Embed Size (px)
Citation preview
This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
Teaching Cultural Competence in Nursing and Health Care

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
Marianne R. Jeffreys, EdD, RN, is a nurse educator whose grant-funded research, consultations, publications, and professional presentations encompass the topics of cultural competence, nontraditional students, student retention and achievement, self-efficacy, teaching, curriculum, and psychometrics. The first edition of her book Teaching Cultural Competence in Nursing and Health Care: Inquiry, Action, and Innovation received the AJN Book of the Year Award; she is also the author of the book Nursing Student Retention: Understanding the Process and Making a Difference, as well as articles, book chapters, and videos. Her conceptual models and questionnaires have been requested worldwide and used in various disciplines. She is currently a professor of nursing at the City University of New York (CUNY) Graduate College and at CUNY College of Staten Island.
Dr. Jeffreys received a BS in nursing from the State University of New York College at Plattsburgh and MA, MEd, and EdD degrees in nursing education from Teachers College, Columbia University. She is a Fellow of the New York Academy of Medicine. Her awards include the international Leininger Award for Excellence in Transcul-tural Nursing, Columbia University’s Teachers College Award for Scholarship and Research, and the Mu Upsilon Chapter of Sigma Theta Tau Excellence in Profes-sional Nursing Award. She was named Consultant of the Month (December 2007) by the National Center for Cultural Competence. Her expertise has been requested for grant-funded projects (from, e.g., the U.S. Department of Health and Human Resources, Health Resources and Services Administration and the W.K. Kellogg Foundation), as well as for institutional and departmental workshops.
This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
Teaching Cultural Competence in Nursing and Health Care
Inquiry, Action, and Innovation
Third Edition
Marianne R. Jeffreys, EdD, RN

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
Copyright © 2016 Springer Publishing Company, LLC
All rights reserved.
No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise, without the prior per-mission of Springer Publishing Company, LLC, or authorization through payment of the appropriate fees to the Copyright Clearance Center, Inc., 222 Rosewood Drive, Danvers, MA 01923, 978-750-8400, fax 978-646-8600, [email protected] or on the Web at www.copyright.com.
Springer Publishing Company, LLC11 West 42nd StreetNew York, NY 10036www.springerpub.com
Acquisitions Editor: Joseph MoritaComposition: S4Carlisle
ISBN: 978-0-8261-1996-4e-book ISBN: 978-0-8261-1997-1
15 16 17 18 / 5 4 3 2 1
The author and the publisher of this Work have made every effort to use sources believed to be reliable to provide information that is accurate and compatible with the standards generally accepted at the time of publication. Because medical science is continually advancing, our knowledge base continues to expand. Therefore, as new information becomes available, changes in procedures become necessary. We recommend that the reader always consult current research and specific institutional policies before performing any clinical procedure. The author and publisher shall not be liable for any special, conse-quential, or exemplary damages resulting, in whole or in part, from the readers’ use of, or reliance on, the information contained in this book. The publisher has no responsibility for the persistence or ac-curacy of URLs for external or third-party Internet websites referred to in this publication and does not guarantee that any content on such websites is, or will remain, accurate or appropriate.
Library of Congress Cataloging-in-Publication DataJeffreys, Marianne R., author. Teaching cultural competence in nursing and health care inquiry, action, and innovation / Marianne R. Jeffreys. — Third edition. p. ; cm. Includes bibliographical references and index. ISBN 978-0-8261-1996-4 — ISBN 978-0-8261-1997-1 (e-book) I. Title. [DNLM: 1. Transcultural Nursing—education. 2. Cultural Competency—education. WY 18] RT86.5 610.73—dc23 2015036958
Special discounts on bulk quantities of our books are available to corporations, professional associations, pharmaceutical companies, health care organizations, and other qualifying groups. If you are interested in a custom book, including chapters from more than one of our titles, we can provide that service as well.
For details, please contact:Special Sales Department, Springer Publishing Company, LLC11 West 42nd Street, 15th Floor, New York, NY 10036-8002Phone: 877-687-7476 or 212-431-4370; Fax: 212-941-7842E-mail: [email protected]
Printed in the United States of America by McNaughton & Gunn.

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
To my son, Daniel W. Edley

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
vii
Contents
Contributors xiPreface xv
PART I. GETTING STARTED 1
1. Overview of Key Issues and Concerns, with contributions from Kevin Antoine 3
2. Dynamics of Diversity: Becoming Better Health Care Providers Through Cultural Competence 41
3. A Model to Guide Cultural Competence Education 65
PART II. TOOLS FOR ASSESSMENT AND EVALUATION 89
4. Transcultural Self-Efficacy Tool (TSET), with contributions from Fatma Basalan
.Iz, Ayla Baylk Temel, Jing Chen, Mark
Fridline, Faye J. Grund, Margaret M. Halter, Maria Malliarou, Carol Reece, Pavlos Sarafis, Sharon See, and Lisa Young 91
5. A Guide for Interpreting Learners’ Transcultural Self-Efficacy (TSE) Perceptions, Identifying At-Risk Individuals, and Avoiding Pitfalls 141
6. Cultural Competence Clinical Evaluation Tool (CCCET) and Clinical Setting Assessment Tool–Diversity and Disparity (CSAT–DD), with contributions from Enis Dogan and Lynn Schmidt 161
This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
viii CONTENTS
PART III. EDUCATIONAL ACTIVITIES FOR EASY APPLICATION: ACADEMIC SETTINGS 195
7. Academic Settings: General Overview, Faculty Self-Assessment, and Curriculum Evaluation, with contributions from Phyllis D. Barham, Richardean Benjamin, Patricia Burrell, Phyllis M. Eaton, Grace Hoyer, Kay Palmer, Carolyn M. Rutledge, Joanne K. Singleton, Jason T. Slyer, and Lynn Wiles 199
8. Enhancing Cultural Competence: Face-to-Face Classrooms, Hybrid, and Online Courses, with contributions from Theresa M. Adams and Kathleen M. Nevel 243
9. Enhancing Cultural Competence: Clinical Settings, Immersion Experiences, Service-Learning, Simulation, and Nursing Skills Laboratory, with contributions from Roxanne Amerson, Susan Fancher, Rachelle Larsen, Polly M. McArthur, Sandra J. Mixer, LuAnn Reif, and Monique Rogers-Walker 289
10. Case Exemplar: Linking Strategies—Spotlight on the Cultural Discovery Integrated Approach, with contributions from Mary O’Donnell and Judy Xiao 335
11. Case Exemplar: Linking Strategies—Spotlight on the Innovative Field Trip Experience, with contributions from Lenore Bertone, Jo-Ann Douglas, Vivien Li, and Sara Newman 363
12. Faculty Advisement and Helpfulness: A Culturally Congruent Approach 387
This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
CONTENTS ix
PART IV. EDUCATIONAL ACTIVITIES FOR EASY APPLICATION: HEALTH CARE INSTITUTIONS 411
13. Health Care Institutions: General Overview, Inquiry, Action, and Innovation, with contributions from Carolyn Bloch, Stephen R. Marrone, and Jeanette Velez 413
14. Case Exemplar: Linking Strategies—Spotlight on Employee Orientation Programs to Enhance Cultural Competence, with contributions from Cynthia Karczewski 467
15. Case Exemplar: Linking Strategies—Spotlight on Employee In-Service Education to Enhance Cultural Competence, with contributions from Patricia Bartley-Daniele and Karen Kennedy 491
PART V. EDUCATIONAL ACTIVITIES FOR EASY APPLICATION: PROFESSIONAL ASSOCIATIONS, PARTNERSHIPS, AND FUTURE DIRECTIONS 517
16. Professional Associations: General Overview, Inquiry, Action, and Innovation, with contributions from Margaret Andrews, Eleanor T. Campbell, John Collins, Stephen R. Marrone, and Michelle Romano 519
17. New Priorities: Challenges and Future Directions 561
Appendix: Studies Involving Jeffreys’s Transcultural Self-Efficacy Tool (TSET) and/or Jeffreys’s Cultural Competence and Confidence (CCC) Model, with contributions from Eda Ozkara San 575
Index 583

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
xi
Theresa M. Adams, PhD, RN, CSNAssociate Professor of NursingAlvernia UniversityReading, Pennsylvania
Roxanne Amerson, PhD, RN, BC, CTN-A
Associate Professor of NursingClemson UniversityClemson, South Carolina
Margaret Andrews, PhD, RN, CTN-A, FAAN
Director and Professor of NursingSchool of Health Professions and
StudiesUniversity of Michigan-FlintFlint, Michigan
Kevin Antoine, JDAssistant Vice President for Diversity &
InclusionAssistant Professor of Health Law &
PolicyState University of New York (SUNY)
DownstateBrooklyn, New York
Phyllis D. Barham, RN, MS(Retired), Senior Lecturer and Chief
Academic AdvisorBachelor of Science in Nursing
ProgramOld Dominion UniversityNorfolk, Virginia
Patricia Bartley-Daniele, PhD, FNP-BC, CCRN, CNRN, CAPAN, CAPA
Nurse PractitionerDepartment of Advanced Practice
NursingDepartment of AnesthesiaNew York University Langone
Medical CenterNew York, New York
Richardean Benjamin, PhD, PMHCNS-BC, MPH, ANEF, FAAN
Associate DeanCollege of Health SciencesOld Dominion UniversityNorfolk, Virginia
Lenore Bertone, MS, RNAdjunct Instructor, NursingThe City University of New York
(CUNY) College of Staten IslandStaten Island, New YorkTreatment Team LeaderSouth Beach Psychiatric CenterStaten Island, New York
Carolyn Bloch, PhD, RN, CNS, CTN-AFaculty, Ambulatory Care ServicesLos Angeles County and University of
Southern California Medical CenterLos Angeles, California
Contributors
This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
xii CONTRIBUTORS
Patricia Burrell, PhD, APRN, APMHCNS-BC, CNE
Assistant Dean of Nursing StudentsEvaluation & Research Director,
Transcultural Nursing CenterProfessor of NursingCollege of Nursing and Health
SciencesHawaii Pacific UniversityKaneohe, Hawaii
Eleanor T. Campbell, EdD, NP-CAssociate Professor, NursingDirector, Graduate ProgramsLehman College, The City University
of New York (CUNY)Bronx, New York
Jing Chen, MSN, RNOffice Deputy Director of Nursing
SchoolShanghai Polytechnic CollegeShanghai, China
John Collins, PhDc, RNProgram Manager-Flint NursingSchool of Health Professions and StudiesUniversity of Michigan-FlintFlint, Michigan
Enis Dogan, EdDAssociate Director for ResearchPartnership for Assessment of
Readiness for College and Careers (PARCC)
Washington, DC
Jo-Ann Douglas, MS, CRNPCertified Registered Nurse
PractitionerCardiovascular MedicineUniversity of Maryland Medical
CenterBaltimore, MarylandBeth Israel Medical CenterNew York, New York
Phyllis M. Eaton, PhD, RN, PMHCNS-BC
DeanBeazley School of NursingTidewater Community CollegePortsmouth, Virginia
Susan Fancher, BSN, RN, CHSE Simulation Director, Clinical Faculty,
NursingUniversity of TennesseeKnoxville, Tennessee
Mark Fridline, PhDAssociate Instructor, StatisticsUniversity of Akron Akron, Ohio
Faye J. Grund, PhD, APRN Dean, School of NursingAshland UniversityAshland, Ohio
Margaret M. Halter, PhD, APRN Associate DeanCollege of Nursing and Health
Sciences (2011–2013)Ashland UniversityAshland, Ohio
Grace Hoyer, EdD, RNAssistant Professor, NursingGrand Valley State UniversityAllendale, Michigan
Fatma Basalan Iz, PhD, RNAssistant ProfessorSüleyman Demirel University Faculty
of Health SciencesCommunity Health Nursing
DepartmentIsparta, Turkey
This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
CONTRIBUTORS xiii
Cynthia Karczewski, MS, RNManhattan Borough Nursing DirectorNew York City Department of Health
and Mental HygieneOffice of School HealthNew York, New York
Karen Kennedy, MS, RN, OCNStaff NurseBone Marrow Transplant UnitHackensack University Medical CenterHackensack, New Jersey
Rachelle Larsen, PhD, RNProfessor, NursingCollege of St. Benedict/St. John’s
UniversitySt. Joseph, Minnesota
Vivien Li, MS, NP-CNurse PractitionerRadiation OncologyMaimonides Medical CenterBrooklyn, New York
Maria Malliarou, MSc, MHA, PhD, RNScientific Collaborator, NursingTechnological Educational Institution
of Thessalia Lamia, Greece
Stephen R. Marrone, EdD, RN-BC, CTN-A
Associate Professor of NursingLong Island UniversityHarriet Rothkopf Heilbrunn School of
NursingBrooklyn, New YorkAdjunct Assistant Professor of
Nursing EducationTeachers College, Columbia UniversityExecutive Program for NursesNew York, New York
Polly M. McArthur, PhD, RN Clinical Assistant Professor, NursingUniversity of TennesseeKnoxville, Tennessee
Sandra J. Mixer, PhD, RN, CTN-AAssistant Professor, NursingUniversity of TennesseeKnoxville, Tennessee
Kathleen M. Nevel, PhD, MEIEAdjunct FacultyAlvernia UniversityReading, Pennsylvania
Sara Newman, MS, RN, ANP-BC, CNS, PC
Lead Home Care ConsultantVisiting Nurse
Service of New YorkNew York, New York
Mary O’Donnell, PhD, RNAssociate Professor and ChairNursing DepartmentThe City University of New York
(CUNY) College of Staten IslandStaten Island, New York
Kay Palmer, MSN, RN, CRRNUndergraduate Program DirectorAssociate ProfessorOld Dominion UniversityNorfolk, Virginia
Carol Reece, DNP, APRN Assistant Professor, NursingAshland UniversityAshland, Ohio
LuAnn Reif, PhD, RNProfessor, NursingCollege of St. Benedict/St. John’s
UniversitySt. Joseph, Minnesota
Monique Rogers-Walker, PhD, RNAssociate Senior ProfessorBenjamin León
School of NursingMiami Dade CollegeMiami, Florida

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
Michelle Romano, EdD (c), MS, RNC-OB
Former Director of Membership and Constitute Affairs
National Student Nurses’ AssociationBrooklyn, New York
Carolyn M. Rutledge, PhD, FNP-BCProfessorDirector, Doctor of Nursing Practice
(DNP) ProgramOld Dominion UniversityNorfolk, Virginia
Eda Ozkara San, MBA, RNPhD student at The City University
of New York (CUNY) Graduate Center
New York, New YorkPart-Time Clinical Instructor, NursingNew York UniversityNew York, New YorkPart-Time Clinical Instructor, NursingPace UniversityNew York, New York
Pavlos Sarafis, MSc, MPH, MHA, PhD, RN
Lecturer, NursingTechnological Educational Institution
of Thessalia Lamia, Greece
Lynn Schmidt, PhD, RNAssociate Dean, NursingAnderson UniversityAnderson, Indiana
Sharon See, MSN, RNCClinical Assistant Professor, NursingAshland UniversityAshland, Ohio
Joanne K. Singleton, PhD, RN, FNP-BC, FNAP, FNYAM
ProfessorDoctor of Nursing Practice Program
Director 2007-2015
Department of Graduate StudiesLienhard School of NursingPace UniversityWestchester and New York, New York
Jason T. Slyer, DNP, RN, FNP-BCClinical Assistant ProfessorDoctor of Nursing Practice Program
DirectorLienhard School of NursingPace UniversityWestchester and New York, New York
Ayla Baylk Temel, PhD, RNProfessor of NursingEge University Nursing FacultyCommunity Health Nursing
DepartmentIzmir, Turkey
Jeanette Velez, MA, CDPAdministrative Program Manager/
Physician LiaisonHuron, a Cleveland Clinic HospitalEast Cleveland, Ohio
Lynn Wiles, PhD, RN, CENAssistant ProfessorDirector of Technology and
SimulationSchool of NursingOld Dominion UniversityNorfolk, Virginia
Judy Xiao, MA, MSAssociate ProfessorInstruction/Reference LibrarianLibraryThe City University of New York
(CUNY) College of Staten IslandStaten Island, New York
Lisa Young, DNP, APRNAssistant Professor, NursingAshland UniversityAshland, Ohio
xiv CONTRIBUTORS

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
xv
Preparing nurses and other health professionals to provide quality health care in the increasingly multicultural and global society of the 21st century requires a comprehensive approach that emphasizes cultural competence education throughout professional education and professional life. Nurses and other health care providers, educators, administrators, professional association leaders, man-agers, and researchers are called upon to do the following:
• Provide optimal care for the large number of culturally diverse patient populations
• Implement cultural competence education strategies in academic and hospital settings for diverse learners
• Evaluate outcomes of cultural competence education• Prevent multicultural workplace conflict and promote multicultural work-
place harmony• Personally engage in lifelong cultural competence education
These tasks can seem daunting and overwhelming without appropriate resources. If you want to develop optimal cultural competence in yourself and oth-ers, Teaching Cultural Competence in Nursing and Health Care, Third Edition, and the Cultural Competence Education Resource Toolkit, Third Edition, are the how-to resources for you. Content from the toolkit is available to readers of the book, and can be requested at www.springerpub.com/cctoolkit. Those interested in using the toolkit for research and other purposes can purchase a license at this same url. These hands-on, user-friendly resources reveal a systematic seven-step approach that takes nurses, educators, administrators, professional association leaders, managers, educators, students, and other health care providers from their own starting points toward the pinnacle—optimal cultural competence. Appropri-ate for all levels and settings (academic, health care institutions, employee educa-tion, professional associations, and continuing education), the book and toolkit end the struggle to find ready-to-use materials for planning, implementing, and evaluating cultural competence education strategies and programs.
New book features, information updates, new research findings, and expanded ready-to-apply strategies and exemplars are woven throughout all the chapters. All chapters begin with a thought-provoking meaningful quote followed by a realistic snapshot scenario that leads into the comprehensive and updated nar-rative text. Other enhanced third-edition book features include integrated reflection boxes interspersed strategically throughout the chapters, easy application action steps, toolkit resource boxes, end-of-chapter references, and discussion questions.
Preface

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
xvi PREFACE
Responding to readers’ requests for “more,” the third edition also includes separate and expanded chapters for curriculum (Chapter 7); face-to-face class-rooms, hybrid, and online courses (Chapter 8); and clinical settings, immersion experiences, service-learning, simulation, and nursing skills laboratory (Chapter 9). New research further supporting Jeffreys’s Cultural Competence and Confidence (CCC) model and its associated questionnaires is presented in a detailed, yet con-densed and easy-to-read format that meets the needs of novice and experienced researchers. Four updated chapters targeting health care institutions and profes-sional associations provide easy-to-apply examples, ideas, and evidence-based best practices for promoting multicultural workplace harmony and safety, enhancing cultural competence education, networking and pooling resources, assuming lead-ership for key current and future issues, and evaluating outcomes.
The new book and toolkit include:
• A model to guide cultural competence education• Questionnaires for measuring and evaluating learning and performance• A guide for identifying at-risk individuals and avoiding pitfalls• A wide selection of educational activities• Techniques for diverse learners• Chapters detailing employee orientation, in-services, and continuing education• Chapters detailing multidimensional strategies for undergraduates and graduates• Introductory snapshot scenarios, vignettes, case examples, illustrations, tables,
and assessment tools• Interactive assessment and planning tools• Professional association networking and partnership ideas• Abstracts and sample research reports from researchers evaluating strategies
Based on the results of several postdoctoral grant-funded studies, practical teach-ing experience with academically and culturally diverse learners across all levels, and multidisciplinary literature, the book and toolkit provide resources and a wealth of information for all user groups.
The book is divided into five parts: Part I, Getting Started; Part II, Tools for Assessment and Evaluation; Part III, Educational Activities for Easy Application: Academic Settings; Part IV, Educational Activities for Easy Application: Health Care Institutions; and Part V, Educational Activities for Easy Application: Profes-sional Associations, Partnerships, and Future Directions.
Part I is composed of three chapters filled with resources to help educators begin teaching cultural competence. Essential background information about the multidimensional process of teaching cultural competence offers a valuable guide for educators at all levels who are planning, implementing, and evaluating cultural competence education.
Educators and researchers are continually challenged to measure outcomes following educational interventions. Part II addresses this challenge by introduc-ing several quantitative questionnaires and assessment tools (to be found in the toolkit) and discussing implementation and data interpretation strategies in a
This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
PREFACE xvii
detailed, user-friendly approach that can be easily adapted by novice and ad-vanced researchers. Questionnaires, assessment and planning tools, a cultural competence documentation log, and a research report template are easily ac-cessed in the accompanying Cultural Competence Education Resource Toolkit (Third Edition). (See details concerning toolkit access in the final section of the Preface.)
Parts III, IV, and V offer a wide selection of educational activities that can easily be applied by educators everywhere. Three chapters (7, 13, and 16) provide a general overview and a menu of activities for use in three areas: the academic setting, the health care institution, and professional associations. Chapter dis-cussions, supplementary diagrams, and descriptions of toolkit items explore the seven steps essential for optimal cultural competence development. These are:
• Self-assessment• Active promotion• Systematic inquiry• Decisive action• Innovation• Measurement• Evaluation
Five chapters (10, 11, 12, 14, and 15) creatively link strategies via detailed case exemplars that spotlight various populations and settings.
The book’s final chapter (Chapter 17) presents important implications for educators everywhere. Educators are challenged to commit to a focused and transformational change that will not only advance the science and art of cultural competence education, but will also result in culturally congruent care, ultimately benefiting health care consumers worldwide. The urgent expansion of educational research specifically focused on the teaching and learning of optimal cultural com-petence is emphasized, and areas for further inquiry and research, as well as future goals, are proposed. Extensive references are provided at the end of each chapter. An appendix lists over 50 studies involving Jeffreys’s Transcultural Self-Efficacy Tool (TSET) and/or Jeffreys’s CCC model.
Unquestionably, implementing creative, evidence-based educational activities, which promote positive cultural competence learning outcomes for culturally diverse students and health care professionals, continues to be a challenge. A greater challenge is to reach beyond competence (a minimum expectation) toward optimal cultural competence. This quest recognizes that all individuals, groups, and organizations have the potential for “more.” Optimal cultural competence embraces the “diversity of diversity,” requires ongoing ac-tive learning, fosters multicultural workplace harmony, and promotes the deliv-ery of the highest level of culturally congruent patient care.
Why optimal cultural competence?First, culture is a crucial factor in promoting wellness, preventing illness, re-
storing health, facilitating coping, and enhancing quality of life for all individuals, families, and communities. Unfortunately, the two main goals of the U.S. Depart-ment of Health and Human Services report Healthy People 2010 have not been met. The first goal—to increase quality and years of healthy life for all—can only be achieved when an examination of “quality of life” and the meaning of “health

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
and well-being” within a cultural context are put into service. The second goal was to eliminate health disparities among different segments of the population, which necessitated culture-specific and competent actions designed to eliminate dispari-ties; however, health disparities remain overwhelming within the United States and globally. As such, customized health care that responds to a client’s cultural values, beliefs, and traditions (culturally congruent care) remains an urgent need. For health care professionals with some cultural competence skills, the challenge now is to go beyond minimal expectations toward optimal cultural competence. It is also imperative that health professionals without cultural competence education actively begin their journey to develop optimal cultural competence.
Second, culturally congruent health care is a basic human right, not a privi-lege, and therefore every human is entitled to it. The International Council of Nurses, Code for Nurses (1), the American Nurses Association (ANA) Code of Ethics (2), and the National Standards for Culturally and Linguistically Appropriate Services in Health Care (3) are important documents that serve as reminders of this. Cri-teria devised by accreditation and credentialing agencies such as the Joint Com-mission on Accreditation of Healthcare Organizations, the National Committee on Quality Assurance, the American Medical Association, the Accreditation Commission for the Education of Nursing, and the Commission on Collegiate Nursing Education strive to ensure that culturally competent health care series and education are provided. The essential inclusion of cultural competence as viewed from an ethical and legal standpoint is addressed at varying levels within the disciplines of nursing, medicine, physical therapy, occupational therapy, speech-language pathology, dentistry, psychology, and social work. Not only are nurses, physicians, other health care providers, and institutions ethically and morally obligated to provide the best culturally congruent care possible (optimal cultural competence), they are also legally mandated to do so. Within the scope of professional practice, nurses and other health professionals are expected to actively seek out ways to promote culturally congruent care at optimal levels.
The AJN award-winning first edition of Teaching Cultural Competence in Nursing and Health Care introduced readers to easy-to-use teaching-learning strategies for cultural competence education. Positive comments about the first edition, along with a surge of requests for “more” from academic and employee educators, researchers, practicing health professionals, and students from around the world and in various disciplines, inspired the writing of the expanded sec-ond edition and the creation of the Cultural Competence Education Resource Toolkit.
Why a third edition? First, positive comments about the second edition and the toolkit, combined with an outpouring of completed studies and educational innovations utilizing the book’s and toolkit’s educational resources, strategies, model, questionnaires, and assessment tools, led to a realization that the body of evidence concerning the quality of the TSET and CCC model grew substantially and warranted swift dissemination. Second, ongoing requests for “more” from researchers and educators amidst a rapidly changing world urged the need for a third edition. Third, the positive feedback concerning the new interactive book features introduced to the latest edition of my other book, Nursing Student Reten-tion: Understanding the Process and Making a Difference, convinced me that these new features, if applied to Teaching Cultural Competence in Nursing and Health
xviii PREFACE

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
Care: Inquiry, Action, and Innovation, would make a tremendous difference in cap-turing interest, evoking awareness, and infusing active engagement activities, leading to deeper levels of learning, commitment, and creativity in a variety of ways among diverse readers and learners. The ideas and suggestions presented here are not meant to be exhaustive, but are offered to stimulate new ideas and invite health professionals to explore new paths on the journey to developing cultural competence in themselves and in others. Readers are encouraged to pause, reflect, and question throughout the book in order to gain new insights and perspectives. Everyone is empowered to contribute to a transformational change in health care that prioritizes optimal cultural competence development and embraces diversity.
KEY FEATURES AND HOW TO BEST USE THIS BOOKThis book and toolkit offer an ensemble of thoughtfully interconnected features in a lively, interactive, and informative fashion. Optimal benefits will be best achieved by using all the distinctive features together. A quick guide to readers on distinctive features and how to best use this book follows:
Opening Quotation: Readers are asked to pause and reflect on the quotation. Later, after completing the chapter, readers are asked to reflect on the quo-tation again. What does it mean? How is it significant?
Snapshot Scenario: A realistic scenario prompts readers to read on and discover what the multidisciplinary literature says about the issue and what solutions are available. Readers are asked to reflect on the scenario before proceeding into the chapter. What are the major points? What new information do you seek?
Chapter Content: Each chapter provides a wealth of new information and evidence-based strategies reported in the nursing and higher education lit-erature; readers can ease into and experience the abundance of literature without feeling overwhelmed. Integrated reflection exercise boxes strategi-cally placed throughout each chapter will aid in retaining important ideas and perspectives.
Key Point Summary: This recap highlights three to five key summary synthesis points within the chapter.
Easy Application Action Steps: This feature lists quick, easy steps for immediate application in any setting.
Educator-in-Action Vignette: This scenario synthesizes chapter information and demonstrates its direct application via realistic case exemplars.
Toolkit Resource Box: This list suggests toolkit items for use from the Cultural Competence Education Resource Toolkit that are most applicable to chapter content areas. (See more detailed information about the toolkit in the Pref-ace sections that follow.)
Discussion Questions: An assemblage of questions that creatively blends chap-ter features and content in order to heighten awareness, deepen commit-ment, stimulate new ideas, and apply knowledge are found throughout all chapters. Readers are asked to answer each question individually and substantiate their answer from readings and activities in the book. Readers
PREFACE xix
This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
can then proceed to discuss questions and answers with a small group of peers, faculty, and/or administrators.
References: Extensive journal, book, web, and other references document rel-evant resources.
ABOUT THE CULTURAL COMPETENCE EDUCATION RESOURCE TOOLKITThe Cultural Competence Education Resource Toolkit contains a wealth of hands-on, user-friendly resources for nurses, physicians, other health care pro-viders, educators, administrators, professional association leaders, managers, and students in health professions.
Content from the toolkit is available to readers of the book, and can be requested at www.springerpub.com/cctoolkit. Those interested in using the tool-kit for research and other purposes can purchase a license at this same url.
Toolkit items correspond with the seven essential steps for optimal cul-tural competence development: (1) self-assessment; (2) active promotion; (3) systematic inquiry; (4) decisive action; (5) innovation; (6) measurement; and (7) evaluation.
The 23 toolkit items are organized into three parts:
• Part 1: Questionnaires and Research Resources (12 items)• Part 2: Model and Illustrated Pathway (2 items)• Part 3: Educational Assessment and Planning Tools (9 items)
INFORMATION FOR READERSPurchasers of this book are encouraged to read the Cultural Competence Educa-tion Resource Toolkit, Third Edition, in conjunction with reading the book. Each chapter contains a Toolkit Resource Box that lists the toolkit items most relevant for the chapter. Readers may learn about licensing, permission, and accessing the toolkit at http://www.springerpub.com/cctoolkit.
APPLIED PURPOSES BEYOND READING: RESEARCH, TEACHING, CONFERENCES, AND MORE (PERMISSION LICENSE REQUIRED)Appropriate for all levels and settings (academic, health care institutions, employee education, professional associations, and continuing education), the book and toolkit end the struggle to find evidence-based, comprehensive, ready-to-use materials for planning, implementing, and evaluating cultural compe-tence education strategies and programs. These resources will be of benefit to a broad range of audiences at all levels: researchers, educators, administrators, nurses, physicians, other health care providers, association leaders, managers, and students in health professions. Consistently high positive feedback and the numerous publications and presentations resulting from researchers, educators, and students worldwide who already chose to apply various combinations of the
xx PREFACE

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
Cultural Competence Education Resource Toolkit items in a variety of settings and health care disciplines demonstrate the toolkit’s empirical and practical signifi-cance in contributing to cultural competence development. (See examples in this book [e.g., select exhibits, application strategies, vignettes, snapshot scenarios, etc.]; additional examples may be found by reading research studies listed in the book’s appendix and the literature.)
REFERENCES1. International Council of Nurses. (1973). Code for nurses. Geneva, Switzerland: Author.2. American Nurses Association. (2013). Code of ethics interpretive statements. Washing-
ton, DC: Author.3. Office of Minority Health. (2013). National standards for culturally and linguistically
appropriate services in health care: A blueprint for enhancing and sustaining CLAS policy and practice. Washington, DC: U.S. Department of Health and Human Services.
PREFACE xxi

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
1
PA R T I
Getting Started
Part I, Getting Started, contains three chapters filled with resources and tools to help educators begin teaching cultural competence. Possessing essential back-ground information about the multidimensional process of teaching cultural competence is immensely valuable for educators at all levels when planning, implementing, and evaluating cultural competence education.
Chapter 1 overviews key issues, concerns, and new challenges facing health care consumers, professionals, and educators. Professional goals, societal needs, ethical considerations, legal issues, changing demographics, and learner characteristics are highlighted. Select cultural values and beliefs are vividly compared and contrasted in a supplementary table that enhances the text. The chapter concludes with a discussion of factors influencing cultural competence development among culturally diverse learners and proposes that confidence, or in the context of this book, transcultural self-efficacy (TSE), is a major com-ponent in cultural competence development and a strong influencing factor in achieving culturally congruent care.
Creating environments that embrace diversity, meeting the culture-specific needs of patients, preventing multicultural workplace conflict, and promoting multicultural workplace harmony are portrayed in Chapter 2. These endeavors begin with diversity awareness of self and others, with each defined at the beginning of the chapter. Several poignant clinical and workplace ex-amples illustrate the significance of actively weaving in cultural competence throughout all aspects of health care settings. The acronym COMPETENCE assists health care professionals in remembering essential elements for optimal cultural competence development. A new section, “Creating a Cultural Safe Practice Environment: Patient and Visitor Roles” presents new ideas and issues to consider for multicultural workplace safety.
Chapter 3 presents a model to guide cultural competence education—the Cultural Competence and Confidence (CCC) model. The underlying assump-tions, principles, concepts, and terms associated with the model’s development are concisely presented. A unique feature of the model (and the book) is that its major concepts, propositions, and constructs are supported by quantitative studies using a questionnaire also discussed in this book and available in the

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
2 I GETTING STARTED
Jeffreys Cultural Competence Education Resource Toolkit, Third Edition (Jeffreys, 2016). Findings from multimethod and qualitative studies also support the underlying model. (Over 50 studies utilizing the CCC model and/or its associ-ated Transcultural Self-Efficacy Tool [TSET] are listed in the book’s appendix.) The newly revised illustration of the model enhances understanding of the text. Optimal cultural competence is at the core (core value or goal) and has been added as a visible reminder of its significance. The seven steps in the process of developing optimal cultural competence are introduced: (1) self-assessment, (2) active promotion, (3) systematic inquiry, (4) decisive action, (5) innovation, (6) measurement, and (7) evaluation. A corresponding graphic diagram depicts continual movement, development, and interaction between all steps signifying ongoing inquiry, action, and innovation. A close-up illustration expands on the CCC model illustration by tracing the proposed influences of TSE (confidence) on a learner’s actions, performance, and persistence for learning associated with cultural competency development and culturally congruent care.
The CCC model has relevance to other disciplines through recognizing the essential inclusion of cultural competence within clinical practice and in initial and/or ongoing educational preparation, such as medicine, physical therapy, occupational therapy, speech-language pathology, dentistry, psychol-ogy, and social work. The introductory Snapshot Scenario depicts the need and relevance of an evidence-based model in the quest to prepare culturally competent health professionals equipped to meet the changing needs of diverse populations. The model is brought to life through a realistic Educator-in-Action vignette featuring cultural competence education in the health care institution (hospital setting).
This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
3
O N E
Overview of Key Issues and Concerns
with contributions from Kevin Antoine
Educators everywhere are challenged to learn how to lead the quest for culturally congruent health care by implementing creative, evidence-based educational activities that promote positive cultural competence learning outcomes for diverse students and health care professionals, aiming to reach beyond minimal competence to the achievement of optimal cultural competence.
SNAPSHOT SCENARIO
Carrie: I want to provide the best care possible to my patients. This goal has be-come increasingly challenging in such a rapidly changing world.
Hope: I hope I’m meeting the needs of my patients and their families. The patient population is becoming so much more diverse.
Minnie: It’s so overwhelming with all the changes in the health care system, glo-balization, new and different patient populations, and complex diseases. I try to give the standard care to everyone and that just has to be good enough. Meeting even the minimum requirements is challenging. I can’t do anything extra special.
Justine: Social justice demands cultural competence. Without culturally congru-ent care, disparities in health and health care will continue to exist. Cultural competence is a right, not a privilege. Therefore, culturally congruent care is not special; it’s an expectation. It’s part of quality and safety for every patient.
Maxwell: I agree. “Good enough” is just not good enough. Health care profession-als should strive for developing optimal cultural competence. Everyone deserves the best. Would you want a minimum standard of care for yourself or for a loved one? Or would you opt for and expect optimal care?
Ernesto: I really want to provide high quality care that incorporates culture but I’m not at all sure about how to begin.

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
4 I GETTING STARTED
Desiree: I also desire to make a positive difference in health care through develop-ing optimal cultural competence, but I’m not confident that I know key issues, obstacles, or solutions.
Barry: There are lots of barriers towards developing culturally competent health professionals. One of the biggest barriers is a lack of diversity within the profes-sional workforce and academia.
Rainbow: I was raised to appreciate all types of diversity, so valuing diversity in the workforce is very important to me. I’m not confident about my role as a new graduate nurse or about how to shine amid the clouds of uncertainty and evolve from novice to expert. It’s all a new process.
Waldo: Who knows where I am in this process of developing cultural compe-tence? I feel lost and alone in this, even though I’m always surrounded by many people (including other nurses) representing a “diversity of diversity.”
Dora: I think we could all benefit from exploring key issues, searching for an-swers, and discovering what resources are available to help us on this journey of self-discovery and learning.
Bob: Part of our discovery should be utilizing valid tools and toolkits effectively in a complementary and scaffold fashion in order to build a strong foundation that will support and sustain future growth and expansion toward optimal cul-tural competence.
Wanda: What are some key issues and topics? What resources are available? Where should I start? How can I become more confident in providing culturally congruent care and meeting the needs of diverse patients?
Meeting the health care needs of culturally diverse clients has become even more challenging and complex. In addition to acknowledging the cultural evolu-tion (growth and change) occurring in the United States (and other parts of the world), it is imperative that nursing and other health care professions appreciate and understand the impending cultural revolution. The term cultural revolution implies a “revolution of thinking” that seeks to embrace the evolution of a differ-ent, broader worldview (1). Both cultural evolution and cultural revolution have the potential to bring about a different worldview regarding cultural care and caring by including key issues previously nonexistent, underrepresented, or in-visible in nursing and health care literature. This new vision challenges all health care professionals to embark upon a new journey in the quest for cultural com-petence and culturally congruent care for all clients (1). This new journey also challenges health care professionals and organizations to go beyond the goal of achieving “competence” (minimum standard) toward the goal of achieving “op-timal” cultural competence (standard of excellence). Educators everywhere are additionally challenged to learn how to lead the quest for culturally congruent health care by implementing creative, evidence-based educational activities that

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
1 OVERVIEW OF KEY ISSUES AND CONCERNS 5
promote positive cultural competence learning outcomes for culturally diverse students and health care professionals who are aiming to reach beyond minimal competence to the achievement of optimal cultural competence.
This transformational journey begins by seeking to understand the key is-sues, concerns, and new challenges facing health care consumers and profession-als today and in the future. This chapter evokes professional awareness, sparks interest, stimulates revolutionary thought, highlights vital information, and shares new ideas concerning the health care needs of culturally diverse clients and the development of cultural competence among culturally diverse health care pro-fessionals. Cultural competence has been described as a multidimensional process that aims to achieve culturally congruent health care (1–8). Culturally congruent health care refers to health care that is customized to fit with the client’s cultural values, beliefs, traditions, practices, and lifestyle (4). It is beyond the scope of this chapter to provide a summary review of the existing literature concerning cultural competence and health care. Rather, this chapter emphasizes select points from the literature, identifies future complexities and challenges in health care, dis-cusses factors influencing cultural competency development, and proposes a con-struct involved in the process of cultural competence development and education.
COMPLEXITIES, CHANGES, AND CHALLENGES IN HEALTH CARERapid increase in global migration, changes in demographic patterns, varying fertility rates, increased numbers of multiracial and multiethnic individuals, and advanced technology contribute to cultural evolution. For the purpose of this book, cultural evolution refers to the process of cultural growth and change within a society (1). In the existing nursing literature, cultural growth, change, and the need for culturally congruent nursing care has been reported across the world. Although this book features cultural changes in the United States, readers should recognize that globalization is a worldwide phenomenon, with populations now moving more frequently than ever before. Because more people are migrating to several different places, the acculturation experience may include cultural values and beliefs (CVB) assimilated from more than one source, resulting in new ways of expressing traditional CVB and/or resulting in new cultural values and be-lief patterns. Consequently, health care professionals are challenged to meet the needs of changing societies in new and different ways.
The U.S. Census Bureau (9) and Healthy People 2020 (10) provide valuable data about select population characteristics; however, they are limited to provid-ing information about cultural values, beliefs, behaviors, and practices associ-ated with the many diverse cultural groups existing within the United States.
What do you already know about cultural competence and health care? What do you seek to learn about cultural competence and health care? What are some key issues that contribute to complexities, changes, and challenges in health care?

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
6 I GETTING STARTED
For example, it is helpful to know that minority populations are increasing more rapidly than White, non-Hispanic, nonimmigrant populations (as determined by such variables as age and fertility rates), further justifying and demanding in-creased population-specific resource allocation (11–16). It is also crucial to have identified health disparities, high priority areas, goals, and proposed strategies for improvement; however, nurses and other health care professionals must be-come actively aware of the diverse cultural groups comprising each designated minority category if Healthy People 2020 goals (and beyond) are to be met (8, 12, 13, 17, 18). For example, the “Hispanic” category may include individuals whose heritage may be traced to Cuba, Nicaragua, Mexico, Puerto Rico, Peru, Spain, and/or other countries, each also representing much diversity within and be-tween groups. Diversity may exist based on birthplace, citizenship status, reason for migration, migration history, food, religion, ethnicity, race, language, kinship and family networks, educational background and opportunities, employment skills and opportunities, lifestyle, gender, sexual orientation, socioeconomic sta-tus (class), politics, past discrimination and bias experiences, health status and health risk, age, insurance coverage, and other variables that go well beyond the restrictive labels of a few ethnic and/or racial groups. The diversity of diversity recognizes that culture is more than just “labels” and necessitates individualized appraisal to incorporate culturally congruent care and achieve optimal outcomes.
The projected increase of multiracial and multiethnic (multiple heritage) individuals in the United States (19–27) and throughout the world demonstrates a growing change in demographic patterns, adding to this new cultural evolu-tion. Forced single category choices and/or the “other” category make the unique culture of the multiracial and multiethnic individual invisible (1, 28, 29). In the 2000 U.S. Census, 6,826,228 individuals identified as being of more than one race (9), and by 2050 it is estimated that one in five Americans will identify as being multiracial (30). Although the 2000 U.S. Census permitted individuals to select more than one racial/ethnic category, the lateness of this option demonstrates the reluctance of society to acknowledge and appreciate the existence of mestizo (mixing) in the United States (31). The late repeal of the last laws against misce-genation (race mixing) in the 1970s attests not only to societal reluctance, but also to political resistance reflecting the racial ideologies of some White Americans (32). Current politics and policies have not kept pace with changing demograph-ics and raise questions about attitudes toward multiracial people, prevalence of anti-discrimination policies directed at individuals who identify with a single race, and other disparities that keep multiracial and multiple heritage individu-als “invisible” (26, 27, 29, 33, 34).
Inconsistent use of data from individuals selecting more than one census category is confusing and typically favors the antiquated process of assigning individuals to one category only; usually the minority status or politically ad-vantageous category is selected. For example, when reporting the number of “minority” individuals within a public school system for the purpose of dem-onstrating integration within a predominantly White school, someone selecting “Black” and “White” would be assigned as being “Black.” In reality, it may be impossible for a multiethnic and/or multiracial individual to choose one ethnic or racial identity over the other (25, 34–36). Multiple heritage identity can include

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
1 OVERVIEW OF KEY ISSUES AND CONCERNS 7
membership within one select group, simultaneous membership in two or more distinct groups, synthesis (blending) of cultures, and/or fluid identities with different groups that change with time, circumstance, and setting (24, 25, 37–39). Moreover, multiple heritage individuals often describe being “multiracial” or “multiethnic” as a separate and unique culture (24–26, 34, 39). Culturally con-gruent care must begin by openly acknowledging the uniqueness of multiple heritage individuals and seeking to learn about their lived experience. Multiple heritage individuals present unique concerns and challenges for transcultural nurses, other health care professionals, and educators because of little related research and few published studies in nursing and health care (1, 25–29, 34).
Similarly, other underrepresented, invisible, unpopular, or new issues pres-ent complexities and challenges to health care professionals because of the lack of substantive research, resources, and expertise specifically targeting such topics related to culture and changing populations (cultural evolution). With the rapid changes and influx of new populations from around the world, nurses are, more than ever before, faced with the challenge of caring for many different cultural groups. Changes are occurring more rapidly in urban, suburban, and rural areas, often with cultural groups clustering together in ethnic neighborhoods. This means that there is less time for nurses to learn about and become accustomed to new cul-tural groups. Lack of nurses with transcultural nursing expertise presents a severe barrier in meeting the health care needs of diverse client populations (4–7, 40–42).
Political changes throughout the world have resulted in large migration waves from former socialist, communist, monarchal, and dictatorship nations. Too many choices (in health care planning options) may overwhelm individuals who are not used to such freedoms (43). Mismatches in expectations between health care professionals and clients can cause poor health outcomes, stress, and dissatisfac-tion. Nurses unfamiliar with various political systems and the potential impact on clients’ perceptions may be unprepared to provide culturally congruent care for these clients. Understanding the ethnohistory, especially the influence of politics, economics, discrimination, and intergroup and intragroup conflicts, is an important cultural dimension that warrants further attention (4–8, 13, 17–19, 43–46). Despite the commonality of national origin, cultural experiences may be quite different for persons seeking asylum, refugees, and immigrants, and may vary at different points in history, necessitating an accurate and individualized appraisal.
Health care professionals are also challenged to differentiate between nu-merous minority groups around the world (who may have been victims of overt and/or covert stereotyping, prejudice, discrimination, and racism) and domi-nant groups. Within the United States, it has been well documented that discrim-ination, stereotyping, prejudice, and racism has existed and continues to exist in nursing and health care (47–59). This unpopular topic has not gained the suffi-cient attention and action necessary to actively dismantle stereotyping, prejudice, discrimination, and racism. Raising awareness is insufficient; taking appropriate and definitive action through well-planned positive innovative interventions fol-lowed by evaluation strategies will help in moving beyond complacent “passive advocacy” to positive “active innovative advocacy.” Such innovative actions re-quire the development of cultural competence and sincere commitment on the part of health care professionals.

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
8 I GETTING STARTED
Groups referred to as “subcultures” have been identified as “vulnerable populations”; such populations present complex scenarios to health care pro-fessionals today and will continue to do so in the future (11–18, 46, 60, 61). For example, undocumented individuals, migrant workers, tenant farmers, and the homeless often present unique health care challenges due to lack of health in-surance, illiteracy, poverty, and fear. In addition, tenant farmers, migrant work-ers, and landowners of varying socioeconomic levels may be grouped together under the heading of “rural health”; thus, the truly unique culture(s) and needs within and between groups across various geographic regions may remain un-discovered. Because tenant farmers may receive food and housing as part of their wages, they may not be eligible for food stamps; Medicaid; Women, Infants, and Children (WIC) services; public assistance; or other social services. Employee benefits such as health insurance and dental insurance are usually nonexistent. Funds for clothing, soap, toothpaste, toothbrushes, and other toiletries may be scarce, making tenant farmers susceptible to preventable diseases. Geographic isolation and lack of transportation are barriers encountered within rural com-munities, thus presenting another barrier to health care access. Within the United States, health insurance diversity presents inconsistencies in health care, espe-cially in health promotion and illness prevention. Consequently, primary care for treatment of acute and advanced problems is not routinely accessible with delayed entry into the health care system occurring. Evaluating the short- and long-term effects of U.S. health care reform on access, quality, cost, health pro-motion, illness prevention, management of chronic illness, and life span for vul-nerable and/or marginalized populations will yield new information for future informed decision making (see Exhibit 1.1).
The global economic crisis, rising unemployment rates, loss of (or changes in) health insurance coverage, job and retirement uncertainty, increased housing foreclosures, and general economic unrest present multifaceted problems that political leaders, financial advisers, and the general public are poorly equipped to address effectively and with which they are inexperienced. Within a multicul-tural society, different CVB concerning economic stability, lifestyle expectations, and acceptance of charity, debt, and profit further complicate these problems. Stress associated with periods of economic uncertainty and doubt may present greater numbers of individuals seeking and/or needing mental health services and/or other health services for diseases often triggered or exacerbated by stress. Inability to pay for medical services, medications, housing, and food may aggravate health and social problems as well as intensify personal debt, thereby broaden-ing deficits in the overall economy. The global economic crisis has spurred the forced, rapid movement and lifestyle changes of individuals, families, and even whole communities.
Rapidly moving populations bring unfamiliar diseases, new diseases, treatments, and medicines, challenging health care professionals to become quickly proficient in accurate diagnosis, treatment, and prevention. For example, nurses unfamiliar with malaria may be suddenly faced with several refugees from Africa who require treatment for malaria. New diseases, reappearing or re-emerging “old” diseases, and/or new resistant strains of old diseases can cause epidemics if not identified early and then properly controlled. Medicines and

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
1 OVERVIEW OF KEY ISSUES AND CONCERNS 9
treatments considered “alternative” or “complementary” within the culture of Western medicine may actually be considered “routine” in other cultures. Med-icines considered “routine” within the culture of Western medicine may have varying and adverse effects on different ethnic or racial groups due to health beliefs and/or due to genetic differences in body processes (e. g., metabolism) and/or anatomical characteristics (e. g., sun absorption based on skin color). The growing new field of ethnopharmacology attests to the urgent need to investi-gate the pharmacokinetics, pharmacodynamics, and overall pharmacological ef-fects of drugs within specific cultural groups. Unfortunately, insurance company approval for a drug therapy regimen is often guided by drug studies among pri-marily homogeneous populations, rather than taking into account new, however sparse, empirical evidence provided by ethnopharmacological studies.
Inconsistencies in the expected roles of the nurse may vary from culture to culture, therefore confounding the therapeutic nurse-client interaction, nurse-nurse interaction, nurse-physician interaction, and nurse-family interaction. Differences in nursing practices throughout the world influence how the nurse views power, autonomy, collaboration, and clinical judgments (2, 4–8, 62–67). Whether the nurse is viewed as a well-educated professional, vocational ser-vice provider, paraprofessional, uneducated worker, or servant will greatly im-pact the therapeutic and working relationship (8, 67). Furthermore, whether the nurse is viewed as an outsider, “stranger,” “trusted friend,” or insider will sig-nificantly influence the nurse–client relationship, the achievement of culturally congruent care, and optimal health outcomes (5–7, 68). The mismatch between the diversity of registered nurses and U.S. populations presents one large bar-rier to meeting the needs of diverse populations. For example, White nurses of European American heritage represent approximately 83% of all registered nurses (69).
Expected roles and perceptions about other health care professionals will also vary from culture to culture, thus necessitating an accurate appraisal of cli-ents’ baseline knowledge, beliefs, and expectations, if culturally congruent care is to be achievable by the multidisciplinary health care team. Gender roles and expectations about members of the health care team are variable. Within certain cultures, it may be unacceptable (or less acceptable) for women to become physi-cians and provide care for male patients; conversely, it may be unacceptable (or less acceptable) for men to become nurses and provide care for female patients (67, 70). In some cultures there may not be a word or concept for “psychologist,” “psychiatrist,” “dietician,” “social worker,” “physical therapist,” “ occupational therapist,” “respiratory therapist,” or “recreational therapist,” thus presenting new challenges for health care professionals in Western society. For example, there is no word in Korean for psychologist or psychiatrist; mental illness re-mains highly stigmatized, with clients and families encountering great difficul-ties when mental illness occurs (71, 72). In some countries, nurses may be trained to perform radiologic procedures and physical therapy interventions (73). This broad diversity calls for students, nurses, the nursing profession, and other health care professionals to become active participants (and partners) in the pro-cess of developing cultural competence and actively seek and embrace a broad (even revolutionary) worldview of diversity.

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
10 I GETTING STARTED
ETHICAL AND LEGAL ISSUESCulturally congruent health care is a basic human right, not a privilege (4, 14–16, 74–81); therefore, every human should be entitled to culturally con-gruent care (see Exhibit 1.1). In addition, empirical findings clearly document the strong link between culturally congruent care and the achievement of posi-tive health outcomes. Increasing numbers of lawsuits with clients claiming that culturally appropriate care was not rendered by hospitals, physicians, nurses, and other health care providers attest to the complicated legal issues that may arise from culturally incongruent care. Furthermore, clients are often winning their cases in court (5). The International Council of Nurses’ Code for Nurses (76), the American Nurses Association’s Code of Ethics (74), and the National Standards for Culturally and Linguistically Appropriate Services in Health Care (80, 81) are several important documents that serve as direct reminders and provide guidance to health professionals. Not only are nurses and other health care providers ethically and morally obligated to provide the best culturally congruent care possible, but nurses and health care providers are also legally mandated to do so. Within the scope of professional practice, nurses and other health professionals are expected to actively seek out ways to promote cultur-ally congruent care as an essential part of professional practice. For example, the discipline of social work recognized that the “shifts in the ethnic composi-tion of American society in the coming 45 years . . . and the realities of racism, discrimination, and oppression combine to make cultural competence essential to effective social work practice, and thus to social work education” (82). The essential inclusion of cultural competence from an ethical and a legal stand-point is addressed at varying levels within the disciplines/fields of dentistry, medicine, occupational therapy, physical therapy, physician assistant, psychol-ogy, rehabilitative counseling, social work, and speech-language pathology (14, 15, 73, 83–100). The goal of including cultural competence necessitates a systematic, empirically supported action plan.
To “assist, support, facilitate, or enhance” culturally competent care, Leininger (4) proposed three modes for guiding nursing decisions and actions: (a) culture care preservation and/or maintenance; (b) culture care accommoda-tion and/or negotiation; and (c) culture care repatterning and/or restructuring that also have multidisciplinary relevance. Because culturally congruent care can only occur when culture care values, expressions, or patterns are known and used appropriately, a systematic, thorough cultural assessment is a neces-sary precursor to planning and implementing care (101). Assessing, planning, implementing, and evaluating culturally congruent care requires active, ongoing
Which topics or issues in the previous text presented you with the most new learning? Which topics and issues do you routinely consider within your current professional role? How will your new and/or expanded learning influence your future educational, research, networking, collaborative, and practice roles?

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
1 OVERVIEW OF KEY ISSUES AND CONCERNS 11
(continued)
EXHIBIT 1.1Tracing the Legal Right to Health Care, International
and U.S. Law, Changing Demographics, and Implications for Cultural Competence
Kevin Antoine, J.D.Assistant Vice President for Diversity & Inclusion
Assistant Professor of Health Law & PolicyState University of New York (SUNY) Downstate
Brooklyn, NY
More than 60 years ago, emerging from the end of World War II as the leader of the free world, the United States was the driving force in drafting the international treaties that would establish the United Nations (UN), the World Health Organiztion (WHO), and the Universal Declaration of Human Rights (UDHR). The United States ratified the constitution of the WHO, which recognized health care as a fundamen-tal right (1). The UN Charter and the UDHR also recognized a legal right to health care and advocated the involvement of many sectors of society in removing barriers to health care access and treatment (2).
In 1992, the United States also ratified the International Covenant on Civil and Political Rights (ICCPR), which established universal stan-dards for the protection of basic civil and political liberties and recog-nized a fundamental right to health care (3).
Ratification of an international treaty is the only act under the U.S. Constitution that gives an international treaty legal status in the United States. The U.S. Constitution requires that the Senate give its advice and consent with a two-thirds vote in favor of a treaty (4). A treaty becomes domestic law in the United States after the president ratifies it by signing it (5). Therefore, after the Senate’s advice and consent and ratification by the president, a treaty is equivalent to federal law.
Accordingly, under U.S. Constitutional law, these treaties—the UN Charter, the WHO Constitution, and the UDHR—have been the law in the United States since the 1940s, and the ICCP has been the law since 1992. Only under the last in time rule can a later enacted federal statute supersede a treaty subsequent to its ratification.
The last in time rule was established by the U.S. Supreme Court in the case of Ping v. U.S. (1889) (6). In 1858, the United States and China ratified a treaty addressing immigration between the two countries, granting reciprocal rights of unrestricted travel between them. In 1888, subsequent to the discovery of gold in California, the United States Con-gress enacted a federal statute severely limiting Chinese laborers from entering the United States, which violated the terms of the 1858 treaty.
This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
12 I GETTING STARTED
(continued)
EXHIBIT 1.1 (continued)
In upholding the federal statute, the U.S. Supreme Court held that a federal statute could supersede a treaty if enacted after ratification of the treaty, and a treaty could supersede a federal statute if ratified after the enactment of a federal statute. A ratified treaty becomes self-executing enforceable law (7). However, if the treaty requires the U.S. Congress to enact implementing legislation then the treaty is non-self executing (8). With respect to the UN Charter, the WHO Constitution, and the UDHR, there have been no later enacted federal statutes that repealed the United States’ ratification of these treaties. In addition, the UN Charter, the WHO Constitution, and the UDHR were self-executing treaties that required no implementing of U.S. congressional legislation. Therefore, arguably, Americans have had a right to health care since the late 1940s when the United States ratified the UN Charter, WHO Con-stitution, and the UDHR.
With the right to health care established as a fundamental right in the late 1940s, access and treatment to health care must comply with the U.S. Constitution’s equal protection clause of the Fourteenth Amend-ment (9). In addition, health care is a major commercial entity in the U.S. and as such is subject to regulation via the commerce clause of the U.S. Constitution. The commerce clause grants the U.S. Congress the author-ity to regulate commerce between the states, notwithstanding whether the suppliers of commerce are government or private commercial sup-pliers. For example, it is through the commerce clause that Title VII of the Civil Rights Act of 1964 allows federal agencies to sue both government and private employers for workplace discrimination. The shipping of goods and products, as well as engaging in commercial business across state lines, is interstate commerce that is subject to federal regulation via the commerce clause. Likewise, health care is a major commercial industry engaged in interstate commerce subject to federal regulation via the commerce clause.
The commerce clause can be used to ensure that the fundamental right of access and treatment to health care is not denied much in the same manner the commerce clause is used by civil rights laws to enforce federal nondiscrimination laws. This would ensure national uniformity in addressing fair access and treatment to health care.
The United States recognized a legal right to health care when it ratified the WHO’s Constitution, the UN Charter, and the Universal Declaration of Human Rights more than 60 years ago. Access to health care in the United States already is a fundamental right as an extension to the ratification of these treaties.
This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
1 OVERVIEW OF KEY ISSUES AND CONCERNS 13
(continued)
PATIENT PROTECTION AND AFFORDABLE CARE ACTIn 2010, the Patient Protection and Affordable Care Act, more com-monly cited as the Affordable Care Act (ACA), was signed into law in the United States. Goals of the ACA, include making health insurance affordable by expanding government and private insurance, lowering the uninsured health care rate, increasing health care quality, not deny-ing coverage based on pre-existing medical conditions, addressing non-discrimination in access and treatment of health care, improving patient demographic data collection and recording, improving the quality of care by addressing cultural and linguistic competence, and increasing diversity throughout the health care workforce.
Although the ACA offers additional coverage for many who previ-ously did not qualify for, or could not afford, medical coverage, the ACA still does not guarantee health care as a constitutional right. Instead, it mandates Americans to purchase health insurance from a private or government provider.
Several states challenged the ACA’s mandate that Americans had to purchase health insurance from a private or government provider. The U.S. Supreme Court ruled that the ACA is constitutional as a tax (mandating individuals to purchase health insurance or pay penalty tax). The irony is that Americans who are too poor to purchase health insurance will be fined the penalty tax which they probably will not be able to pay either, resulting in more government fines, penalties, or prosecution. Arguably, in some instances the ACA may hurt the same Americans it was designed to help. To date, the United States remains the lone industrialized nation without universal health care coverage.
ACA GOALS, CHANGING DEMOGRAPHICS, AND CULTURAL COMPETENCEThe Census Bureau projects a far more diverse population by 2060. Therefore, the goals of the ACA must necessarily keep pace with the changing demographics in the United States in the next 45 years. Several examples include population increases among Hispanics (56 million to 128 million); African Americans (41 million to 61 million); Asian Ameri-cans (15 million to 30 million); Native Americans and Alaska Natives (5.2 million to 11.2 million). Meanwhile, the non-Hispanic White population is the only population projected to shrink, decreasing by 20 million and accounting for 43% of the U.S. population (10). In addition, more than one in five Americans are projected to identify as being multiracial (11).
EXHIBIT 1.1 (continued)

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
14 I GETTING STARTED
(continued)
Presently, according to the Health Profession for Diversity Coalition, Hispanics, African Americans, and Native Americans only account for 9% of physicians, 7% of dentists, and 12% of nurses (12). As the nation’s general population becomes more diverse, there will be a correlation in the demographics of the patient populations. Therefore, addressing the cultural and linguistic competence of the health care workforce will be essential in order to improve the quality of health care provided to the increasingly diverse patient population. The ACA’s health care workforce provisions address both present and future needs of increasing diversity within both the health care workforce and the diverse patient population.
The ACA’s health care workforce provisions aim to increase diver-sity in the health care workforce and encompass all major health care professions and settings; these include but are not limited to: medicine, nursing, dentistry, physical therapy, emergency care, mental health, primary care, and public health. Pursuant to the ACA, the National Health Care Workforce Commission (the Commission) was established to provide data on the health care workforce. Although the Commission has yet to be funded by Congress, the framework is in place to pro-vide much needed information on the nation’s health care workforce. Additionally, the ACA’s federal workforce diversity grants were created to develop a culturally competent workforce through cultural compe-tence education within academic, employee, and continuing education settings. Targeted focus areas include provision of culturally congruent care with regard to patients’ religious and nonreligious preferences, di-etary habits, access to transportation, preferred language in discussing a patient’s medical condition, gender identity, sexual orientation, and end-of-life preferences.
A diverse health care workforce, educationally prepared to pro-vide culturally competent care to diverse patients, improves access to health care, increases patient satisfaction, and builds respect and trust between the patient and the health care professional (13). The cultural competency provisions and nondiscrimination provisions of the ACA and global health initiatives of the WHO offer the United States a new approach from a legal and constitutional perspective to address non-discrimination in access to health care and treatment, to improve the quality of care by addressing cultural and linguistic competence, and to increase diversity throughout the nation’s health care workforce.
Hopefully the ACA is laying the foundation for the United States to join the WHO and other industrialized nations in recognizing health care as a fundamental right.
EXHIBIT 1.1 (continued)

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
1 OVERVIEW OF KEY ISSUES AND CONCERNS 15
learning based on theoretical support and empirical evidence. The goal of cul-turally congruent care can only be achieved through the process of developing (learning and teaching) cultural competence (102, 103).
To what extent are ethical and legal guidelines concerning cultural competence influencing cultural competence education and practice within and across disciplines? What else can be done?
BARRIERSProfessional goals, societal needs, ethical considerations, and legal issues all declare the need to prioritize cultural competence development, necessitating a conscious, committed, and transformational change in current nursing practice, education, and research (104). Although nursing and other health care profes-sions can be transformed through the teaching of transcultural nursing (5–7, 40–42, 101, 105–107), two major barriers prevent a rapid effective transformation. One major barrier is the lack of faculty and advanced practice nurses formally trained in transcultural nursing and in the teaching of transcultural nursing (104–113). The second major barrier is the limited research evaluating the effec-tiveness of teaching interventions on the development of cultural competence (13–15, 42, 104, 110–117). These two barriers are further complicated by the
1. World Health Organization’s Constitution.2. Articles 55 and 56 of the UN Charter, Article 25 of the UDHR, Article 1 of the WHO Constitution.3. Jimmy Carter, U.S. Finally Ratifies Human Rights Covenant. The Carter Center (1992).4. Article 2 Section 2 of the U.S. Constitution.5. Article 6 of the U.S. Constitution.6. Ping v. US, 130 US 581 (1889).7. Martin, Schnably, Wilson, Simon, Tushnet. International Human Rights and Humani-tarian Law: Treaties, Cases and Analysis (2006).8. Ibid9. The laws of a state must treat an individual in the same manner as others in similar conditions and circumstances.10. U.S. Census Bureau and Center for Diseases Control and Prevention.11. Farley, R. (2001). Identifying with multiple races. Report 01-491. Ann Arbor, MI: Uni-versity of Michigan, Population Studies Center. (As cited in Shih, M., & Sanchez, D. T. (2009). When race becomes even more complex: Toward understanding the landscape of multiracial identity and experiences. Journal of Social Issues, 65(1), 2.) 12. U.S. Census Bureau, Census 2000 Special Equal Employment Opportunity (EEO) Tabulation. 13. American Medical Student Association. Enriching Medicine Through Diversity (2015).
EXHIBIT 1.1 (continued)

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
16 I GETTING STARTED
(a) changing demographics of students and health care professionals and (b) se-vere shortages of nurses and nursing faculty. Other health professions have also acknowledged the lack of diversity within their respective fields, as well as the lack of faculty prepared to incorporate substantive cultural competence education within professional education as severe barriers to effective transformation (84–94, 96–99, 118). Several of these factors are highlighted in the following sections.
Parts III, IV, and V of this book present action strategies, innovations, and practical examples for cultural competence education and evaluation aimed at overcoming barriers and invigorating an effective transformation that reaches beyond “minimal” competence to “optimal” cultural competence. The goal of optimal cultural competence recognizes that cultural competence is not an end product, but an ongoing developmental process; therefore, individuals, groups, and organizations can continually “improve,” striving for “peak performance” outcomes or standards of excellence. Steps essential for optimal cultural com-petence development include: self-assessment, active promotion, systematic in-quiry, decisive action, innovation, measurement, and evaluation. These seven steps are integrated throughout Parts III, IV, and V of this book and the accom-panying toolkit (119).
What are the demographic characteristics within your current work setting? To what extent is the diversity of diversity representative of local neighborhoods, nearby regions, and national demographics? (Note: The diversity of diversity recognizes that diversity may exist based on birthplace, citizenship status, reason for migration, migration history, food, religion, ethnicity, race, language, kinship and family networks, educational background and opportunities, employment skills and opportunities, lifestyle, gender, sexual orientation, socioeconomic status (class), politics, past discrimination and bias experiences, health status and health risk, age, insurance coverage, and other variables that go well beyond the restrictive labels of a few ethnic and/or racial groups.) What impact does/could the match or mismatch of varying demographic characteristics make on the development of and the provision of cultural competence in health care? What suggestions or ideas do you propose?
CHANGING DEMOGRAPHICS OF STUDENTS AND HEALTH CARE PROFESSIONALSThe projected increase in immigration, globalization, and minority population growth has the potential to enrich the diversity of the nursing profession and to help meet the needs of an expanding culturally diverse society (8, 13–17, 49–59, 111, 113, 120–130). What has actually occurred is that the dramatic shift in de-mographics, the restructured workforce, and a less academically prepared col-lege applicant pool have created a more diverse nursing applicant pool. Nursing students today represent greater diversity in age, ethnicity and race, gender, pri-mary language, prior educational experience, family’s educational background, prior work experience, and enrollment status than ever before (59, 129–133).
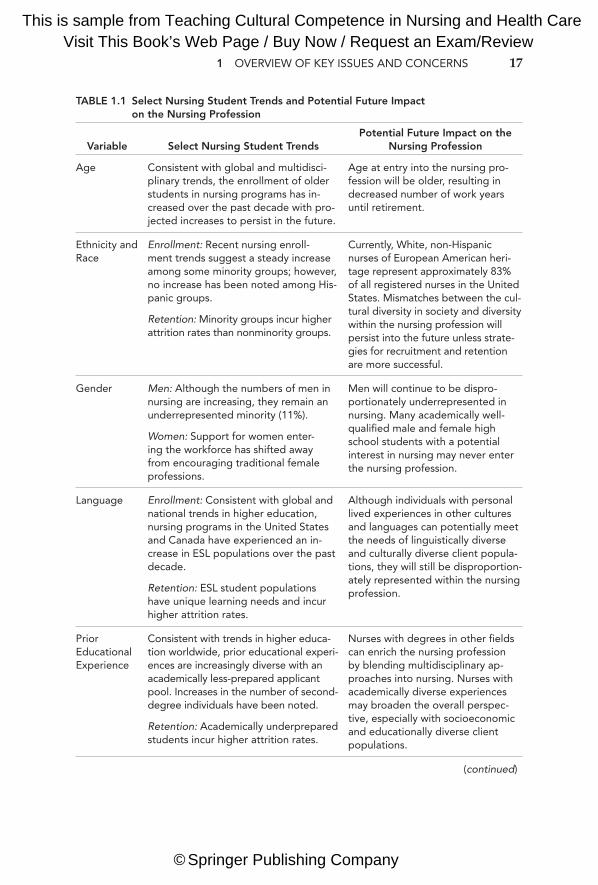
This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
1 OVERVIEW OF KEY ISSUES AND CONCERNS 17
(continued)
TABLE 1.1 Select Nursing Student Trends and Potential Future Impact on the Nursing Profession
Variable Select Nursing Student TrendsPotential Future Impact on the
Nursing Profession
Age Consistent with global and multidisci-plinary trends, the enrollment of older students in nursing programs has in-creased over the past decade with pro-jected increases to persist in the future.
Age at entry into the nursing pro-fession will be older, resulting in decreased number of work years until retirement.
Ethnicity and Race
Enrollment: Recent nursing enroll-ment trends suggest a steady increase among some minority groups; however, no increase has been noted among His-panic groups.
Retention: Minority groups incur higher attrition rates than nonminority groups.
Currently, White, non-Hispanic nurses of European American heri-tage represent approximately 83% of all registered nurses in the United States. Mismatches between the cul-tural diversity in society and diversity within the nursing profession will persist into the future unless strate-gies for recruitment and retention are more successful.
Gender Men: Although the numbers of men in nursing are increasing, they remain an underrepresented minority (11%).
Women: Support for women enter-ing the workforce has shifted away from encouraging traditional female professions.
Men will continue to be dispro-portionately underrepresented in nursing. Many academically well-qualified male and female high school students with a potential interest in nursing may never enter the nursing profession.
Language Enrollment: Consistent with global and national trends in higher education, nursing programs in the United States and Canada have experienced an in-crease in ESL populations over the past decade.
Retention: ESL student populations have unique learning needs and incur higher attrition rates.
Although individuals with personal lived experiences in other cultures and languages can potentially meet the needs of linguistically diverse and culturally diverse client popula-tions, they will still be disproportion-ately represented within the nursing profession.
Prior Educational Experience
Consistent with trends in higher educa-tion worldwide, prior educational experi-ences are increasingly diverse with an academically less-prepared applicant pool. Increases in the number of second-degree individuals have been noted.
Retention: Academically underprepared students incur higher attrition rates.
Nurses with degrees in other fields can enrich the nursing profession by blending multidisciplinary ap-proaches into nursing. Nurses with academically diverse experiences may broaden the overall perspec-tive, especially with socioeconomic and educationally diverse client populations.
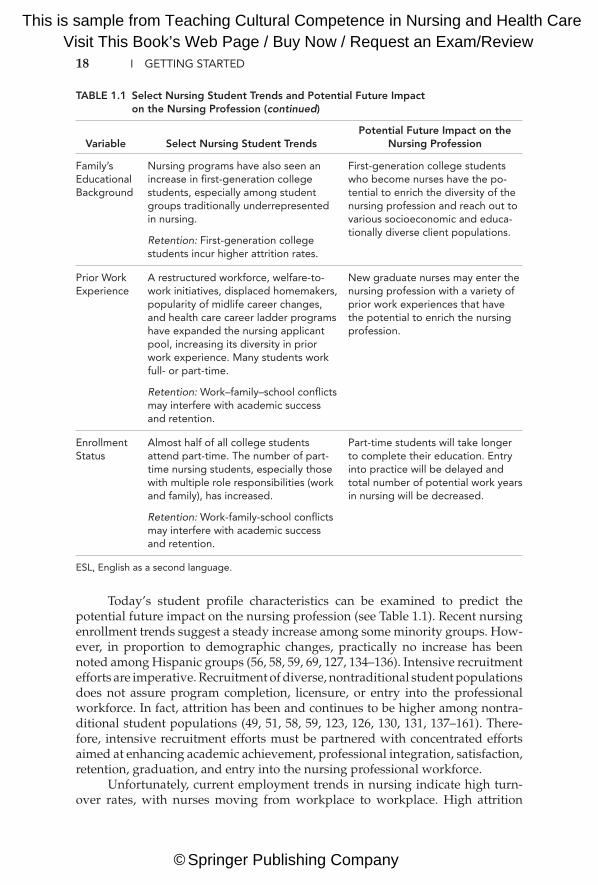
This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
18 I GETTING STARTED
TABLE 1.1 Select Nursing Student Trends and Potential Future Impact on the Nursing Profession (continued)
Family’s Educational Background
Nursing programs have also seen an increase in first-generation college students, especially among student groups traditionally underrepresented in nursing.
Retention: First-generation college students incur higher attrition rates.
First-generation college students who become nurses have the po-tential to enrich the diversity of the nursing profession and reach out to various socioeconomic and educa-tionally diverse client populations.
Prior Work Experience
A restructured workforce, welfare-to-work initiatives, displaced homemakers, popularity of midlife career changes, and health care career ladder programs have expanded the nursing applicant pool, increasing its diversity in prior work experience. Many students work full- or part-time.
Retention: Work–family–school conflicts may interfere with academic success and retention.
New graduate nurses may enter the nursing profession with a variety of prior work experiences that have the potential to enrich the nursing profession.
Enrollment Status
Almost half of all college students attend part-time. The number of part-time nursing students, especially those with multiple role responsibilities (work and family), has increased.
Retention: Work-family-school conflicts may interfere with academic success and retention.
Part-time students will take longer to complete their education. Entry into practice will be delayed and total number of potential work years in nursing will be decreased.
ESL, English as a second language.
Variable Select Nursing Student TrendsPotential Future Impact on the
Nursing Profession
Today’s student profile characteristics can be examined to predict the potential future impact on the nursing profession (see Table 1.1). Recent nursing enrollment trends suggest a steady increase among some minority groups. How-ever, in proportion to demographic changes, practically no increase has been noted among Hispanic groups (56, 58, 59, 69, 127, 134–136). Intensive recruitment efforts are imperative. Recruitment of diverse, nontraditional student populations does not assure program completion, licensure, or entry into the professional workforce. In fact, attrition has been and continues to be higher among nontra-ditional student populations (49, 51, 58, 59, 123, 126, 130, 131, 137–161). There-fore, intensive recruitment efforts must be partnered with concentrated efforts aimed at enhancing academic achievement, professional integration, satisfaction, retention, graduation, and entry into the nursing professional workforce.
Unfortunately, current employment trends in nursing indicate high turn-over rates, with nurses moving from workplace to workplace. High attrition

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
1 OVERVIEW OF KEY ISSUES AND CONCERNS 19
rates for new nurses leaving the nursing profession are also a major concern. The nursing shortage, high acuity of patient care, diminished resources, and an aging society emphasize the need to prioritize retention of nurses in the workplace. Alleviating the nursing shortage, optimizing opportunities for career advance-ment, offering incentives for educational advancement, and striving to promote professional (and workplace) satisfaction are broad objectives aimed at facilitat-ing nurse retention.
The recruitment of foreign nurses has been one strategy implemented to alleviate the nursing shortage, which has contributed to the changing profile characteristics of professional nurses. Foreign nurses are a heterogeneous group, representing much diversity in profile characteristics and in prior work experi-ence as a registered nurse. The recruitment of foreign nurses must incorporate culturally congruent strategies to ease their transition into the workplace setting, create multicultural workplace harmony, and promote professional satisfaction and opportunities for career advancement (62–66, 118). Bridging the gaps be-tween diverse groups of nurses is essential to preventing multicultural work-place conflict and promoting multicultural workplace harmony (see Chapter 2).
What recruitment and retention strategies are consistently implemented and evaluated within your current workplace setting? To what extent are they effective in recruiting and retaining underrepresented groups in nursing (or other health professions)? To what extent are culturally competent evidence-based best practices interwoven and visible within recruitment and retention strategies? What else should be done?
PREPARING CULTURALLY COMPETENT HEALTH CARE PROFESSIONALSGoals of culturally congruent health care and multicultural workplace har-mony can only be achieved by preparing health care professionals to actively engage in the process of cultural competence. Adequate preparation necessi-tates a diagnostic-prescriptive plan guided by a comprehensive understanding of the teaching–learning process of cultural competency development. Such a comprehensive plan must incorporate a detailed assessment and understanding of learner characteristics. Each learner characteristic provides vital information that is integral to determining special needs and strengths.
Meeting the needs of culturally diverse learners is a growing challenge in academia, the professional workplace, and within professional associations. Be-cause all students, nurses, and other health professionals belong to one or more cultural groups before entering professional education, they bring their patterns of learned values, beliefs, and behaviors into the academic and professional set-ting. Values are standards that have eminent worth, meaning, and importance in one’s life; values guide behavior. These cultural values are the “powerful directive forces that give order and meaning to people’s thinking, decisions, and actions” (101). Cultural values guide thinking, decisions, and actions within the student

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
20 I GETTING STARTED
and/or nurse role as well as in other aspects of their lives. Students, nurses, and other health professionals also hold numerous beliefs (ideas, convictions, philo-sophical opinions, or tenets) that are accepted as true without requiring evidence or proof. Beliefs are often unconsciously accepted as truths (8, 68).
Cultural values and beliefs unconsciously and consciously guide think-ing, decisions, and actions that ultimately affect the process of learning and the outcomes of learning. High levels of cultural congruence serve as a bridge to promote positive learning experiences and positive academic and/or psycho-logical outcomes; high levels of cultural incongruence are proposed as being inversely related to positive learning experiences and academic and/or psy-chological outcomes (59, 131, 162). Cultural congruence refers to the degree of fit between the learner’s values and beliefs and the values and beliefs of their surrounding environment (59, 131, 162–165). Here, the surrounding environ-ment refers to the environment of nursing education within the nursing pro-fession and the educational institution, workplace, or professional association setting.
Nursing is a unique culture that reflects its own cultural style. Cultural styles are the “recurring elements, expressions, and qualities that characterize a desig-nated cultural group through their series of action-patterns, beliefs, and values” (166, p. 155). The dominant values and norms of a cultural group guide the devel-opment of cultural styles (166). Currently (within the United States), the culture of nursing reflects many of the dominant societal values and beliefs held in the United States. Similarly, nursing education reflects many of the Western European value systems predominant in U.S. universities. Because nursing has its own set of CVB, students must become enculturated into nursing. Enculturation is a learning process whereby students learn to take on or live by the values, norms, and expec-tations of the nursing profession (167). Sufficient assistance during enculturation adjustment can minimize acculturation stress and enhance enculturation.
Another unique challenge facing nurse educators is to enculturate foreign-educated physicians and other second-career individuals who are entering nurs-ing programs (59, 60, 120, 131, 133, 168–170). Unfortunately, cultural competence as a priority professional value received delayed popularity among the nursing profession overall, with little emphasis or inclusion in nursing curricula, prac-tice, research, theory, administration, and the literature. Consequently, today’s nurse educators may be inadequately prepared to enculturate students into the new era of the nursing profession that embraces cultural diversity via a diversity of diversity approach and supports cultural competence development. Similarly, within other health disciplines, cultural competence as a priority or even as an essential professional value received delayed attention in professional practice settings and professional curricula, thereby contributing to a multidisciplinary health care culture poorly equipped to meet the culture-specific care needs of diverse patients in a multicultural workplace environment.
Although increases in culturally diverse students have been noted in higher education and in nursing, the values and beliefs underlying nursing education have been slow to change in accordance with changing student population needs. Ethnocentric tendencies and cultural blindness have been major obstacles to the needed changes in nursing education. Ethnocentric tendencies refer to the belief
This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
1 OVERVIEW OF KEY ISSUES AND CONCERNS 21
that the values and beliefs traditionally held within nursing education are su-preme. Consequently, traditional teaching–learning practices are upheld. Too of-ten, cultural blindness exists in nursing education. Within the context of nursing education, cultural blindness is the inability to recognize the different CVB that exist among diverse student populations. Because cultural blindness does not ac-knowledge that differences exist, cultural imposition of dominant nursing educa-tion values and beliefs undoubtedly occur. Cultural imposition can cause cultural shock, cultural clashes, cultural pain, and cultural assault among students whose CVB are incongruent with the dominant nursing CVB (59, 157).
Nurse educators are challenged to explore various CVB within nursing, nursing education, higher education, and student cultures and to make cultur-ally sensitive and appropriate decisions, actions, and innovations. Table 1.2 se-lectively compares and contrasts CVB of nursing education, higher education generally, and seven other cultural groups. Based on a review of the literature, traditional views within the identified cultures were included, but these are in no way meant to stereotype individuals within the cultures. Readers are cautioned about making stereotypes and are reminded to explore CVB of individual learn-ers. It is beyond the scope of this book to provide in-depth explanations about each category, yet the importance of an in-depth understanding must be recog-nized. The selective approach is meant to spark interest, stimulate awareness, and encourage further exploration among educators before attempting the de-sign of culturally relevant and congruent educational strategies. This approach is critical, because the need to understand, respect, maintain, and support the different CVB of culturally diverse learners is a precursor to culturally relevant and competent education (47, 51, 58, 59, 126–128, 132, 150, 152, 157, 170–178).
The teaching–learning process of cultural competence must consider the vari-ous philosophies and approaches to learning. Whether the teacher is perceived to be an authority figure, partner, coach, mentor, professional, or member of a service occupation will influence the teaching–learning process (see Table 1.2). Preferred teaching–learning styles may be active (learner-centered) or passive (teacher- centered). Although student-centered learning has long been advocated, nursing curricula have been slow to embrace this philosophy and to address the needs of diverse learner styles (59, 170, 178). Teaching–learning strategies perceived as fun and likable by some may be perceived as aggressive (debate), competitive (gaming), threatening (web-based, role-playing, or small group activity), boring (rote memori-zation), and/or irrelevant by others. Learner goals and philosophies that emphasize the “process” of learning focus on the journey of “becoming” culturally competent through the integration of cognitive, practical, and affective learning. Process learn-ers recognize that the journey itself is the “learning”; obstacles, mistakes, and hard-ships along the way are part of the expected developmental process that requires extra effort, sincere commitment, motivation, and persistence. Process learners real-ize that there is no final end product labeled “cultural competence”; rather, cultural competence is dynamic and ongoing. In contrast, “product” learners are focused on obtaining an end product through the mastery of content. Memorizing a multitude of “facts” about a culture becomes important rather than comprehensively understand-ing, applying, and appreciating the cultural context or rationale behind the “fact.” There is less concern with how to learn to apply knowledge and develop skills, and

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
22
Nursing Education
African American
Arab Muslim Americans
Chinese American
Haitian American
Irish American
Mexican American
Orthodox Jewish
American
Ori
enta
tio
n Individual Group Group Group Group Individual Group Individual
Tim
e P
erce
pti
on
Present and future oriented
Punctuality valued
Present oriented
Punctuality less important
Predestina-tion. Individual should work hard to make best of life. Punctuality re-laxed except in business.
History of past important.
Traditionally late-ness for appoint-ments is expected. More recently, lateness is consid-ered rude.
Past, present, future
Future predetermined
Relaxed punctuality
Past, present, future
Flexible sense of time.
Present oriented
Relaxed punctuality
Past, present, future
Punctuality valued
Verb
al C
om
mun
icat
ion
Direct, specific, and quick com-munication pre-ferred. Expects individuals to indicate when something is not understood.
Loud tones (in comparison to other cultures) are preferred.
Views and feel-ings are shared openly with fam-ily and trusted friends.
Highly contex-tual. Unspoken expectations more important than spoken. Speed loud and expressive.
Moderate to low tones preferred. Loud tone as-sociated with anger. Answers “yes” when asked if something is understood
Reluctant to talk about feelings and views.
Speech is quick, loud, high-pitched.
Low contextual language where meaning is explicit rather than implicit. Personal top-ics are private. Thoughts and feelings shared only with close family and friends.
Personal topics may be taboo. Feelings and views only shared with trusted fam-ily and friends. “Small talk” ex-pected to begin communication encounter.
Direct com-munication. Men avoid idle conversations with women.
TABLE 1.2 Comparison of Select Traditional Cultural Values and Beliefs
(continued)
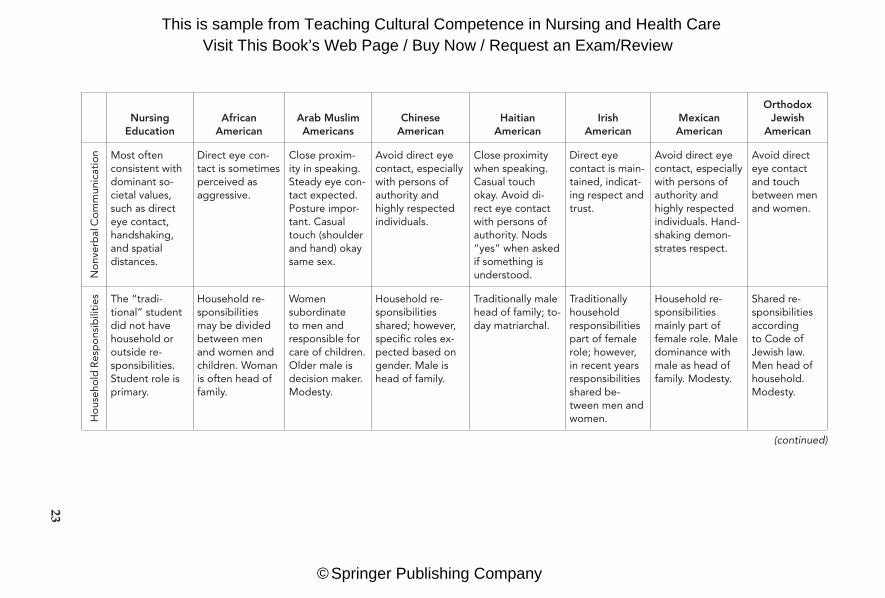
This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
23
Nursing Education
African American
Arab Muslim Americans
Chinese American
Haitian American
Irish American
Mexican American
Orthodox Jewish
American
No
nver
bal
Co
mm
unic
atio
n Most often consistent with dominant so-cietal values, such as direct eye contact, handshaking, and spatial distances.
Direct eye con-tact is sometimes perceived as aggressive.
Close proxim-ity in speaking. Steady eye con-tact expected. Posture impor-tant. Casual touch (shoulder and hand) okay same sex.
Avoid direct eye contact, especially with persons of authority and highly respected individuals.
Close proximity when speaking. Casual touch okay. Avoid di-rect eye contact with persons of authority. Nods “yes” when asked if something is understood.
Direct eye contact is main-tained, indicat-ing respect and trust.
Avoid direct eye contact, especially with persons of authority and highly respected individuals. Hand-shaking demon-strates respect.
Avoid direct eye contact and touch between men and women.
Ho
useh
old
Res
po
nsib
iliti
es The “tradi-tional” student did not have household or outside re-sponsibilities. Student role is primary.
Household re-sponsibilities may be divided between men and women and children. Woman is often head of family.
Women subordinate to men and responsible for care of children. Older male is decision maker. Modesty.
Household re-sponsibilities shared; however, specific roles ex-pected based on gender. Male is head of family.
Traditionally male head of family; to-day matriarchal.
Traditionally household responsibilities part of female role; however, in recent years responsibilities shared be-tween men and women.
Household re-sponsibilities mainly part of female role. Male dominance with male as head of family. Modesty.
Shared re-sponsibilities according to Code of Jewish law. Men head of household. Modesty.
(continued)
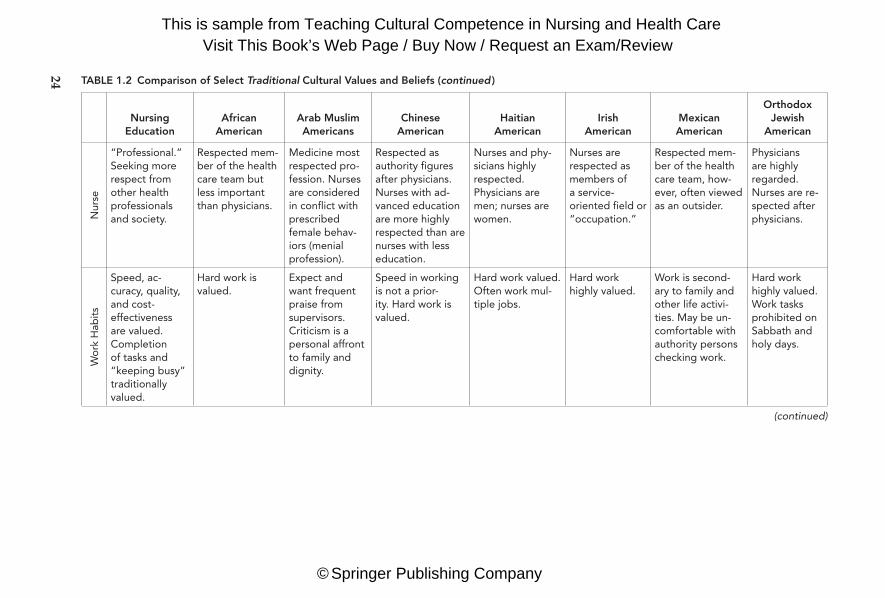
This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
24
Nursing Education
African American
Arab Muslim Americans
Chinese American
Haitian American
Irish American
Mexican American
Orthodox Jewish
American
Nur
se
“Professional.” Seeking more respect from other health professionals and society.
Respected mem-ber of the health care team but less important than physicians.
Medicine most respected pro-fession. Nurses are considered in conflict with prescribed female behav-iors (menial profession).
Respected as authority figures after physicians. Nurses with ad-vanced education are more highly respected than are nurses with less education.
Nurses and phy-sicians highly respected. Physicians are men; nurses are women.
Nurses are respected as members of a service- oriented field or “occupation.”
Respected mem-ber of the health care team, how-ever, often viewed as an outsider.
Physicians are highly regarded. Nurses are re-spected after physicians.
Wo
rk H
abit
s
Speed, ac-curacy, quality, and cost- effectiveness are valued. Completion of tasks and “keeping busy” traditionally valued.
Hard work is valued.
Expect and want frequent praise from supervisors. Criticism is a personal affront to family and dignity.
Speed in working is not a prior-ity. Hard work is valued.
Hard work valued. Often work mul-tiple jobs.
Hard work highly valued.
Work is second-ary to family and other life activi-ties. May be un-comfortable with authority persons checking work.
Hard work highly valued. Work tasks prohibited on Sabbath and holy days.
TABLE 1.2 Comparison of Select Traditional Cultural Values and Beliefs (continued )
(continued)

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
Nursing Education
African American
Arab Muslim Americans
Chinese American
Haitian American
Irish American
Mexican American
Orthodox Jewish
American
Aut
ono
my
Competition with author-ity. Assertive. Autonomous decision making within the scope of nursing prac-tice expected.
Self-reliance and autonomy en-couraged within group. Past discrimination experiences may discourage au-tonomy. Females are often head of household and decision makers.
Males more au-tonomous. Fe-males defer to males and older females.
Defers to person in authority, often seeking approval before making decisions. Avoids conflict and values harmony.
Self-reliance and autonomy encouraged within group. Past discrimina-tion experiences may discourage autonomy.
Autonomy and independence outside the family is en-couraged while family loyalty is still maintained.
Defers to person in authority with males as dominant decision makers. Input of others is considered in decision making. Autonomy for females is more difficult than for males. Avoids competition and conflict.
Expected to be au-tonomous and question or challenge oth-ers as needed.
Hel
p-S
eeki
ng B
ehav
iors Individual is
expected to initiate help- seeking behaviors.
Varied: May seek help within own social network before seeking outside help.
Delayed help-seeking by women due to modesty is-sues. Mental health needs and disabilities stigmatized.
Stigma for seeking help for emotional disorders & stress.
May be reluctant to approach for help by attempt-ing to “save face.”
Varied: May seek help within own folk net-work. Stigma for seeking help with emotional disorders.
May delay seek-ing help. Denial of problems is a way of coping with physical and emotional problems.
Varied. May seek help within own social network before seeking outside help.
Religious duty to actively seek help from health pro-fessionals to keep in good health. Seek guidance from rabbi.
Sources: Jeffreys, M. R. (2012). Nursing student retention: Understanding the process and making a difference. (2nd ed.). New York, NY: Springer Publishing. Purnell, L. D. (2009). Guide to culturally competent health care. (2nd ed.), Philadelphia, PA: F. A. Davis.
25

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
26 I GETTING STARTED
even less concern with affective learning (values, attitudes, and beliefs). Product learners would be greatly disturbed, dissatisfied, and poorly motivated with an ap-proach that views the end point for becoming culturally competent as infinite.
Perceived barriers to learning, mismatches in teacher–learner expectations, and poor learning experiences will hinder the learning process of cultural compe-tence. For example, faculty beliefs that nonminority students are less confident in caring for culturally different clients than minority students is stereotypical and inaccurate (179–186). Similarly, the belief that minority nurses are intrinsically equipped to care for culturally diverse clients is also inaccurate and negates the uniqueness of the many cultures that comprise the federally recognized “minor-ity” group categories and disregards the many cultures that comprise nonminor-ity groups. The danger is that minority students’ and nurses’ educational needs with respect to providing culturally congruent care for many different groups of culturally different clients (different in culture from care provider) may be ignored. Expectations that are more, less, or different, based solely on ethnic or racial background, are grossly inadequate, because other diverse profile charac-teristics and their potential influence on learning must be objectively appraised.
Meeting the needs of learners representing diversity in age, ethnicity and race, gender, primary language, prior educational experience, family’s educa-tional background, prior work experience, and/or enrollment means embracing a broader, more inclusive worldview that appreciates various forms of diversity. Awareness of how each profile variable can potentially influence learning is a necessary first step in understanding the multidimensional process of cultural competence development. For example, the learning needs and expectations of foreign-educated learners may be very different from what educators initially perceive, creating an obstacle for learning, achievement, and satisfaction (59, 62–66, 120, 157, 187, 188). Acculturation stress, adaptation, assimilation, CVB to-ward education, experiences with second language, and expectations can impact greatly upon learning and achievement (51, 58, 59, 150, 188–195). Other stressors that may affect specific subgroups in nursing include: perceived cultural incon-gruence, perceived (or fear of) discrimination and bias, student (learner) role in-congruence, maternal role stress, perceived multiple role stress, and gender role identity stress (59). In addition, students who work in the health care field as unlicensed personnel, licensed practical nurses, or health care paraprofessionals may have difficulty adjusting to a new role, new worldview, and critical thinking and decision making within a nursing perspective that is guided by the profes-sional scope of nursing practice (59, 131, 157). Second-career students entering nursing may also bring new visions; however, second-career nursing students and graduates in accelerated programs present new challenges for professional socialization and integration (59, 60, 131, 132, 157, 178, 196, 197).
New graduate nurses may experience reality shock with their new profes-sional role, workload, and responsibilities; experienced nurses may encounter burnout. Inactive nurses returning to the workforce after a gap in work expe-rience benefit from refresher courses and other transitional strategies to ease them into the new workplace environment (198). Recently, researchers have begun to realize the need to explore the relationships between psychological distress, effort-reward imbalance, and the nursing work environment among

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
1 OVERVIEW OF KEY ISSUES AND CONCERNS 27
different generations: Baby boomers, Generation X, and Generation Y (59, 199). The generation of the Millennials challenges educators to keep pace with the social and educational technologies that these learners expect (170, 187, 200–203). For example, the net generation (1980 to 2004) expects technology, participates actively in the learning process, wants immediate response to learning, multi-tasks, prefers group work, and enjoys being mentored by older generations. In contrast, Generation X (1960 to 1980) are self-directed learners who are less tech-nology proficient, can delay gratification, and seek learning with practical ap-plication. Baby boomers (1940 to 1960) are generally less technology proficient, because technology is viewed as a new approach rather than an expected ap-proach, are more familiar with passive learning styles, and expect a caring and connected work environment (59, 60, 187, 203).
The nursing profession has the challenging opportunity to meet the unique needs of various populations of nurses, improve nurse retention, decrease the nursing shortage, and promote cultural competence. Evidence-based transitional programs, specialized orientation programs, ongoing employee workshops, and refresher courses that integrate the values, skills, and knowledge needed for cul-tural competence in the workplace have the potential to address these needs. Unfortunately, state and certifying boards/associations have varied continuing education (CE) and competency requirements for license renewal and reentry (60, 204) and none require documentation of CE programs in cultural competence. Among other health professionals, inconsistencies in licensure renewal, certifica-tion, CE, and practice requirements also exist. For example, physicians licensed in New Jersey are now required to complete CE in cultural competence, yet this is not a universal medical requirement throughout the United States. Professional inconsistencies (in any discipline) may translate into questioning the need for the requirement, decreased motivation, resentment, and lack of commitment on the part of the professional, thereby defeating the overall goal of actively engaging the health professional in lifelong commitment to cultural competence development.
To what extent are the multidimensional factors influencing the persistence, retention, satisfaction, stress, and optimal success considered and addressed with students, staff education, or other learners in your setting? What else should be done?
CULTURAL COMPETENCE AND CONFIDENCEDespite the numerous complexities, changes, and challenges faced by many nurs-ing students and nurses today, some individuals are more actively engaged in cultural competence development whereas others are not. Some individuals are more motivated to pursue cultural competence development and are more com-mitted to the goal of culturally congruent care than others. Therefore, the evalu-ation of factors that may influence motivation, persistence, and commitment for cultural competency development is a necessary precursor to any educational design strategy. Confidence (self-efficacy) is one such factor that is emphasized

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
28 I GETTING STARTED
in this book. According to Bandura (205), the construct of self- efficacy is the indi-viduals’ perceived confidence for learning or performing specific tasks or skills necessary to achieve a particular goal. Furthermore, self-efficacy is the belief that one can perform or succeed at learning a specific task, despite obstacles and hardships, and will expend whatever energy is necessary to accomplish the task (205). Consequently, confidence is inextricably linked as a major component in cultural competence development and an influencing factor in the achievement of culturally congruent care. Confidence is an integral component in the action-strategy acronym COMPETENCE, introduced and illustrated in the next chapter. The acronym may be used by the multidisciplinary health care team to (a) guide clinical practice with culturally diverse patients and (b) promote multicultural workplace harmony and prevent multicultural workplace conflict among cultur-ally diverse health care workers. Chapter 3 proposes a new conceptual model to understand and guide cultural competence education, research, and practice.
To what extent does confidence (self-efficacy) influence your learning and performance of transcultural skills and cultural competence? Among clients of different cultural backgrounds, how knowledgeable are you about the ways in which cultural factors may influence patient care? Using the broad definition of culture (recognizing the diversity of diversity), how confident are you about interviewing clients of different cultural backgrounds to learn about their values and beliefs? How confident are you about your attitudes, values, and beliefs concerning culturally different people? (complete Jeffreys Toolkit Item 1 Transcultural Self-Efficacy Tool [TSET] or Item 2 [TSET–Multidisciplinary Healthcare Provider]).
KEY POINT SUMMARY
• Rapid growth in worldwide migration, changes in demographic patterns, varying fertility rates, increased numbers of multiracial and multiethnic indi-viduals, and advanced technology contribute to cultural evolution.
• Culturally congruent health care refers to health care that is customized to fit with the client’s cultural values and beliefs, traditions, practices, and lifestyle.
• Goals of culturally congruent health care and multicultural workplace harmony can only be achieved by preparing (teaching) health care professionals to ac-tively engage in the (learning) process of cultural competence that aims to go beyond the goal of achieving “competence” (minimum standard) toward the goal of achieving “optimal” cultural competence (standard of excellence).
• Meeting the needs of learners representing diversity in age, ethnicity and race, gender, primary language, prior educational experience, family’s educational background, prior work experience, and/or enrollment means embracing a broader, more inclusive worldview that appreciates various forms of diversity and must consider the various philosophies and approaches to learning.
• Confidence (self-efficacy) is an important factor that may influence motiva-tion, persistence, and commitment to cultural competency development.
This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
1 OVERVIEW OF KEY ISSUES AND CONCERNS 29
APPLICATION STRATEGIES
EASY APPLICATION ACTION STEPS
Touring topics and issues: Appraising knowledge1. Skim the topics and issues presented in the chapter. 2. Identify the three topics or issues you know about most.3. Contemplate why you know most about them.4. Identify the three topics or issues you know about least.5. Contemplate why you know least about them.
Touring topics and issues: Appraising confidence, motivation, stress, interest, apathyAdapt steps 1–5, substituting appraisal of knowledge for confidence, motivation, stress, interest, and apathy.
Touring topics and issues: Prioritizing further inquiry
1. Select the three topics or issues on which further exploration would most en-hance your current professional role.
2. Develop a plan and timeline for further research on these topics or issues.
TOOLKIT RESOURCE BOXItem 1—Transcultural Self-Efficacy Tool (TSET)Item 2—Transcultural Self-Efficacy Tool–Multidisciplinary Healthcare Pro-
vider (TSET–MHP)
DISCUSSION QUESTIONS
1. Review Table 1.1. Which nursing student trend intrigued you the most? Why? Discuss.
2. Review Table 1.1. Which nursing student trend has the greatest potential to positively impact the health care needs of diverse populations? Why? Discuss.
3. Review Table 1.2. Discuss strategies for appraising, adapting, and evaluating information in Table 1.2 without perpetuating stereotypes based upon labeled or assumed backgrounds. What are the benefits of comparing and contrasting select cultural values and beliefs presented in Table 1.2?
4. What are some of the barriers to achieving a rapid transformation in health care through transcultural nursing? Propose innovative ideas for addressing at least one of the barriers.
5. Is culturally congruent care a right or a privilege? Why? Discuss.
REFERENCES1. Jeffreys, M. R., & Zoucha, R. (2001). The invisible culture of the multiracial, multieth-
nic individual: A transcultural imperative. Journal of Cultural Diversity, 8(3), 79–83.

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
30 I GETTING STARTED
2. Andrews, M. M., & Boyle, J. S. (2012). Transcultural concepts in nursing care (6th ed.). Philadelphia, PA: Wolters Kluwer/Lippincott, Williams, & Wilkins.
3. Campinha-Bacote, J. (2003). The process of cultural competence in the delivery of healthcare services: A culturally competent model of care (4th ed.). Cincinnati, OH: Transcultural C.A.R.E. Associates.
4. Leininger, M. M. (1991). Culture care diversity and universality: A theory of nursing. New York, NY: National League for Nursing.
5. Leininger, M. M., & McFarland, M. R. (2002). Transcultural nursing: Concepts, theories, research, and practice (3rd ed.). New York, NY: McGraw-Hill.
6. Leininger, M. M., & McFarland, M. R. (2006). Culture care diversity and universality: A worldwide nursing theory (2nd ed.). Boston, MA: Jones and Bartlett.
7. McFarland, M. R., & Wehbe-Alamah, H. (2015). Leininger’s culture care diversity and universality: A worldwide nursing theory. Boston, MA: Jones and Bartlett.
8. Purnell, L. D. (2013). Transcultural health care: A culturally competent approach (4th ed.). Philadelphia, PA: F. A. Davis.
9. U.S. Census Bureau. (2011). United States Census 2010. Retrieved from http://www .census.gov/2010census
10. Department of Health and Human Services. (2009). Healthy People 2020. Retrieved from http://www.healthypeople.gov
11. Kosoko-Lasaki, S., Cook, C. T., & O’Brien, R. L. (2009). Cultural proficiency in address-ing health disparities. Boston, MA: Jones and Bartlett.
12. De Chesnay, M., & Anderson, B. A. (2008). Caring for the vulnerable: Perspectives in nursing theory, practice, and research. Boston, MA: Jones and Bartlett.
13. Dreachslin, J. L., Gilbert, M. J., & Malone, B. (2013). Diversity and cultural competence in health care: A systems approach. San Francisco, CA: Jossey-Bass.
14. Sullivan, C. G. (2015). American Academy of Nursing on Policy: Implementing cul-turally competent care. Nursing Outlook, 63(2), 227–229.
15. Douglas, M. K., Rosenkoetter, M., Pacquiao, D. F., Callister, L. C., Hattar-Pollara, M., Lauderdale, J., . . . Purnell, L. (2014). Guidelines for implementing culturally compe-tent care. Journal of Transcultural Nursing, 25(2), 109–121.
16. Miller, J. E., Leininger, M., Leuning, C., Pacquiao, D., Andrews, M., Ludwig-Beymer, P., & Papadopoulos, I. (2008). Transcultural Nursing Society position statement on human rights. Journal of Transcultural Nursing, 19(5), 5–7.
17. Kersey-Matusiak, G. (2013). Delivering culturally competent nursing care. New York, NY: Springer Publishing.
18. Basuray, J. (2013). Culture and health: Concept and practice (Rev. ed.). Ronkonkoma, NY: Linus.
19. Glittenberg, J. (2004). A transdisciplinary, transcultural model for health care. Journal of Transcultural Nursing, 15(1), 6–10.
20. Johnson, T. P., et al. (1997). Dimensions of self-identification among multiracial and multiethnic respondents in survey interviews. Evaluation Review, 21(6), 671–687.
21. Lee, S. M., & Fernandez, M. (1998). Trends in Asian American racial/ethnic intermar-riage: A comparison of 1980 and 1990 census data. Sociological Perspectives, 41(2), 323–342.
22. Perlmann, J. (1997). Multiracials, intermarriage, and ethnicity. Society, 6, 20–23.23. Sands, N., & Schuh, J. H. (2004). Identifying interventions to improve the retention
of biracial students: A case study. Journal of College Student Retention: Research, Theory, and Practice, 5(4), 349–363.
24. Spickard, P. R., & Fong, R. (1995). Pacific Islander Americans and the question of mul-tiethnicity: A vision of America’s future? Social Forces, 73(4), 1365–1383.
25. Shih, M., & Sanchez, D. T. (2009). When race becomes even more complex: Toward understanding the landscape of multiracial identity and experiences. Journal of Social Issues, 65(1), 1–11.
This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
1 OVERVIEW OF KEY ISSUES AND CONCERNS 31
26. Smith, T. D., & Maton, K. I. (2015). Perceptions and experiences in higher education: A national study of multiracial Asian American and Latino/a students in psychology. Cultural Diversity and Ethnic Minority Psychology, 21(1), 97–104.
27. Campbell, M. E., & Herman, M. R. (2010). Politics and policies: Attitudes toward mul-tiracial Americans. Ethnic and Racial Studies, 33(9), 1511–1536.
28. Jeffreys, M. R. (2005). Clinical nurse specialists as cultural brokers, change agents, and partners in meeting the needs of culturally diverse populations. Journal of Multi-cultural Nursing and Health, 11(2), 41–48.
29. Nadal, K. L., Sriken, J., Davidoff, K. C., Wong, Y., & McLean, K. (2013). Microag-gressions within families: Experiences of multiracial people. Family Relations, 62, 190–201.
30. Farley, R. (2001). Identifying with multiple races. Report 01-491. Ann Arbor, MI: Univer-sity of Michigan, Population Studies Center (as cited in Shih, M., & Sanchez, D. T. (2009). When race becomes even more complex: Toward understanding the land-scape of multiracial identity and experiences. Journal of Social Issues, 65(1), p. 2.)
31. Nash, G. B. (1995). The hidden history of mestizo in America. Journal of American History, 82(3), 941–962.
32. Pascoe, P. (1996). Miscegenation law, court cases, and ideologies of “race” in twenti-eth-century America. Journal of American History, 83(1), 44–69.
33. Giamo, L. S., Schmitt, M. T., & Outten, R. (2012). Perceived discrimination, group identification, and life satisfaction among multiracial people: A test of the rejec-tion-identification model. Cultural Diversity and Ethnic Minority Psychology, 18(4), 319–328.
34. Nazish, S. M., & O’Brien, K. M. (2011). Challenges and resilience in the lives of urban, multiracial adults: An instrument development study. Journal of Counseling Psychology, 58(4), 494–507.
35. Hall, C. C. I. (1992). Coloring outside the lines. In M. P. P. Root (Ed.), Racially mixed people in America (pp. 326–329). Newbury Park, CA: Sage.
36. Pinderhughes, E. (1995). Biracial identity—asset or handicap? In H. W. Harris, C. Blue, & E. E. H. Griffith, Racial and ethnic identity: Psychological development and creative expression (pp. 73–93). New York, NY: Routledge.
37. Daniel, G. R. (1992). Beyond black and white: The new multiracial consciousness. In M. P. P. Root (Ed.), Racially mixed people in America (pp. 333–341). Newbury Park, CA: Sage.
38. Root, M. P. P. (1992). Within, between, and beyond race. In M. P. P. Root (Ed.), Racially mixed people in America (pp. 3–11). Newbury Park, CA: Sage.
39. Root, M. P. P. (1997). Multiracial Asians: Models of ethnic identity. Ameriasia Journal, 23(1), 29–41.
40. Sagar, P. L. (2015). Transcultural nursing certification: Its role in nursing education, practice administration, and research. In M. McFarland & H. Wehbe-Alamah (Eds.), Leininger’s culture care diversity and universality: A worldwide nursing theory (3rd ed., pp. 579–600). Boston, MA: Jones and Bartlett.
41. Sagar, P. L. (2012). Transcultural nursing theory and models: Application in nursing educa-tion, practice, and administration. New York, NY: Springer Publishing.
42. Sagar, P. L. (2014). Transcultural nursing education strategies. New York, NY: Springer Publishing.
43. Miller, J. (1997). Politics and care: A study of Czech Americans within Leininger’s Theory of Culture Care Diversity and Universality. Journal of Transcultural Nursing, 9(1), 3–13.
44. Davidson, P. M., Meleis, A., Daly, J., & Douglas, M. (2003). Globalisation as we enter the 21st century: Reflections and directions for nursing education, science, research and clinical practice. Contemporary Nurse, 15(3), 162–174.

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
32 I GETTING STARTED
45. Murray, J. P., Wenger, A. F. Z., Downes, E. A., & Terrazas, S. B. (2011). Educating health professionals in low-resource countries: A global approach. New York, NY: Springer Publishing.
46. Holtz, C. (2008). Global health care. Boston, MA: Jones and Bartlett.47. Abrums, M. E., & Leppa, C. (2001). Beyond cultural competence: Teaching about race,
gender, class, and sexual orientation. Journal of Nursing Education, 40(6), 270–275.48. American Nurses Association. (1998). Position statement on discrimination and racism in
health care. Silver Spring, MD: Author. 49. Barbee, E. L., & Gibson, S. E. (2001). Our dismal progress: The recruitment of non-
Whites into nursing. Journal of Nursing Education, 40(6), 243–245.50. Bolton, L. B., Giger, J. N., & Georges, C. A. (2004). Structural and racial barriers to health
care. In L. Fitzpatrick (Ed.), Annual review of nursing research (Vol. 22, pp. 39–58). New York, NY: Springer Publishing.
51. Bosher, S. D., & Pharris, M. D. (2009). Transforming nursing education: The culturally inclusive environment. New York, NY: Springer Publishing.
52. Farella, C. (2002). School of hard knocks: Is racism a fixture of nursing academia? Nursing Spectrum, 14(12) NY/NJ, 34–35.
53. Huff, R. M., & Kline, M. V. (1999). Promoting health in multicultural populations: A hand-book for practitioners. Thousand Oaks, CA: Sage.
54. Porter, C. P., & Barbee, E. (2004). Race and racism in nursing research: Past, present, and future. In L. Fitzpatrick (Ed.), Annual review of nursing research (Vol. 22, pp. 9–38). New York, NY: Springer Publishing.
55. Wilson, D. W. (2007). From their own voices: The lived experience of African American registered nurses. Journal of Transcultural Nursing, 18(2), 142–149.
56. Moceri, J. T. (2014). Hispanic nurses’ experiences of bias in the workplace. Journal of Transcultural Nursing, 25(1), 15–22.
57. Qaabidh, L. L., Wesley, Y., Gulstone, J., & George-Jackson, G. (2011). Career advance-ment, Black nurses and healthcare disparities: Overcoming the odds. Journal of Chi Eta Phi Sorority, 55(1), 2–6.
58. Beard, K. V. (2014). Strengthening diversity in nursing: The practices and prepared-ness of nursing faculty. Journal of Nursing Education and Practice, 4(11), 59–65.
59. Jeffreys, M. R. (2012). Nursing student retention: Understanding the process and making a difference (2nd ed.). New York, NY: Springer Publishing.
60. Finkelman, A., & Kenner, C. (2016). Professional nursing concepts: Competencies for qual-ity leadership (3rd ed.). Burlington, MA: Jones and Bartlett.
61. Giger, J., Davidhizar, R. E., Purnell, L., Harden, J. T., Phillips, J., & Strickland, O. (2007). American Academy of Nursing Expert Panel Report: Developing cultural competence to eliminate health disparities in ethnic minorities and other vulnerable populations. Journal of Transcultural Nursing, 18(2), 95–102.
62. Sherman, R. O., & Eggenberger, T. (2008). Transitioning internationally recruited nurses into clinical settings. Journal of Continuing Education in Nursing, 39(12), 535–544.
63. Zizzo, K. A., & Xu, Y. (2009). Post-hire transitional programs for international nurses: A systematic review. Journal of Continuing Education in Nursing, 40(2), 57–64.
64. Sherwood, G. D., & Shaffer, F. A. (2014). The role of internationally educated nurses in a quality, safe workforce. Nursing Outlook, 62, 46–52.
65. Pittman, P., et al. (2013). Perceptions of employment-based discrimination among newly-arrived foreign-educated nurses. American Journal of Nursing, 114(1), 26–35.
66. Xu, Y., & He, F. (2012). Transition programs for internationally educated nurses: What can the United States learn from the United Kingdom, Australia, and Canada? Nurs-ing Economics, 30(4), 215–223.
67. Purnell, L. D., & Paulanka, B. J. (2008). Transcultural health care: A culturally competent approach (3rd ed.). Philadelphia, PA: F. A. Davis.
This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
1 OVERVIEW OF KEY ISSUES AND CONCERNS 33
68. Leininger, M. M. (2002). Transcultural food functions, beliefs, and practices. In M. M. Leininger & M. R. McFarland (Eds.), Transcultural nursing: Concepts, theories, research, and practice (3rd ed., pp. 205–216). New York, NY: McGraw-Hill.
69. U.S. Department of Health and Human Services. (2010). The registered nurse popula-tion: Findings from the March 2008 National Sample Survey of Registered Nurses. Retrieved from http://bhpr.hrsa.gov/healthworkforce/rnsurveys/rnsurveyfinal.pdf
70. St. Hill, P., Lipson, J. G., & Meleis, A. I. (2003). Caring for women cross-culturally. Philadelphia, PA: F. A. Davis.
71. Donnelly, P. J. L. (1992). The impact of culture on psychotherapy: Korean clients’ expectations in psychotherapy, Journal of the New York State Nurses Association, 23(2), 12–19.
72. Donnelly, P. J. L. (2005). Mental health beliefs and help seeking behaviors of Korean American parents of adult children with schizophrenia. Journal of Multicultural Nurs-ing and Health, 11(2), 23–24.
73. Lattanzi, J. B., & Purnell, L. D. (2006). Developing cultural competence in physical therapy practice. Philadelphia, PA: F. A. Davis.
74. American Nurses Association. (2013). Code of ethics interpretive statements. Washington DC: Author.
75. Cameron-Traub, E. (2002). Western ethical, moral, and legal dimensions within the culture care theory. In M. Leininger & M. McFarland (Eds.), Transcultural nursing: Concepts, theories, research, and practice (pp. 169–177). New York, NY: McGraw-Hill.
76. International Council of Nurses. (1973). Code for nurses. Geneva, Switzerland: Author.
77. Leininger, M. (1991). Transcultural care principles, human rights, and ethical consid-erations. Journal of Transcultural Nursing, 3(1), 21–23.
78. World Health Organization. (2002). 25 Questions and answers on health and human rights. Health and Human Rights Publication Series, Issue 1, Author.
79. World Health Organization. (2006). Constitution of the World Health Organization, Basic Documents, 45th ed., Supplement, October 2006, Author.
80. Office of Minority Health. (2001). National standards for culturally and linguistically appropriate services in health care. Washington, DC: U.S. Department of Health and Human Services.
81. Office of Minority Health. (2013). National standards for culturally and linguistically appropriate services in health care: A blueprint for enhancing and sustaining CLAS policy and practice. Washington, DC: U.S. Department of Health and Human Services.
82. Krentzman, A. R., & Townsend, A. L. (2008). Review of multidisciplinary measures of cultural competence for use in social work education. Journal of Social Work Education, 44(2), 1–25.
83. Suh, E. E. (2004). The model of cultural competence through an evolutionary concept analysis. Journal of Transcultural Nursing, 15(4), 93–102.
84. American Dental Association. (2014). Accreditation standards for advanced education programs in general dentistry: Commission on dental accreditation. Chicago, IL: Author.
85. Yoder, K. M. (2006). A framework for service-learning in dental education. Journal of Dental Education, 70(2), 115–123.
86. American Association of Medical Colleges. (2015). Assessing change: Evaluating cul-tural competence education and training. Washington, DC: Author.
87. Humbert, T. K., Burket, A., Deveney, R., & Kennedy, K. (2012). Occupational therapy students’ perspectives regarding international cross-cultural experiences. Australian Occupational Therapy Journal, 59, 225–234.
88. Nochajski, S. M., & Matteliano, M. A. (2008). A guide to cultural competence in the cur-riculum: Occupational therapy. Buffalo, NY: Center for International Rehabilitation Research Information and Exchange.

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
34 I GETTING STARTED
89. American Physical Therapy Association. (2008). Blueprint for teaching cultural compe-tence in physical therapy education. Alexandria, VA: Author.
90. Panzarella, K. J., & Matteliano, M. A. (2008). A guide to cultural competence in the curric-ulum: Physical therapy. Buffalo, NY: Center for International Rehabilitation Research Information and Exchange.
91. Hayward, L. M., & Charrette, A. L. (2012). Integrating cultural competence and core values: An international service-learning model. Journal of Physical Therapy Education, 26(1), 78–89.
92. Kelly, P. J. (2013). A framework for service learning in physician assistant education that fosters cultural competency. The Journal of Physician Assistant Education, 24(2), 32–37.
93. Gerstein, L. H., Heppner, P. P., Aegisdottir, S., Leung, S.-M.A., & Norsworthy, K. L. (2009). International handbook of cross-cultural counseling: Cultural assumptions and prac-tices worldwide. Washington, DC: Sage.
94. Ponterotto, J. G., Cassas, J. M., Suzuki, L. A., & Alexander, C. M. (2010). Handbook of multicultural counseling (3rd ed.). Washington, DC: Sage.
95. American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: Author.
96. Lee, G. K., & Matteliano, M. A. (2009). A guide to cultural competence in the curriculum: Rehabilitative counseling. Buffalo, NY: Center for International Rehabilitation Research Information and Exchange.
97. Lubinski, R., & Matteliano, M. A. (2008). A guide to cultural competence in the curricu-lum: Speech-language pathology. Buffalo, NY: Center for International Rehabilitation Research Information and Exchange.
98. National Association of Social Workers. (2001). Standards for cultural competence in so-cial work practice. Washington, DC: Author.
99. National Association of Social Workers. (2007). Indicators for the achievement of the NASW standards for cultural competence in social work practice. Washington, DC: Author.
100. National Association of Social Workers. (2009). Code of ethics. Washington, DC: Author.
101. Leininger, M. M. (1995). Transcultural nursing: Concepts, theories, research, and practice. Blacklick, OH: McGraw-Hill College Custom Services.
102. Jeffreys, M. R. (2006). Cultural competence in clinical practice. Imprint, 53(2), 36–41.103. Jeffreys, M. R. (2006). Teaching cultural competence in nursing and health care: Inquiry,
action, and innovation. New York, NY: Springer Publishing.104. Jeffreys, M. R. (2002). A transcultural core course in the clinical nurse specialist cur-
riculum. Clinical Nurse Specialist: The Journal for Advanced Nursing Practice, 16(4), 195–202.
105. Leininger, M. M. (1995). Teaching transcultural nursing in undergraduate and gradu-ate programs. Journal of Transcultural Nursing, 6(2), 10–26.
106. Andrews, M. (1995). Transcultural nursing: Transforming the curriculum. Journal of Transcultural Nursing, 6(2), 4–9.
107. Mixer, S. J. (2015). Application of culture care theory in teaching cultural compe-tence and culturally congruent care. In M. McFarland & H. Wehbe-Alamah (Eds.), Leininger’s culture care diversity and universality: A worldwide nursing theory (3rd ed., pp. 369–387). Boston, MA: Jones and Bartlett.
108. American Association of Colleges of Nursing. (2014). Nursing faculty shortage [Fact sheet]. Washington, DC: Author.
109. Ryan, M., Carlton, K. H., & Ali, N. (2000). Transcultural nursing concepts and experi-ences in nursing curricula. Journal of Transcultural Nursing, 11(4), 300–307.

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
1 OVERVIEW OF KEY ISSUES AND CONCERNS 35
110. Douglas, M. K., & Pacquiao, D. (2010). Core curriculum for transcultural nursing and health care. Journal of Transcultural Nursing, 21(Supplement 1).
111. American Association of Colleges of Nursing. (2009). Establishing a culturally compe-tent master’s and doctorally prepared nursing workforce. Washington, DC: Author.
112. American Association of Colleges of Nursing. (2011). Toolkit for cultural competence in masters and doctoral nursing education. Washington, DC: Author.
113. American Association of Colleges of Nursing. (2008). Cultural competency in baccalau-reate nursing education. Washington, DC: Author.
114. American Association of Colleges of Nursing. (2008). Toolkit for cultural competent edu-cation for baccalaureate nurses. Washington, DC: Author.
115. American Association of Colleges of Nursing. (2006). The essentials of doctoral educa-tion for advanced nursing practice. Washington, DC: Author.
116. American Association of Colleges of Nursing. (2008). The essentials of baccalaureate education for professional nursing practice. Washington, DC: Author.
117. American Association of Colleges of Nursing. (2011). The essentials of master’s educa-tion in nursing. Washington, DC: Author.
118. Rosenkoetter, M. M., & Nardi, D. A. (2007). American Academy of Nursing Expert Panel on Global Nursing and Health: White paper on global nursing and health. Jour-nal of Transcultural Nursing, 18(4), 305–315.
119. Jeffreys, M. R. (2016). Cultural competence education resource toolkit (3rd ed.). New York, NY: Springer Publishing.
120. Grossman, D., & Jorda, M. L. (2008). Transitioning foreign-educated physicians to nurses: The new Americans in nursing. Journal of Nursing Education, 47(12), 544–551.
121. Tagliareni, M. E. (2008). Quoted in J. Sapers, Shaping the future of nursing. TC Today, 33(1), 13–17.
122. Schumacher, G., Risco, K., & Conway, A. (2008). The Schumacher model: Fostering scholarship and excellence in nursing and for recruiting and grooming new faculty. Journal of Nursing Education, 47(12), 571–575.
123. Bessent, H. (Ed.). (1997). Strategies for recruitment, retention, and graduation of minority nurses in colleges of nursing. Washington, DC: American Nurses Publishing.
124. Department of Health and Human Services. (2000). Healthy People 2010: Under-standing and improving health (2nd ed.). Washington DC: U.S. Government Printing Office.
125. National League for Nursing. (2009). A commitment to diversity in nursing and nursing education. [Reflection and Dialogue]. Retrieved from http://www.nln.org/about/ position-statements/nln-reflections-dialogue/read/dialogue-reflection/2009/01/01/dialogue-reflection-on-a-commitment-to-diversity-in-nursing-and-nursing-education
126. Tucker-Allen, S., & Long, E. (1999). Recruitment and retention of minority nursing students: Stories of success. Lisle, IL: Tucker Publications.
127. Villaruel, A. M., Canales, M., & Torres, S. (2001). Bridges and barriers: Educational mobility of Hispanic nurses. Journal of Nursing Education, 40(6), 245–251.
128. Yoder, M. K. (2001). The bridging approach: Effective strategies for teaching ethni-cally diverse nursing students. Journal of Transcultural Nursing, 12, 319–325.
129. Jeffreys, M. R. (2013). Diverse learners. In D. Hunt (Ed.), The new nurse educator: Mas-tering academe (pp. 247–248). New York, NY: Springer Publishing.
130. Jeffreys, M. R. (2014). Student retention and success: Optimizing outcomes through HOLISTIC COMPETENCE and proactive inclusive enrichment (PIE). Teaching and Learning in Nursing, 9(4), 164–170.
131. Jeffreys, M. R. (2015). Jeffreys’s Nursing Universal Retention and Success (NURS) Model: Overview and action ideas for optimizing outcomes A-Z. Nurse Education Today, 35, 425–431.

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
36 I GETTING STARTED
132. Hunt, D. D. (2013). The new nurse educator: Mastering academe. New York, NY: Springer Publishing.
133. Hallmark, B. F., Thomas, C. M., & Gantt, L. (2014). The educational practices construct of the NLN/Jeffries framework: State of the science. Clinical Simulation in Nursing, 10, 345–352.
134. Ramirez, C. (2009). Latino nursing career opportunity program: A project designed to increase the number of Latino nurses. In S. D. Bosher & M. D. Pharris (Ed.), Transform-ing nursing education: The culturally inclusive environment (pp. 313–327). New York, NY: Springer Publishing.
135. Heller, B. R., Oros, M. T., & Durney-Crowley, J. (2000). The future of nursing educa-tion: 10 trends to watch. Nursing and Health Care Perspectives, 21(1), 9–13.
136. Bond, M. L., Gray, J. R., Baxley, S., Cason, C. L., & Denke, L. (2008). Voices of Hispanic students in baccalaureate nursing programs: Are we listening? Nursing Education Perspectives, 29(3), 136–142.
137. Seidman, A. (2005). College student retention: Formula for student success. Westport, CT: Praeger.
138. Seidman, A. (2007). Minority student retention: The best of the Journal of College Student Retention: Research, theory, and practice. Amityville, NY: Baywood.
139. Bessent, H. (Ed.). (1997). Strategies for recruitment, retention, and graduation of minority nurses in colleges of nursing. Washington, DC: American Nurses Publishing.
140. Mills-Wisneski, S. M. (2003). African-American baccalaureate nursing students’ per-ceptions of nursing programs and factors that support or restrict academic success. (Doctoral dissertation, Widener University, 2003.) UMI Dissertation Service, 3083001.
141. Gardner, J. (2005). Barriers influencing the success of racial and ethnic minority stu-dents in nursing programs. Journal of Transcultural Nursing, 16(2), 155–162.
142. Gilchrist, K. L., & Rector, C. (2007). Can you keep them? Strategies to attract and retain nursing students from diverse populations: Best practices in nursing educa-tion. Journal of Transcultural Nursing, 18(3), 277–285.
143. DeLapp, T., Hautman, M. A., & Anderson, M. S. (2008). Recruitment and retention of Alaska natives into nursing (RRANN). Journal of Nursing Education, 47(7), 293–297.
144. Evans, B. C. (2008). “Attached at the umbilicus”: Barriers to educational success for Hispanic/Latino and American Indian nursing students. Journal of Professional Nursing, 24, 205–217.
145. Ackerman-Barger, P. W. (2010). Embracing multiculturalism in nursing learning envi-ronments. Journal of Nursing Education, 49(12), 677–682.
146. Bean, J. P., & Metzner, B. (1985). A conceptual model of nontraditional undergraduate student attrition. Review of Educational Research, 55, 485–540.
147. Braxton, J. M. (Ed.). (2000). Reworking the student departure puzzle. Nashville, TN: Vanderbilt University Press.
148. Dowell, M. A. (1996). Issues in recruitment and retention of minority nursing stu-dents. Journal of Nursing Education, 35(7), 293–297.
149. Levin, M. E., & Levin, J. R. (1991). A critical examination of academic retention programs for at-risk minority college students. Journal of College Student Development, 32, 322–334.
150. Manifold, C., & Rambur, B. (2001). Predictors of attrition in American Indian nursing students. Journal of Nursing Education, 40(6), 279–281.
151. Metzner, B., & Bean, J. P. (1987). The estimation of a conceptual model of nontradi-tional undergraduate student attrition. Research in Higher Education, 27, 15–38.
152. Yurkovich, E. E. (2001). Working with American Indians toward educational success. Journal of Nursing Education, 40(6), 259–269.
153. Jeffreys, M. R. (1993). The relationship of self-efficacy and select academic and environmen-tal variables on academic achievement and retention. Doctoral dissertation. Unpublished manuscript. New York, NY: Teachers College, Columbia University.
This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
1 OVERVIEW OF KEY ISSUES AND CONCERNS 37
154. Jeffreys, M. R. (2001). Evaluating enrichment program study groups: Academic out-comes, psychological outcomes, and variables influencing retention. Nurse Educator, 26(3), 142–149.
155. Jeffreys, M. R. (2002). Students’ perceptions of variables influencing retention: A pre-test and post-test approach. Nurse Educator, 27(1), 16–19. [Erratum, 2002, 27(2), 64].
156. Jeffreys, M. R. (2003). Strategies for promoting nontraditional student retention and success. In M. Oermann & K. Heinrich (Eds.), Annual review of nursing education (Vol. I, pp. 61–90). New York, NY: Springer Publishing.
157. Jeffreys, M. R. (2004). Nursing student retention: Understanding the process and making a difference. New York, NY: Springer Publishing.
158. Jeffreys, M. R. (2007). Nontraditional students’ perceptions of variables influencing retention: A multi-site study. Nurse Educator, 32(4), 161–167.
159. Jeffreys, M. R. (2007). Tracking students through program entry, progression, gradua-tion, and licensure: Assessing undergraduate nursing student retention and success. Nurse Education Today, 27, 406–419.
160. Jeffreys, M. R. (1998). Predicting nontraditional student retention and academic achievement. Nurse Educator, 23(1), 42–48.
161. Jeffreys, M. R. (1995). Joining together family, faculty, and friends: New ideas for en-hancing nontraditional student success. Nurse Educator, 20(3), 11.
162. Jeffreys, M. R. (2004). Nursing student retention: Understanding the process and making a difference. New York, NY: Springer Publishing.
163. Constantine, M. G., & Watt, S. K. (2002). Cultural congruity, womanist identity at-titudes, and life satisfaction among African American college women attending historically black and predominantly white institutions. Journal of College Student De-velopment, 43(2), 184–193.
164. Constantine, M. G., Robinson, J. S., Wilton, L., & Caldwell, L. D. (2002). Collec-tive self-esteem and perceived social support as predictors of cultural congruity among Black and Latino college students. Journal of College Student Development, 43(3), 307–316.
165. Gloria, A. M., & Kurpius, S. E. R. (1996). The validation of the cultural congruity scale and the university environment scale with Chicano/a students. Hispanic Journal of Behavioral Sciences, 18(4), 533–549.
166. Leininger, M. M. (1994). Transcultural nursing: Concepts, theories, and practices. Columbus, OH: Greyden Press.
167. Leininger, M. M. (2002). Essential transcultural nursing care concepts, principles, examples, and policy statements. In M. M., Leininger & M. R., McFarland (Eds.), Transcultural nursing: Concepts, theories, research, and practice (3rd ed., pp. 45–69). New York, NY: McGraw-Hill.
168. Johnson, S. A., & Johnson, L. J. (2008). Second-degree, entry-into-practice master’s of nursing program: Lessons learned. Nurse Educator, 33(5), 228–232.
169. Hegge, M. J., & Hallman, P. A. (2008). Changing nursing culture to welcome second-degree students: Herding and corralling sacred cows. Journal of Nursing Education, 47(12), 552–556.
170. Bellack, J. P. (2009). Integrating diversity. Journal of Nursing Education, 48(9), 475–476.171. Crow, K. (1993). Multiculturalism and pluralistic thought in nursing education: Na-
tive American world view and the nursing academic world view. Journal of Nursing Education, 32(5), 198–204.
172. Davidhizar, R., Dowd, S. B., & Giger, J. N. (1998). Educating the culturally diverse healthcare student. Nurse Educator, 23(2), 38–42.
173. Labun, E. (2002). The Red River College Model: Enhancing success for native Canadian and other nursing students from disenfranchised groups. Journal of Trans-cultural Nursing, 13(4), 311–317.
This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
38 I GETTING STARTED
174. Rew, L. (1996). Affirming cultural diversity: A pathways model for nursing faculty. Journal of Nursing Education, 35(7), 310–314.
175. Sommer, S. (2001). Multicultural nursing education. Journal of Nursing Education, 40(6), 276–278.
176. Weaver, H. N. (2001). Indigenous nurses and professional education: Friends or foes? Journal of Nursing Education, 40(6), 252–258.
177. Williams, R. P., & Calvillo, E. R. (2002). Maximizing learning among students from culturally diverse backgrounds. Nurse Educator, 27(5), 222–226.
178. Oermann, M. H. (2015). Teaching in nursing and role of the nurse educator: The complete guide to best practice in teaching, evaluation, and curriculum development. New York, NY: Springer Publishing.
179. Jeffreys, M. R. (2000). Development and psychometric evaluation of the Transcultural Self-Efficacy Tool: A synthesis of findings. Journal of Transcultural Nursing, 11(2), 127–136.
180. Jeffreys, M. R., & Smodlaka, I. (1998). Exploring the factorial composition of the Transcultural Self-Efficacy Tool. International Journal of Nursing Studies, 35, 217–225.
181. Jeffreys, M. R., & Smodlaka, I. (1999). Changes in students’ transcultural self-efficacy perceptions following an integrated approach to culture care. Journal of Multicultural Nursing and Health, 5(2), 6–12. [Erratum, 2000, 6(1), 20].
182. Jeffreys, M. R., & Smodlaka, I. (1999). Construct validation of the Transcultural Self-Efficacy Tool. Journal of Nursing Education, 38, 222–227.
183. Lim, J., Downie, J., & Nathan, P. (2004). Nursing students’ self-efficacy in providing transcultural care. Nurse Education Today, 24(6), 428–434.
184. Jeffreys, M. R., & Dogan, E. (2013). Evaluating cultural competence in the clinical practicum. Nursing Education Perspectives, 34(2), 88–94.
185. Jeffreys, M. R., & Dogan, E. (2012). Evaluating the influence of cultural competence education on students’ transcultural self-efficacy perceptions. Journal of Transcultural Nursing, 23(2), 188–197.
186. Jeffreys, M. R., & Dogan, E. (2010). Factor analysis of the Transcultural Self-Efficacy Tool (TSET). Journal of Nursing Measurement, 18(2), 120–139.
187. Billings, D., & Kowalski, K. (2008). Inclusive teaching. Journal of Continuing Education in Nursing, 39(7), 296–297.
188. Jalili-Grenier, F., & Chase, M. M. (1997). Retention of nursing students with English as a second language. Journal of Advanced Nursing, 25, 199–203.
189. Flege, J. E., & Liu, S. (2001). The effects of experience on adults’ acquisition of a sec-ond language. Studies in Second Language Acquisition, 23(4), 527–552.
190. Fuertes, J. N., & Westbrook, F. D. (1996). Using the social, attitudinal, familial, and environmental (S.A.F.E.) acculturation stress scale to assess the adjustment needs of Hispanic college students. Measurement and Evaluation in Counseling and Development, 29, 67–76.
191. Kataoka-Yahiro, M. R., & Abriam-Yago, K. (1997). Culturally competent teaching strategies for Asian nursing students for whom English is a second language. Journal of Cultural Diversity, 4(3), 83–87.
192. Kurz, J. M. (1993). The adult ESL baccalaureate nursing student. Journal of Nursing Education, 32(5), 227–229.
193. Olenchak, F. R., & Hebert, T. P. (2002). Endangered academic talent: Lessons learned from gifted first-generation college males. Journal of College Student Development, 43(2), 195–212.
194. Smart, J. F., & Smart, D. W. (1995). Acculturative stress: The experience of the His-panic immigrant. The Counseling Psychologist, 23, 25–42.
195. Upton, T. A., & Lee-Thompson, L-C. (2001). The role of the first language in second language reading. Studies in Second Language Acquisition, 23(4), 469–495.

This is sample from Teaching Cultural Competence in Nursing and Health CareVisit This Book’s Web Page / Buy Now / Request an Exam/Review
© Springer Publishing Company
1 OVERVIEW OF KEY ISSUES AND CONCERNS 39
196. Sweet, S., & Fusner, S. (2008). Social integration of the advanced placement LPN: A peer mentoring program. Nurse Educator, 33(5), 202–205.
197. Penprase, B., & Koczara, S. (2009). Understanding the experiences of accelerated second-degree nursing students and graduates: A review of the literature. Journal of Continuing Education in Nursing, 40(2), 74–78.
198. Hammer, V. R., & Craig, G. P. (2008). The experiences of inactive nurses returned to nursing after completing a refresher course. Journal of Continuing Education in Nursing, 39(8), 358–367.
199. Lavoie-Tremblay, M., Wright, D., Desforges, N., Gelinas, C., Marchionni, C., & Drevniok, U. (2008). Creating a healthy workplace for new-generation nurses. Journal of Nursing Scholarship, 40(3), 290–297.
200. Zalon, M. L. (2008). Using technology to build community in professional associa-tions. The Journal of Continuing Education in Nursing, 39(5), 235–240.
201. Johnson, S. A., & Romanello, M. L. (2005). Generational diversity: Teaching and learn-ing approaches. Nurse Educator, 30(5), 212–216.
202. Mangold, K. (2007). Educating a new generation: Teaching baby boomer faculty about millennial students. Nurse Educator, 32(1), 21–23.
203. Hendricks, J. M., & Cope, V. C. (2012). Generational diversity: What nurse managers need to know. Journal of Advanced Nursing, 69(3), 717–725.
204. Yoder-Wise, P. S. (2009). State and certifying boards/associations: CE and compe-tency requirements. Journal of Continuing Education in Nursing, 40(1), 3–11.
205. Bandura, A. (1986). Social foundations of thought and action: A social cognitive theory. Englewood Cliffs, NJ: Prentice-Hall.





























