Embed Size (px)
Citation preview

TECHNICAL ADVICE DOCUMENT
DISASTER MEDICINE:
HOSPITAL PREPARATION ACTION PLAN
13 – TREATMENT – CASE MANAGEMENT (THESE ACTION PLANS WILL BE RELEASED AS SEQUENTIAL NUMBERED ACTION PLANS TO BE
USED BY HOSPITALS TO PREPARE FOR COVID-19)
The Actions Plans are presented as a free service to hospitals by the panel and by Right to Care
DR LESLEY BAMFORD CASE MANAGEMENT STREAM LEADER
CONSULTANCY PANEL CASE MANAGEMENT
Dr Lesley Bamford Case Management Stream Lead - IMT [email protected] Prof Lee Wallis Head Emergency Medicine - UCT [email protected] Prof Ian Sanne Infectious Disease Specialist [email protected] Dr Terrence Carter Hosp Management Consultant [email protected] Dr John Black Infectious Disease Specialist [email protected] Dr Vernon Wessels Disaster Medicine Expert: ER-24 [email protected] Dr Charl van Loggerenberg Disaster Medicine Expert Life Health [email protected]
DISASTER MEDICINE CONSULTANCY PANEL
Col (ret) Theo Ligthelm Disaster Medicine Consultant [email protected] Dr Wayne Smith Head Disaster Medicine WC [email protected] Col (ret) Willie Nieuwoudt Disaster Medicine Consultant [email protected] Me Mande Toubkin Disaster Medicine Expert Netcare [email protected] Col Franco Chamberlain Disaster Medicine Consultant [email protected] Dr Vernon Wessels Disaster Medicine Expert: ER-24 [email protected] Me René Grobler Disaster Medicine Expert Netcare [email protected] Dr Charl van Loggerenberg Disaster Medicine Expert Life Health [email protected]

2
1 CONTENTS
CONSULTANCY PANEL CASE MANAGEMENT .......................................................................................................... 1
DISASTER MEDICINE CONSULTANCY PANEL ........................................................................................................... 1
2 ACTION PLAN 13: CASE MANAGEMENT ......................................................................................................... 3
3 INTRODUCTION .............................................................................................................................................. 3
4 MILD DISEASE: PACKAGE OF CARE ................................................................................................................. 4
5 MODERATE DISEASE: PACKAGE OF CARE ....................................................................................................... 5
6 PALLIATIVE CARE: PACKAGE OF CARE............................................................................................................. 9
7 RESPIRATORY SUPPORT INCLUDING PRONING AND HIGH FLOW NASAL OXYGEN ........................................ 9
7.1 HFNO Device ....................................................................................................................................... 10
7.2 Advantages .......................................................................................................................................... 11
7.3 Concerns.............................................................................................................................................. 12
7.4 Indications ........................................................................................................................................... 12
7.5 Contraindications ................................................................................................................................ 13
7.6 Use ...................................................................................................................................................... 13
8 MEDICINE SUPPLY ......................................................................................................................................... 14
9 CONSUMABLES ............................................................................................................................................. 14
10 SUMMARY ............................................................................................................................................... 16
11 Links ......................................................................................................................................................... 17

3
2 ACTION PLAN 13: CASE MANAGEMENT
The following action plan is recommended for hospitals AT THIS STAGE by the Consultancy Panel while preparing
for the COVID-19 Pandemic.
This technical advice document must be read in conjunction with the National Health Plan for COVID-19
(National Dept of Health, 7 May 2020) and COVID-19 Health Care Surge Strategy (National Dept of Health, 30
April 2020).
DISASTER MEDICINE CSCATTT ALGORITHM1
C: Command and Control S: Safety C: Communication A: Assessments T: Triage T: Treatment Case Management
The various steps of this Algorithm will be addressed in the follow-up Action Plans.
3 INTRODUCTION
This Action Plan is focused on preparing the facility for providing clinical care to patients with COVID-19. It is
based on the Guideline: Clinical Management of Suspect or Confirmed COVID-19 (Currently Version 4) (National
Dept of Health and NICD, 18 May 2020).
This Action Plan does not cover triage of patients, as this is covered in Action Plan 10. All patients must be
streamed or divided into suspected/confirmed Covid-19 cases and non-Covid-19 cases at the entrance to the
hospital. Thereafter, all suspected suspected/confirmed Covid-19 cases should be triaged to receive one of the
four packages of care which are outlined in this action plan.
The four packages of care are:
• Mild disease
• Moderate disease
• Severe/critical disease
• Palliative care
It should be noted that these definitions are not fully aligned with those used by the World Health Organization
in their clinical guidelines. The simplified approach was chosen as it aligns more closely with the South African
1 (Advanced Life Support Group, 2019)

4
Clinical Guidelines as well as levels of care within the South African health system (home/low care bed, standard
hospital bed, critical care (ICU and high care) which have also been used in other components of planning.
The overview of all four care packages is shown in Annexure A, whilst each care package is discussed individually
in the following four sections. Hospitals primarily need to prepare to provide inpatient care to patients with
moderate and severe disease. Patients with mild disease may be seen and managed in outpatient departments.
Clinical management of patients with Covid-19 remains relatively straightforward, but is dependent on
availability of sufficient trained personnel and adequate supplies of:
• Infrastructure, beds and equipment
• Oxygen and other respiratory support
• Medicines
• Consumables
• Personal Protective Equipment (PPE)
This action plan includes some information on oxygen and other respiratory support, medicines and
consumables.
Provision of oxygen and other respiratory support remains the cornerstone of clinical care for patients with
Covid-19. Whilst a standard approach to provision of increasing concentration and flow rate of oxygen remains
relevant in Covid-19 disease, provision of non-invasive ventilation appears to be more beneficial than previously
thought. For this reason, information on provision of High Flow Nasal oxygen is described in some detail. The
section on Oxygen and Respiratory Support should be read in conjunction with Action Plan 11 which includes
information on delivery of oxygen.
Hospitals must also plan for the increased quantities of medicines and consumables that are likely to be required
in increased volumes during the Covid-19 surge.
4 MILD DISEASE: PACKAGE OF CARE
The majority of symptomatic Covid-19 patients will present with mild disease. The criteria for mild disease are
shown in Error! Not a valid bookmark self-reference. and are:
• SpO2 ≥95% on room air
• Respiratory rate <25
• Heart rate <120
• Temp 36-39°C
• Mental status normal

5
Table 1: Package of care for mild disease
Level of care Clinical Criteria Package of care Criteria: transfer to higher level of care
Criteria: down referral
Mild
dis
eas
e
Basic nursing
care
- Self-
isolation at
home
- Isolation
facility (low
level care)
SpO2 ≥95% on
room air
Respiratory
rate <25
Heart rate
<120
Temp 36-39°C
Mental status
normal
Optimise treatment
for co-morbid
conditions
Screen/test for TB
and HIV (if status
unknown)
Basic IPC measures
Bed-rest, if needed
Symptomatic relief
of fever/pain
Intake of sufficient
fluids
Access to HCW
advice (telephonic or
face-to-face)
Presence of danger
signs:
- Shortness of
breath
- Persistent chest
pain
- Coughing up
blood
- Confusion/severe
sleepiness
- Blue lips
Meets clinical
criteria for moderate
or severe disease.
De-isolate: 10
days after onset
of symptoms
KEY RESOURCES
Clinical management of suspected or confirmed COVID-19 disease V4
COVID-19 Disease: Infection Prevention and Control Guidelines V2
Adult Primary Care: COVID-19: Guidance for Professional Health Workers in PHC Facilities
Advice on self-isolation at home
Patients with mild disease do not require in-patient (hospital) care; they require basic nursing care (also termed low level care in the Surge plan document). However, they must be isolated from others – this can be achieved through self-isolation at home, or, where necessary, through admission to an isolation facility. Patients who are self-isolating should monitor their symptoms are on a daily basis and be able to access medical care if their condition deteriorates. It may necessary to admit patients with mild disease who do not meet these criteria, especially where they are at high risk for developing severe disease. Attention should be paid to ensuring that any co-morbid conditions (especially diabetes and hypertension) are optimally controlled, and that patients have access to an adequate supply of medication. Patients with Covid-19 may not be regular users of health services and their interaction with the health service should also be used as an opportunity to screen for other conditions especially HIV and TB.
5 MODERATE DISEASE: PACKAGE OF CARE
The main characteristic of patients with moderate disease, is their requirement to receive oxygen. All levels of
hospitals are therefore required to ensure that they have sufficient beds each with a reliable supply of oxygen.
Whilst it is recommended that patients with moderate disease are admitted to established/permanent
hospitals, they can also be cared for in field hospitals, providing a reliable supply of oxygen is available.

6
Table 2: Moderate disease: Package of care
Level of care Clinical
Criteria
Package of care Referral Criteria
To higher
level of care
Down referral
Mo
de
rate
dis
eas
e
Standard care/
general beds in all
levels of hospital
(must have oxygen)
Requires
oxygen to
maintain
SpO2 ≥92%
Respiratory
rate >25
Oxygen administration via
face-mask
Specific therapy (currently
dexamethasone, others
only as part of clinical trials)
Antibiotic therapy if co-
infection
suspected/confirmed
Supportive care including
anti-thrombolytic
prophylaxis, fluid
management, relief of
pain/other symptoms, etc.
Physiotherapy
Monitoring including pulse
oximetry
IPC measures
Meets clinical
criteria for
severe
disease
AND
Meets
criteria for
critical care
admission
Discharge home or transfer to low care bed once oxygen no longer required. (De-isolate: 10 days after stable off oxygen)
If critically ill and does not meet criteria for critical care admission, consider transfer to palliative care bed
KEY RESOURCES Clinical management of suspected or confirmed COVID-19 disease V4 COVID-19 Disease: Infection Prevention and Control Guidelines V2 Adult Essential Medicine List Standard Treatment Guidelines.
Medical treatment
In addition to oxygen, all hospitalised patients should receive a ten-day course of Dexamethasone (6mg IV daily
for 10 days) or equivalent corticosteroid. All hospitalised patients should also receive low-molecular weight
heparin. Admitted patients should receive prophylactic doses (e.g. enoxaparin 40mg subcutaneously daily).
Morbidly obese and patients with renal failure may require dose adjustments (consult Adult Hospital EML
Standard Treatment Guidelines). However, patients who require mechanical ventilation or supplemental
oxygen at ≥ 60% oxygen concentration as well patients with serum D-dimers greater than 6-times the upper
limit of normal should receive therapeutic doses of LMW heparin (e.g. enoxaparin 1mg/kg subcutaneously 12-
hourly).
Antibiotic therapy is not routinely recommended but should be provided if secondary bacterial infection is
suspected. Antibiotic therapy should be provided in line with the Essential Medicine List (EML) Standard
Treatment Guidelines.
Attention should be paid to control of hypertension, diabetes, asthma and other underlying conditions. The
acute illness as well as administration of dexamethasone may exacerbate hyperglycaemia in diabetic patients
requiring careful monitoring and appropriate treatment (see EML STG).

7
Monitoring
Monitoring of oxygenation using pulse oximetry is critical. Laboratory tests may be needed to exclude other
causes of pneumonia and to monitor for complications.
Referral
Most patients with moderate disease will be cared for in district hospitals. However, a proportion of patients
will deteriorate. Timely identification and referral of patients who are likely (and eligible) to require critical care
is desirable, especially as transport of critically ill patients is associated with poor outcomes.
Radiological findings have been found to be a predictor of a poor outcome, but have not been validated in South
Africa. Where referral is difficult, provision of HFNO outside of critical care settings (including in district hospitals)
should be considered.
Earlier referrals to higher levels of care may be considered in resource poor
or remote settings where difficulties in oxygenation occur or delays in
referral are anticipated.

8
SEVERE DISEASE: PACKAGE OF CARE
Patients who develop severe acute respiratory syndrome or hypoxaemic respiratory failure should ideally be
admitted to a critical care bed in a high care or intensive care unit. Most patients will require ventilation either
mechanical or non-mechanical. As noted above, HFNO appears to play a role in reducing the need for mechanical
ventilation.
Table 3: Severe disease: package of care
Level of care Clinical
Criteria Package of care
Referral Criteria
To higher
level of care Down referral
Seve
re/C
riti
cal D
ise
ase
Critical care bed
Ideally in a standard
ICU or temporary
ICU within a
structured
supported
environment where
the supporting
services for
intensive care are
already established.
HFNO and CPAP
may be provided in
general bed if
resources (staff, O2,
monitoring) allow
Signs of SARS /
severe
hypoxaemic
respiratory
failure:
Respiratory
rate > 40
SpO2 less than
90% or an
arterial blood
sample with
PaO2 < 8.0 kPa
(while using a
40% facemask)
Heart rate >
120 beats per
minute
High-flow nasal oxygen
(HFNO), continuous
positive airway pressure
(CPAP) or other non-
invasive ventilation
Mechanical ventilation (if
indicated)
Specific therapy
(currently
dexamethasone, others
only as part of clinical
trials)
Intensive care monitoring
Supportive care including
anti-thrombolytic
prophylaxis, fluid
management, relief of
pain/other symptoms,
specialised nutrition
support
Management of
complications including
co-infection, thrombosis,
etc
Monitoring: radiology, lab
Physiotherapy
IPC measures
Not applicable Transfer to standard care bed once extubated/stable
Consider withdrawal of care and transfer to palliative care bed if condition deteriorates/poor response to critical care.
KEY RESOURCES
Clinical management of suspected or confirmed COVID-19 disease V4
COVID-19 Disease: Infection Prevention and Control Guidelines V2
Detailed management of patients in critical care is beyond the scope of this action plan. However, the principles
remain the same, with care being primarily supportive in nature. Particular attention should be paid to fluid
management, relief of pain and anxiety, physiotherapy and specialised nutritional support.

9
6 PALLIATIVE CARE: PACKAGE OF CARE
A number of groups of patients will require palliative care including palliative care patients who are diagnosed
with Covid-19, patients who are not eligible for ventilation and patients where ventilation is withdrawn due to
a lack of response. The palliative care package should focus on management of symptoms, end-of-life care and
management of death and bereavement.
Level of care Clinical Criteria Package of care
Referral Criteria
To higher level of care
Down referral
Pal
liati
ve C
are
Palliative care
bed
(but package
should be
provided
wherever
necessary).
Palliative Care
patients who are
diagnosed with
COVID-19
Patients where
ventilation is
withdrawn due to
no response
Patients who are
not eligible for
ventilation
Withdrawal of
ventilation/other
interventions
Hospital-based care for
patients with severe
symptoms who are not
candidates for critical
care admission
Management of
symptoms (dyspnoea,
anxiety, pain, etc)
End-of-life care
Management of the
deceased
Not applicable Transfer home or
to bed in
institution with
low level care
KEY RESOURCES
Clinical management of suspected or confirmed COVID-19 disease V4
COVID-19 Disease: Infection Prevention and Control Guidelines V2
Providing Palliative Care in South Africa during the COVID-19 Pandemic (The Association of Palliative Care
Practitioners of South Africa).
7 RESPIRATORY SUPPORT INCLUDING PRONING AND HIGH FLOW NASAL OXYGEN
Oxygen remains the main supportive treatment for COVID-19. It is therefore essential that facilities plan for the
administration of oxygen and respiratory support to nearly all moderate, severe and critical COVID-19 patients.
The National Incident Management Team for COVID-19 has recommended that ONLY PATIENTS REQUIRING
OXYGEN should be admitted to general hospital beds and that mild patients not in need of oxygen (at the
time) could be admitted to temporary facilities or surge facilities at hospitals, that are not equipped for
oxygen administration.
• Mask administration. Most patients will initially require administration of 40% oxygen with a mask.
(Certain comorbidities may indicate lower percentage oxygen administration.) Facilities must therefore
plan for an adequate stock of 40% oxygen masks. Although it is expected that most of the patients will
be adults, current figures indicate that paediatric masks will also be necessary.
• Patients unfortunately desaturate very quickly requiring non-rebreather mask oxygenation. It is
therefore essential that all hospitals plan for non-rebreather masks with a reservoir bag.

10
• There are limited use for nebulised drugs. Precautions is necessary in administering nebulisation due
to the theoretical possibility that the vapour may carry exhaled droplets, especially when patients
cough. A N-95 mask and visor is recommended for staff supporting a patient during nebulisation. Ensure
effective decontamination of nebulisers if it must be moved between Covid and non-Covid areas (not
recommended at all).
• Some experiments were done with nasal prongs at 15 l and a non-rebreather mask over the prongs also
at 15 l from a second flowmeter. This technique dries the nasal mucosa. However, it is recommended
that hospitals plan for this double flowmeter technique for an emergency.
• Continuous Positive Airway Pressure (CPAP) and Bilevel Positive Airway Pressure (BiPAP). Mask or
helmet administered CPAP or BiPAP is a simple technique that can be used in many facilities to manage
COVID-19 on condition that the necessary supervision and observation is available. Hospitals should
plan to have this capability available2.
• High Flow Nasal Oxygen (HFNO) is a technique where a high flowrate of humidified warmed oxygen is
administered via a nasal canula. These apparatuses require electricity at the bed side and can use an
oxygen flow of up to 60 l/min. The flowrate is not generally available at ward-level oxygen outlets. This
technique has shown high success rates in Europe and in the Western Cape – hospitals are therefore
urged to plan for spaces in the hospital where this type of apparatus can be utilised with the required
oxygen flow. Although in general HFNO would generally be provided in a critical care setting, it may be
provided in a standard care setting providing adequate staff, PPE and monitoring are available.
It is essential to take note that the use of several high flow nasal oxygen units and possibly CPAP
units in the same venue may lead to a build-up of the ambient oxygen concentration in the room
due to wasting during exhalation, causing an increased fire risk.
The use of a natural well-ventilated venue (open windows) is strongly recommended.
Ensure that fire extinguishers in the areas are serviced and staff trained to use it.
Staff must also be orientated where to turn off oxygen supply to an area in the event of a fire.
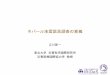
7.1 HFNO DEVICE
High-flow nasal cannula (HFNC) oxygen therapy is a technique configured to deliver adequately heated and
humidified medical gas at a high flow rate. The device consists of a flow generator (providing gas flow rates up
to 60Lmin), an air-oxygen blender (that reliably achieves escalation of FiO2 from 0.21-1.0 at user selected flow
rates), and a humidifier that humidifies the gas mixture at temperatures of between 31-37°C (adjusted to patient
comfort). To minimize condensation, the heated humidified gas is delivered via heated tubing through nasal
prongs or cannula. The device is demonstrated in Figure 1.
2 A national project is underway to supply high numbers of these apparatuses to hospitals.

11
From: REF[1] Nishimura M.
7.2 ADVANTAGES
HFNC is considered to have a number of physiological effects including:
• low levels of positive end-expiratory pressure (PEEP), at best up to 10 cm H20, that may assist in
increasing lung volume and recruitment of alveoli;3,4
• reduction of anatomical dead space as the high flow washes out CO2;5
• maintenance of a constant FiO2 as the difference between inspiratory flow and delivered flow is small;6
• adequate humidification contributing to good muco-ciliary function and patient comfort;7 and
• decreased work of breathing.8
Other general advantages in COVID-19 patients include that it:
• may be implemented and managed by non-ICU specialists outside ICU;
• does not require invasive monitoring;
• does not need as intensive nursing care as for invasive ventilation;
• can be combined with awake self-proning;
3 Parke R, McGunness S, Eccleston M. Nasal high-flow therapy delivers low level positive airway pressure. Br J Anaesth. 2009;103:886–90. 4 Corley A, Caruana LR, Barnett AG, et al. Oxygen delivery through high-flow nasal cannulae increase end-expiratory lung volume and reduce respiratory rate in post-cardiac surgical patients. Br J Anaesth. 2011;107(6):998–1004. 5 Frizzola M, Miller TL, Rodriguez ME, et al. High-flow nasal cannula: impact on oxygenation and ventilation in an acute lung model. Pediatr Pulmonol. 2011;46:67–74 6 Ritchie JE, Williams AB, Gerard C, et al. Evaluation of a humidified nasal high-flow oxygen system, using oxygraphy, capnography and measurement of upper airway pressures. Anaesth Intensive Care. 2011;39:1103–10. 7 Oto J, Nakataki E, Okuda N, et al. Hygrometric properties of inspired gas and oral dryness in patients with acute respiratory failure during noninvasive ventilation. Respir Care. 2014;59(1):39–45. 8 Pham TM, O'Malley L, Mayfield S, et al. The effect of high flow nasal cannula therapy on the work of breathing in infants with bronchiolitis. Pediatr Pulmonol 2015;50(7):713–720.

12
• may be a lower-resource alternative to mechanical ventilation in some patients;
• Is relatively well tolerated and not too cumbersome allowing patient self-care or assisted care while
applying the therapy, including daily functions such as eating.
7.3 CONCERNS
The two main concerns relate to the risk of aerosolization and the adequacy of oxygen supplies. All respiratory
therapy has the potential to create aerosols. A caution with HFNC initially arose because of a concern for possible
generation of droplets and aerosols created or propelled by oxygen therapy via this delivery system with a
consequent increased risk of disease transmission. Subsequent research has indicated that this risk is extremely
low. Dispersion studies have shown that, compared to oxygen therapy with a mask or standard nasal cannulae
at 5 L/min, the utilization of HFNC is no riskier with respect to either dispersion or microbiological contamination
into the environment.9,10 The risk may be further mitigated by the additional application of, for example, a
surgical mask to the patient.
As high flows (up to 60L/min) are used with HFNC systems, a concern rose on the adequacy of hospital oxygen
supplies if the therapy was applied to a large number of patients within the same facility. The high flow of oxygen
exceeds the requirements for routine general ward beds (4-15L/min), and for ICU or ventilated patients
(30L/min).11 This concern relates to storage and delivery of oxygen, and questions the ability of banks or storage
tanks for liquid oxygen to cope with demand in maintaining a constant flow and pressure to reticulation and
supply points. Medical engineering consultation is required about oxygen supply at individual hospitals including
number of HFNC units that can be supported.
7.4 INDICATIONS
For patients who are deteriorating or not improving on conventional oxygen therapy and supportive care, but
who do not appear to be in imminent danger of collapse, HFNC oxygen therapy likely offers benefit. Consider
HFNC in awake, co-operative patient if SpO2 <92% despite O2 15L/min.
Initiation of HFNC does not by default imply that a patient’s care will be escalated to invasive ventilation. Certain
patient groups will be reasonably triaged to receive HFNC as their last escalated oxygen therapy intervention.
These decisions should be made in accordance with local facility triage team protocols as well as national
guidelines (e.g. the CCSSA triage guidelines).
9 Hui DS, Chow BK, Lo T, et al. Exhaled air dispersion during high-flow nasal cannula therapy versus CPAP via different
masks. Eur Respir J. 2019;53(4). Epub 2019/02/02. doi: 10.1183/13993003.02339-2018. PubMed PMID: 30705129. 10 Li J, Fink JB, Ehrmann S. High-flow nasal cannula for COVID-19 patients: low risk of bio-aerosol dispersion. Eur Respir J. 2020;55(5). Epub 2020/04/18. doi: 10.1183/13993003.00892-2020. PubMed PMID: 32299867; PMCID: PMC7163690 11 Oxygen sources and distribution for COVID-19 treatment centres Interim Guidance. Geneva: World Health Organization;
2020 (https://apps.who.int/iris/bitstream/handle/10665/331746/WHO-2019-nCoV-Oxygen_sources-2020.1-
eng.pdf?sequence=1&isAllowed=y, accessed 18 June 2020).

13
7.5 CONTRAINDICATIONS
• Patients with hypercapnia (exacerbation of obstructive lung disease), haemodynamic instability, multiorgan
failure or abnormal mental status should generally not receive HFNC oxygen therapy in place of other
options such as invasive ventilation.
• Adults with emergency signs (obstructed or absent breathing, severe respiratory distress, central cyanosis,
shock, coma and/or convulsions) should receive emergency airway management and O2 therapy during
resuscitation to target SpO2 ≥ 94% .12
7.6 USE13
• Discuss early with ICU team to ascertain ceilings of treatment at presentation in order to avoid inappropriate
escalation of ventilatory support.
• Ideally HFNC O2 therapy should be applied in single negative pressure rooms. If unavailable, then cohorting
of patients requiring HFNC in designated wards is an alternative.
• Appropriate administrative controls need to be in place
• Ensure adequate environmental ventilation of at least 12 air changes per hour, equivalent to a room with
door and windows open or suitable extraction or air conditioner to achieve same, or with HEPA (high
efficiency particulate air) filtration if recirculated air.
• Personal protective equipment (PPE), including N95/ FFP2 respirators, to be worn by the staff to reduce
nosocomial infections.
• Ensure proper size and fit of nasal cannula. Most interfaces come with a lanyard and two clips to secure
the piping to the hospital gown or pillow. If not, tape to the cheeks so prongs do not leave the nostrils.
• A surgical face mask should be placed on the patient at all times to reduce bioaerosolisation.
• Effective HFNC may rely on patient being able to keep their mouth closed and maintain nasal breathing to
ensure best performance of the device as mouth opening decreases the PEEP effect. Patient training may
be important in achieving the best result.
• Patients should be monitored with continuous pulse oximetry to enable monitoring of response and for
early identification of rapid deterioration.
• Initial settings: Flow 50-60L/min and FiO2 0.8-1.0, titrated to aim initially for SpO2 >90% are recommended.
• Where hospital oxygen supply is constrained, consider using minimum O2 flow necessary to maintain SpO2.
Titrate FiO2 to maximum support prior to increasing flow greater than 35L/min.
• Patients receiving a trial of HFNC should be in a monitored setting and cared for by personnel experienced
with HFNC and capable of performing endotracheal intubation in case the patient acutely deteriorates or
does not improve after a short trial (about 1 hour).
• Once HFNC has been initiated, need to assess the patient regularly to determine if the patient needs to be
intubated.
• There should be a low threshold for intubation where there is clinical decline (which may include a rising O2
requirement, consistently or rapid increase in respiratory rate, consistently or rapidly declining SpO2,
increased work of breathing/exhaustion, and altered mental state).
Intubation should not be delayed if the patient acutely deteriorates or does not improve after a short trial.
12 WHO-ICRC Basic Emergency Care: approach to the acutely ill and injured. Geneva: World Health Organization; 2018 (https://www.who.int/publications-detail/basic-emergency-care-approach-to-the-acutely-ill-and-injured, accessed 14 May 2020). 13 World Health Organization. Clinical management of COVID-19. Interim guidance. 27 May 2020. WHO/2019-nCoV/clinical/2020.5

14
8 MEDICINE SUPPLY
The following medicines are likely to be required in higher than usual volumes during the Covid-19 surge, and it
is important that hospitals ensure that they have adequate supplies. More detailed lists have been shared with
provincial pharmaceutical service managers.
Table 4: List of medicines which will be required in higher than usual volumes
Medicines Reason
Dexamethasone or equivalent corticosteroid
Treatment of Covid-19 patients requiring oxygen
Heparin All admitted patients (patients requiring more than 60% oxygen should receive therapeutic doses, whilst other patients should receive prophylactic doses)
Antibiotics Secondary bacterial infections. Patients who develop signs of infection more than 48 hours after admission should be assumed to have a Hospital Acquired Infection and should receive appropriate antibiotics (see Adult Hospital EML STG).
Insulin and oral hypoglycaemics
Diabetics are at risk of developing severe disease and are more likely to require admission. Glycaemic control is likely to be compromised resulting increased insulin requirements
Salbutamol inhalers Used instead of nebulisation (danger of aerosolisation)
Paracetomal Tramadol Morphine
Pain relief
Benzodiazepines Propofol
Sedation
Muscle relaxants Atropine Neostigmine
Use during intubation and ventilation
Inotropes and pressors Hypotension
9 CONSUMABLES
The following consumables are likely to be required in higher than usual volumes, and hospitals should ensure
that adequate supplies are available.
Table 5: List of medicines which will be required in higher than usual volumes
Medical Purpose Name
Airway Adjunct Dressing, ET tube
Dressing, ET tube
Airway Management
Catheter Mount
Colorimetric CO2 detector, adult
Cricothyrotomy kit
Endotracheal tube introducer, Bougie
Endotracheal tube introducer, Stylet
Endotracheal tube oral/nasal cuffed
Laryngeal Mask Airway
Nasopharyngeal Airway
Oropharyngeal airway, Guedel

15
Tracheostomy tube fenestrated cuffless
Tracheostomy tube, cuffed
Dressings
Bandage, crepe
Cotton wool balls
Dressing pack
Dressing, IV catheter placement
Gauze
Emergency thoracic Closed chest drain system eg Sinapi chest drain system
Intercostal chest tubes
Gasto-Enteral Feeding Nasogastric tubes
General Medical Supplies
Defibrillator pads
Drapes
Gauze
Linen savers
IVI and central access plus giving sets
Central Venous Catheter Kit
Central Venous Catheter Kit
Extension sets
Extension sets
Extension sets
Intravenous administration set
Intravenous administration set
Intravenous administration set
Intravenous cannula
Short lines
Mechanical Ventilation
Breathing Circuit, Airvo™2
Breathing Circuit, ICU
Breathing Circuit, Theatre
Circuits for HFNO
Connector and oxgen delivery accessories
Filters
Resuscitation bags
Monitoring Pulse Oximeter
Needles and Syringes
Hypodermic Needles
Syringe, feeding
Syringe, feeding
Syringe, feeding
Syringe, insulin
Syringe, three-part, luer lock
Oxygen Therapy
Hood, CPAP
Mask, CPAP
Mask, Venturi
Masks, Anaesthetic
Masks, non-rebreathing
Nasal cannula
Nebuliser set
Nebuliser, Aerogen Solo
PEEP valves
Suction Closed suction catheters

16
Inline suction device
Suction catheter, flexible
Suction catheter, Yankauer, regular tip with control
Tubing, silicone (suction)
Suture Material Sutures
Urine Collection Urinary catheters, Foleys
Urine bag
10 SUMMARY
Treatment facilities required for COVID-19 can be summarised as standard medical pneumonia care facilities.
However, a few areas requiring special attention are:
• Proning patients
• Oxygen needs
• Palliative care needs
• Psycho-social support needs
This action plan will be followed by a sequentially
numbered Action Plan continuing the preparation

17
11 LINKS
WHO Clinical management of
COVID-19
https://www.who.int/publications/i/item/clinical-management-of-covid-19
Clinical Treatment Guidelines (Version 4)
https://www.nicd.ac.za/wp-content/uploads/2020/05/Clinical-
management-of-suspected-or-confirmed-COVID-19-Version-4.pdf
Hospital Readiness Checklist
https://docs.google.com/forms/d/e/1FAIpQLSeeRsgKVfPtSILkVMSfYyqkGjPAnjKbtaxuW4nt1hN
UvgmT6w/viewform?fbzx=-390608713341965087

Level of care Clinical Criteria Package of care Criteria: transfer to higher
level of care Criteria: down
referral M
ild d
ise
ase
Basic nursing care - Self-isolation at home - Isolation facility (low level
care)
SpO2 ≥ 95% on room air
Respiratory rate < 25 Heart rate < 120 Temp 36-39°C Mental status normal
Optimise treatment for co-morbid conditions Screen/test for TB and HIV (if status unknown) Basic Infection Prevention and Control (IPC) measures including isolation Bed-rest Symptomatic relief of fever/pain Intake of sufficient fluids Access to HCW advice (telephonic or face-to-face)
Presence of danger signs: - Shortness of breath - Persistent chest pain - Coughing up blood - Confusion/severe
sleepiness - Blue lips Meets clinical criteria for moderate or severe disease.
De-isolate: 10 days after onset of symptoms
Mo
de
rate
dis
eas
e
Standard care bed in hospital (must have oxygen)
Requires Oxygen to maintain SpO
2 ≥ 92%
Respiratory rate > 25
Oxygen administration via face-mask Specific therapy; - Dexamethasone - Others as part of clinical trials Antibiotic therapy if co-infection suspected/confirmed Supportive care including anti-coagulation (with LMW heparin), fluid management, relief of pain/other symptoms, etc. Physiotherapy Monitoring including pulse oximetry Infection control and prevention measures
Meets clinical criteria for severe disease AND Meets criteria for critical care admission
Discharge home or transfer to low care bed once oxygen no longer required. (De-isolate: 10 days after stable off oxygen)
If critically ill and does not meet criteria for critical care admission, consider transfer to palliative care bed
Seve
re d
ise
ase
Critical care bed Ideally provided in a structured supported environment where supporting services for critical care are already established. Where resources allow, HFNO and CPAP should be provided in a general bed.
Signs of SARS / severe hypoxaemic respiratory failure: - Respiratory rate > 40 - SpO2 less than 90% or an
arterial blood sample with PaO2 < 8.0 kPa (while using a 40% facemask)
- Heart rate > 120 beats per minute
High-flow nasal oxygen (HFNO), continuous positive airway pressure (CPAP) or other non-invasive ventilation Mechanical ventilation (if indicated) Specific therapy; - Dexamethasone - Others as part of clinical trials Management of complications including co-infection, thrombosis, etc. Intensive care monitoring Supportive care including anti-coagulation (with LMW heparin), fluid management, relief of pain/other symptoms, specialised nutrition support Physiotherapy Infection control and prevention measures
Transfer to standard care bed once extubated/stable for ongoing care and rehabilitation
Consider withdrawal of care and transfer to palliative care bed if condition deteriorates/poor response to critical care.

19
Level of care Clinical Criteria Package of care Criteria: transfer to higher
level of care Criteria: down
referral
Pal
liati
ve C
are
Palliative care bed (but package should be provided wherever necessary).
Palliative Care patients who are diagnosed with COVID-19 Patients where ventilation is withdrawn due to no response Patients who are not eligible for ventilation
Withdrawal of ventilation/other interventions Hospital-based care for patients with severe symptoms who are not candidates for critical care admission Management of symptoms (dyspnea, anxiety, pain, etc.) End-of-life care Management of the deceased
Transfer home or to palliative care bed in institution with low level care

COVID-19 HOSPITAL PREPARATION
CHECK-LIST FOR PREPARATION THIS FAR Ser No
Action Date Completed
1. Training completed in triage Sieve and Sort for all screening and receiving personnel and posters are printed and available for use.
2. Triage tags are available and supports the Triage process
3. Posters for doffing and donning PPE from the NDOH Guidelines are printed and available
4. Screening, testing and triage facility was planned, and equipment is available
5. Surge capacity of the facility is calculated and recorded indicating:
• Additional space for ICU/ventilation capabilities
• Additional patient care space for high dependency care
• Additional patient care space for low dependency care
6. Bed repairs / additional sources to provide beds to surge capacity in in place
7. All available ventilators were identified and process to service the unserviceable ventilators is in place / consider off label use of anaesthetic machines if resources available
8. Oxygen cylinders and regulators are checked and serviced
9. Supply line for oxygen cylinders refills were reviewed and checked, supplier can shorten turn-around time if required
10. The Red Area that will be used for patient care was identified and include all the levels of care available at the hospital
11. The Red Area is separated from the rest of the hospital by a Yellow Transit Area. The Yellow Area has adequate facilities to decontaminate staff and equipment coming out of Red Area.
12. Plan is in place to move COVID-19 patients from Red Area to and from x-ray department
13. The Green Support Area has been identified
14. All areas are demarcated, and signage is available to be placed when required.
15. The PPE guidelines from the National Department of Health was evaluated and all needs determined.
16. PPE stock is ready and sufficient for at least seven (7) days
17. Temporary ventilation capability is planned for movement of patients if required and oxygen is available for transfers.
18. Planned beds can accommodate Fowlers position and oxygen administration.
19. Palliative Care is considered, facilities and staff were planned
20. Hospital Command is planned, and members of command identified
21. Command Centre is prepared
22. Communication capabilities are available for Command centre
23. Daily bed statistic monitoring is in place
24. Patients that
• Can be discharged
• Can be transferred to a lower level of care
• Need to stay at current level of care
• Require for transferring to a higher level of care Are identified on a daily basis.
25. Safety officers are identified to supervise and control use of PPE
26. Every area is informed of PPE requirements in that area and posters for requirement, donning and doffing is displayed

21
Ser No
Action Date Completed
27. Access control is in place: channelling all patients through screening facility
28. Red Isolation Area is locked-down with strict access control
29. Planning is in place for:
• Patient control in isolation area
• Visitor control
• Separated minors
• Specimen security
• Body security
• Traffic and transport control
30. Decontamination is planned and decontamination solutions identified
31. Measurements and mixing instructions for decontamination are issued and solutions are replaced daily (where applicable)
32. Containers and process is in place to decontaminate visors
33. Equipment for vehicle/ambulance decontamination is made available and solutions replaced daily (where applicable)
34. Body management is planned and equipment/bags ready
35. All space in the hospital complex was evaluated for possible use as surge capacity
36. The identified spaces were categorised for use for the applicable level of care
37. The capacity of each area was calculated utilising the criteria
38. The needs to operationalise these surge areas are calculated and planned for these needs are in place
39. The calculated capacity of all surge areas as well as the lead time to activate each area is recorded
40. The higher command structure is informed of the surge capacity of the hospital
41. Screening and Triage Facility is in place and maintain a unidirectional flow
42. Streaming and screening are implemented for all patients arriving
43. Screening tools are printed and available. Staff is trained in the utilisation and implementation
44. Triage tool for possible COVID-19 is printed and implemented. Staff trained in the use of tool
45. Triage Sieve and Sort tools are printed and staff is trained in the utilisation to address influx of patients
46. District Hospitals and Temporary Facilities are utilising and implementing the upscaling tools for decision making to refer patients to higher levels of care
47. COVID General hospital beds are planned
48. Oxygen administration was analysed and planned
49. Monitoring equipment for all beds are in place
50. Radiography was reviewed and planning in place to provide service to Red Isolation Area
51. Pharmaceutical supplies are planned and brought in line with number of beds
52. Critical Care beds are planned
53. Intubation equipment, process and protective equipment are in place
54. Maximum Mechanical ventilation capability is prepared and serviced
55. Major respiratory support (CPAP + HFNO) planned and ready