Embed Size (px)
Citation preview

Telegeriatrics: delivery of multiTelegeriatrics: delivery of multidisciplinary care to residents of disciplinary care to residents of
nursing homesnursing homes
1Dr. Elsie Hui
2Professor Magnus Hjelm2Professor Jean Woo
1Community Geriatric Assessment Team, Shatin Hospital and 2The Chinese University of Hong Kong
BackgroundBackground

Nursing Homes in Hong KongNursing Homes in Hong Kong
• 50,000 of Hong Kong’s 0.6 million elderly reside in nursing homes.
• Over half live in private, profit-making homes of variable standard of care.
• Nursing homes are not supported by general practitioners.
• Emergency Department attendance and hospital admissions are high.

CGATCGAT• Community Geriatric Assessment Team
(CGAT) serves nursing homes.
• Geriatrician, nurse, physiotherapist and occupational therapist.
• Provides multidisciplinary outreach services.
• In Shatin, CGAT supports 20 institutions, 2000+ clients.
• Limitations - infrequent visits, unable to respond rapidly to urgent problems.

Telemedicine in GeriatricsTelemedicine in Geriatrics
• Relatively few specialists looking after growing numbers of older patients.
• Elderly have difficulty accessing health care because of social isolation, poor mobility, low awareness, etc.
• Require multidisciplinary input and holistic approach, with sequential follow-up, preferably in their own homes.

ObjectivesObjectives
To explore whether Telemedicine is as effective as, or superior to, conventional outreach activities in providing a multidisciplinary service to elderly patients in nursing homes.

MethodsMethods

Telemedicine HardwareTelemedicine Hardware• Videophone system - Polycom® Viewst
ation 512K, 30 frames per second.
• 3 ISDN lines per station.
• Video camera, microphone, colour TV
• Optional - headphones, video recorder, computer, stethoscope




Equipment CostsEquipment Costs
One-off Total
Videophone $49 700ISDN installation $1 785
$51 485
Recurrent (monthly)
maintenance $417
ISDN charges Rental $1 080 Usage($0.09/min)
$13.50
$1 510.50

SubjectsSubjects
• 195-bed nursing home in Shatin• Current outreach services from CGAT:
routine and urgent medical assessment
multidisciplinary input - nursing, physiotherapy, occupational therapy
• Specialist clinics participating in study:
Dermatology
Psychogeriatrics
Podiatry

InterventionIntervention
• Telemedicine was used to replace all conventional outreach activities (CGAT) or outpatients visits (derm, psy, podiatry).
• A site visit would be made if telemedicine was considered inadequate for patient management or decision-making.
• The service was available during office hours, five days a week.

Activities assessedActivities assessedMedical• history taking• review of case notes/
drug charts• physical exam• nursing orders
Assessment of:• mobility• ADL• mental state• skin and wounds• swallowing test• catheter care• inhaler technique• home oxygen





Outcome measuresOutcome measures
1. Can telemedicine replace previous outreach or outpatient activities?
2. Can telemedicine increase productivity?
3. Is telemedicine cheaper than conventional services?
4. Does telemedicine reduce utilization of hospital-based health services?
5. How acceptable is telemedicine to users?

FindingsFindings

Table 1. Summary of activities and feasibility of Telemedicine
Discipline Patient-episodes % adequatewith telemed
Geriatrician 356 97.2
Psychogeriatrician 149 99.3
Dermatologist 74 74
Nurse 101 88.7
PT 105 87.1
OT 117 59.8
Podiatrist 99 84.9

• Telemedicine was adequate in the majority of cases and disciplines.
• Areas of limitation: Geriatrician - new cases, chest auscultation essential
Dermatologist - biopsy necessary
Nurse - complex procedures
Physio - chest PT
OT - measurement for equipment
Podiatrist - wound debridement

Telemedicine Increases ProductivityTelemedicine Increases Productivity
Geriatrician• Time savings - 2½ hours per telemedicine session
compared with 4 hours per outreach visit.• Increased productivity - number of patients increased
by 44.4% (from 45 to 65).
Occupational Therapist• Waiting time for new referrals shortened from 7 to 2
days.• 5 telemedicine sessions were held per month versus
only 3 visits per month before study.

Telemedicine is CheaperTelemedicine is CheaperTable 2. Cost comparison between Telemedicine and outreach service oroutpatients
Discipline Telemedicine Outreach OutpatientsGeriatrician $40.3 $153 $455
Psychogeriatrician $91.6 $105.9 $455
Dermatologist $117.9 N/A $455
Nurse $22.7 $67 N/A
PT $63.6 $330.4 N/A
OT $54.6 $290.8 N/A
Podiatrist $29.2 $160.8N/A = not applicable

Savings over Savings over One Year One Year (Geriatrician)(Geriatrician)
By replacing outreach geriatric clinics with telemedicine:
[($153 x 45) - ($40.3 x 65)] x 4
= $17062
By diverting 20 cases from outpatients to telemedicine:
$455 x 20 x 4 = $36400
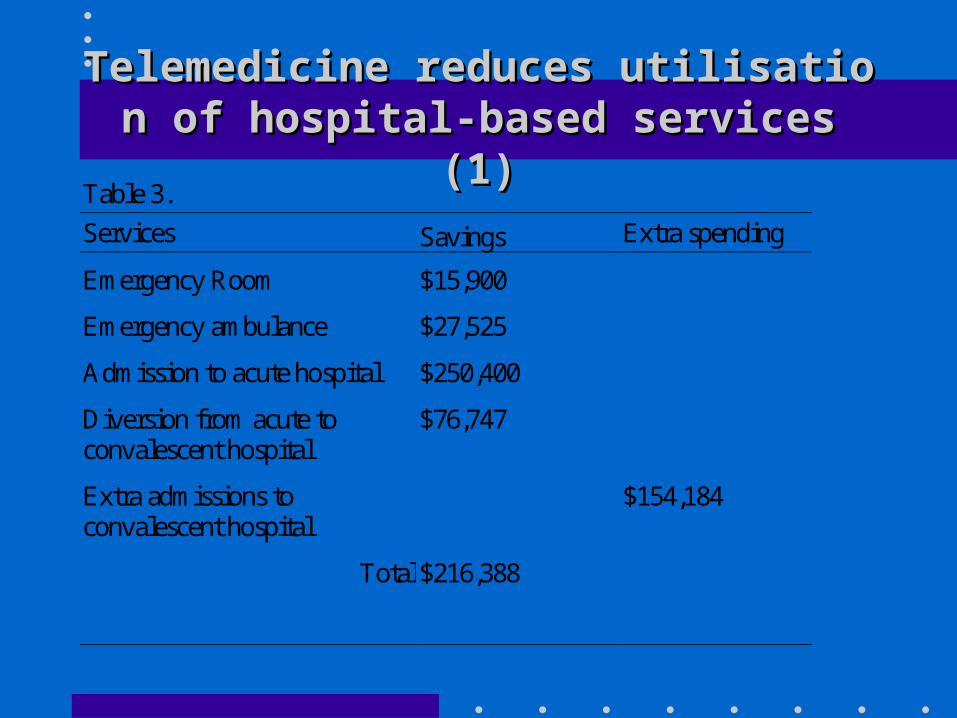
Telemedicine reduces utilisation of hospitaTelemedicine reduces utilisation of hospital-based services (1)l-based services (1)
Table 3.
Services Savings Extra spending
Emergency Room $15,900
Emergency ambulance $27,525
Admission to acute hospital $250,400
Diversion from acute toconvalescent hospital
$76,747
Extra admissions toconvalescent hospital
$154,184
Total $216,388

Telemedicine reduces utilisation of hospitaTelemedicine reduces utilisation of hospital-based services (2)l-based services (2)
Compared with same period pre-study:
• Emergency Room attendances decreased by 10% - Telemedicine was only available during office hours whereas 55% of emergency visits were out of hours.
• Acute hospital admissions decreased by 11%

Total Savings (Geriatrician)
• Provision of geriatrician’s services (medical follow-up, triaging of urgent cases) via telemedicine resulted in savings for the health authority amounting to $273,594 over one year.

User SatisfactionUser Satisfaction11
Patients (total 1001 episodes)
• 35% unable to answer (demented, communication difficulties).
• Depending on the discipline, 82% to 95% were satisfied with this mode of care delivery.

User SatisfactionUser Satisfaction22
Nursing Home Staff
• equipment easy to use
• increased accessibility to CGAT
• workload - 50% increased versus 50% decreased!

ConclusionsConclusions• Telemedicine is an acceptable
alternative to conventional geriatric services for nursing home residents.
• It results in significant cost and time savings, increases productivity and decreases utilization of emergency and inpatient services by providing timely intervention.
RemarksRemarks
• Quality can be improved by availability of a stethoscope device
• Cost effectiveness will be enhanced by extending the hours of service and supporting more homes.
• Costs will further reduce with rapid advances in information technology.