Embed Size (px)
Citation preview

TEMPLATE DESIGN © 2008
www.PosterPresentations.com
Uterus didelphys with right cervical hypoplasia and type-1 diabetic pregnancies alternating in both uterine cavities – an unusual caseUterus didelphys with right cervical hypoplasia and type-1 diabetic pregnancies alternating in both uterine cavities – an unusual case Dumitrascu I., Schaas C., Gonta O., Matasariu R., Onofriescu M., Tarnovanu M.C.
University of Medicina and Pharmacy “Gr.T.Popa” and University Women’s Hospital Cuza Voda Iasi, Romania
Introduction
Discussion and conclusions
Discussion and conclusions
References
1. Fedele L, Zamberletti D, D'Alberton A, Vercellini P, Candiani GB. Gestational aspects of uterus didelphys. ConJ Reprod Med. 1988 Apr;33(4):353-5.
2. Maneschi I, Maneschi F, Parlato M, Fucà G, Incandela S. Reproductive performance in women with uterusdidelphys. Acta Eur Fertil. 1989 May-Jun;20(3):121-4.
3. Ludmir J, Samuels P, Brooks S, Mennuti MT. Pregnancy outcome of patients with uncorrected uterine anomalies managed in a high-risk obstetric setting. Obstet Gynecol. 1990 Jun;75(6):906-10.
4. Simón C, Martinez L, Pardo F, Tortajada M, Pellicer A. Müllerian defects in women with normal reproductive outcome. Fertil Steril. 1991 Dec;56(6):1192-3.
5. Giannopoulos T, Croucher C. Successful consecutive pregnancies in separate horns of a uterus didelphys. J Obstet Gynaecol. 2004 Apr;24(3):314.
6. Acién P, Acién M, Sánchez-Ferrer ML. Müllerian anomalies "without a classification": from the didelphys-unicollis uterus to the bicervical uteruswith or without septate vagina. Fertil Steril. 2009 Jun;91(6):2369-75
7. Rana A, Gurung G, Manandhar B, Ghimire RK. Simultaneous occurrence of hematometrocolpos and consecutive pregnancies in uterine didelphys : a case report. Nepal Med Coll J. 2008 Jun;10(2):136-8.
8. Hua M, Odibo AO, Longman RE, Macones GA, Roehl KA, Cahill AG. Congenital uterine anomalies and adverse pregnancyoutcomes. Am J Obstet Gynecol. 2011 Dec;205(6):558.e1-5
9. Heinonen PK. Uterus didelphys: a report of 26 cases. Eur J Obstet Gynecol Reprod Biol. 1984 Jul;17(5):345-50.
10. Monks P. Uterus didelphys associated with unilateral cervical atresia and renal agenesis. Aust N Z J Obstet Gynaecol. 1979 Nov;19(4):245-6.
11. Altchek A, Paciuc J. Successful pregnancy following surgery in the obstructed uterus in a uterus didelphys with unilateral distal vaginal agenesis and ipsilateral renal agenesis: case report and literature review. J Pediatr Adolesc Gynecol. 2009 Oct;22(5):e159-62.
12. De Gennaro F. Habitual alternate pregnancy in undetected utersdidelphys. Minerva Ginecol. 1967 Mar 31;19(6):301-3.
13. Kohl MF. Abortion of decidual cast complicating pregnancy inuterus didelphys. Am J Obstet Gynecol. 1952 Mar;63(3):676-8.
14. Rana R, Pasrija S, Puri M. Herlyn-Werner-Wunderlich syndrome with pregnancy: a rare presentation. Congenit Anom (Kyoto). 2008 Sep;48(3):142-3.
Uterus didelphys represents a uterine malformation where the uterus is present as a paired organ as the embryogenetic fusion of the mullerian ducts failed to occur. As a result there is a double uterus with two separate cervices. Breech presentation, premature delivery and fetal death are more common in these patients, as are urinary tract malformations. Cesarean section is usually needed.
An unusual case of a type 1 diabetic patient with uterus didelphys, right cervical hypoplasia, single vagina, right renal agenesis and type 1 diabetes mellitus is presented. Since it has very similar features excepting that unilateral vaginal agenesis is replaced by unilateral cervical agenesis, we consider it a variant of Herlyn Werner-Wunderlich or OHVIRA syndrome
Since our patient was diagnosed during pregnancy, a histerosalpingography could not be performed, but ultrasonography and direct examination during laparotomy for C-section confirmed the diagnosis.Patients with a double uterus may need special attention during pregnancy as premature birth and malpresentation are common. The non-pregnant hemiuterus develops a decidual cast which can either eliminate spontaneously after delivery with important bleeding or can complicate with pyometra. To prevent these risks a curettage should be performed after delivery.
Case presentation
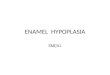
A 26-years old female patient was examined in our hospital for complaints of left pelvic pain associated with amenorroea for 6 weeks. She had menarche at the age of 14 and her menstrual cycles were painful with heavy flow. She was diagnosed with type 1 diabetes shortly after pubery at the age of 15 and she was prescribed subcutaneous insulin therapy. Her blood glucose and HbA1c were normal. General and abdominal physical examinations were normal. The vaginal speculum examination showed only one cervix slightly deviated to the left and a very small punctiform opening in the lateral right cul-de-sac, which was missed at previous examinations. She was referred to ultrasonography of abdomen and pelvis, which showed two separated uterine bodies, the left one anteverted, containing a 6 weeks normal single living pregnancy and continuing with a cervix, and a right one retroverted and without an intravaginal cervix. The first baby, in a cephalic presentation, was delivered prematurely at 30 weeks and 1850 grams by C-section. During the operation the two completely separated uterine bodies were seen, each having a normal tube and ovary on its side. The immediate postoperative recovery was uneventful, but after three weeks the patient returned with fever, abdominal pain and purulent fetid vaginal discharge. At the abdominal palpation a 20 cm right painful iliac fossa mass was found. Vaginal speculum examination revealed that the source for the purulent discharge was the punctiform opening of the right uterus from the right vaginal cul-de-sac. Vaginal and abdominal ultrasound showed a normal left uterine cavity and an enlarged fluid-filled right uterine cavity with 30 mm thickened endometrium, Vaginal cultures demonstrated an infection with E.coli for which intravenous therapy with Colimycine 50000UI/kg was started. The right uterine opening was dilated and 300 mL of pus were evacuated from the right hemiuterus. After 24 hours the patient’s body temperature returned to normal and a right D&C was performed under general anesthesia, extracting a very large amount of decidua.
After 16 months the patient returned with a second pregnancy in the right hemiuterus. Since she had no intravaginal cervix, she was proposed an abdominal cerclage which she refused. Surprisingly the pregnancy went on uneventfully until the age of 35 weeks, when a 3100 g baby in breech presentation was delivered by C-section. To prevent pyometra recurrence, this time we performed a D&C of the left hemiuterus immediately after the C-section, extracting the decidua. The postpartum period was complicated only by an low urinary infection. After 24 months the patient became pregnant again in the left uterus. The third pregnancy was complicated by premature contractions starting at 24 weeks, which required admission and continuous surveillance for 8 weeks, during which the patient received tocolytics and bed rest. At 32 weeks she was discharged from the hospital by request, and after 7 days, at 33 weeks of pregnancy, she had a precipitated VBAC of a 2300 g premature healthy baby. A D&C of the right uterine cavity were performed again, to prevent postpartum hemorrhage and pyometra.Definitive contraception by tubal ligation through umbilical minilaparotomy was performed 12 hours after delivery at patient’s request. One month after delivery she was admitted again for acute torsion of a right paratubal cyst which resolved spontaneously and did not require surgery.
OPTIONALLOGO HERE
OPTIONALLOGO HERE
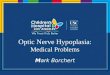
type 1 diabetes mellitus
right renal agenesis
Case presentation
It should not be assumed that cervical agenesis must be associated with cervical incompetence, since in our case the uterus was perfectly continent until 35 weeks of pregnancy and premature labor started probably rather due to the small uterine capacity. Interestingly, the pregnancies carried in the left uterus which had a cervix were delivered more prematurely than the pregnancy carried in the uterus with cervical agenesis.Associated type-1 diabetes is an extra challenge, since it predisposes to perinatal infections and big babies which accomodate poorly in a half-sized uterine cavity. A congenital solitary kidney associated with cervical hypoplasia on the same side could also add a problem in terms of renal function and pregnancy-induced hydronephrosis. Despite associations of uterus didelphys with infertility and recurrent abortions being cited as common, there are cases where conception is not a problem, and patients are able not only to conceive, but to carry their pregnancies until a reasonable pregnancy age.
2 pregnancies
1 CS 30 wk 1850 g
1 VBAC 33 wk 2300 g
1 pregnancy
1 CS 35 wk 3100 g