Embed Size (px)
Citation preview

450 Cavero et al. February 1994
American Heart Journal
I). In both patients a substantial improvement in clinical status and LV function was accompanied by an increase in the aortic valve gradient during follow-up. The two pa- tients reported on here represent rare examples of critical AS first seen during adolescence. The natural history of congenital valvular AS is one of frequent progression pos- sibly resulting from disproportionate body growth as com- pared to the valve orifice or an actual decrease in aortic valve area.5 However, CHF has not been reported during late childhood or adolescence. In the natural history study,2 which included 473 patients with congenital AS, CHF was not encountered beyond infancy. In infants, the relatively rapid growth and increasing tissue demands, together with a limited cardiac reserve, may precipitate CHF in a subgroup of patients with severe AS. The precise reasons CHF first occurred during adolescence in the patients re- ported here is not clear. No precipitating causes (such as anemia or infection) were identified. Possible explanations include an actual decrease in aortic valve area or a relative decrease as a result of the adolescent growth spurt. In summary, congenital valvular AS can rarely manifest with CHF during adolescence. Balloon aortic valvotomy is a valuable treatment option for this potentially life-threat- ening situation.
REFERENCES
1. Fyler DC. Aortic outflow abnormalities. In: Fyler DC, ed. Na- das pediatric cardiology. Philadelphia: Hanley & Belfus, 1992493-512.
2. Wagner HR, Mlison RC, Kaene JF, O’Neal Humphries J, Na- das AS. Clinical course in aortic stenosis: Report from the Joint Study on the Natural History of Congenital Heart De- fects. Circulation 1977;56:47-56.
3. Lababidi, Wu JR, Walls JT. Percutaneous balloon aortic val- vuloplasty; results in 23 patients. Am J Cardiol 1984;53:194-9.
4. Grossman W. Cardiac catheterization and angiography. 3rd ed. Philadelphia: Lea & Febiger, 1986:238.
5. El-Said G, Galioto FM, Mullins CE, McNamara DG. Natural hemodynamic history of congenital aortic stenosis in child- hood. Am J Cardiol 1972;30:6-12.
Takayasu’s disease causing pulmonary hypertension and right heart failure
Miguel Angel Cavero, MD,a Carolina Maicas, MD,a Lorenzo Silva, MD,a Javier Ortigosa, MD,” Miguel Yebra, MD,b Crescencio Camacho, MD,a and Manuel de Artaza, MD,a Madrid, Spain
Takayasu’s disease (TD) is a chronic inflammatory arteri- opathy of unknown origin, mainly involving the aorta and its larger branches, but often affecting the pulmonary cir- culation as well. It is most prevalent in young women.
From the Departments of Tardiology and bInterm Medicine, Hospital Puerta de Hierro.
Reprint requests: Miguel Angel Cavero, MD, Cl Isla de Oza, 64,4, izq., 28035 Madrid, Spain.
An? HEART J 1994;127:450-1.
Copyright 8’ 1994 by Mosby-Year Book, Inc. oooz-8703/94/$1.00 + .lO 4/4/51117
There is an initial phase characterized by general symp- toms such as malaise, fever, arthralgias, and anorexia, fol- lowed months to years later by symptoms of ischemia in organs affected by the vascular lesions. Common manifes- tations include absent pulses, bruits, hypertension (due to renal arterial involvement), left heart failure, stroke, syn- cope, ocular symptoms, and claudication of the limbs.
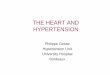
We present the case of a 44-year-old man whose history of this disorder began at the age of 24 years with severe in- termittent claudication of the lower limbs. He did not have diabetes or hypertension, he did not smoke, and his cholesterol levels were normal, Aortography revealed marked bilateral iliofemoral involvement, with stenosis at several levels. He underwent bilateral femoral thromboen- darterectomy with no improvement of his symptoms. The cause of the arteriopathy was left undetermined. The pa- tient remained clinically stable for years, but in the months preceding his admission to our center he had progressive right heart failure, with abdominal swelling, edema of the lower limbs, and exercise intolerance. He continued to have intermittent claudication after walking 30 m. He did not complain of arthritis, rash, skin changes, oral ulcers, or cartilage inflammation. Physical examination disclosed jugular distension, and his arterial pressure was 165/90 mm Hg in the right arm and 135/90 in the left. His heart rate was 130 beats/min. He had normal pulses in the upper limbs, but no pulse at all could be detected in the lower limbs. There was a murmur in the left subclavian area; on cardiac auscultation a grade 4/6 holosystolic murmur could be heard in the left sternal border and apex; the second pulmonary sound was increased in intensity. Pulmonary auscultation was normal. The patient had tense ascites and edema in the lower limbs up to the knees. Laboratory studies showed a slight alteration in liver function tests and a prolonged prothrombin time; the erythrocyte sedimen- tation rate was 4 mm at 1 hour. Electrocardiography (ECG) disclosed atria1 flutter with 2:l conduction, signs of right ventricle enlargement, and right bundle branch block. Chest x-ray film revealed moderate cardiomegaly and an enlarged right pulmonary artery (PA); the left PA could not be visualized. The left lung was slightly reduced in size and appeared with diminished pulmonary flow. Echocardio- gram showed enlargement of the right cavities, moderate tricuspid regurgitation, and signs of severe pulmonary hy- pertension (PH); the left cavities were normal. Pulmonary perfusion scan indicated absence of perfusion to the left lung. Aortography disclosed proximal segmentary stenosis of the left subclavian artery and complete obstruction of the infrarenal aorta, inferior mesenteric artery, and both common iliac arteries (Fig. 1). Both deep femoral arteries were filled via collateral circulation. Linear calcification involving the aortic arch and descending thoracic and ab- dominal aorta could be observed. Pulmonary arteriography was also performed, showing a marked dilatation of the main PA and its right branch and a total stoppage of the left branch near its origin (Fig. 2). PA pressures were 90/30 mm Hg (mean 45). Pulmonary wedge pressure was 14 mm Hg. The patient was administered digitalis, diuretics, and warfarin, with moderate clinical improvement. The vascu- lar lesions were not considered to be susceptible to surgical repair.

Volume 127, Number 2
American Heart Journal Shirali et al. 451
Fig. 1. Digital substraction angiography of aorta showing total stoppage below level of renal arteries (arrow).
Fig. 2. Pulmonary angiography in posteroanterior projec- tion showing abrupt cutoff of left pulmonary artery. Marked dilatation of right pulmonary artery is also seen.
This case fulfills the diagnostic criteria for TD recently defined by the American College of Rheumato1ogy.l The involvement of pulmonary circulation justifies its inclusion in group IV of the classification of Lupi-Herrera et al.” In TD, pulmonary vascular involvement is common (up to 50 % of cases),” with stenotic lesions, solitary or multiple, of varying degrees that can affect the pulmonary arterial tree at any level. Generally, the pulmonary involvement has no clinical impact, although in some cases PH develops. Symptoms and signs of right heart failure caused by PH are extremely rare; we have only found one such report in the literature.4 Other disorders can be considered in the differential diagnosis of this disease. Arteriosclerosis pro- duces vascular involvement, mainly of the abdominal aorta, especially in the aortoiliac region, but this diagnosis seems very improbable given the age of onset and the ah-
sence of vascular risk factors and would not explain the in- volvement of lung. Agenesis of left PA might produce a similar angiographic image, but resting PH is uncommon in adult patients.5 Pulmonary thromboembolism can also produce angiographic images similar to those of our pa- tient,6 but the absence of clinical evidence of acute pulmo- nary embolism and deep vein thrombosis and the normal right PA and its branches, make the diagnosis improbable. Likewise, in the latter two disorders, vascular involvement in the aortic region would remain unexplained. In conclu- sion, we propose that TD be included among the causes of PH and right heart failure in young patients, especially if there are signs of vascular involvement in the aorta and its branches.
REFERENCES
1. Arend WP, Michel BA, Bloch DA, Hunder CG, Calabrese LH, Edworthy SM, Fauci AS, Leavitt RY, Lie JT, Lightfoot RW Jr. The American College of Rheumatology 1990 criteria for the classification of Takayasu arteritis. Arthritis Rheum 1990;33:1129-34.
2. Lupi-Herrera E, SBnchez-Torres G, Marcushamer J, Mi- spireta J, Horwitz S, Vela JE. Takayasu arteritis: clinical study of 107 cases. AM HEART J 1977;93:94-103.
3. Kaichiro Ishikawa. Diagnostic approach and proposed criteria for the clinical diagnosis of Takavasu’s arterionathv. J Am Co11 Cardiol 1988;12:964-72. ”
_ I
4. Moore JW, Reardon MJ, Cooley DA, Vargo TA. Severe Taka- yasu’s arteritis of the pulmonary arteries: report of a case with successful surgical treatment. J Am Co11 Cardiol 1985;5:369- 73.
5. Werber J, Ramilo J, London R, Harris V. Unilateral absence of a nulmonarv artery. Chest 1983:64:729-32.
6. Moser KM, OGon LK, Schlusselberg M, Daily PO, Dembitsky WP. Chronic thromboembolic occlusion in the adult can mimic pulmonary artery agenesis. Chest 1989;95:503-8.
Double aortic arch and bilateral patent ducti arteriosi associated with transposition of the great arteries: Missing clinical link in an embryologic theory
Girish S. Shirali, MD: Tal Geva, MD, David A. Ott, MD,b and J. Timothy Bricker, MDa Houston, Texas
The normal embryologic development of the aortic arches in human beings was first delineated by Congdon.’ Subse- quently, Edwards2 proposed a theory to explain normal and deviant development of the aortic arch system. Ed-
From %he Lillie Frank Abercrombie Section of Cardiology, Texas Children’s Hospital, Department of Pediatrics, Baylor College of Medicine; and the bDepartment of Thoracic and Cardiovascular Surgery, Texas Children’s Hospital, Texas Heart Institute.
Reprint requests: J. Timothy Bricker, MD, Division of Pediatric Cardiology, Texas Children’s Hospital, 6621 Fannin, Suite 260, Houston, TX 77030.
AM HEART J 1994;127:451-3.
Copyright (ii 1994 by Mosby-Year Book, Inc. 0002.8703/94/$1.00 + .lO 4/4/51109



![Significance of Simultaneous Splenic Artery Resection in ... · portal hypertension (LPH), causing variceal bleeding and thrombocytopenia by hypersplenism [3, 4]. Variceal bleeding](https://img.dokumen.tips/doc/110x75/5f08c2047e708231d42393cb/significance-of-simultaneous-splenic-artery-resection-in-portal-hypertension.jpg)























