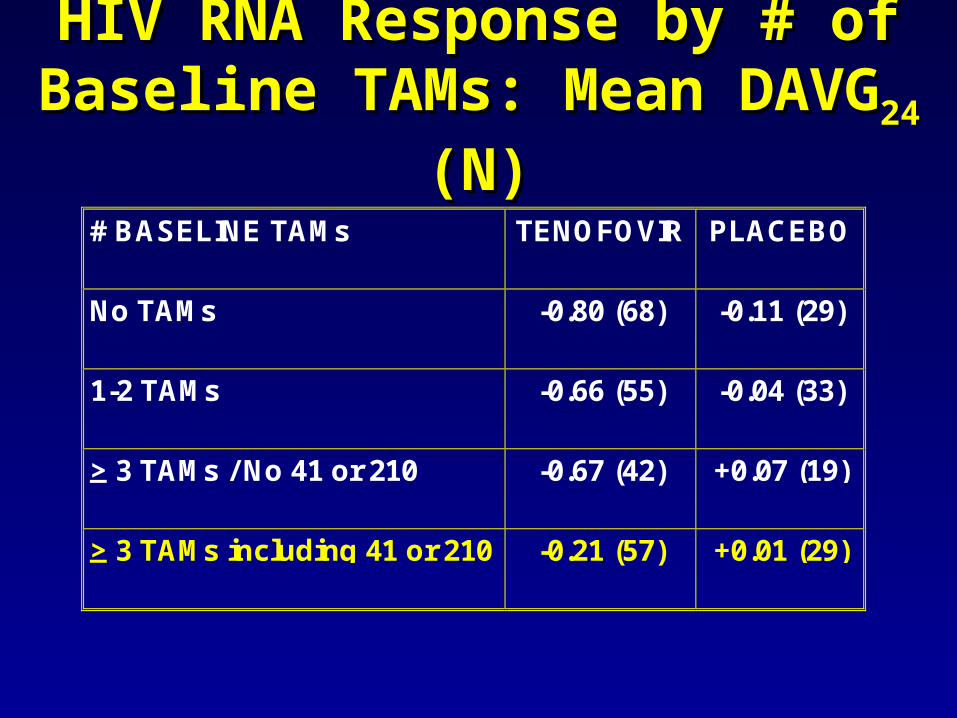
HIV RNA Response by # of HIV RNA Response by # of Baseline TAMs: Mean DAVGBaseline TAMs: Mean DAVG2424 (N) (N)
# BASELINE TAMs TENOFOVIR PLACEBO
No TAMs -0.80 (68) -0.11 (29)
1-2 TAMs -0.66 (55) -0.04 (33)
> 3 TAMs / No 41 or 210 -0.67 (42) +0.07 (19)
> 3 TAMs including 41 or 210 -0.21 (57) +0.01 (29)

Other NRTI Mutations and HIV Other NRTI Mutations and HIV RNA ResponseRNA Response
• L74V/I affects tenofovir efficacyL74V/I affects tenofovir efficacy– DAVGDAVG24 24 = -0.17 (n=18)= -0.17 (n=18)
– Rates similar regardless if 41 or 210 mutation present Rates similar regardless if 41 or 210 mutation present with 74 (-0.12 to -0.19)with 74 (-0.12 to -0.19)
• K65R mutation reduces susceptibility to tenofovir K65R mutation reduces susceptibility to tenofovir in vitroin vitro– DAVGDAVG24 24 = 0 (N=6)= 0 (N=6)
• More data needed to make any definitive More data needed to make any definitive conclusionsconclusions

Phenotypic ResultsPhenotypic Results

Phenotypic AnalysesPhenotypic Analyses
• To determine if tenofovir or other To determine if tenofovir or other NRTI baseline susceptibility affected NRTI baseline susceptibility affected responseresponse
• Baseline TNF susceptibility:Baseline TNF susceptibility:– TNF TNF << 4 fold 4 fold
• DAVGDAVG24 24 = -0.61 (n=91)= -0.61 (n=91)
– TNF > 4 foldTNF > 4 fold• DAVGDAVG24 24 = -0.12 (N=9)= -0.12 (N=9)

Resistance SummaryResistance Summary• Genotypic data suggest potential for some Genotypic data suggest potential for some
cross resistance between tenofovir and cross resistance between tenofovir and specific NRTI mutations or patterns of specific NRTI mutations or patterns of mutationsmutations
• However too few patients expressing some However too few patients expressing some primary NRTI or multi-drug resistant NRTI primary NRTI or multi-drug resistant NRTI mutations to determine clinical significancemutations to determine clinical significance
• No cross resistance between tenofovir and No cross resistance between tenofovir and lamivudinelamivudine

Resistance SummaryResistance Summary• 41 or 210 mutation diminished responses, whereas 41 or 210 mutation diminished responses, whereas
67, 70, 215 and 219 did not67, 70, 215 and 219 did not• Number and types of TAMs affect tenofovir efficacyNumber and types of TAMs affect tenofovir efficacy
– Efficacy reduced for Efficacy reduced for >> 3 TAMs which include M41L or 3 TAMs which include M41L or L210WL210W
• K65R and L74V/I mutation may affect tenofovir K65R and L74V/I mutation may affect tenofovir efficacyefficacy
• Reduced susceptibility to TNF (> 4 fold) at baseline Reduced susceptibility to TNF (> 4 fold) at baseline diminishes tenofovir efficacydiminishes tenofovir efficacy

Safety SummarySafety Summary

Safety SummarySafety Summary• Treatment with TNF appears to be well toleratedTreatment with TNF appears to be well tolerated• Most common AEs: Most common AEs: asthenia (19%), headache
(14%), diarrhea (22%), nausea (20%) and pharyngitis (18%)
• GI events greater in TNF group vs PBO – diarrhea (22% vs 17%) – flatulence (6% vs 2%) – nausea (20% vs 15%) – vomiting (12% vs 6%)

Nonclinical Assessment of Nonclinical Assessment of Bone AbnormalitiesBone Abnormalities
James G. Farrelly, Ph.D.James G. Farrelly, Ph.D.
Pharmacology SupervisorPharmacology Supervisor

Toxicity in Rat and Dog Toxicity in Rat and Dog Four Week Gavage StudiesFour Week Gavage Studies
• Doses up to 500 mg/kg/day in ratsDoses up to 500 mg/kg/day in rats– Little toxicity seenLittle toxicity seen
• Doses up to 30 mg/kg/day in dogsDoses up to 30 mg/kg/day in dogs– Minor toxicity in kidney but no Minor toxicity in kidney but no
bone toxicitybone toxicity

Toxicity in Rat Toxicity in Rat 42 Week Gavage Study42 Week Gavage Study
• Doses @ 0, 30, 100, 300, 1000 mg/kg/d for 42 wks with 13 Doses @ 0, 30, 100, 300, 1000 mg/kg/d for 42 wks with 13 wk recovery and a 13 week interim evaluationwk recovery and a 13 week interim evaluation
• Bone Effects:Bone Effects: Bone mineral content and densityBone mineral content and density Cortical thickness of femurCortical thickness of femur Deoxypyridinoline at three highest doses Deoxypyridinoline at three highest doses Osteocalcin at the two highest doses Osteocalcin at the two highest doses Plasma phosphorus Plasma phosphorus Urinary calcium and phosphorus Urinary calcium and phosphorus PTH PTH

Toxicity in Dog 42 Week Gavage Toxicity in Dog 42 Week Gavage StudyStudy
• Doses @ 0, 3, 10, and 30 mg/kg/d for Doses @ 0, 3, 10, and 30 mg/kg/d for 42 wks with 13 wk recovery and a 13 42 wks with 13 wk recovery and a 13 week interim evaluationweek interim evaluation
• Bone EffectsBone Effects Bone mineral content and density Bone mineral content and density Urinary N-telopeptide Urinary N-telopeptide Urinary calcium and phosphorus Urinary calcium and phosphorus Bone specific ALP Bone specific ALP 1,25-dihydroxy vitamin D1,25-dihydroxy vitamin D33
Toxicity in Mouse Toxicity in Mouse 13 Week Gavage Study13 Week Gavage Study
• Range-finding study to determine the Range-finding study to determine the maximum tolerated dose for a two year maximum tolerated dose for a two year carcinogenicity studycarcinogenicity study– Doses studied = 0, 100, 300, 600 mg/kg/dDoses studied = 0, 100, 300, 600 mg/kg/d
• Toxicity was seen in the kidney and Toxicity was seen in the kidney and duodenumduodenum
• Carcinogenicity study is still ongoingCarcinogenicity study is still ongoing

Intravenous Study in Cynomolgus Intravenous Study in Cynomolgus MonkeysMonkeys
• Monkeys were dosed for 14 days Monkeys were dosed for 14 days by the intravenous route at doses by the intravenous route at doses up to 25 mg/kg/day with tenofovirup to 25 mg/kg/day with tenofovir
• No bone toxicities were seen in No bone toxicities were seen in this studythis study
• There were treatment findings in There were treatment findings in the kidneysthe kidneys

Rhesus Monkey Efficacy StudiesRhesus Monkey Efficacy Studies
• Studies designed to assess efficacy Studies designed to assess efficacy against SIVagainst SIV
• Doses Studied = 10 and 30 mg/kg/dayDoses Studied = 10 and 30 mg/kg/day
• Bone toxicities seen after 10 months Bone toxicities seen after 10 months dosingdosing
• NewbornNewborn monkeys showed earlier bone monkeys showed earlier bone toxicity when dosed at 30 mg/kg/daytoxicity when dosed at 30 mg/kg/day
• At 10 mg/kg/day, no bone toxicity was At 10 mg/kg/day, no bone toxicity was seen in newborns dosed for two yearsseen in newborns dosed for two years

Rhesus Monkey Efficacy Studies, Cont.Rhesus Monkey Efficacy Studies, Cont.
Bone ToxicityBone Toxicity• Seen as abnormal growth plates and trabecula Seen as abnormal growth plates and trabecula
of femurs and ribsof femurs and ribs• Also seen were bone deformities and Also seen were bone deformities and
displacements, rib fractures and reduced bone displacements, rib fractures and reduced bone density with bone lossdensity with bone loss
• Reduction in serum phosphorusReduction in serum phosphorus• Elevated ALPElevated ALP• Non-hyperglycemic glucosuria and proteinuriaNon-hyperglycemic glucosuria and proteinuria
• Serum calcium unchangedSerum calcium unchanged

Rhesus Monkey Efficacy Studies, Cont.Rhesus Monkey Efficacy Studies, Cont.
• It was concluded that treatment of It was concluded that treatment of rhesus monkeys at 30 mg/kg/day results rhesus monkeys at 30 mg/kg/day results in a mineralization defect in developing in a mineralization defect in developing and growing cortical boneand growing cortical bone
• The defect was considered to be The defect was considered to be osteomalaciaosteomalacia
• The defect was reversed by reducing the The defect was reversed by reducing the dose to 10 mg/kg/day or stopping dose to 10 mg/kg/day or stopping treatmenttreatment

Reproductive Toxicology StudiesReproductive Toxicology Studies
• No bone toxicity was seen in reproductive No bone toxicity was seen in reproductive toxicology studiestoxicology studies
• Rats dosed to 600 mg/kg/dayRats dosed to 600 mg/kg/day
• Rabbits dosed to 300 mg/kg/dayRabbits dosed to 300 mg/kg/day

ConclusionsConclusions
• Tenofovir and tenofovir DF induce Tenofovir and tenofovir DF induce bone toxicities in three animal species bone toxicities in three animal species consistent with a diagnosis of consistent with a diagnosis of osteomalaciaosteomalacia
• The mechanism is unknownThe mechanism is unknown

Conclusions, Cont.Conclusions, Cont.
The evidence from toxicology studies in The evidence from toxicology studies in three species as well as from a number of three species as well as from a number of in vivo and in vitro studies is consistent in vivo and in vitro studies is consistent with the hypothesis that the bone effects with the hypothesis that the bone effects are secondary to a negative phosphate are secondary to a negative phosphate balance associated with drug-related balance associated with drug-related impairment of intestinal phosphate impairment of intestinal phosphate absorption and/or renal reabsorption of absorption and/or renal reabsorption of phosphate and not a direct effect on bonephosphate and not a direct effect on bone

Clinical Assessment of Clinical Assessment of Bone AbnormalitiesBone Abnormalities

Animal Exposures in Relation Animal Exposures in Relation to Human Exposuresto Human Exposures
• Margin of safetyMargin of safety– BMD reduction in rats and dogs 6-10 BMD reduction in rats and dogs 6-10
times higher than human exposures times higher than human exposures (AUC)(AUC)
– Osteomalacia in monkeys 12 times Osteomalacia in monkeys 12 times higher than human exposures (AUC)higher than human exposures (AUC)
Clinical Assessment of Clinical Assessment of Bone AbnormalitiesBone Abnormalities
• No clinically significant changes in No clinically significant changes in phosphate, calcium, PTH or BMD phosphate, calcium, PTH or BMD observed over timeobserved over time– PTH and BMD only available for a small PTH and BMD only available for a small
subset of patientssubset of patients

Incidence of Clinical Incidence of Clinical Fractures: Fractures:
• 5.5% in study 9025.5% in study 902
• Proportion of patients with fracture Proportion of patients with fracture in study 902 is higher than that seen in study 902 is higher than that seen in FDA meta-analysis of 13 trialsin FDA meta-analysis of 13 trials 2% (202/10166)2% (202/10166)
• Observation may be due to small Observation may be due to small sample size but further investigation sample size but further investigation of potential safety signal warrantedof potential safety signal warranted

STUDIES 902 AND 907:FRACTURES/PATIENTS (#)
RATE (PERSON YR.)(95% CI)
TNF Placebo
0-6 months 6/7171.7
(0.6 – 3.8)
3/2103.2
(0.7 – 9.2)6-12 months 2/635
0.8(0.1 – 2.7)
0/110
(0 – 92.2)12-18 months 5/352
5(1.6 – 11.7)
0/40
(0- na)18-24 months 1/119
1.9(0.1 – 10.7)
-
> 24 months 1/922.9
(0.1 – 15.9)
-

Clinical Assessment of Clinical Assessment of Bone AbnormalitiesBone Abnormalities
• Review of entire non clinical and clinical safety Review of entire non clinical and clinical safety and PK data, it is unlikely TNF-related fractures and PK data, it is unlikely TNF-related fractures will occur over 48 weekswill occur over 48 weeks– Assuming mechanism is mediated by renal Assuming mechanism is mediated by renal
phosphate wasting or decreases in intestinal phosphate wasting or decreases in intestinal absorption of phosphateabsorption of phosphate
– No significant changes in renal parameters, in No significant changes in renal parameters, in particular phosphateparticular phosphate
– Rate of fractures does not increase over 6 month Rate of fractures does not increase over 6 month time intervalstime intervals

Clinical Assessment of Clinical Assessment of Bone AbnormalitiesBone Abnormalities
• Insufficient numbers of patients Insufficient numbers of patients receiving prolonged TNF treatment receiving prolonged TNF treatment and lack of control arm past 24 and lack of control arm past 24 weeks weeks
• Therefore difficult to conclude Therefore difficult to conclude whether or not TNF will cause clinical whether or not TNF will cause clinical fractures over time or if the risk will fractures over time or if the risk will increase over timeincrease over time

Traditional Approval:Traditional Approval:
Traditional Approval PlansTraditional Approval Plans
• Two studies required assessing HIV Two studies required assessing HIV RNA over 48+ weeksRNA over 48+ weeks
• First study: Treatment Naïve Patients First study: Treatment Naïve Patients – Study 903Study 903– TNF + 3TC + EFV vs D4T + 3TC + EFVTNF + 3TC + EFV vs D4T + 3TC + EFV
• Second study:Second study:– proposed in treatment experienced proposed in treatment experienced
childrenchildren

Two - Part Hybrid (N=100)Two - Part Hybrid (N=100)
Stable ARV
> 8 weeks
randomized
1:1
TNF
PBO
TNF
PBO
OBR wk 2
2 wks 46 wks
Endpoint: DAVG2 and DAVG48
Patient Population:• HIV RNA > 30,000 copies/mL• CD4% < 20% or <30% with OI in last 90 days• TX Experienced with at least 1 member of
each drug class

Summary of Regulatory Summary of Regulatory IssuesIssues

Summary of Regulatory Issues:Summary of Regulatory Issues:IndicationIndication
• Study population in studies 902 and 907 Study population in studies 902 and 907 quite selectquite select– antiretroviral experiencedantiretroviral experienced– mean baseline values 3.4 log and 410 cellsmean baseline values 3.4 log and 410 cells
Summary of Regulatory Issues:Summary of Regulatory Issues:IndicationIndication
• Committee discussion regarding most Committee discussion regarding most appropriate indicationappropriate indication– For the treatment of HIV infectionFor the treatment of HIV infection
• includes both treatment naïve or treatment includes both treatment naïve or treatment experienced patientsexperienced patients
– For the treatment of HIV infection in For the treatment of HIV infection in patients who have received prior patients who have received prior antiretroviral therapyantiretroviral therapy

Summary of Regulatory Issues: Summary of Regulatory Issues: Bone AbnormalitiesBone Abnormalities
• Non clinical bone toxicityNon clinical bone toxicity– Reductions in bone mineral density Reductions in bone mineral density
seen in 3 animal speciesseen in 3 animal species– Exact mechanism(s) unknown but may Exact mechanism(s) unknown but may
be due to renal phosphate wasting or be due to renal phosphate wasting or decrease in intestinal absorption of decrease in intestinal absorption of phosphatephosphate

Summary of Regulatory Issues:Summary of Regulatory Issues:Bone AbnormalitiesBone Abnormalities
• Clinical bone toxicityClinical bone toxicity– No clinically significant changes in No clinically significant changes in
phosphate, calcium , PTH or BMD observed phosphate, calcium , PTH or BMD observed over timeover time• PTH and BMD only available for a small subset of PTH and BMD only available for a small subset of
patientspatients
– Rates of fractures does not increase over 6 Rates of fractures does not increase over 6 month intervalsmonth intervals
• Controlled safety data in more patients for Controlled safety data in more patients for longer duration neededlonger duration needed

Summary of Regulatory Issues:Summary of Regulatory Issues:Bone AbnormalitiesBone Abnormalities
• Please provide your assessment of the Please provide your assessment of the nonclinical and clinical data with regard to nonclinical and clinical data with regard to bone effects.bone effects.
• Are there additional non clinical or clinical Are there additional non clinical or clinical studies that the applicant should conduct to studies that the applicant should conduct to further evaluate tenofovir associated bone further evaluate tenofovir associated bone abnormalities?abnormalities?

Summary of Regulatory Issues:Summary of Regulatory Issues:Clinical VirologyClinical Virology
• Prospective and Exploratory AnalysesProspective and Exploratory Analyses• Limitations of exploratory analyses Limitations of exploratory analyses
include:include:– Limited # of patients for some primary NRTI Limited # of patients for some primary NRTI
and multi-drug resistant mutations to and multi-drug resistant mutations to determine clinical significancedetermine clinical significance
– Large number of potential comparisons limit Large number of potential comparisons limit ability to conduct tests for statistical ability to conduct tests for statistical significancesignificance

• Please provide comments on the clinical resistance Please provide comments on the clinical resistance analyses conducted during the development of analyses conducted during the development of tenofovir. tenofovir.
• Please provide recommendations for the types of Please provide recommendations for the types of clinical virology analyses that should be conducted clinical virology analyses that should be conducted for future antiretroviral drug development and for future antiretroviral drug development and suggestions for type of resistance data/analyses suggestions for type of resistance data/analyses warranting display in package insertswarranting display in package inserts
Summary of Regulatory Issues:Summary of Regulatory Issues:Clinical VirologyClinical Virology

Summary of Regulatory Issues: Summary of Regulatory Issues: Accelerated Approval and Accelerated Approval and
Phase 4 CommitmentsPhase 4 Commitments
• Please provide comments on the Please provide comments on the proposed second study for traditional proposed second study for traditional approvalapproval
• Please provide comments for other study Please provide comments for other study designs or patient populations that should designs or patient populations that should be studied as phase 4 commitmentsbe studied as phase 4 commitments

Tenofovir Review TeamTenofovir Review Team• Clinical:Clinical: Kimberly Struble, Pharm.D., Jeff Murray, M.D., Kimberly Struble, Pharm.D., Jeff Murray, M.D.,
M.P.H., and Bruce Schneider, M.D.M.P.H., and Bruce Schneider, M.D.
• Stats:Stats: Rafia Bhore, Ph.D., and Greg Soon, Ph.D. Rafia Bhore, Ph.D., and Greg Soon, Ph.D.
• Micro: Micro: Nara Battula, Ph.D.Nara Battula, Ph.D.
• Clin Pharm:Clin Pharm: Jooran Kim, Pharm.D., and Kellie Jooran Kim, Pharm.D., and Kellie Reynolds, Pharm.D.Reynolds, Pharm.D.
• Pharm/toxPharm/tox: Pete Verma, Ph.D., and Jim Farrelly, Ph.D.: Pete Verma, Ph.D., and Jim Farrelly, Ph.D.
• Chemistry:Chemistry: Rao Kambhampati, Ph.D and Steve Miller, Rao Kambhampati, Ph.D and Steve Miller, Ph.D.Ph.D.
• Project Management:Project Management: Marsha Holloman, BS Pharm, J.D. Marsha Holloman, BS Pharm, J.D.



























![[Doravirina/ lamivudina / tenofovir disoproxil fumarato]](https://img.dokumen.tips/doc/110x75/628cd7cb477f9d51636f75dc/doravirina-lamivudina-tenofovir-disoproxil-fumarato.jpg)

