Embed Size (px)
Citation preview

Large Molecule Therapeutics
Targeting Aberrant DNA Double-Strand Break Repair inTriple-Negative Breast Cancer with Alpha-Particle EmitterRadiolabeled Anti-EGFR Antibody
Hong Song1, Mohammad Hedayati2, Robert F. Hobbs1, Chunbo Shao3, Frank Bruchertseifer5,Alfred Morgenstern5, Theodore L. DeWeese2,4, and George Sgouros1,4
AbstractThe higher potential efficacy of alpha-particle radiopharmaceutical therapy lies in the 3- to 8-fold greater
relative biological effectiveness (RBE) of alpha particles relative to photon or beta-particle radiation. This
greater RBE, however, also applies to normal tissue, thereby reducing the potential advantage of high RBE. As
alpha particles typically cause DNA double-strand breaks (DSB), targeting tumors that are defective in DSB
repair effectively increases the RBE, yielding a secondary, RBE-based differentiation between tumor and
normal tissue that is complementary to conventional, receptor-mediated tumor targeting. In some triple-
negative breast cancers (TNBC; ER�/PR�/HER-2�), germlinemutation in BRCA-1, a key gene in homologous
recombination DSB repair, predisposes patients to early onset of breast cancer. These patients have few
treatment options once the cancer hasmetastasized. In this study,we investigated the efficacy of alpha-particle
emitter, 213Bi-labeled anti-EGF receptor antibody, cetuximab, inBRCA-1–defectiveTNBC. 213Bi-cetuximabwas
found to be significantly more effective in the BRCA-1–mutated TNBC cell line HCC1937 than BRCA-1–
competent TNBC cell MDA-MB-231. siRNA knockdown of BRCA-1 or DNA-dependent protein kinase,
catalytic subunit (DNA-PKcs), a key gene in non–homologous end-joining DSB repair pathway, also sensitized
TNBC cells to 213Bi-cetuximab. Furthermore, the small-molecule inhibitor of DNA-PKcs, NU7441, sensitized
BRCA-1–competent TNBC cells to alpha-particle radiation. Immunofluorescent staining of g-H2AX foci and
comet assay confirmed that enhanced RBE is caused by impaired DSB repair. These data offer a novel strategy
for enhancing conventional receptor-mediated targeting with an additional, potentially synergistic radio-
biological targeting that could be applied to TNBC. Mol Cancer Ther; 12(10); 2043–54. �2013 AACR.
IntroductionRadioimmunotherapy of established large solid tumors
has not achieved clinical success (1, 2), partly becauseradiolabeled antibodies are not able to penetrate anddeliver sufficient doses (typically less than 30 Gy) to elicitresponses (3, 4). Accordingly, radioimmunotherapy ofsolid tumors is best implemented when the tumor size issmall or, ideally, at a very early stage when the tumors arestill microscopic clusters of malignant cells (5, 6). In con-trast, in patients with non–Hodgkin lymphoma, equiva-lent or even lower tumor doses are able to elicit objective
responses (7). Several factors contribute to this differentialresponse; these include the unique biologic efficacy of anti-CD20 antibody, uniform and high expression of the CD20antigen, and the easy accessibility of lymphoma cells toradiolabeled antibodies (8). More importantly, comparedwith solid tumors, non–Hodgkin lymphoma cells areexquisitely sensitive to radiation with typical D0 values inthe range of 1.3 to 1.8 Gy without an appreciable shoulderon the survival curves (9). Genetic analysis has revealedthat the increased radiosensitivity of non–Hodgkin lym-phoma cells can be attributed to impairedDNA repair dueto inactivation of ataxia-telangiectasia mutated kinase(ATM), p53 and DNA-PKcs genes (10).
Solid tumors are often associated with defects in theDNAdamage response (DDR) pathways and loss-of-func-tion in DDR. Germline mutations in these genes causegenomic instability and predispose patients to the devel-opment of cancer (11). For example, 5% to 10% of hered-itary breast cancer (12), 10% to 15% of ovarian cancer (13),and 5% to 10% of pancreatic cancers (14) are caused bymutations in BRCA-1/2, key genes involved in DSB repairresponses. Familial form of colorectal cancer (about 3%–4%), hereditarynon–polyposis colorectal cancer (HNPCC),is associated with defective mutations in DNA mismatch
Authors' Affiliations: 1Division of Nuclear Medicine, Russell H. MorganDepartment of Radiology andRadiological Science, Departments of 2Radi-ation Oncology and Molecular Radiation Sciences, and 3Otolaryngology-Head and Neck Surgery, 4Sidney Kimmel Comprehensive Cancer Center,Johns Hopkins University School of Medicine, Baltimore, Maryland; and5European Commission, Joint Research Centre, Institute for TransuraniumElements, Karlsruhe, Germany
Corresponding Author: George Sgouros, The Johns Hopkins UniversitySchool of Medicine, Rm 4M61 Cancer Research Building II, 1550 OrleansStreet, Baltimore, MD 21231. Phone: 410-614-0116; Fax: 413-487-3753;E-mail: [email protected]
doi: 10.1158/1535-7163.MCT-13-0108
�2013 American Association for Cancer Research.
MolecularCancer
Therapeutics
www.aacrjournals.org 2043
on May 27, 2018. © 2013 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst July 19, 2013; DOI: 10.1158/1535-7163.MCT-13-0108

repair genes, such as MSH2 and MLH1 (15). In glioblas-toma, promoter methylation on O6-methylguanine-DNAmethyltransferase (MGMT) gene in base alkylation rever-sion repair was found in 40% of patients and is a reliablepredictor for clinical outcome (16).
The differential DDR between normal tissue cellswith intact DNA repair and repair-defective tumors cellscan be used to further enhance the efficacy of highlypotent alpha-particle radiopharmaceutical therapy. Alphaparticles travel a short distance (<100 mm) and deposithighly focused energy along their tracks (80 keV/mm)enabling a single track to generate DSB (17). Eukaryoticcells can repair DSBs through two main pathways, homo-logous recombination (HR) and non–homologous endjoining (NHEJ; ref. 18). Here, we hypothesized that tar-geted alpha-particle radiation is more effective againstsolid tumors that contain somatic loss-of-function muta-tions in genes involved in HR and NHEJ pathways andexamined the feasibility of radiobiological targeting thatmay complement or synergizewith conventional receptor-mediated targeting. The BRCA-1–defective triple-negativebreast cancer (TNBC) model was used to evaluate thisapproach.
Breast cancer is a heterogeneous disease where tumorsdisplay highly varied histopathologic features, geneexpression profiles, response to therapy, and prognosiseven though they arise from the same organ. Studies ingenome-wide gene expression profiles have establishedfour breast cancer types: luminal (type A and B), HER-2–positive, normal breast–like, and basal-like (19). Amongthe four types of breast cancer, basal-like breast cancersconstitute approximately 15% of all breast cancers and aretypically ER�, PR�, and HER-2�. TNBC is poorly differ-entiated and highly aggressive; patients with TNBC arealmost twice as likely as other patients with breast cancerto developdistantmetastasis and, therefore, suffer shortersurvival (20). BRCA-1–defective tumors often belong toTNBC and share many clinical and pathologic features(21). Importantly, most TNBCs have high expression ofEGF receptor (EGFR; ref. 22) making it an ideal target foralpha radioimmunotherapy.
Our previous studies have shown that alpha-particleemitter, 213Bi-labeled, anti-ratHER-2/neumonoclonal anti-body 7.16.4 prolongs the survival ofHER-2/neu transgenicmice (neuN) bearing syngeneic breast cancer bone metas-tasis and lungmetastasis butdidnot lead to cure (23, 24). Inthis study, we first evaluated the efficacy of alpha emitter213Bi-labeled anti-EGFRmonoclonal antibody (cetuximab)in TNBC cells with mutated BRCA-1. Then, we testedinhibition of DNA-dependent protein kinase, catalyticsubunit (DNA-PKcs), a key enzyme in the NHEJ pathway,to sensitize 213Bi-cetuximab.
Materials and MethodsBreast cancer cell lines and reagents
Four humanTNBC cell lines,MDA-MB-231,MDA-MB-436, MDA-MB-468, HCC1937 (BRCA-1–defective), and a
control cell lineMCF-7 (ERþ, PRþ, HER-2�)were obtainedfrom the American Type Culture Collection (ATCC). Thecell lines were authenticated and tested by ATCC usingshort tandem repeat profiling and karyotyping tests. Thecell lineswere grown inRPMI-1640media containing 10%FBS, 0.5% penicillin/streptomycin (Invitrogen), 1% L-glu-tamine, 1% nonessential amino acids, 1% sodium pyru-vate, 0.02% gentamicin, and 0.2% insulin (Sigma) andmaintained at 37�C in 5% CO2. Anti-human EGFR mono-clonal antibody, cetuximab, was obtained from Eli Lilly &Co. under a Material Transfer Agreement. Anti-humanphospho-Histone H2AX (Ser139) monoclonal antibodywas purchased from Millipore. Alexa Fluor 488–conju-gated goat anti-mouse antibody was purchased fromInvitrogen. DNA-PKcs inhibitor NU7441 was purchasedfrom Tocris Bioscience.
Antibody radiolabeling with 213Bi and 111InCetuximab was conjugated to SCN-CHX-A00-DTPA as
described earlier (23). 225Ac was provided by the InstituteforTransuraniumElements (Karlsruhe,Germany; refs. 25,26) and 213Bi was eluted from an 225Ac/213Bi generatorbuilt in-house (27). Cetuximab conjugated to the chelatewas incubated with 213Bi (10 mCi/mg) for 8 minutes in areaction buffer (pH 4.5) containing 3 Mol/L ammoniumacetate (Fisher Scientific) and 150 mg/mL L-ascorbic acid(Sigma) preheated to 37�C. The radiolabeling reactionwasquenched with 1 mL of 100 mmol/L EDTA and radiola-beled cetuximab was purified by size-exclusion Micro-spin G-25 column (GE Healthcare). Cetuximab was alsoradiolabeled with 111In (PerkinElmer) according to apublished procedure (28). The reaction efficiency andpurity of the radioimmunoconjugates was determinedwith instant thin layer chromatography (ITLC) usingsilica gel impregnated paper (Agilent Technologies). Theimmunoreactivity of 13Bi-cetuximab was evaluated byincubating 5 ng of 213Bi-cetuximab with excess antigenbinding sites (1� 107MDA-MB-231 cells) twice on ice for30 minutes each time. Antibody immunoreactivity wascalculated as the percentage of 213Bi-cetuximab bound tothe cells.
EGFR expression measured by flow cytometry andScatchard analysis
Expression of EGFR on the four TNBC cells wasdetermined by fluorescein isothiocynate (FITC)-labeledcetuximab using FACSCalibur (Becton Dickinson Bios-ciences). The EGFR expression level was also quantifiedby Scatchard analysis. Briefly, 1 � 106 cells were incu-bated with serial dilutions of 111In-cetuximab (0.01 to 4.0mg/mL) for 45 minutes at 4�C. Cells were washed withPBS three times before both cell pellets and supernatantswere collected and counted with a gamma counter(CompuGamma CS, Pharmacia). The equilibrium-bind-ing curve of bound/free antibody versus bound anti-body concentrationwas fitted and the number of bindingsites, Bmax, and antibody dissociation constant, KD, werecalculated.
Song et al.
Mol Cancer Ther; 12(10) October 2013 Molecular Cancer Therapeutics2044
on May 27, 2018. © 2013 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst July 19, 2013; DOI: 10.1158/1535-7163.MCT-13-0108

siRNA knockdown of BRCA-1, DNA-PKcs, andRT-PCRThe siRNA knockdown studies are carried out mainly
to account for impact of the receptor number and cell sizeson cell survival after DSB induction by radiolabeled anti-body. siRNAs targeting BRCA-1 and DNA-PKcs as wellas nontargeting scrambled siRNA were obtained fromAmbion. Twenty-four hours before transfection, TNBCcells were plated into 24-well plates at a density of 5 �104 cells per well in cell culture media without antibiotics.Cells were transfected with Lipofectamine (Invitrogen) inOPTI-MEMmedia (Invitrogen) at a siRNAconcentrationof20 pmol/well (add 100 mL of siRNA:Lipofectamine 2000complexes to 0.5 mL medium). Forty-eight hours aftertransfection, breast cancer cells were examined for knock-down of gene expression by real time reverse transcription(RT)PCR.Total cellularRNAwas isolatedwithPerfectPureRNA Cultured Cell Kit (5 Prime) according to the manu-facturer’s instruction.For cDNAsynthesis, 1mgofRNAwasreverse transcribed using qScript cDNA Synthesis Kit(Quanta Bioscience). BRCA-1 and DNA-PKcs mRNA levelwere measured by quantitative real-time RT-PCR usingSYBR Green PCR Master Mix on an ABI Prism 7900HTSequence Detection System (Applied Biosystems). The pri-mers for BRCA-1 are: forwardGGCTATCCTCTCAGAGT-GACATTTTA, reverse GCTTTATCAGGTTATGTTGCATGGT; forDNA-PKcs are: forwardCCACTTACAGGATC-ATAGCGACGAATGC, reverse CGTGCGGGTAGTTAT-CAGTGATTT. b-Actin mRNA level was used as controland the primers are: forwardACCAACTGGGACGACAT-GGAG, reverse GTGAGGATCTTCATGAG GTAGTC.
Specific kill of TNBC cells by 213Bi-cetuximabSurvival curves of TNBC cells after treatment with
213Bi-cetuximab were measured by colony formationassay. The four TNBC cells and MCF-7 cells were platedin 24-well plates. Two days after cell plating, they wereincubated with 213Bi-cetuximab (concentration from 1.0–8.0 mCi/mL) overnight in duplicates and transferred toPetri dishes for colony growth. All survival curves studieswere repeated again to confirm the findings. To investi-gate the effects of BRCA-1 and DNA-PKcs on cell kill byalpha radiation, TNBCcellswere transfectedwith siRNAstargeting BRCA-1 andDNA-PKcs. Forty-eight hours aftertransfection, cells were treatedwith 213Bi-cetuximab over-night and transferred to Petri dishes for colony growth. Tocompare the effect of small-molecule inhibitor of DNA-PKcs on cell kill by alpha radiation, TNBC cells weretreated with NU7441 (1.0 mmol/L) one hour before213Bi-cetuximab treatment and cells were continuouslyincubated with NU7441 for 16 hours before they weretransferred for colony formation (29).
Immunofluorescent staining of g-H2AX foci as abiomarker for DSBsDSBs induced by 213Bi-cetuximab were measured by
immunofluorescent staining of phosphorylated histoneH2AX (g-H2AX). TNBC and MCF-7 cells were treated
with 8 mCi 213Bi-cetuximab. At various time points (20minutes, 1, 2, 4, 6, and 24 hours) after initiation of 213Bi-cetuximab treatment, cells were washed with PBS andfixed with 2% paraformaldehyde. After incubation with0.5% NP-40 to permeabilize cell membrane, g-H2AX wasdetected by mouse anti-human phosphorylated histoneH2AX (Ser139) andAlexa Fluor 488–conjugated goat anti-mouse IgG. Cell nuclei were stained with Hoechst 33342(Invitrogen). The fluorescent images were examined andcaptured by a Nikon E800 fluorescent microscopeequipped with NIS-Element software (Nikon). The num-ber of g-H2AX foci per cell was counted (>50 cells per datapoint).
For TNBC cells transfectedwith siRNA targeting eitherDNA-PKcs or BRCA-1, the number of g-H2AX fociwas counted at 1 and 24 hours after treatment with213Bi-cetuximab. In addition, to compare the effect ofsmall-molecule DNA-PKcs inhibitor NU7441 on DSBrepair after alpha radiation, TNBC cells were treated withNU7441 as described before with 213Bi-cetuximab and thenumber of g-H2AX foci was quantified at 1 and 24 hoursafter treatment.
Comet assay and cell-cycle analysisMDA-MB-231 andHCC1937 cells were incubatedwith
213Bi-cetuximab (8mCi/mL) in cell culturemedia contain-ing 2%FBS at 37�C. Cellswere harvested for comet assaysunder neutral condition at 1 or 24 hours after initiation ofincubation using the Trevigen CometAssay kit (Trevi-gen). Briefly, cells were mixed with low melting pointagarose and plated on microscope slides and allowed togel. Cells were then lysed for 1 hour at 4�C followed byrinse in TBE buffer [10.8% (w/v) Tris base, 5.5% (w/v)boric acid, and 0.93% (w/v) EDTA]. After electrophoresisin TBE buffer for 30 minutes at 1 V/cm, slides werewashed in water and dehydrated with ethanol, air driedovernight, and then treated with SYBR Green for DNAstaining. Comets were imaged using a Zeiss Imager.Z1fluorescent microscopy (Carl Zeiss AG) and analyzedusing the software CometScore (Autocomet.com). TheOlive Tail Moment (OTM) was calculated as the averageof at least 70 comets.
For cell-cycle assay, at 1 or 24 hours after 213Bi-cetuximab treatment, cells were harvested and fixedin 70% ethanol overnight. After PBS wash, cells werestained with 0.02 mg/mL propidium iodide (Sigma) in0.1% (v/v) Triton X-100/PBS containing 0.2 mg RNaseA (Sigma). Flow cytometry was conducted on a FACS-Calibur and data were analyzed with Cell Quest Pro(BD Bioscience).
Biodistribution of radiolabeled cetuximabin EGFR-positive TNBC
Nude mice (5 mice/group) were injected with 1 � 106
MDA-MB-231 cells subcutaneously in the mammary fatpad region. Tenweeks after tumor inoculation (tumor size0.5–1.0 cm in diameter), mice were injected intravenouslywith approximately 20 mCi 111In-cetuximab and were
Targeting Defective DNA DSB Repair with Alpha Radiation
www.aacrjournals.org Mol Cancer Ther; 12(10) October 2013 2045
on May 27, 2018. © 2013 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst July 19, 2013; DOI: 10.1158/1535-7163.MCT-13-0108

then sacrificed at 1, 3, 6, 24, 48, and 72 hours postinjection.Major organs, including blood, heart, lungs, liver, spleen,kidney, stomach, intestine, muscle, femur, and tumorwere collected and counted in the gamma counter. Theuptake of 111In-cetuximab in the tumor and organs wasdecay corrected to the time of injection and calculated as%ID/g � SD.
DosimetryBiodistribution data from 111In-cetuximabwere convert-
ed to 213Bi-cetuximab biodistribution based on our previ-ous findings that radioisotope properties of 111In is a goodsurrogate for 213Bi antibody kinetics (23). An exponentialexpression was fitted to the time activity data, and thecumulativeactivity in eachnormal organwas calculatedbyanalytic integration of the fitted expression. Absorbeddoses were calculated as described in the study conductedby Sgouros and colleagues (30). Absorbed dose is thus cal-
culated asD¼ (~A� Daþ ~A� De)/M,whereinD is absorb-
ed dose (no RBE adjustment), ~A is the total number ofdisintegrations in an organ or tumor,M is theweight of theorgan, and the mean energy emitted per nuclear transition
for alphaparticles,Da, andelectrons,De, is 1.33� 10�12 and1.05� 10�13 Gy kg/Bq-s, respectively. For cell level dosim-etry, the absorbed dose to the TNBC cells treated withnonbinding antibody was calculated as the absorbed doseto the irradiatedmedia volume assuming all alpha-particle
energies are absorbed locally:D ¼ DEBi2132
R t10
A0e�lt
rV0dtwhere
DEBi213 is the mean alpha-particle and electron energy perdecay (Gy-kg/Bq-s), t1 is the time of treatment, A0 is theinitial activity, r is the density of the cell (assuming waterequivalent at 1.0 g/cm3),V0 is the volume of the treatment,andl is thedecay constant for 213Bi. The absorbeddosewasdivided by two, as the cells are attached to the bottom ofthe tissue culture plates and are assumed to receive halfof the radiation from above them. The absorbed dose toEGFR-positiveTNBCcells targetedby213Bi-cetuximabwascalculated using a cellular S factor (31, 32) for 213Bi, themeasured number of EGF receptors per cell, and assum-ing receptor saturation at 1 hour after generator elution.
D ¼ SBi213;N CS
R t10 SA0Ne�ltdt, where SBi-213, N CS is the
cellular S factor, SA0 is the specific activity, and N isthe number of EGF receptors per cell. The sizes of cell andcell nuclei were measured by fluorescent microscopy
A
Co
un
ts
FL1-H
150
120
90
60
30
0
100
1
0.1
0.01
0.001
1.000
0.100
0.010
0.001
25
20
15
10
5
0
101 102
MCF-7
MDA-MB-436
MDA-MB-468
Su
rviv
ing
fra
cti
on
Su
rviv
ing
fra
cti
on
Olive m
om
en
t
HCC1937
1032 4 6 80 10
2 4 6 8 100 12
104
B
C
E
D
MDA-MB-231
MCF-7
MDA-MB-436
MDA-MB-468
HCC1937
MDA-MB-231
MCF-7
MDA-MB-436
MDA-MB-468
HCC1937
HCC1937
MDA-MB-231
HCC1937
Control
HCC1937
Cetuximab-Bi213
MDA-MB-231
Control
MDA-MB-231
Cetuximab-Bi213
MDA-MB-231
1 h
24
h
1 h neutral24 h neutral
1 h
24
h
Control 213Bi-Cetuximab
Cetuximab-Bi213 (μμCi/mL)
*
Cs-137 irradiator (Gy)
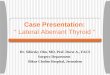
Figure 1. Radiosensitivity of TNBCcell lines. A, flow cytometry foundhigh expression of EGFR in all fourTNBC cells (MDA-MB-231, MDA-MB-436, HCC1937, MDA-MB-468). MCF-7 cells have very low-level expression of EGFR andwereused as negative control in thestudies. B, cell survival curves ofTNBC cells and MCF-7 cells aftertreatment by 137Cs (gamma)radiation. BRCA-1–defectiveHCC1937 was found to be themost radiosensitive cell line. MDA-MB-468 cells are also relativelysensitive to 137Cs radiation whendelivered at 0.5 Gy per minute. C,cell survival curves of TNBC cellsandMCF-7 cells after treatment byalpha-particle emitter–labeled213Bi-cetuximab. BRCA-1–defective HCC1937 cells are moresensitive to 213Bi-cetuximabcompared with MDA-MB-231 andMDA-MB-436 cells. MDA-MB-468cells are the most sensitive amongthe TNBC cells treated. D, DNAdamage caused by 213Bi-cetuximab at 1hour after treatmentand DNA damage repair at 24hours after treatment in MDA-MB-231 and HCC937 cells asassessed by neutral Comet assay.Representative images showinghead and tail fluorescentintensities of MDA-MB-231 andHCC1937 cells. E, quantification ofcomet tail Olive moments at 1 and24 hours after treatments.
Song et al.
Mol Cancer Ther; 12(10) October 2013 Molecular Cancer Therapeutics2046
on May 27, 2018. © 2013 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst July 19, 2013; DOI: 10.1158/1535-7163.MCT-13-0108

(Nikon 80i) and analyzed with NIS-Element imaginganalysis software (Nikon) after cells were stained withHoechst 33342 (Invitrogen). Cell and nucleus radiusof MDA-MB-231 cell were measured as 9.2 � 0.8 and6.4 � 0.8 mm, respectively.
Statistical analysisThe statistical significance of differences between two
groupswasanalyzedusingMedCalc (MedCalc. Software).Differences with P values < 0.05 were considered statisti-cally significant.
ResultsEGFR expression, radiolabeling, and antibodyimmunoreactivityFlow cytometry with cetuximab-FITC found EGFR
expression on all four TNBC cell lines, but not onMCF-7 cells (Fig. 1A). MDA-MB-468 had the highestexpression level. The results of Scatchard analysis using111In-cetuximab are shown in tabular form in Table 1,with increased EGFR expression on MDA-MB-436,MDA-MB-231, HCC1937, and MDA-MB-468 cells. Alsoshown on Table 1 are the KD values of radiolabeledcetuximab for these cell lines, which are similar to valuesobtained with unlabeled antibody. Reaction efficiencyand purity after size exclusion purification of 213Bi-labeled cetuximab was 93.5% � 1.7% (n ¼ 7) and97.2% � 0.4% (n ¼ 4) as determined by ITLC. Bothreaction efficiency and purity of 111In-labeled Cetuxi-mab were routinely more than 98%. The fraction of213Bi-cetuximab that is able to bind MDA-MB-231 cellsin the immunoreactivity assay was 89.7%.
In vitro cytotoxicity of 213Bi-cetuximab to TNBCcells and immunofluorescent staining of g-H2AX
213Bi-cetuximabkills EGFR-expressingTNBCcells effec-tively (Fig. 1C). The activity concentrations that can kill50% (ED50) of MDA-MB-231 and MDA-MB-436 cells are3.2 and 3.5 mCi/mL, compared with 7.8 mCi/mL in EGFR-negative MCF-7 cells. Noticeably, the radiosensitivity ofBRCA-1–defective HCC1937 cells to 213Bi-cetuximab issignificantly enhanced with an ED50 of 0.63 mCi/mL.MDA-MB-468 cells are the most sensitive to 213Bi-cetux-imab treatment with an ED50 of 0.50 mCi/mL. Neutral
Comet assay showed that DSBs are repaired in MDA-MB-231 cells but not in BRCA-1–defective HCC1937 cellsat 24 hours after treatment (Fig. 1D). Two-way ANOVAtest showed significant decrease inOlivemoment inMDA-MB-231 cells from 1 to 24 hours (�, P < 0.0001) but not inHCC1937 cells (P¼ 0.88). The difference in Olive momentbetween MDA-MB-231 and HCC1937 cells is also statisti-cally significant at 1 hour (P ¼ 0.02) and 24 hour (P <0.001; Fig. 1E). Pretreating TNBC cells with the DNA-PKcsinhibitor NU7441 (1.0 mmol/L) further improved the effi-cacy of 213Bi-cetuximab for TNBC cells (Fig. 2A–C), withED50 of 0.61, 0.77, 0.58 mCi/mL for MDA-MB-231, MDA-MB-436, and HCC1937 cells, respectively.
Immunofluorescent staining of g-H2AX at 1 and 24hours after treatment with 213Bi-cetuximab is shown
Table 1. Dissociation constant (KD) andreceptor density for the cell lines used in thisstudy
Cell line KD (nmol/L) EGFR/cell
MDA-MB-231 0.8 2.8 � 105
MDA-MB-436 0.2 0.8 � 105
HCC1937 0.8 4.5 � 105
MDA-MB-468 2.0 2.7 � 106
A
B
C
1.00
0.10
0.01
Su
rviv
ing
fra
cti
on
1.00
0.10
0.01
Su
rviv
ing
fra
cti
on
2 4 6 8 100 12
MDA-MB-231
Cetuximab-Bi213
Cetuximab-Bi213 + NU7441
MDA-MB-436
Cetuximab-Bi213
Cetuximab-Bi213 + NU7441
Cetuximab-Bi213
Cetuximab-Bi213 + NU7441
Cetuximab-Bi213 (μμCi/mL)
0 2 4 6 8 10 12
Cetuximab-Bi213 (μCi/mL)
0 2 4 6 8 10 12
Cetuximab-Bi213 (μCi/mL)
HCC1937
1.000
0.100
0.010
0.001
Su
rviv
ing
fra
cti
on
Figure 2. DNA-PKcs inhibitor NU7441 enhances cytotoxicity of 213Bi-cetuximab in TNBC cells. Cell survival curves of MDA-MB-231 (A),MDA-MB-436 (B), and HCC1937 (C) after treatment by 213Bi-cetuximabor 213Bi-cetuximab plus NU7441.
Targeting Defective DNA DSB Repair with Alpha Radiation
www.aacrjournals.org Mol Cancer Ther; 12(10) October 2013 2047
on May 27, 2018. © 2013 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst July 19, 2013; DOI: 10.1158/1535-7163.MCT-13-0108

in Fig. 3. Unlike random g-H2AX foci that are usuallyformed after the cells are irradiated with gamma rays(data not shown), the g-H2AX foci typically formednoticeable straight-line tracks within cell nuclei after
treatment by 213Bi-cetuximab, indicating DSBs caused byalpha-particle tracks (e.g., Fig. 3A). The time course ofg-H2AX foci formation after alpha radiation treatmentwas evaluated at 20 minutes, 1, 2, 4, 6, and 24 hours after
A
B
1 h 24 h
1 h
Nu
mb
er
of
γγ-H
2A
X f
oci
50
40
30
20
10
0
24 h
*
1 h NU7441 24 h NU7441
1 h 24 h
MCF-7
MDA-MB-436
MDA-MB-468
HCC1937
MDA-MB-231
NU7441 NU7441
NU7441 NU7441
NU7441 NU7441
NU7441 NU7441
NU7441 NU7441
MCF-7 MCF-7 MCF-7 MCF-7
MDA-MB-436 MDA-MB-436 MDA-MB-436 MDA-MB-436
MDA-MB-468 MDA-MB-468 MDA-MB-468 MDA-MB-468
HCC1937 HCC1937 HCC1937
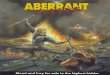
MDA-MB-231 MDA-MB-231 MDA-MB-231 Figure 3. A, representative imagesshowing immunofluorescentlystained g-H2AX foci at 1 and 24hours after treatment with 213Bi-cetuximab or 213Bi-cetuximabplusNU7441 in MCF-7 and the fourTNBC cell lines studied. B,quantification of number ofg-H2AX foci at 1 and 24 hours aftertreatment by 213Bi-cetuximab or213Bi-cetuximab plus NU7441.Two-way ANOVA test showed thatthere was a statistically significantdecrease (�) of DSBs foci in MDA-MB-231 (P < 0.001), MDA-MB-436(P < 0.001), and MCF-7 (P < 0.001)cells from 1 to 24 hours aftertreatment with 213Bi-cetuximabalone,whereas such decreasewasnot observed in HCC1937 (P ¼0.13) and MDA-MB-468 (P ¼ 0.63)cells. NU7441 treatmentsignificantly inhibited the decreaseof g-H2AX foci from1 to 24 hours inMDA-MB-231 (P¼0.43) andMDA-MB-436 (P¼0.68) cells, but did notaffect HCC1937 and MDA-MB-468 cells.
Song et al.
Mol Cancer Ther; 12(10) October 2013 Molecular Cancer Therapeutics2048
on May 27, 2018. © 2013 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst July 19, 2013; DOI: 10.1158/1535-7163.MCT-13-0108

initiation of treatment. The number of g-H2AX foci peak-ed at 1 hour and decreased gradually thereafter (data notshown). The reduction in g-H2AX foci from 1 to 24 hourswas therefore used as a measure of DSB repair capacityafter 213Bi-cetuximab treatment. InMCF-7,MDA-MB-231,and MDA-MB-436 cells, the number of g-H2AX foci percell all decreased significantly from 15.5 � 4.8 (1 hour) to5.2 � 2.4 (24 hours), 18.7 � 4.7 (1 hour) to 10.0 � 5.1 (24hours) and 16.0 � 3.8 (1 hour) to 4.9 � 2.3 (24 hours),respectively. In contrast, in BRCA-1–defective HCC1937cells and MDA-MB-468 cells, there was no significantchange in the number of g-H2AX foci at 1 hour (22.5 �6.6 and 31.3 � 8.0) and 24 hours (20.3 � 6.5 and 33.8 �10.3; Fig. 3B), strongly suggesting compromised, if notcomplete lack of DSB repair in these two cell lines.Treatment ofMCF-7,MDA-MB-231, andMDA-MB-436
cells by the DNA-PKcs inhibitor NU7441 and 213Bi-cetux-imab abolished the significant decrease of g-H2AX focifrom 1 hour to the 24-hour period, likely a result of DSBrepair inhibition (Fig. 3). For the two cell lines alreadysensitive to 213Bi-cetuximab, HCC1937, and MDA-MB-
468, adding NU7441 to 213Bi-cetuximab did not affect thenumber of g-H2AX foci from 1 hour to 24 hours. (Fig. 3B).
siRNA knockdown of BRCA-1 or DNA-PKcsenhanced radiosensitivity of TNBC cells
Gene expression of either BRCA-1 or DNA-PKcs wasdownregulated in the four TNBC cells, MCF-7, MDA-MB-231, MDA-MB-436, and HCC1937 after transfectionof siRNA targeting either BRCA-1 or DNA-PKcs as con-firmed by real-time RT-PCR (Fig. 4A). Knockdown ofeitherDNA-PKcs or BRCA-1 improved the radiosensitiv-ity of TNBC cells to 213Bi-cetuximab. In MCF-7 cells, theED50 was reduced from 6.5 mCi/mL from control siRNAto 3.4 and 1.9 mCi/mL in cells knocked down withBRCA-1 or DNA-PKcs siRNA, respectively (Fig. 4B). InMDA-MB-231 cells treated with 213Bi-cetuximab, theED50 improved significantly from 1.8 mCi/mL in cellstransfected by negative control scrambled siRNA to 0.56mCi/mL in cells transfected by siRNA targeting BRCA-1and to 0.78 mCi/mL in cells transfected by siRNA target-ing DNA-PKcs (Fig. 4C). Likewise, siRNA knockdown of
A
B C
D E
MCF-7
MCF-7
BRCA1 siRNA DNA-PKcs siRNAControl siRNA
Perc
en
tag
e e
xp
ressio
n (
%) 120
100
80
60
40
20
0
MDA-MB-436
MDA-MB-436
HCC1937
HCC1937
MDA-MB-231
MDA-MB-231
1.00
0.10
0.01
Su
rviv
ing
fra
cti
on
1.00
0.10
0.01
Su
rviv
ing
fra
cti
on
1.00
0.10
0.01
Su
rviv
ing
fra
cti
on
2 4 6 8 100 12
Cetuximab-Bi213 (μμCi/mL)
Cetuximab-Bi213 + siRNA Control
Cetuximab-Bi213 + siRNA BRCA-1
Cetuximab-Bi213 + siRNA DNA-PKcs
Cetuximab-Bi213 + siRNA Control
Cetuximab-Bi213 + siRNA Control
Cetuximab-Bi213 + siRNA BRCA1
Cetuximab-Bi213 + siRNA DNA-PKcs
Cetuximab-Bi213 + siRNA Control
Cetuximab-Bi213 + siRNA BRCA1
Cetuximab-Bi213 + siRNA DNA-PKcs
2 4 6 8 100 12
Cetuximab-Bi213 (μCi/mL)
2 4 6 8 100 12
Cetuximab-Bi213 (μCi/mL)
2 4 6 8 100 12
Cetuximab-Bi213 (μCi/mL)
1.000
0.100
0.010
0.001
Su
rviv
ing
fra
cti
on
Figure 4. siRNA knockdown ofBRCA-1 (HR) and DNA-PKcs(NHEJ) enhances theradiosensitivity of breast cancercells. A, real-time RT-PCRconfirmed siRNA knockdown ofBRCA-1 andDNA-PKcs in MCF-7,MDA-MB-231, MDA-MB-436, andHCC1937 cells. Cell survivalcurves are shown for MCF-7 cells(B), MDA-MB-231 cells (C), MDA-MB-436 cells (D), and HCC1937cells (E) to alpha-particle radiationdelivered by 213Bi-cetuximab.
Targeting Defective DNA DSB Repair with Alpha Radiation
www.aacrjournals.org Mol Cancer Ther; 12(10) October 2013 2049
on May 27, 2018. © 2013 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst July 19, 2013; DOI: 10.1158/1535-7163.MCT-13-0108

BRCA-1 in MDA-MB-436 cells enhanced its radiosensi-tivity to 213Bi-cetxumiab with an ED50 change from 5.6 to1.4 mCi/mL (Fig. 4D). In the BRCA-1–mutated HCC1937cells, knockdown ofDNA-PKcs slightly reduced the ED50
from 0.60 to 0.53 mCi/mL, consistent with that observedin the parental cells treated with DNA-PKcs inhibitorNU7441 and 213Bi-cetuximab.
Immunofluorescent staining of g-H2AX foci confirmedthe inhibition of DSB repair in MDA-MB-231 cells trans-fectedwith siRNAtargetingDNA-PKcsorBRCA-1 (Fig. 5).Cell-cycle analysis showed that both TNBC cells, MDA-MB-231 and HCC1937, were arrested in G2–M phase aftertreatment with 213Bi-cetuximab. Inhibiting DNA-PKcs inMDA-MB-231 cells further enhanced theG2–Marrest after213Bi-cetuximab treatment (Fig. 6).
Biodistribution of 111In-cetuximab EGFR-positiveTNBC tumors
The biodistribution of 111In-cetuximab in nude micebearing a subcutaneous MDA-MB-231 tumor is shownin Fig. 7. 111In-cetuximab was cleared slowly from bloodwith an effective half-life of 40.8 hours andaccumulated in
theMDA-MB-231 tumors; %ID/g in the tumors increasedfrom 2.9 � 0.5% at 1 hour to its peak of 40.6 � 8.9% at 48hours after injection. Tumor uptake persisted at 72 hoursat 38.0 � 7.9%ID/g. Like most antibodies, liver is thenormal organ after blood with the highest uptake of21.1 � 9.5%ID/g at 1 hour. Consistent with the findingthat cetuximab does not cross react with mouse EGFR, nosignificant uptake in other normal organs was observed.Finally, 111In-cetuximab cleared slowly frommajor organswith half-life ranging from 40.8 to 173.3 hours.
DosimetryAbsorbed doses from 120 mCi 213Bi-cetuximab to nor-
mal organs are shown inTable 2. Theblood-absorbeddosefrom alpha particles is 5.23 Gy and liver has the highestnormal organ absorbed dose with 4.28 and 0.22 Gy fromalpha- and beta-particle emissions, respectively. Theseresults are consistent with our observations in other dosi-metric studies of alpha-particle emitter–labeled intactantibodies (23). The RBE for MDA-MB-231 cells based oncalculations using nonspecific and specific antibodyshowed that nonspecific 213Bi-rituximab gives an RBEof 3.8 using 37% cell survival as biologic endpoint and137Cs gamma rays as reference, whereas a similar RBE of3.7was found for 213Bi-cetuximab.WhenDSB repair genesDNA-PKcs and BRCA-1 are knocked down by siRNA, theRBEs increased significantly to 8.6 and 15.6, respectively(Table 3).
DiscussionIn this study, we showed that targeting alpha-particle
radiation (213Bi) with anti-EGFR antibody cetuximab ishighly effective in killing BRCA-1–defective TNBC cellswhere DSB repair is compromised. We further showedthat inhibiting DSB repair pathways, either the HRpathway via BRCA-1 or NHEJ pathway via DNA-PKcs,preferentially sensitizes breast cancer cells with intactDSB repair function to alpha particles. Thus, similarto the concept of prescreening HER-2–positive breastcancer before treatment with trastuzumab, one couldenvision, in the era of cancer genomics, prescreeningbreast tumors with loss-of-function mutations in DSBrepair genes would increase the efficacy of targetedalpha radioimmunotherapy.
Targeted alpha-particle emitters are currently underclinical investigations for leukemia (33), ovarian cancer(34), malignant melanoma (35), and glioblastoma (36)because of their high potency. The recent clinical successof Radium-223 (Alpharadin) in castration-resistant pros-tate cancer with bone metastases (37) supports furtherdevelopment of alpha-particle emitters and highlights theimportance of a unique biologic mechanism in the highlyspecific accumulation of targeted radioisotopes. EGFR ishighly expressed on a variety of epithelial cancers, 99mTc,64Cu, 86Y, 89Zr anti-EGFR antibodies (cetuximab, panitu-mumab) have been extensively investigated as imagingagents in colorectal cancer, head and neck squamous cell
1 h 24 h
BRCA-1 siRNA BRCA-1 siRNA
DNA-PKcs siRNA DNA-PKcs siRNA
Control siRNA Control siRNA
MDA-MB-231 MDA-MB-231
MDA-MB-231 MDA-MB-231
MDA-MB-231 MDA-MB-231
Figure 5. g-H2AX immunofluorescent staining shows that knockdown ofBRCA-1 and DNA-PKcs genes inhibited the resolution of g-H2AX at 24hours in MDA-MB-231 cells.
Song et al.
Mol Cancer Ther; 12(10) October 2013 Molecular Cancer Therapeutics2050
on May 27, 2018. © 2013 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst July 19, 2013; DOI: 10.1158/1535-7163.MCT-13-0108

carcinoma (HNSCC), and lung cancer (38–40). As radio-therapeutics, anti-EGFR antibodies have been labeledwith both beta emitters 90Y and 177Lu, and alpha emitter,213Bi, and were found effective in several preclinicalmodels of HNSCC, bladder, and colorectal cancer (41,42). Few clinical trials have been launched partially due to
the prevalent expression of EGFR on normal epithelialcells that lead to skin and gastrointestinal toxicity obs-erved in cetuximab trials (43). A clinical study of intra-venous 125I-labeled anti-EGFR antibody 425 with radio-therapy in patients with glioblastoma found no survivalbenefit compared with radiotherapy alone (44). Targeting
Co
un
ts
FL2
0 200 400 600 800 1,000
FL2
0 200 400 600 800 1,000
FL2
0 200 400 600 800 1,000
FL2
0 200 400 600 800 1,000
1 h 24 h
30
02
40
18
01
20
60
0
30
02
40
18
01
20
60
0
Co
un
ts
30
02
40
18
01
20
60
0
30
02
40
18
01
20
60
0
NU7441 NU7441
MDA-MB-231 MDA-MB-231
HCC1937
Sub-G1: 1.3
G1: 57.8
G2–M: 18.2
S: 20.5
Sub-G1: 1.5
G1: 29.3
G2–M: 56.5
S: 9.5
Sub-G1: 2.2
G1: 42.3
G2–M: 33.8
S: 20.8
Sub-G1: 2.8
G1: 20.3
G2–M: 70.1
S: 5.3
HCC1937Figure 6. Cell-cycle analysisshowed alpha-particle–inducedcell-cycle arrest in G2–M phase inBRCA-1–defective HCC1937 andNU7441-treated MDA-MB-231cells.
Cetuximab-In1111 h
60
50
40
30
20
10
0
6 h
48 h
%ID
/g
3 h
24 h
72 h
MDA-MB-231 tumor
Blood Heart Lung Liver Spleen Kidney Stomach Intestine Muscle Femur Tumor
Figure 7. Biodistribution of 111In-cetuximab in nude mice (5 mice/group) bearing subcutaneousMDA-MB-231 tumors. Mice weresacrificed at 1, 3, 6, 24, 48, and72 hours after injection ofradiolabeled cetuximab. Tumoruptake of cetuximab peakedat 48 hours postinjection.
Targeting Defective DNA DSB Repair with Alpha Radiation
www.aacrjournals.org Mol Cancer Ther; 12(10) October 2013 2051
on May 27, 2018. © 2013 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst July 19, 2013; DOI: 10.1158/1535-7163.MCT-13-0108

TNBCcellswithhighEGFRexpression level anddefectiveDSB repair pathways can potentially open a therapeuticwindow that leads to clinical responses with toleratedtoxicity to normal tissues.
Tumors that have homologous loss-of-functiondefects at DSB repair pathway genes often arise fromthe normal tissues that are heterozygous and preserveDNA repair function. Nieuwenhuis and colleaguesmea-sured the rejoining of DNA breaks in normal fibroblastand lymphocytes cells with heterozygous BRCA-1/BRCA-2 mutations after X-ray radiation and found nodefect in their ability to repair DNA breaks (45). Inexternal beam radiotherapy, multiple studies were notable to link pathogenic heterozygous mutations in DDRgenes such as ATM, BRCA-1, BRCA-2, and RAD50 tonormal tissue radiosensitivity (46). These findings sug-gest that high LET alpha-particle radiation could betargeted to treat tumors with homozygous loss-of-func-tion in DNA repair while sparing normal tissues withheterozygous DNA repair genes.
In cells deficient in NHEJ and HR, we found thatcompromised repair of DSB lesions, rather than initiallyproduced DSBs by alpha-particle radiation, determines
cell survival. This is consistent with heavy ion-beamstudies. Irradiation of glioblastoma cells MO59J deficientinDNA-PKcswith heavy ion beam found no reduction ofg-H2AX foci after 21 hours (47). In Ku80-deficient (NHEJ-deficient) Chinese hamster ovary (CHO) cells treatedwithalpha particles, significantly more g-H2AX foci werepresent (58.4%–69.5%) 2 hours after radiation comparedwith normal CHO cells (36.5%–42.8%; ref. 48).
Cell survival curvesshowedthat 213Bi-cetuximab ismostefficacious in BRCA-1–defective HCC1937 cells andBRCA-1 knockdown MDA-MB-231 cells. In patients withTNBC that are not BRCA-1–defective, agents that lead toBRCA-1 inhibition combined with targeted alpha radio-therapy would be useful. Until recently, only a handfulof BRCA-1 inhibitors, however, are under early stageevaluation primarily due to low specificity, as many ofthese protein–protein interactions, unlike enzyme activesites, also have large, multiple contact points and poorlydefined topology (49). Many other DSB repair inhibitorsare currently available for combinationwith targetedalphatherapy for TNBC including the DNA-PKcs inhibitor usedin this study (29), ATM inhibitor andRad51 inhibitors (50).
PARP-1 inhibitors are also under clinical investigationfor patients with breast and ovarian cancer with BRCA-1mutations under the synthetic lethality hypothesis (21). Aphase II trial showed that PARP-1 inhibitor iniparib incombination with gemcitabine and carboplatin signifi-cantly improved progression-free survival and overallsurvival in patients with TNBC (51). The subsequentphase III trial, however, failed to confirm its survivalbenefit (52). As alpha-particle emitter radiolabeled anti-body is targeting the same DNA repair deficiency asPARP-1 inhibitors, these clinical results suggested thepotential of alpha radioimmunotherapy in patients withTNBC, but at the same time warrant more careful pre-clinical studies of, for example, the correlation of EGFRexpression level, mutation rate with their deficiency inBRCA-1, and response to alpha radiation.
An interesting observation in this study is that MDA-MB-468 cells were exquisitely sensitive to the treatment of213Bi-cetuximab, evenmore so than the BRCA-1–defectiveHCC1937 cells. One of the main reasons probably is itshigh expression of EGFR receptors (almost 10 timeshigher) comparedwith other TNBC cells lines, potentiallydelivering significantly higher alpha doses to the tumorcells. In addition, the cell survival curve with gamma raysshowed that the MDA-MB-468 cells are sensitive to radi-ation and exhibit a diminished shoulder region, consistentwith its radiosensitivity to UV radiation attributed to thedeficient RB gene and deficiency in recovery of mRNAsynthesis (53). The possible dysregulation ofDSB repair inMDA-MB-468 cells remains to be studied.
We have conducted initial in vivo evaluation of 213Bi-cetuximab in a mouse model of TNBC. Because of poortumorigenesis of the HCC1937 cells, however, we cannotinterpret the data reliably. We are currently developing amore robustmousemodel to evaluate the efficacy of alpharadioimmunotherapy in tumors with homozygous
Table 2. Tissue-absorbed doses
Absorbed dose (Gy)
Tissue a-Particle Electron
Blood 5.23 0.27Heart 1.34 0.07Lung 2.14 0.11Liver 4.28 0.22Spleen 1.21 0.06Kidney 1.15 0.06Stomach 0.37 0.02Intestine 0.66 0.03Muscle 0.19 0.01Femur 0.40 0.02
Table 3. Radiosensitivity (D0) and RBE of theMDA-MB-231cell line under different exposureand DNA repair pathway inhibition conditions
Agent, manipulationD0
(Gy) RBEa
213Bi-Rituximab (irrelevant Ab) 0.84 3.8213Bi-Cetuximab 0.87 3.7213Bi-Cetuximab, siRNA scrambled control 0.69 4.7213Bi-Cetuximab, siRNA DNA-PKcs-/DNA-PKcs-
0.37 8.6
213Bi-Cetuximab, siRNA BRCA1-/BRCA1- 0.21 15.6
aRBE is reported using 37% cell survival as the biologicendpoint andCs-137gamma rays as the reference radiation.
Song et al.
Mol Cancer Ther; 12(10) October 2013 Molecular Cancer Therapeutics2052
on May 27, 2018. © 2013 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst July 19, 2013; DOI: 10.1158/1535-7163.MCT-13-0108

loss-of-function and toxicity in normal tissues with het-erozygous at DSB repair genes.In conclusion, we have shown that TNBC can be tar-
geted by alpha-particle emitter–labeled anti-EGFR anti-body. The defective DSB repair machinery in a subset ofTNBC can be uniquely suitable for alpha radiation treat-ment. New approaches combining inhibitors of DSBrepair pathways and internal alpha-particle emitters tar-geting remain to be explored. Finally, the safety of such anapproach in patients with heterozygous expression ofDSB repair genes needs to be evaluated.
Disclosure of Potential Conflicts of InterestG. Sgouros has ownership interest in a patent licensed to Actinium
Pharmaceuticals, Inc. No potential conflicts of interest were disclosed bythe other authors.
Authors' ContributionsConception and design: H. Song, G. SgourosDevelopment of methodology: H. Song, M. Hedayati
Acquisition of data (provided animals, acquired and managed patients,provided facilities, etc.):H. Song, M. Hedayati, C. Shao, F. Bruchertseifer,T.L. DeWeeseAnalysis and interpretation of data (e.g., statistical analysis, biostatis-tics, computational analysis): H. Song, M. Hedayati, R.F. Hobbs, G.SgourosWriting, review, and/or revisionof themanuscript:H. Song,M.Hedayati,R.F. Hobbs, C. Shao, A. Morgenstern, T.L. DeWeese, G. SgourosAdministrative, technical, or material support (i.e., reporting or orga-nizing data, constructing databases): H. Song, R.F. Hobbs, F. Bruchert-seifer, A. Morgenstern, G. SgourosStudy supervision: H. Song, G. Sgouros
Grant SupportThis work was supported by NIH grant R01 CA 113797 (to G. Sgouros)
and Maryland Stem Cell Research Fund (MSCRF) grant 2009-MSCRFE-0109-00 (to H. Song).
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received February 13, 2013; revised June 18, 2013; accepted July 14, 2013;published OnlineFirst July 19, 2013.
References1. Goldenberg DM. Targeted therapy of cancer with radiolabeled anti-
bodies. J Nucl Med 2002;43:693–713.2. Song H, Sgouros G. Radioimmunotherapy of solid tumors: searching
for the right target. Curr Drug Deliv 2011;8:26–44.3. Pai-Scherf LH, Carrasquillo JA, Paik C, Gansow O, Whatley M, Pear-
son D, et al. Imaging and phase I study of 111In- and 90Y-labeled anti-LewisY monoclonal antibody B3. Clin Cancer Res 2000;6:1720–30.
4. Sharkey RM, Goldenberg DM, Murthy S, Pinsky H, Vagg R, Pawlyk D,et al. Clinical evaluation of tumor targeting with a high-affinity, antic-arcinoembryonic-antigen-specific, murine monoclonal antibody, MN-14. Cancer 1993;71:2082–96.
5. Ballangrud AM, Yang WH, Palm S, Enmon R, Borchardt PE, PellegriniVA, et al. Alpha-particle emitting atomic generator (Actinium-225)-labeled trastuzumab (Herceptin) targeting of breast cancer spheroids:efficacy versus HER2/neu expression. Clin Cancer Res 2004;10:4489–97.
6. Ballangrud AM, Yang WH, Charlton DE, McDevitt MR, Hamacher KA,PanageasKS, et al. Responseof LNCaPspheroids after treatmentwithan alpha-particle emitter (213Bi)-labeled anti-prostate-specific mem-brane antigen antibody (J591). Cancer Res 2001;61:2008–14.
7. Sgouros G, Squeri S, Ballangrud AM, Kolbert KS, Teitcher JB, Pana-geas KS, et al. Patient-specific, 3-dimensional dosimetry in non-Hodgkin's lymphoma patients treated with 131I-anti-B1 antibody:assessment of tumor dose-response. J Nucl Med 2003;44:260–8.
8. Hernandez MC, Knox SJ. Radiobiology of radioimmunotherapy with90Y ibritumomab tiuxetan (Zevalin). Semin Oncol 2003;30:6–10.
9. Johansson L, Carlsson J, Nilsson K. Radiosensitivity of human B-lymphocytic lymphomas in vitro. Int J Radiat Biol Relat Stud PhysChem Med 1982;41:411–20.
10. M'Kacher R, Bennaceur A, Farace F, Lauge A, Plassa LF, Wittmer E,et al. Multiple molecular mechanisms contribute to radiation sensitivityin mantle cell lymphoma. Oncogene 2003;22:7905–12.
11. Lord CJ, Ashworth A. The DNA damage response and cancer therapy.Nature 2012;481:287–94.
12. Fackenthal JD, OlopadeOI. Breast cancer risk associatedwith BRCA1and BRCA2 in diverse populations. Nat Rev Cancer 2007;7:937–48.
13. Risch HA, McLaughlin JR, Cole DE, Rosen B, Bradley L, Kwan E, et al.Prevalence and penetrance of germline BRCA1 and BRCA2mutationsin a population series of 649 women with ovarian cancer. Am J HumGenet 2001;68:700–10.
14. Goggins M, Schutte M, Lu J, Moskaluk CA, Weinstein CL, PetersenGM, et al. Germline BRCA2 genemutations in patients with apparentlysporadic pancreatic carcinomas. Cancer Res 1996;56:5360–4.
15. LynchHT, de la Chapelle A. Hereditary colorectal cancer. N Engl JMed2003;348:919–32.
16. Esteller M, Garcia-Foncillas J, Andion E, Goodman SN, Hidalgo OF,Vanaclocha V, et al. Inactivation of theDNA-repair geneMGMTand theclinical response of gliomas to alkylating agents. N Engl J Med2000;343:1350–4.
17. McDevitt MR, Sgouros G, Finn RD, Humm JL, Jurcic JG, Larson SM,et al. Radioimmunotherapy with alpha-emitting nuclides. Eur J NuclMed 1998;25:1341–51.
18. Kasparek TR, Humphrey TC. DNA double-strand break repair path-ways, chromosomal rearrangements and cancer. Semin Cell Dev Biol2011;22:886–97.
19. PerouCM,Sorlie T, EisenMB, van deRijnM, Jeffrey SS, ReesCA, et al.Molecular portraits of human breast tumours. Nature 2000;406:747–52.
20. Dent R, Trudeau M, Pritchard KI, Hanna WM, Kahn HK, Sawka CA,et al. Triple-negative breast cancer: clinical features and patterns ofrecurrence. Clin Cancer Res 2007;13:4429–34.
21. Anders CK, Winer EP, Ford JM, Dent R, Silver DP, Sledge GW, et al.Poly(ADP-Ribose) polymerase inhibition: "targeted" therapy for triple-negative breast cancer. Clin Cancer Res 2010;16:4702–10.
22. Neve RM, Chin K, Fridlyand J, Yeh J, Baehner FL, Fevr T, et al. Acollectionof breast cancer cell lines for the studyof functionally distinctcancer subtypes. Cancer Cell 2006;10:515–27.
23. Song H, Shahverdi K, Huso DL, Esaias C, Fox J, Liedy A, et al. 213Bi(alpha-emitter)-antibody targeting of breast cancer metastases in theneu-N transgenic mouse model. Cancer Res 2008;68:3873–80.
24. SongH,HobbsRF, VajraveluR,HusoDL, EsaiasC,ApostolidisC, et al.Radioimmunotherapy of breast cancer metastases with alpha-particleemitter 225Ac: comparing efficacy with 213Bi and 90Y. Cancer Res2009;69:8941–8.
25. Apostolidis C,Molinet R, Rasmussen G,Morgenstern A. Production ofAc-225 from Th-229 for targeted alpha therapy. Anal Chem 2005;77:6288–91.
26. Zielinska B, Apostolidis C, Bruchertseifer F, Morgenstern A. Animproved method for the production of Ac-225/Bi-213 from Th-229for targeted alpha therapy. Solvent Extr Ion Exc 2007;25:339–49.
27. McDevitt MR, Finn RD, Sgouros G, Ma D, Scheinberg DA. An 225Ac/213Bi generator system for therapeutic clinical applications: construc-tion and operation. Appl Radiat Isot 1999;50:895–904.
28. Song H, Shahverdi K, Huso DL, Wang Y, Fox JJ, Hobbs RF, et al. Animmunotolerant HER-2/neu transgenic mouse model of metastaticbreast cancer. Clin Cancer Res 2008;14:6116–24.
Targeting Defective DNA DSB Repair with Alpha Radiation
www.aacrjournals.org Mol Cancer Ther; 12(10) October 2013 2053
on May 27, 2018. © 2013 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst July 19, 2013; DOI: 10.1158/1535-7163.MCT-13-0108

29. Zhao Y, Thomas HD, Batey MA, Cowell IG, Richardson CJ, Griffin RJ,et al. Preclinical evaluation of a potent novel DNA-dependent proteinkinase inhibitor NU7441. Cancer Res 2006;66:5354–62.
30. Sgouros G, Ballangrud ÅM, Humm JL, Jurcic JG, McDevitt MR, ErdiYE, et al. Pharmacokinetics and dosimetry of an alpha-particle emitterlabeled antibody: 213Bi-HuM195 (anti-CD33) in patients with leukemia.J Nucl Med 1999;40:1935–46.
31. Howell RW, RaoDV, Bouchet LG, BolchWE, Goddu SM.MIRD cellularS values. Reston, VA: Society of Nuclear Medicine; 1997.
32. Hamacher KA, Den RB, Den EI, Sgouros G. Cellular dose conversionfactors for alpha-particle–emitting radionuclides of interest in radio-nuclide therapy. J Nucl Med 2001;42:1216–21.
33. Rosenblat TL, McDevitt MR, Mulford DA, Pandit-Taskar N, Divgi CR,Panageas KS, et al. Sequential cytarabine and alpha-particle immu-notherapy with bismuth-213-lintuzumab (HuM195) for acute myeloidleukemia. Clin Cancer Res 2010;16:5303–11.
34. Andersson H, Cederkrantz E, Back T, Divgi C, Elgqvist J, HimmelmanJ, et al. Intraperitoneal alpha-particle radioimmunotherapy of ovariancancer patients: pharmacokinetics and dosimetry of (211)At-MX35 F(ab')2–a phase I study. J Nucl Med 2009;50:1153–60.
35. Allen BJ, Singla AA, Rizvi SM, Graham P, Bruchertseifer F, Aposto-lidis C, et al. Analysis of patient survival in a Phase I trial of systemictargeted alpha-therapy for metastatic melanoma. Immunotherapy2011;3:1041–50.
36. Kneifel S, Cordier D, Good S, Ionescu MC, Ghaffari A, Hofer S, et al.Local targeting of malignant gliomas by the diffusible peptidic vector1,4,7,10-tetraazacyclododecane-1-glutaric acid-4,7,10-triacetic acid-substance p. Clin Cancer Res 2006;12:3843–50.
37. Nilsson S, Franzen L, Parker C, Tyrrell C, Blom R, Tennvall J, et al.Bone-targeted radium-223 in symptomatic, hormone-refractory pros-tate cancer: a randomised, multicentre, placebo-controlled phase IIstudy. Lancet Oncol 2007;8:587–94.
38. Nayak TK,ReginoCA,WongKJ,MilenicDE,Garmestani K, BaidooKE,et al. PET imaging of HER1-expressing xenografts in mice with 86Y-CHX-A00-DTPA-cetuximab. Eur J Nucl Med Mol Imaging 2010;37:1368–76.
39. Nayak TK, Garmestani K, Milenic DE, Brechbiel MW. PET and MRI ofmetastatic peritoneal and pulmonary colorectal cancer in mice withhuman epidermal growth factor receptor 1-targeted 89Zr-labeledpanitumumab. J Nucl Med 2012;53:113–20.
40. Schechter NR, Wendt RE III, Yang DJ, Azhdarinia A, Erwin WD,Stachowiak AM, et al. Radiation dosimetry of 99mTc-labeled C225in patients with squamous cell carcinoma of the head and neck. J NuclMed 2004;45:1683–7.
41. Pfost B, Seidl C, Autenrieth M, Saur D, Bruchertseifer F, MorgensternA, et al. Intravesical alpha-radioimmunotherapy with 213Bi-anti-
EGFR-mAb defeats human bladder carcinoma in xenografted nudemice. J Nucl Med 2009;50:1700–8.
42. Milenic DE, Wong KJ, Baidoo KE, Ray GL, Garmestani K, Williams M,et al. Cetuximab: preclinical evaluation of a monoclonal antibodytargeting EGFR for radioimmunodiagnostic and radioimmunothera-peutic applications. Cancer Biother Radiopharm 2008;23:619–31.
43. Van Cutsem E, Kohne CH, Hitre E, Zaluski J, Chang Chien CR,Makhson A, et al. Cetuximab and chemotherapy as initial treatmentfor metastatic colorectal cancer. N Engl J Med 2009;360:1408–17.
44. Wygoda Z, Kula D, Bierzynska-Macyszyn G, Larysz D, Jarzab M,Wlaszczuk P, et al. Use of monoclonal anti-EGFR antibody in theradioimmunotherapy of malignant gliomas in the context of EGFRexpression in grade III and IV tumors. Hybridoma 2006;25:125–32.
45. Nieuwenhuis B, Van Assen-Bolt AJ, Van Waarde-Verhagen MA, Sij-mons RH, Van der Hout AH, Bauch T, et al. BRCA1 and BRCA2heterozygosity and repair of X-ray-induced DNA damage. Int J RadiatBiol 2002;78:285–95.
46. Andreassen CN, Alsner J. Genetic variants and normal tissue toxicityafter radiotherapy: a systematic review. Radiother Oncol 2009;92:299–309.
47. Karlsson KH, Stenerlow B. Focus formation of DNA repair proteins innormal and repair-deficient cells irradiated with high-LET ions. RadiatRes 2004;161:517–27.
48. Kinashi Y, Takahashi S, Kashino G, Okayasu R, Masunaga S, SuzukiM, et al. DNA double-strand break induction in Ku80-deficient CHOcells following Boron Neutron Capture Reaction. Radiat Oncol2011;6:106.
49. Pessetto ZY, Yan Y, Bessho T, Natarajan A. Inhibition of BRCT(BRCA1)-phosphoprotein interaction enhances the cytotoxic effectof olaparib in breast cancer cells: a proof of concept study forsynthetic lethal therapeutic option. Breast Cancer Res Treat 2012;134:511–7.
50. Huang F, Motlekar NA, Burgwin CM, Napper AD, Diamond SL, MazinAV. Identification of specific inhibitors of human RAD51 recombinaseusing high-throughput screening. Acs Chem Biol 2011;6:628–35.
51. O'Shaughnessy J, Osborne C, Pippen JE, Yoffe M, Patt D, Rocha C,et al. Iniparib plus chemotherapy in metastatic triple-negative breastcancer. N Engl J Med 2011;364:205–14.
52. O'Shaughnessy J, Schwartzberg LS, Danso MA, Rugo HS, Miller K,Yardley R, et al. A randomized phase III study of iniparib (BSI-201) incombination with gemcitabine/carboplatin (G/C) in metastatic triple-negative breast cancer (TNBC). J Clin Oncol 2011;29:S1007.
53. Billecke CA, LjungmanME, McKay BC, Rehemtulla A, Taneja N, EthierSP. Lack of functional pRb results in attenuated recovery of mRNAsynthesis and increased apoptosis following UV radiation in humanbreast cancer cells. Oncogene 2002;21:4481–9.
Song et al.
Mol Cancer Ther; 12(10) October 2013 Molecular Cancer Therapeutics2054
on May 27, 2018. © 2013 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst July 19, 2013; DOI: 10.1158/1535-7163.MCT-13-0108

2013;12:2043-2054. Published OnlineFirst July 19, 2013.Mol Cancer Ther Hong Song, Mohammad Hedayati, Robert F. Hobbs, et al. Radiolabeled Anti-EGFR AntibodyTriple-Negative Breast Cancer with Alpha-Particle Emitter Targeting Aberrant DNA Double-Strand Break Repair in
Updated version
10.1158/1535-7163.MCT-13-0108doi:
Access the most recent version of this article at:
Cited articles
http://mct.aacrjournals.org/content/12/10/2043.full#ref-list-1
This article cites 52 articles, 20 of which you can access for free at:
Citing articles
http://mct.aacrjournals.org/content/12/10/2043.full#related-urls
This article has been cited by 1 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://mct.aacrjournals.org/content/12/10/2043To request permission to re-use all or part of this article, use this link
on May 27, 2018. © 2013 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst July 19, 2013; DOI: 10.1158/1535-7163.MCT-13-0108