-
Tenecteplase in Central Retinal Artery Occlusion
Stephen James Ryan LIS Nevrologi
Stipendiat Oslo Universitetssykehus
-
Ischemic stroke is defined as an «episode of neurological
dysfunction caused by focal cerebral, spinal or retinal
infarction»
C.R.A.O. • Stroke emergency – Time is Brain • Ophthalmologic
emergency – Time Is Vision
• High risk of permanent blindness without prompt
revascularization
• No evidence-based treatment option
-
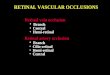
Ophthalmologic diagnosis Bedside findings • Visual acuity:
Counting fingers/light
perception • Afferent pupillary defect
Fundoscopic findings • Superficial opacification or
whitening
of the retina in the posterior pole • Cherry-red spot: a bright
red foveal
area • Box-carring of retinal arteries and veins • Retinal
arterial attenuation • Optic disc edema
-
4
Conclusions: This study showed that the administration of
intravenous alteplase within 4.5 hours of symptom onset is
associated with a higher likelihood of a favourable visual outcome
for acute central retinal artery occlusion.
-
• Design: A Prospective, randomized-controlled, double-dummy,
double-blind phase 3 multi-centre trial of TNK 0.25 mg/kg + placebo
vs. ASA + placebo (2 arms with 1:1 block randomization).
• Main objective: To assess the effect of IV TNK ≤ 4.5 h onset
of CRAO in a large multi-site trial.
• Primary endpoint: Proportion of patients with ≤ 0.7 logMAR
visual acuity 30 days after treatment, representing an improvement
in visual acuity of at least 0.3 logMAR
• Sample size: 78
TenCRAOS - Overview
-
6
-
7
-
Diagnostikk og behandling med studiemedisin
(injeksjon og kapsel) innen 4,5 timer
Overvåking og undersøkelser på
nevrologisk avdeling/slagenhet
1-3 dager
Kontroll hos øyelege og nevrolog etter
1 mnd
Kontroll hos øyelege og nevrolog etter
3 mnd
Where, What and When
-
Recruitment period:
October 2020
to January 2024
-
Inclusion criteria
• Non-arteritic central retinal artery occlusion with ≥ 1.0
logMAR visual acuitiy and symptoms lasting less than 4.5 hours.
• Ability to administer the Investigator Medicinal Product (IMP)
within 4.5 hours of symptom onset.
• Age ≥18 years. • Informed written consent of the patient. • A
woman of childbearing potential (WOCBP) must confirm that in
her
opinion, she cannot be pregnant, OR if there is a possibility
that she is pregnant, a negative pregnancy test must be confirmed
before any IMP is given.
10
-
Exclusion criteria • Other active intervention targeting
CRAO.
• Branch retinal artery occlusion, cilioretinal artery supplying
the macula, combined arterial-venous occlusion, proliferative
diabetic retinopathy, elevated intraocular pressure (> 30 mmHg)
or clinical suspicion of ophthalmic artery occlusion occlusion
(e.g. choroidal nonperfusion, absence of cherry red spot, no light
perception).
• Systemic diseases; severe general diseases, systemic arterial
hypertension (blood pressure >185/110 mmHg), despite medical
therapy, or clinical suspicion of acute systemic inflammation.
• Presence of intracranial haemorrhage on brain MRI/CT.
• Loooooong list!
11
-
Studiemedisin – Investigation Medicinal Product
-
Velkommen til TenCRAOS-møte!
Fredag 30. oktober kl 11.30-13 På Zoom og Rikshospitalet
Study Team Oslo: PI – Anne Hege Aamodt; CI – Stephen James Ryan;
SN – Christian Kefaloykos;
SN – Ansar Quadeer
-
Many thanks to TEN-CRAOS Collaborators!
14
Haukeland University Hospital V. Novotny, J Krohn, E. Rødahl
Stavanger University Hospital M Kurz
St. Olav University Hospital H Ellekjær, D Austeng
UNN SH Johnsen, S. Ingebrigtsen
Nordland Hospital Trust M Carlsson
Helse Nord Trøndelag Trust S Schüler
Nordmøre and Romsdal Regional Hospital ÅH Morsund
Sørlandet Hospital Trust R Solhoff
Vestfold Hospital Trust SB Krogseth
Østfold Hospital Trust B Ratajczak-Tretel
Innlandet Hospital Trust AH Farmen Vestre Viken Hospital Trust I
Nakstad, Telemark Hospital Trust H Tobro OUS Morten C. Moe, Ø
Jørstad, IC Olsen, KL Kraglund, D Atar, Brian Enriquez, Karolina
Skagen, EC Sandset, M Skjelland, E Berge, M. Beyer and colleagues
at Dep of Neurol/Ophthalmol.
Rigshospitalet UH Copenhagen TC Truelsen Aarhus University
Hospital, Coordinating center in Denmark T Bek, C Ziegler Aalborg
University Hospital S Due Karolinska University Hospital,
Coordinating center in Sweden M Mazya Helsinki University Hospital,
coordinating center in Finland D Strabian, Petra IIjas Turku UH P
Ylikotila, R Roine, J Ruuskanen, University Hospital Antwerp,
coordinating center in Belgium P Vanacker Mater Misericordiae
University Hospital, coordinating center in Ireland S Murphy
Vilnius University Hospital Santaros klinikos, coordinating centre
in Lithuania Jurgita Valaikienė, MD Portugal National coordinator,
Centro Hospitalar Universitário de,São João Ricardo Soares Reis
-
Takk for meg! Go raibh mile maith agaibh! Thank you for your
attention!