Embed Size (px)
Citation preview

Eur J Dent Educ 2002: 6: 128–138 Copyright C Blackwell Munksgaard 2002Blackwell Munksgaard . Printed in Denmark
ISSN 1396-5883
Teaching paediatric dentistry by multimedia:a three-year report
L Brearley Messer1, K. Kan1, A. Cameron2 and R. Robinson2
1Paediatric Dentistry, School of Dental Science, The University of Melbourne, Victoria, Australia, and 2Westmead Hospital Dental Clinical School,Westmead, New South Wales, Australia.
Clinical cases can now be simulated utilising multimedia andused to teach case management to dental students. The mod-ules developed should provide intellectual stimulation, user-inter-action and immediate feedback, in addition to being intuitivelynavigated and user-helpful. Five paediatric dental case modules(early childhood caries, anterior trauma, anterior coronal frag-ment, anterior crossbite and dentigerous cyst) were created, in-stalled in a multimedia presentation tool, PathFinder (fromWestmead Hospital Dental Clinical School, New South Wales,Australia), and used to teach three classes of fourth year dentalstudents at The University of Melbourne. Questionnaires, focusgroups and a review were conducted by an external educationalexpert. Students responded anonymously to general learning
Teaching dental students to treat patients competentlypresents many challenges. In recent years, it has be-come increasingly difficult in many dental schools toaccess suitable patients, in particular child patients,for dental students to become sufficiently experiencedin treating children. This declining availability of suit-able patients may prevent students from gaining ade-quate experience in patient management. A disadvan-tage of traditional preclinical laboratory teaching isthat students cannot integrate theoretical and practi-cal skills, resulting in knowledge fragmentation. Forexample, students may not be competent in combin-ing preventive and restorative management whileintegrating diagnosis and treatment planning (1).
Multimedia case simulations may assist in fillingthese gaps, by replicating clinical situations withoutrequiring ‘live’ patients, and by simulating biologicalevents that would not be otherwise possible (2). Themodules can provide an opportunity to develop andconsolidate the concepts of integrated patient care andallow interactive learning in a non-threatening en-vironment. In particular, learning outcomes can ad-dress: (a) history-taking, examination, diagnosis andtreatment planning skills; (b) integration of theoreticaland practical aspects of case management; and (c) rel-evance of medical conditions to oral health and treat-ment planning.
128
questions and case specific questions using a five-point Likertscale (strongly agree to strongly disagree). Student responsesindicated they were very enthusiastic about learning via multime-dia, although a few students disliked this educational approach.Focus groups and external review indicated that the moduleswere navigated readily and were suitably interactive.
Key words: Paediatric dentistry; multimedia; dental education;diagnosis; case management.
C Blackwell Munksgaard 2002
Accepted for publication 17 July 2001
The educational psychology literature indicates thatgood multimedia teaching modules will provide intel-lectual stimulation for the student and immediatefeedback (3). Navigation of the module will be intuit-ive, and interactivity will engage the student in activelearning; the student will have maximum controlwithin the module and the design will include user-helpful features (3, 4).
With the incorporation of multimedia into teachingand learning, there is a need to examine its value ineducation. Evaluation can be either formative or sum-mative; formative evaluation addresses refinementand improvement of instruction, and summativeevaluation addresses the end point of instruction andits impact on effectiveness (5). Formative evaluationis necessary to improve computer-assisted educationand to document its effectiveness (6). Formativeevaluation should be based on a variety of measuresincluding user questionnaires, expert review, obser-vation and interviews (7, 8).
This paper describes the initial experiences with amultimedia presentation tool developed for case-based instruction and used in teaching paediatric den-tistry to three classes of fourth year dental students atthe School of Dental Science, The University of Mel-bourne, Australia, in 1998–2000. The objectives of thisproject were to: (a) create educationally useful and in-

Teaching by multimedia
tellectually stimulating paediatric dental cases and in-stall them in a multimedia presentation tool designedfor case-based instruction, and (b) conduct formativeevaluation of student responses.
Materials and methods
The multimedia presentation toolA multimedia presentation tool, PathFinder, was de-veloped in 1997 (by authors AC and RR, WestmeadHospital Dental Clinical School, Westmead, NSW2045, Australia) for case-based instruction, and be-came available to other dental schools in 1998. Todate, 12 paediatric dental case modules have beencreated (by authors KK and LBM) and installed inPathFinder at the School of Dental Science, The Uni-versity of Melbourne. Five of the modules have beenused by three classes of fourth year dental students(1998–2000).
The PathFinder specifications are: CPU: Pentium166 or better; Bus: PCI; CD: 4X or better; video card:2 MB memory; individual monitor: 15–17 inches;memory: 48–64 MB RAM; hard disk space: 1 GB mini-mum; operating system: Windows 95, NT 4.0 orbetter. At The University of Melbourne, Apple Macin-tosh G3266 MH computers are used, 64 MB RAM,hard disk space 4 GB, virtual PC2 (simulating Penti-um 98 MH, 38 MB RAM).
Creation and installation of casesIn designing modules, photographs and radiographsfrom actual patients were used to create fictional pa-tients with symptoms, presenting features and histo-ries. The cases were installed in PathFinder accordingto the developers’ instructions. Images were scannedand inserted into selected screens (as ‘thumbnails’ tobe enlarged for detailed viewing), and descriptionsadded for significant areas (accessed by clicking on‘hotspots’). In creating histories, many questions adentist might ask were inserted, followed by the pa-tient’s responses and a summary of each response,which the user could record in the patient’s file. Thedifferential and definitive diagnoses and treatmentplan, as determined by an ‘expert’, were inserted (ac-cessible to the user after completion of the case). Eachmodule was pretested with paediatric dentists forcontent, intellectual challenge and navigation.
Student use of case modulesThe modules were used in two laboratory sessions(total six hours). Following an on-screen orientationtutorial (with sound), students studied each moduleinteractively, taking histories, conducting examina-
129
tions and special investigations, forming differentialdiagnoses, establishing definitive diagnoses, and de-veloping treatment plans.
The PathFinder screen has four quadrants address-ing the user’s questions (upper left), case images(upper right), parent/patient responses (lower left),and the patient’s file (lower right). Screen tabs (upperand right sides) provide access to history, examina-tion, special investigations, diagnosis and treatmentsections. Information is selected and collected into thepatient’s file using mouse clicks and menus. The pro-gram does not allow direct entry of questions. Follow-ing an examination, a clinical charting (an ‘odontog-ram’) is completed. The user selects case managementfrom on-screen options, taking all information intoconsideration, and prepares a treatment plan. Intellec-tual ‘blocks’ prevent the user from proceeding totreatment without first completing history taking, anexamination and establishing differential and defini-tive diagnoses. At the end, the user compares theirwork with that of the expert.
Each session (for 16 students) was supervised byone tutor (LBM), who answered questions and dis-cussed the modules and other cases in an informaltutorial at the end. The sessions were accompanied bya series of 16 lectures and eight preclinical laboratorysessions, preceding clinical experience in paediatricdentistry in the curriculum.
The case modulesFive modules were studied in the order given below.The scenarios were not provided in advance; this in-formation was obtained by the student from the mod-ule by interpretation and observation. Learning out-comes were provided to the students in advance.
Case number 1: ‘Jane’: Four year-old ‘Jane’ was bornwith feeding difficulties and is still put to bed with abottle of milk. She has occasional asthma during thewinter. She presents with a history of toothache forthe past week that is aggravated by chewing. Pre-viously ‘Jane’ had two appointments with anotherdentist for restorations. Her mother reports ‘Jane’ didnot cope well and cried constantly. At home she ref-uses to have her teeth cleaned. ‘Jane’ lives with hermother, attends kindergarten and visits her father atweekends. Examination indicates she has early child-hood caries (ECC).
Case number 2: ‘James’: ‘James’ presents with an EllisClass 3 fracture of the maxillary left permanent cen-tral incisor and gingival lacerations. The accident, in-volving a basketball, occurred 20min ago without lossof consciousness. ‘James’ is a healthy, 15 year-old stu-dent in the tenth grade, with a history of regular den-

Brearley Messer et al.
tal attendance. He plays competition basketball andfootball.
Case number 3: ‘Brendan’: Fourteen year-old ‘Brend-an’ was referred by his doctor following dentaltrauma involving a homemade slingshot. The crownof his maxillary right permanent lateral incisor is frac-tured in the gingival one-third. The accident occurredtwo hours ago without loss of consciousness. Thetooth fragment was found and a tetanus booster wasgiven. ‘Brendan’ fractured his left arm at the age ofseven years and he is allergic to penicillin. His parentsare separated and his mother has two jobs.
Case number 4: ‘Nancy’: Seven year-old ‘Nancy’ hasmild cerebral palsy and walks with difficulty. She hadorthopaedic surgery at two years of age and uses amodified wheelchair. She lives at home with her par-ents and older sister. ‘Nancy’ is at an age-appropriatelevel in school. Her family moved recently from inter-state. She has visited the dentist regularly. An anteriorsingle tooth crossbite is noted at her examination.
Case number 5: ‘Cindy’: ‘Cindy’ has an unrepairedventricular septal cardiac defect. She is nine years old,currently enjoys fourth grade at the local primaryschool, and has been referred from the school dentalservice for treatment of an unerupted permanenttooth. Radiographic examination indicates a possibledentigerous cyst.
For each case, students were required to take a his-tory, conduct an examination, identify necessaryspecial investigations, establish a diagnosis, prepare atreatment plan and recommend preventive measures.After studying each case, the student should be ableto describe the typical appearance of the condition,the aetiological factors, significance of the family andsocial histories, the most appropriate management,and the prognosis for the case.
Formative evaluation by questionnaireFollowing each module, students completed ananonymous questionnaire designed by an educationexpert (Biomedical Multimedia Unit, The Universityof Melbourne). Not all students in each class attendedthe lab sessions and not all attending students com-pleted the questionnaires. All returned questionnaireswere completed without facetious responses. Studentresponses were: 1998, n Ω48, 41–42 (85–87% re-sponse); 1999, n Ω55, 30–55 (54–100% response); 2000,n Ω51, 32–43 (63–84% response). Questions were key-ed to the learning outcomes for each case. Each ques-tionnaire contained 13–15 questions, scored on a five-point Likert scale (strongly agree, agree, undecided,disagree, strongly disagree).
For all modules, six to eight case-specific questions
130
(CSQ’s) asked students to what extent the modulehelped them to: recognize the clinical appearance /understand the aetiology of the clinical problem; ap-preciate the significance of the medical / family / so-cial history; order / understand / interpret special in-vestigations; know how to treat; develop and justify asequential treatment plan. Seven general learningquestions (GLQ’s) focused on students’ perceptions oflearning (‘I found this case...interesting / realistic /useful / directive / confusing / helps me relatetheory to clinic / assists my preparation for clinicalpractice’). A distractor question, ‘I found this caseconfusing’, was included to verify students’ readingof questions.
Focus groups and external reviewThree focus groups, each with eight to 10 students,lasting two hours, were held in 1998 by an educationexpert (teaching staff did not attend) to discuss ninequestions: (1) What is the purpose of the package? Isthis clear ? (2) How well does the package simulateclinical experience? (3) How does the program guideyou? (4) How clearly and logically is the content pre-sented? (5) How does the package cater for differentexperience levels? (6) How does the package promotegood clinical skills? (7) What other learning opportun-ities are you guided towards? How would staff knowyou are learning? (8) In what form do you get per-formance feedback? Is this effective? (9) How wouldyou improve the program? The expert also observedmodule use by six students (with informed consent).
Simulation of cases in dental simulatorAfter completing the multimedia modules, students‘treated’ the cases in a dental simulator (OSSIM Simu-lator, Medic Corp., Lower Hutt, New Zealand), usingtissue-specific artificial teeth in primary/mixed den-tition mannikins and instruments and proceduressimilar to those used in school clinics. The use of thedental simulator in preclinical teaching has been de-scribed previously (1); student responses to treatingthe current cases under simulation will not be re-ported here.
Results
Students’ responses to modulesThe distribution of student responses for the CSQ’s isshown in Tables1–5.
Case number 1: ‘Jane’: Responses were provided by87% of the class in 1998, 91% in 1999, and 84% in 2000(Table1). Responses in all years were similar for mostCSQ’s. The majority of students agreed or strongly

Teaching by multimedia
TABLE1. Case no. 1: ‘Jane’ (early childhood caries): responses of dental students in 1998 (nΩ42), 1999 (nΩ50) and 2000 (nΩ43) (a) to casespecific questions
‘This case helped me to...’ Percent distribution of student responses (range)
Strongly agree Agree Undecided Disagree Strongly disagree
‘recognize the clinical 23–31 67–72 2 0–2 0appearance’
‘understand the aetiology’ 16–25 57–64 12–18 0–7 0‘appreciate the significance 12–21 55–58 23–24 0–4 0–2
of family history’‘appreciate the impact of 7–16 44–76 14–37 2–4 0
medical history ondental treatment’
‘understand how past 23–24 65–69 5–8 0–5 0–2treatment may affectcurrent behaviour’
‘order and understand need 14–21 62–67 4–18 0–5 0for special investigations’
‘interpret results of special 16–21 65–70 7–14 2–4 0investigations toestablish diagnosis’
‘develop and justify a 12–26 55–67 14–21 0–7 0sequential treatmentplan’
(a) 42 of 48 students in 1998 (87% class response); 50 of 55 students in 1999 (91% class response); 43 of 51 students in 2000 (84% classresponse).
agreed that this case helped them recognize the clin-ical appearance of ECC, understand its aetiology, ap-preciate family history, understand the impact of pasttreatment, use special investigations and prepare atreatment plan. Concerning the impact of medical his-tory on dental treatment, response was more variable,with 14–37% respondents recording indecision.
Case number 2: ‘James’: Responses were provided by85% of the class in 1998, 100% in 1999, and 84% in2000 (Table2). The majority of students agreed orstrongly agreed that this case helped them recognizeanterior trauma, take a trauma history, appreciate so-cial history, order special investigations and interpretresults of these, and develop a treatment plan. Re-sponse was very variable concerning use of a Cvekpulpotomy, with 7–51% recording indecision.
Case number 3: ‘Brendan’: Responses were providedby 87% of the class in 1998, 94% in 1999, and 63%in 2000 (Table3). The majority of students agreed orstrongly agreed that the case helped them recognizeanterior trauma, take a trauma history, recognizewhen to re-attach a coronal fragment and prepare atreatment plan. Responses were more variable con-cerning appreciation of family and social history (14–31% undecided), use of special investigations (12–32%undecided) and interpretation of results of these (12–25% undecided).
Case number 4: ‘Nancy’: Responses were provided by85% of the class in 1998, by 91% in 1999, and 82%in 2000 (Table4). The majority of students agreed or
131
strongly agreed that this case helped them conduct anexamination and recognize anterior crossbite. Re-sponses were more variable concerning appreciationof the medical history (5–23% undecided), family andsocial history (12–28% undecided), the relationshipbetween medical history and treatment (7–24% unde-cided) and preparation of a treatment plan (12–21%undecided).
Case number 5: ‘Cindy’: Responses were provided by87% of the class in 1998, 54% in 1999, and 82% in 2000(Table5) (the low response rate in 1999 was due toinvestigator error in failing to distribute the ques-tionnaires to all attending students). The majority ofstudents agreed or strongly agreed that this casehelped them to recognize a dentigerous cyst, appreci-ate the significance of medical history, use special in-vestigations, consider differential diagnoses, and pre-pare a treatment plan. Responses were more variableconcerning interpretation of results of special investi-gations (12–27% undecided) and consideration of as-sociated medical conditions (19–27% undecided).
The distribution of student responses (pooled over1998–2000) to the GLQ’s are shown in Fig.1. The totalresponses for each case were: ‘Jane’, n Ω135; ‘James’,n Ω139; ‘Brendan’, n Ω126; ‘Nancy’ n Ω134; ‘Cindy’,n Ω114. Students rated all cases interesting, accordinghighest values for strong agreement to ‘James’ (45%),and for agreement to both ‘Nancy’ and ‘Cindy’ (69%;Fig.1a). All cases were considered realistic withhighest values for strong agreement for ‘James’ (39%),

Brearley Messer et al.
TABLE2. Case no. 2: ‘James’ (anterior trauma): responses of dental students in 1998 (nΩ41), 1999 (nΩ55) and 2000 (nΩ43) (a) to case specificquestions
‘This case helped me to...’ Percent distribution of student responses (range)
Strongly agree Agree Undecided Disagree Strongly disagree
‘recognize the clinical 36–44 53–58 5–7 0 0appearance’
‘take a detailed trauma 17–20 65–78 5–13 0–2 0history’
‘appreciate significance of 12–24 63–71 9–19 2–4 0social history’
‘order and understand 7–22 60–76 5–19 2–7 0need for specialinvestigations’
‘interpret results of special 12–20 65–76 5–19 0–5 0investigations’
‘understand when to use a 12–27 22–62 7–51 4–15 0–2Cvek pulpotomy’
‘develop and justify a 15–27 51–63 9–29 2–5 0sequential treatmentplan’
(a) 41 of 48 students in 1998 (85% class response); 55 of 55 students in 1999 (100% class response); 43 of 51 students in 2000 (84% classresponse).
TABLE3. Case no. 3: ‘Brendan’ (coronal tooth fragment): responses of dental students in 1998 (nΩ42), 1999 (nΩ52) and 2000 (nΩ32) (a) to casespecific questions
‘This case helped me to...’ Percent distribution of student responses (range)
Strongly agree Agree Undecided Disagree Strongly disagree
‘recognize the clinical 19–41 56–74 2–7 0–4 0appearance’
‘take a detailed trauma 16–41 56–74 3–7 0–2 0history’
‘appreciate significance of 9–22 54–67 14–31 3–9 0family and socialhistory’
‘order and understand need 9–19 52–66 12–32 5–9 0for special investigations’
‘interpret results of special 12–19 50–69 12–25 5–6 0investigations’
‘recognize when to re-attach 23–34 50–62 9–16 4–5 0–2a coronal tooth fragment’
‘develop and justify a 15–34 59–69 6–16 0–2 0sequential treatmentplan’
(a) 42 of 48 students in 1998 (87% class response); 52 of 55 students in 1999 (94% class response); 32 of 51 students in 2000 (63% classresponse).
and for agreement for ‘Nancy’ (73%; Fig.1b). Studentsrated all cases as useful, with highest values for strongagreement again for ‘James’ (37%), and for agreementfor both ‘Nancy’ and ‘Cindy’ (69%; Fig.1c). Althoughthe highest value for agreement that the case was di-rective was accorded to ‘Nancy’ (68%; Fig.1d), manystudents were uncertain on whether the cases weredirective, with undecided responses ranging from17% (‘Nancy’) to 32% (‘Cindy’). This may have re-flected their uncertainty of the meaning of the term‘directive’. The distractor question (‘case is confus-ing’) was identified correctly by most students, as dis-
132
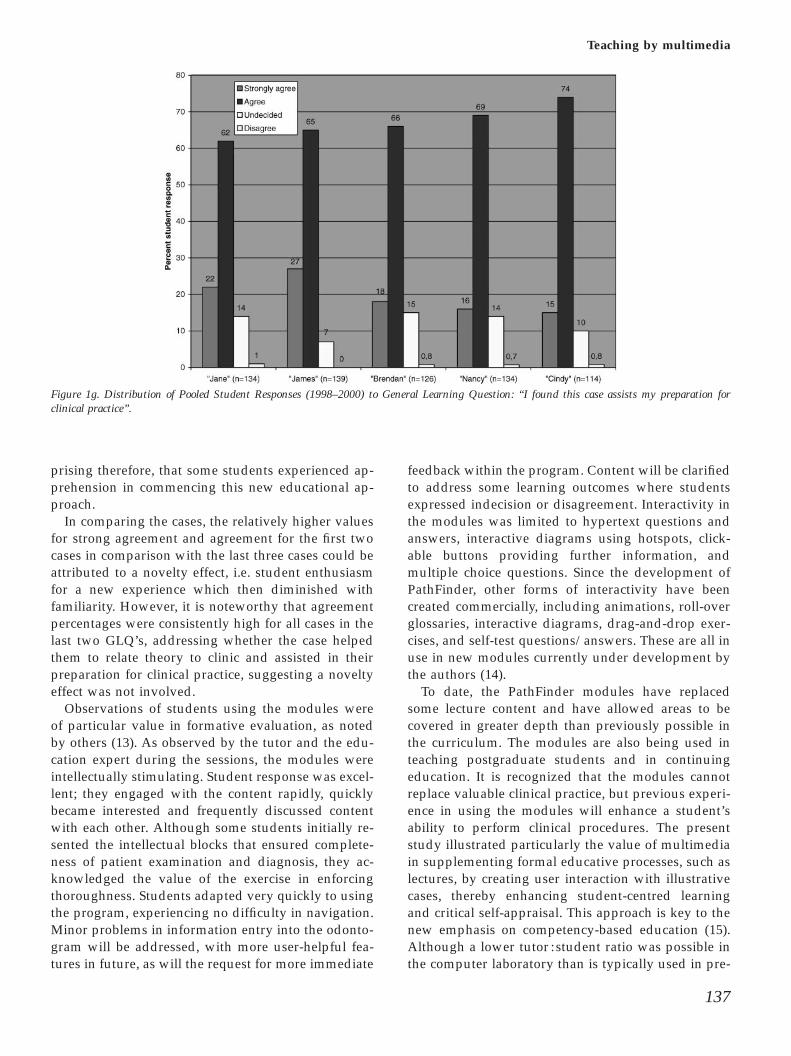
agreement or strong disagreement were the dominantresponses for all cases (Fig.1e). Most students con-sidered that the cases helped them relate theory toclinic, with high values for agreement (67–72%) beingrecorded for all cases (Fig.1f). Similarly, most studentsthought that the cases assisted their preparation forclinical practice, with high values for agreement (62–74%) noted for all cases (Fig.1g).
Focus groups and external reviewA total of 28 students attended the focus groups. Theobservations reported to the authors by the education
Teaching by multimedia
TABLE4. Case no. 4: ‘Nancy’ (anterior crossbite): responses of dental students in 1998 (nΩ41), 1999 (nΩ50) and 2000 (nΩ42) (a) to case specificquestions
‘This case helped me to...’ Percent distribution of student responses (range)
Strongly agree Agree Undecided Disagree Strongly disagree
‘conduct a full examination’ 12–14 74–84 2–10 0–2 0‘appreciate significance of 12–19 62–71 5–23 0–5 0
medical history‘appreciate significance of 12–19 57–62 12–28 2–7 0
family and social history‘recognize the clinical 32–51 49–62 0–4 0–2 0
appearance‘consider the medical 12–17 50–66 7–24 5–12 0
condition in relation tocrossbite treatment
‘develop and justify a 12–14 60–71 12–21 4–5 0sequential treatmentplan
(a) 41 of 48 students in 1998 (85% class response); 50 of 55 students in 1999 (91% class response); 42 of 51 students in 2000 (82% classresponse).
TABLE5. Case no. 5: ‘Cindy’ (dentigerous cyst): responses of dental students in 1998 (nΩ42), 1999 (nΩ30) and 2000 (nΩ42) (a) to case specificquestions
‘This case helped me to...’ Percent distribution of student responses (range)
Strongly agree Agree Undecided Disagree Strongly disagree
‘recognize the clinical 10–24 55–63 7–20 5–17 0–2appearance’
‘appreciate the significance 10–21 67–74 9–17 2–3 0of medical history’
‘order and understand need 20–24 60–67 5–17 0–5 0–3for special investigations’
‘interpret results of special 9–17 57–67 12–27 0–12 0–3investigations toestablish diagnosis’
‘consider differential 10–17 61–69 7–19 2–9 0diagnoses’
‘’consider the medical 7–21 52–59 19–27 7 0condition in relation tomanagement of thepathology’
‘’develop and justify a 7–14 59–69 17 7–9 0sequentialtreatment plan’
(a) 42 of 48 students in 1998 (87% class response); 30 of 55 students in 1999 (54% class response); 42 students of 51 students in 2000 (82%class response).
expert were as follows. Students were unanimous inarticulating package purposes and indicating thesewere clear. The ability of the package to simulate realclinical experience was rated highly by all students.A few commented that the user was unable to struc-ture their own questions or practice patient manage-ment skills, while acknowledging ‘these are better leftfor the clinic’. A few students did not appreciate theintellectual blocks placed to prevent treatment beingperformed before a definitive diagnosis was estab-lished, and a few found the refining of diagnoses to berepetitive. Content was deemed by all to be presented
133
clearly and logically, with easy navigation and muchinteractivity. A few students considered that the pro-gram did not cater for different levels of experience(a glossary was recommended), but this was largelyovercome by its user-friendliness. All students con-sidered the package promoted good diagnostic skills,but could not address patient communication; itprompted them to ‘look up special tests and differentdiseases’ which could be quizzed by staff in later ses-sions. The majority of students would have preferredimmediate feedback provided within the program,rather than retrospective feedback at the end. Im-

Brearley Messer et al.
Figure 1a. Distribution of Pooled Student Responses (1998–2000) to General Learning Question: ‘‘I found this case interesting’’.
Figure 1b. Distribution of Pooled Student Responses (1998–2000) to General Learning Question: ‘‘I found this case realistic’’.
provements suggested included providing referencesand videos to indicate patient responses.
In observing module use, the education expertnoted students engaging well with the content andrapidly becoming absorbed. However, some were in-discriminate in the information they selected for thepatient’s file, preferring to collect everything withoutnoting relevant details. The differential diagnosis sec-tion appeared very helpful, and students were par-ticularly attentive in refining their diagnoses. Thebrevity of images for some cases prompted energeticdiscussion among students about what they would
134
like to order. Such student interactions appeared to bevery useful in exchanging knowledge and infor-mation about navigating the module. The tutor-guided discussion was considered very helpful.
Discussion
Computer-assisted education in dentistry is in itsearly stages; developments in information technologyand implementation are occurring rapidly, and edu-cators must evaluate modules developed internally orpurchased (9–11). Sound instructional design indi-

Teaching by multimedia
Figure 1c. Distribution of Pooled Student Responses (1998–2000) to General Learning Question: ‘‘I found this case useful’’.
Figure 1d. Distribution of Pooled Student Responses (1998–2000) to General Learning Question: ‘‘I found this case directive’’.
cates that the goals of instruction must be clear, sothat students know what is expected of them in navig-ating a module (12). These may not have been clearin parts of some modules in the present study, and fora few of the students reporting negative responses.Nonetheless, it was noted that computer-assisted in-struction was received enthusiastically by most stu-dents (in all years, students requested extra sessionsto study the modules further). Focus groups indicatedthat the students valued the tutor-led discussions,
135
which provided extension of learning and pro-fessional role-modelling.
Future studies will investigate the reasons for somestudents disliking learning by computer modules.Discussion with several of these students indicated anumber of reasons. Firstly, they preferred to studyfrom print material where they were free to choosethe extent and depth of information acquired and toexplore this in a self-directed manner, rather than tohave their learning style preprogrammed or dictated

Brearley Messer et al.
Figure 1e. Distribution of Pooled Student Responses (1998–2000) to General Learning Question: ‘‘I found this case confusing’’.
Figure 1f. Distribution of Pooled Student Responses (1998–2000) to General Learning Question: ‘‘I found this case helps me relate theory to clinic’’.
to them. Secondly, they felt threatened by the ap-parent ‘competition’ with fellow students who weremore computer-literate and therefore perceived tohave an advantage. Thirdly, they felt they were being‘tested’ by the multimedia module when they had notbeen able to prepare ahead. However, some studentsagreed that these anxieties were more apparent thanreal, and their anxiety had lessened by the time theycompleted the second session.
136
The three classes of students studied had little pre-vious experience in computer-based instruction, asused in the dental school curriculum. At the time ofthe present study, computer-assisted education wasused only in two areas of the dental school: paediatricdentistry and oral pathology and oral medicine. Anyprevious experience with computer-assisted edu-cation would likely have been through personal useof computers or in secondary education. It is not sur-
Teaching by multimedia
Figure 1g. Distribution of Pooled Student Responses (1998–2000) to General Learning Question: ‘‘I found this case assists my preparation forclinical practice’’.
prising therefore, that some students experienced ap-prehension in commencing this new educational ap-proach.
In comparing the cases, the relatively higher valuesfor strong agreement and agreement for the first twocases in comparison with the last three cases could beattributed to a novelty effect, i.e. student enthusiasmfor a new experience which then diminished withfamiliarity. However, it is noteworthy that agreementpercentages were consistently high for all cases in thelast two GLQ’s, addressing whether the case helpedthem to relate theory to clinic and assisted in theirpreparation for clinical practice, suggesting a noveltyeffect was not involved.
Observations of students using the modules wereof particular value in formative evaluation, as notedby others (13). As observed by the tutor and the edu-cation expert during the sessions, the modules wereintellectually stimulating. Student response was excel-lent; they engaged with the content rapidly, quicklybecame interested and frequently discussed contentwith each other. Although some students initially re-sented the intellectual blocks that ensured complete-ness of patient examination and diagnosis, they ac-knowledged the value of the exercise in enforcingthoroughness. Students adapted very quickly to usingthe program, experiencing no difficulty in navigation.Minor problems in information entry into the odonto-gram will be addressed, with more user-helpful fea-tures in future, as will the request for more immediate
137
feedback within the program. Content will be clarifiedto address some learning outcomes where studentsexpressed indecision or disagreement. Interactivity inthe modules was limited to hypertext questions andanswers, interactive diagrams using hotspots, click-able buttons providing further information, andmultiple choice questions. Since the development ofPathFinder, other forms of interactivity have beencreated commercially, including animations, roll-overglossaries, interactive diagrams, drag-and-drop exer-cises, and self-test questions/answers. These are all inuse in new modules currently under development bythe authors (14).
To date, the PathFinder modules have replacedsome lecture content and have allowed areas to becovered in greater depth than previously possible inthe curriculum. The modules are also being used inteaching postgraduate students and in continuingeducation. It is recognized that the modules cannotreplace valuable clinical practice, but previous experi-ence in using the modules will enhance a student’sability to perform clinical procedures. The presentstudy illustrated particularly the value of multimediain supplementing formal educative processes, such aslectures, by creating user interaction with illustrativecases, thereby enhancing student-centred learningand critical self-appraisal. This approach is key to thenew emphasis on competency-based education (15).Although a lower tutor : student ratio was possible inthe computer laboratory than is typically used in pre-

Brearley Messer et al.
clinical laboratory classes, the value of having a tutoravailable during the sessions was evident in studentresponses. Computer-assisted education of this typecannot be totally self-directed by students, and teach-ing staff are still necessary, particularly as they canprovide strong professional role models.
Conclusions
Following the creation and installation of five paediat-ric dental cases in a multimedia presentation tool, for-mative evaluation of dental student responses over athree-year period showed that computer-assistedteaching of case management using these moduleswas received enthusiastically by the majority of dentalstudents, although a few students consistently dis-liked computer-assisted education.
Acknowledgements
The authors are grateful for the award of several educationaldevelopmental grants (1998–99) from CAUT and CUTSDCommittees of the Australian federal government, the TALmetCommittee (The University of Melbourne), and the School ofDental Science, The University of Melbourne. The assistanceof Jean-Paul Talary (Westmead) in computer programming,and Drs G. Kennedy and M. Keppell (Biomedical MultimediaUnit, The University of Melbourne) for educational expertiseand multimedia guidance, is acknowledged with gratitude. Thesupport of the teaching staff and the graduate students in Pae-diatric Dentistry at The University of Melbourne School ofDental Science, and particularly Drs T. Johnston, C. Olsen, RPatel, J. Sheahan and N. Vasan and for providing cases iswarmly acknowledged.
References
1. Suvinen TI, Messer LB, Franco E. Clinical simulation inteaching pre-clinical dentistry. Eur J Dent Educ 1998: 2: 25–32.
2. Schleyer TKL. Dentistry 2000: Technology – Digital dentistryin the computer age. J Am Dent Assoc 1999: 130: 1713–1720.
138
3. Heinze-Fry JA, Crovello TJ, Novak JD. Integration of Ausub-elian learning theory and educational computing. The AmBiol Teacher 1984: 46: 152–156.
4. Schuhbeck M, Hassfield S, Koke U, Muhling J. Developmentof interactive multimedia-CBT-program for dental implant-ology and using tests of a program prototype. Eur J DentEduc 1999: 3: 35–43.
5. Dick W, Carey LM. Formative evaluation. In: LJ Briggs, KLGustafson, MH Tillman, eds. Instructional Design. Prin-ciples and Applications. Educational Technology Publi-cations, Englewood Cliffs, New Jersey, USA, 1991: 227–667.
6. Kennedy GE. Defining the dimensions of a formative evalu-ation program: A multi-method, multi-perspective approachto the evaluation of multimedia. In: Collis B, Oliver R, eds.Proceedings of ED-MEDIA 1999 World Conference onEducational Multimedia, Hypermedia and Telecommuni-cations, Seattle, Washington, USA. June 19–24, 1999 Associ-ation for the Advancement of Computing in Education,Charlottesville, Virginia, USA, 1999: 604–609.
7. Herrington J, Oliver R. Multimedia, magic and the way stu-dents respond to a situated learning environment. Aust JEduc Technol 1997: 13: 127–143.
8. Reeves TC, Harmon SW. Systematic evaluation proceduresfor interactive multimedia for education and training. In:Reisman S, ed. Multimedia Computing: Preparing for the21st Century. Idea Group Publishing, Harrisburg, Pennsyl-vania, USA, 1994: 472–505.
9. Mercer PE, Ralph JP. Computer assisted learning and thegeneral dental practitioner. Br Dent J 1998: 184: 43–46.
10. Weerakone S, Turner PJ. Basic computing for dental prac-titioners: 6. Multimedia Comm Dental Update 1998: 25: 418–423.
11. Yip H-K, Barnes IE. Information technology in dental edu-cation. Br Dent J 1999: 187: 327–332.
12. Plasschaert AJ, Wilson NH, Cailleteau JG, Vendonschot EH.Opinions and experiences of dental students and facultyconcerning computer-assisted learning. J Dent Educ 1995:59: 1034–1040.
13. Lechner SK, Lechner KM, Thomas GA. Evaluation of a com-puter-aided learning program in removable partial dentureframework designing. J Prosthod 1999: 8: 100–105.
14. Keppell M, Kan K, Messer LB. Enhancing total patient man-agement skills in dentistry with interactive multimediasimulation. In: Bourdeau J, Heller R, eds. Proceedings of ED-MEDIA 2000 World Conference on Educational Multimedia,Hypermedia and Telecommunications, Montreal, Quebec,Canada, June 26-July 1, 2000. Association for the Advance-ment of Computing in Education, Charlottesville, Virginia,USA, 1639–1640.
15. Yip H-K, Smales RJ. Review of competency-based educationin dentistry. Br Dent J 2000: 189: 324–326.





























