Embed Size (px)
Citation preview

TRAUMATIC BRAIN INJURY
Tara N. Hammond, DVM, DACVECC
Tufts Veterinary Emergency Treatment & Specialties

Traumatic Brain Injury
Epidemiology
Pathophysiology
Physical Exam
Diagnostics
Treatment/Prognosis
Current Literature
Epidemiology (humans) > 2 million head injuries/year
> 60,000 deaths from TBI yearly
80% minor, 10% moderate, 10% severe
Accounts for ~50% of deaths from trauma
Financial burden: $100-200 billion annually
Mortality: 25-35%

Epidemiology (animals) Not known
Causes:HBCBDLDStepped on (pediatrics) ‘High rise’Kick injuriesPenetrating wounds Other blunt force trauma (crush injuries, etc.)

Primary Brain Injury Direct physical consequence of the impact
Skull fractures
Concussion
Contusions ○ site of impact (coupe) ○ opposite hemisphere where the displaced brain
contacts the skull (contrecoup)
Lacerations ○ hematomas

Secondary Brain Injury
Hours to days after insult
Major determinant of ultimate neurological outcome
Intracranial factors
Extracranial factorsSystemic factorsCellular factors
Cerebral Edema
Cytotoxic edema results from:Breakdown of cellular structuresDisruption of cell membrane function Disregulation of cellular ionic gradientIncrease in IC Na and Ca → increases osmolalityFluid accumulation in neurons and astrocytes
Vasogenic edema results from:Damage to BBB → changes in permeabilityEC fluid accumulation

Secondary Brain InjuryIntracranial factors
○ Increased ICP
○ Compromise of BBB
○ Mass lesions
○ Cerebral edema
○ Infection
○ Vasospasm
○ Seizures

Secondary Brain Injury Cellular factors
Disruption of the Na/K ATPase pump ○ ATP depletion ○ accumulation of IC Na ○ worsening cytotoxic edema○ accumulation of intracellular Na and Ca ○ depolarization
Excitotoxic injury: uncontrolled depolarization ○ increase in excitatory neurotransmitters (glutamate) ○ Ca influx into the cytosol ○ worsening cytotoxic edema ○ neurodegeneration of the CNS

Secondary Brain Injury Cellular factors
Cerebral lactic acidosis due to increased anaerobic metabolism○ Hyperkalemia → neuronal depolarization○ Inflammation○ Ischemia-reperfusion injury○ NO accumulation → excessive vasodilation
ROS, lipid peroxidation, cytokine production
Activation of the arachidonic acid, kinin, complement, and coagulation cascades

Systemic Insults
Acid-base disturbancesElectrolyte imbalancesHyper/hypocapniaHyper/hypoglycemiaHyper/hypothermiaHypotensionHypoxiaSystemic inflammation


Oxygen Delivery (DO2)
Decreased DO2 is the main perpetrator of secondary brain injury Further ATP depletion Anaerobic metabolism Lactic acidosis Cellular damage/death
DO2 = CaO2 x CO
CO = HR x SV
CaO2 = (Hb x 1.34 x SaO2) + (0.003 x PaO2)
Effect of anemia, pulmonary contusions, pleural space disease

Cerebral Blood Flow
15% of resting CO
20% total O2 consumed
Determined by: CPP PaO2
PaCO2 Cerebral metabolic demand

Monroe-Kellie Doctrine
Cranial compartment is incompressible Volume inside the cranium is fixed Cranium/contents create a volume equilibrium
blood (10%)CSF(10%)brain tissue (80%)
Any increase in volume of one must be compensated by a decrease in another

Intracranial Pressure Depends on volume of CSF, blood, and brain tissue
in the cranial vault Normal <15mmHg (5-12)
CPP = MAP – ICP Goals: CPP ≥ 70mmHg, SAP ≥ 90mmHg, MAP ≥ 80mmHg
Aggressive attempts to maintain CPP>70mmHg with IVF and pressors should
be avoided due to risk of ARDS – Level II
CPP <50mmHg should be avoided. Target is 50-70mmHg. Patients with
impaired autoregulation will tolerate higher CPPs - Level III

Intracranial Hypertension Major cause of post-traumatic neurological
morbidity/mortality
Limits cerebral perfusion
Promotes hypoxic/ ischemic injury
Compression of brainstem: depressed mental, cardiac, respiratory function and herniation/death

Intracranial Hypertension Humans treated when ICP >20mmHg
Accommodated by:Venous blood shunting out of the skull (can fall by 30-40%) Increased CSF absorption (can reduce the size of the ventricles
up to 90%)Brain tissue is somewhat compressible Hyperventilation → cerebral vasoconstriction and decreased
blood flow into the cranial vault
Intracranial volume can gain ~100-150ml (an average hematoma) in humans without significant increases in ICP

Autoregulation
Pressure: vascular smooth muscle maintains CBF via changes in CVR over MAPs of 50-150mmHg
Outside this range CBF is directly proportional to BP

Autoregulation Chemical: vasoconstriction/dilation in response to CO2
Hypoventilation → ↑PaCO2 → respiratory acidosis sensed by central chemoreceptors → vasodilation of cerebral vasculature, ↑CBF and ↑ICP
Hyperventilation → ↓PaCO2 → respiratory alkalosis sensed by central chemoreceptors → vasoconstriction of cerebral vasculature, ↓CBF and ↓ICP
1mmHg change in PaCO2 → 3-4% change in CBF
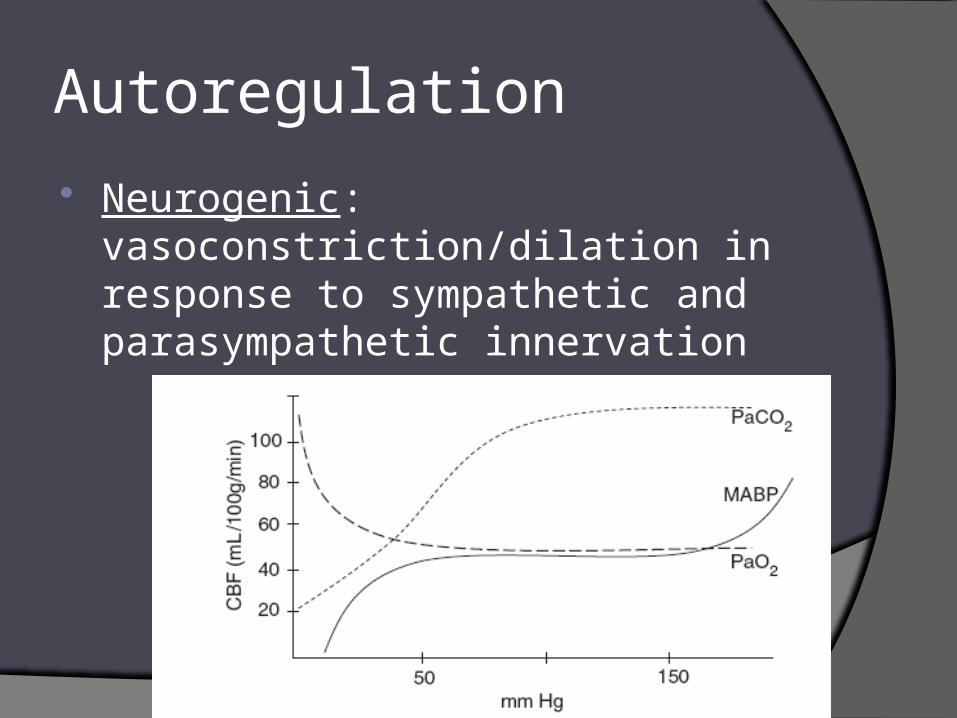
Autoregulation
Neurogenic: vasoconstriction/dilation in response to sympathetic and parasympathetic innervation

Factors affecting CBF
Hyper/hypocapnia Hypoxia Local acidosis Increased cerebral O2 demand Fever Seizures Increased sympathetic activity Systemic hypertension/hypotension

Cushing’s Response Marked elevations in ICP limit CBF
Ischemia causes the vasomotor center of the brain emits a massive SNS discharge
Systemic vasoconstriction/severe hypertension result to elevate MAP and maintain CPP
Hypertension is sensed by baroreceptors (carotids) resulting in a reflex bradycardia via PNS
Hypertension, bradycardia and decreased LOC = severe intracranial hypertension and IMPENDING HERNATION

Triage
Cardiovascular stability
Mentation
Major injuries

Physical exam
Complete PE
Assess other injuries
GCS
Full neurologic exam

Predicted probability of survival in 38 dogs during the 1st 48 hours after TBI
50% probability of survival for GCS of 8
MGCS category was not found to predict patient survival.
Gender, weight, age and presence of skull fractures did not predict survival
Total Score Severity Prognosis
3 - 8 Severe Grave
9 - 14 Moderate Poor to guarded
15 - 18 Slight Good

Modified Glascow Coma Score
Motor activity Score
Normal gait, normal spinal reflexes 6
Hemiparesis, tetraparesis, or decerebrate activity 5
Recumbent, intermittent extensor rigidity 4
Recumbent, constant extensor rigidity 3
Recumbent, constant extensor rigidity with opisthotonus 2
Recumbent, hypotonia of muscles, depressed or absent spinal reflexes
1

Modified Glascow Coma Score
Brain stem reflexes Score
Normal pupillary light reflexes and oculocephalic reflexes 6
Slow pupillary light reflexes and normal to reduced oculocephalic reflexes
5
Bilateral unresponsive meiosis with normal to reduced oculocephalic reflexes
4
Pinpoint pupils with reduced to absent oculocephalic reflexes 3
Unilateral, unresponsive mydriasis with reduced to absent oculocephalic reflexes
2
Bilateral, unresponsive mydriasis with reduced to absent oculocephalic reflexes
1

Modified Glascow Coma Score
Level of consciousness Score
Occasional periods of alertness and responsive to environment 6
Depression or delirium, capable of responding but response may be inappropriate
5
Semicomatose, responsive to visual stimuli 4
Semicomatose, responsive to auditory stimuli 3
Semicomatose, responsive only to repeated noxious stimuli 2
Comatose, unresponsive to repeated noxious stimuli 1

Level of consciousness Provides information about the functionality of the cerebral
cortex and the ascending reticular activating system
Normal
Obtunded - arousable with noise or gentle touch but have decreased responsiveness to the environment
Stuporous - responsive to noxious stimulation only
Comatose - not responsive to any stimulation

Pupils Respond to light
intact rostral brainstem, optic chasm, optic nerves, and retinae
Miosis diencephalon lesion (hypothalamus)
Initially mitotic and then become mydriatic progressive brainstem lesion
Normal to mydriatic, non-responsive pupils injury to oculomotor nerve in the brainstem ipsilateral to the injury
Bilateral mydriasis with no response to light irreversible midbrain damage and herniation
Anisocoria lateralizes lesion

Pupils Vestibulo-ocular reflex
physiologic nystagmus – lack of often indicates brain stem injury
Oculocephalic reflex (Doll’s eye) normal response of moving laterally
toward the side opposite the direction the head is turned
severe brain stem dysfunction if absent

Motor Function/Posturing
Decerebrate rigidity opisthotonus extensor rigidity of all limbs severely altered mentation lesion at or just rostral to the midbrain grave prognosis
Decerebellate rigidity opisthotonus forelimbs are in extension hindlimbs flexed (or sometimes normal) alert and aware lesion of the rostral lobe of the cerebellum
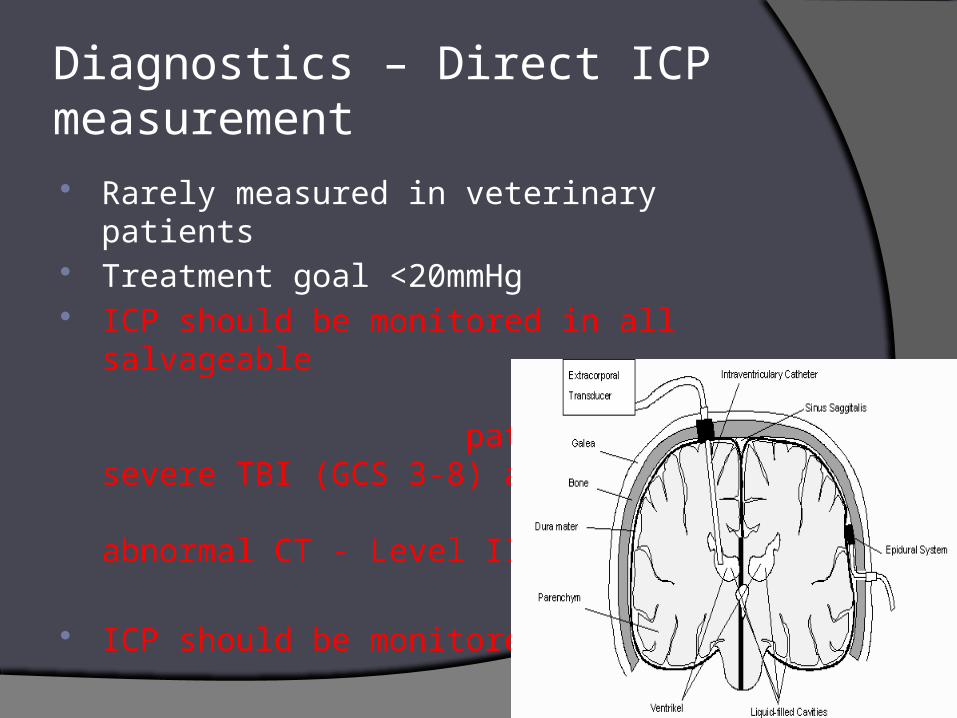
Diagnostics – Direct ICP measurement Rarely measured in veterinary patients Treatment goal <20mmHg ICP should be monitored in all salvageable
patients with severe TBI (GCS 3-8) and abnormal CT - Level II
ICP should be monitored in all patients with severe TBI (GCS 3-8) and a normal CT if 2 or more of the following exist at admission: age >40yo, abnormal posturing, hypotension - Level III

Diagnostics - CT
Skull fractures

Diagnostics - CT•
Multiple, small petechial
hemorrhages at the q gray-white matter
junction characteristic of diffuse axonal injury

Diagnostics - CT
Epidural
hematoma

Diagnostics - CT
Subdural hematoma with
midline shift and obliteration/
compression of ventricles
More common Higher mortality
3rd
Lat vent

Diagnostics - MRI
Hemorrhage

Goals of Treatment Maintain adequate CPP and CBF
Control ICP
Reduce cerebral metabolism
Maintain adequate BP
Avoid hypercarbia, hypoxemia
Treat the rest of the patient

Treat Intracranial hypertension
Reduce brain size Reduce blood flow Reducing CSF
removal of 3cc of CSF = ~10% decrease in ICP and ~2% increase in CPP
Surgical intervention Treatment should be initiated with
ICP>20mmHg – Level II

Mannitol
Osmotic diuretic Pulls free H2O from the intracellular and interstitial spaces of the brain
into the vasculature → reduction of cerebral edema
Transient volume expansion
Decrease in blood viscosity induces cerebral vasoconstriction and maintain CBF
Reduces RBC deformity → improved O2 carrying capacity
Free radical scavenging properties → limited IRI injury
In one study high dose mannitol (1.4g/kg) resulted in significant neurological improvement in humans with TBI versus low dose mannitol (.7g/kg)

Mannitol Risks:
osmotic diuresis can worsen hypovolemia, causing hypotension which offset the beneficial effects on ICP
precipitation of acute renal tubular necrosis ○ maintain serum osmolarity < 320 mOsm/L
What about exacerbation of ongoing intracranial hemorrhage?
○ not a concern
Mannitol is effective at for control of raised ICP at doses of .25-1g/kg. Hypotension should be avoided – Level II
Restrict mannitol use prior to ICP monitoring to patients with signs of herniation or progressive neurologic deterioration not attributable to extracranial causes – Level III

Hypertonic Saline Rapid rise in osmolarity causes fluid movement
from the interstitium and intracellular space to the intravascular space
Reduction of cerebral edema and decrease in ICP without adverse hemodynamic effects
First line therapy when intracranial hypertension exists with hypovolemia
HS encourages regional CBF (and therefore DO2) by minimizing endothelial cell swelling and promoting arteriolar dilation

Hypertonic Saline Modulates the inflammatory response by limiting
cellular adhesion and decreasing excitotoxicity
Shown to minimize vasospasm, promote local vasodilation, and limit endothelial cell swelling
Randomized study of patients with head trauma, persistent coma and ICH resistant to standard therapy, hypertonic saline was MORE effective than mannitol at reducing ICP

Furosemide
Brain Trauma Foundation no longer recommends to treat cerebral edema
No benefit in multiple studies
Potential for intravascular volume depletion → systemic hypotension → ↓ CPP

Steroids
CONTRAINDICATED
Increase morbidity/mortality
Side effects:hyperglycemia immunosuppressiongastrointestinal ulcerationdecreased wound healing

CRASH study Randomized controlled clinical trial
of >10,000 humans
Corticosteroid use:no effect on ICPincreased mortalityworse 2 week and 6 month outcome
Corticosteroids are not recommended for improving outcome or reducing ICP. In TBI patients steroid use has been shown to increase morality and are contraindicated – Level I

Fluid Therapy Fluids should never be restricted
Dehydration only minimally decreases ICP
Hypovolemia can significantly impair CPP
Overhydration should be avoided
Even one episode of hypotension (SAP<90mmHg) doubles mortality
Hypotonic crystalloids should be strictly
Glucose containing fluids should be avoided
Continuous BP monitoring with avoidance of hypotension
(SAP<90mmHG) - Level II

Fluid Therapy Intact BBB is impermeable to colloids
Compromise of the BBB with TBI and fluids may leak into the cerebral interstitium worsening vasogenic edema (?)
Benefit of restoration of MAP (and therefore CPP) far
outweighs this theoretical risk
SAFE trial (Saline vs. Albumin Fluid Evaluation) TBI patients resuscitated with albumin
(vs. .9%NaCl) had:○ a higher mortality rate ○ worse functional neurological outcome at 24m

Pressors
Dopamine has been shown to improve CBF after TBI without causing cerebral vasoconstriction
Vasopressin and norepinephrine can also be used. However, norepinephrine use may be associated with cerebral perfusion compromise (conflicting data)

Ventilation
1 episode of hypoxia (PaO2 <60mmHg) doubles mortality
Provide supplemental O2
Avoid placement of nasal O2
Intubate smoothly
GOALS/SETTINGS: SpO2 >97%, PaO2 >90mmHg
PaCO2 goal 35mmHg (35-40)
Oxygenation should be monitored and hypoxia (PaO2 < 60mmHg, SaO2 <90mmHg) avoided - Level III

Hyperventilation ↓PaCO2 → respiratory alkalosis → vasoconstriction of
cerebral vasculature → ↓CBF and ↓ICP
Routine therapeutic hyperventilation NOT recommended
Short-term, life-saving for patients with acute neurological deterioration and signs of impending herniation
Goal: PaCO2 of 25-30mmHg works within 30 seconds max effect 8min reduce ICP by 25%
Hyperventilation Excessive hyperventilation (PaCO2 < 25mmHg,
>30min) should be avoided worsen cerebral ischemia and secondary
neurological injury
Prophylactic hyperventilation (PaCo2 ≤ 25mmHg) is not recommended – Level II
Hyperventilation is recommended as temporary measure for reduction on increased ICP but should be avoided during the first 24hrs when CBF is critically reduced. If used, SjO2 and PbrO2 are recommended to monitor DO2 - Level III
Seizures Seizures reported in up to 54% of humans
Immediate: < 24 hrs Early: 24 hrs- 7d Late: > 7d
Worsen secondary injury hypoxia, hypercarbia, releasing excitatory neurotransmitters,
depleting energy stores and increasing ICP
Antiseizure prophylaxis controversial overall reduction in the risk of immediate and early seizures with
prophylactic treatment with phenytoin (humans) no benefit associated with treatment longer than 7 days

Anticonvulsants Diazepam - agent of choice for active seizuring
Phenobarbital - most common agent for longer term control markedly decrease activation energy of cerebral tissue cardiovascular and respiratory depressant effects
Other options: KBr, Keppra, Zonisamide
Induction of barbiturate coma with pentobarbital decrease metabolic demands hypotension/ hypoventilation can increase ICP
Prophylactic use of AEDs is indicated to decrease the incidence of early post traumatic seizures. However early post traumatic seizures are not associated with worse outcomes – Level II
Prophylactic use of AEDs is not recommended for late posttraumatic seizures – Level II

Hypothermia – proposed benefits
Reduced :metabolisminflammationcerebral edemabrain volume ICPglutamate levels cytokine release

Hypothermia - complications Iatrogenic hypothermia Decreased immunity Infection Coagulation derangements Hypotension Bradycardia Arrhythmias Decreased myocardial performance

Hypothermia
Data indicates prophylactic hypothermia is not significantly associated with decreased mortality when compared to normothermic controls
Preliminary data suggests that a greater decrease in mortality risk is observed when target temperatures are maintained for >48hrs
Prophylactic hypothermia is associated with significantly higher Glascow Outcome scores when compared to normothermic controls – Level III

11yo SF Wheaton HBC GCS 10 Seizures uncontrolled with traditional therapy Controlled hypothermia (91o-95oF) Mechanical ventilation Full recovery/discharged
Behavior changes reported 8 weeks

Hyperglycemia Associated with increased mortality and worse
neurological outcomes for TBI patients
Higher admission BG associated with lower GCSs
Sympathoadrenal response to injury
Patients with cerebral ischemia and hyperglycemia: increases free radical production increases excitatory amino acid release increases cerebral edema Increase cerebral acidosis altered cerebral vasculature

Hyperglycemia Cerebral acidosis - most important mechanism of
increased secondary brain injury with hyperglycemia
During ischemia the brain relies on anaerobic glycolysis → accumulation of lactate and H+ → cerebral acidosis
Tighter control of BG without reduction in nutritional support is recommended
Insulin CRI to maintain BG between 70 and 120mg/dl (<150)
Avoid glucose-containing solutions

52 dogs, 70 cats
BG within 1h of admit
BG significantly higher in TBI patients
Unlikely a stress response to hospitalization
BG significantly associated with severity
BG not associated with outcome

Supportive Care
Elevate head/neck 15-30o to facilitate venous drainage
Avoid jugular compression Adequate analgesia Basic nursing care Nutritional support (enteral with promotility
agents) Antibiotics Serial neurological exams Continuous monitoring GI protectants

Indications for surgery
Repair/removal depressed skull fractures
Evacuation of hematomas
Debulking of tumors
Decompressive craniectomy to control severely elevated ICP and prevent brain herniation (when refractory to medical therapy)

Pre-oxygenate
Smooth induction imperative
Appropriate IV access
Appropriate monitoring

Opioids
Minimal adverse cardiovascular effects
Reversible
Adverse effectsrespiratory depression hypotensionappropriate dosing and ventilation = safeCRIs better to avoid peaks and troughs

Benzodiazepines Lack adverse intracranial effects
Lack adverse cardiovascular and respiratory effects
Do not reduce ICP
Do cause small reductions in cerebral O2 demands
Enable dose reductions of other drugs

Etomidate Offers cardiovascular and respiratory stability
? neuroprotection
In humans it’s associated with cerebral hypoxia and cerebral ischemia possibly due to: cerebral vasoconstriction hemolysis NO scavenging
At this time the use of this drug is not recommended with TBI

Ketamine Typically avoided - can ↑ ICP
With concurrent propofol administration it helps ↓ ICP
Inhibits NMDA receptor (predominant receptor type responsible for ischemic injury) and may reduce secondary brain injury
Doesn’t cause cardiovascular and respiratory depression
Demonstrated to increase cerebral O2 consumption
Promising research in status epilepticus

Dexmedetomidine
Does not appear to influence ICP in dogs
Reduction in HR and CO can impair CPP
Only be used at very low doses (~1mcg/kg/hr)
Only be used when analgesia with less cardiovascular effects is unavailable/not adequate

Barbiturates Neuroprotective
Reduction in: cerebral O2 requirements, CBF, ICP
Increased protection from excitatory neurotransmitter release
Reduce Na channel conduction and IC Ca entry into the brain limits free radical production, ROS, and IRI injury
Antioxidant effects
Reduce seizure activity
Disadvantages delayed anesthetic recovery, hypotension, respiratory depression

Propofol
possible modulation of GABA receptors antioxidant effects more rapid recovery
Disadvantagesnegative cardiovascular effectsrespiratory depression

Volatile anesthetics
Dose related effects on ICP
Lower concentrations ○ reduce cerebral metabolism ○ decrease in CBF, ICP
At <1.3% MAC isoflurane ○ suppression of metabolic activity persists ○ ICP increases ○ compromised of CCP due to vasodilation and
anesthetic induced hypoventilation/hypercapnia○ systemic hypotension detrimentally affect CPP

Volatile anestheticsHigher alveolar concentrations
○ cerebral pressure autoregulation is disrupted○ perfusion becomes dependant on MAP
If ICP normal low doses are acceptable
If ICP already elevated they should avoided


12wo IF Great Dane Owner fell on
GCS 13, hypothermic, hypotensive, obtunded
BW ↑ Na , ↑ K, ↓ BG
HPA axis disruption due to trauma: Central Diabetes Insipidus – vasopressin ACTH stimulation test = hypoadrenocorticism – steroids, DOCP Thyroid profile = hypothyroid - L-thyroxine Growth hormone decreased Gonadotropin releasing hormone decreased


REFERENCES Armitage-Chan EA, Wetmore LA, Chan DL. Anesthetic management of the
head trauma patient. J Vet Emerg Crit Care 2007; 17(1):5-14.
Bhardwaj A, Ulatowski JA. Hypertonic saline solutions in brain injury. Curr Opin Crit Care 2004; 10(2):126-131.
Chestnut RM, Marshall LF, Klauber MR et al. The role of secondary brain injury in determining outcome from severe head injury. J Trauma 1993; 34:216-222.
Cohen SM, Marion DW. Traumatic brain injury, in Fink MP, et al: (ed): Textbook of critical care: 5th edition. Philadelphia, Elsevier Inc., 2005. Pp. 377-389.
Coles JP, Fryer TD, Coleman MR, et al. Hyperventilation following head injury: effect on ischemic burden and cerebral oxidative metabolism. Crit Care Med 2007; 35(2):568-578.
CRASH trial collaborators. Effect of intravenous corticosteroids on death within 14 days in 10008 adults with clinically significant head injury (MRC CRASH trial): randomized placebo-controlled trial. Lancet 2004; 364(9442): 1321-1328.

REFERENCES Cruz J, Minoja G, Okuchi K, et al. Successful use of the new high-dose mannitol
treatment in patients with Glascow Coma scores of 3 and bilateral abnormal pupillary widening: a randomized trial. J Neurosurg 2004; 100:376-383.
Dewey CW. Emergency management of the head trauma patient. Principles and practice. Vet Clin North Am Small Anim Pract 2000; 30(1):207-225.
Foley C, Bracker K, Drellich S. Hypothalamic-pituitary axis deficiency following traumatic brain injury in a dog. J Vet Emerg Crit Care 2009; 19(3):269-274.
Hayes GM. Severe seizures associated with traumatic brain injury managed by controlled hypothermia, pharmacologic coma, and mechanical ventilation in a dog. J Vet Emerg Crit Care 2009; 19(6):629-634.
Henzler D, Cooper J, Tremayne AB. Early modifiable factors associated with fatal outcome in patients with severe traumatic brain injury: a case control study. Crit Care Med 2007; 35(4)1027-1031
Hopkins AL. Head trauma. Vet Clin North Am 1996; 26(4):875-891

REFERENCES Jeremitsky E, Omert LA, Dunham CM, et al. The impact of hyperglycemia
on patients with severe brain injury 2005; 58(1):47-50.
Journal of Neurotrauma 2007; 24(S1)
Pinto FCG, Capone-Neto A, Prist R, et al. Volume replacement with Lactated Ringer’s or 3% hypertonic saline solution during combined experimental hemorrhagic shock and traumatic brain injury. J Trauma 2006; 60(4):758-764.
Platt SR, Radaelli ST, McDonnell JJ. The prognostic value of the modified
glascow coma scale in head trauma dogs. J Vet Int Med 2001; 15:581-584.
Proulx P, Dhupa N: Severe brain injury- part I pathophysiology. Compend
Contin Educ Pract Vet 1998; 20(8):897-905.
Proulx P, Dhupa N: Severe brain injury - part II therapy. Compend Contin
Educ Pract Vet 1998; 20(9):993-1006.

REFERENCES The Safe Study Investigators. A comparison of albumin and saline for fluid
resuscitation in the intensive care unit. N Engl J Med 2004; 350(22):2247-2256.
Sande A, West C. Traumatic brain injury: a review of pathophysiology and management. J Vet Emerg Crit Care 2010; 20(2):177-190.
Shores A. Craniocerebral Trauma. In Kirk RW ed. Current Veterinary Therapy X. Philadelphia: WB Saunders Co., 1983, Pp. 847-854
Syring RS, Otto CM, Drobatz KJ. Hyperglycemia in dogs and cats with head trauma: 122 cases (1997-1999). J Am Vet Med Assoc 2007; 218(7):1124-1129.
Syring RS. Assessment and treatment of central nervous system abnormalities ion the emergency patient. Vet Clin North Am 2005; 35:343-358.
Vespa PM, O’Phelan K, McArthur D. Pericontusional brain tissue exhibits persistent elevation of lactate/pyruvate ratio independent of cerebral perfusion pressure. Crit Care Med 2007; 35(4)1153-1160.

REFERENCES
Ware ML, Nemani VM, Meeker M, et al. Effects of 23.4% sodium chloride solution in reducing intracranial pressure in patients with traumatic brain injury: a preliminary study. Neurosurgery 2005; 57(4):727-36

Questions?