Embed Size (px)
Citation preview
TAE Trainees Day A time for trainees to share their knowledge under the supervision of seniors Arranged with the ESCMID Trainee Association, German Society for Infectious Diseases (DGI) & Akademie für Infektionsmedizin
Convenors: K. Adams (Hull, GB)
W.V. Kern (Freiburg, DE)
P. Maver (Ljubljana, SI)
Faculty: K. Adams (Hull, GB)
R. Köck (Münster, DE) S. Stone, B. Cookson (London, GB) – no handout available P.A. Grossi (Varese, IT) K. Graf (Hanover, DE)
1
2
Adams - Welcome and TAE President's address
Trainee Association of ESCMIDTrainees Day 2013
Dr Kate AdamsPresident of TAE
Welcome
• Third Trainees Day Session• The only session at ECCMID dedicated to
trainees• Run in collaboration with the German
Society of Infectious Diseases
• To find out more information – visit our website www.escmid.org/tae,– send an e-mail to [email protected] or – contact us through the discussion forum
http://forum.escmid.org– Fill out your evaluation forms!!
3
Adams - Welcome and TAE President's address
Online Quiz
• Running now• Log in through:• Have a go and test your knowledge• Tell a friend• Please fill out the demographic data
4
Köck - Hidden dangers: important epidemiological links between infections and animal exposure
Hidden dangers: importantepidemiological links betweeninfections and animal exposure
Robin Koeck, MD
University Hospital Münster
Institute of Hygiene & National Consulting Laboratory for Hemolytic Uremic Syndrome
Münster, Germany
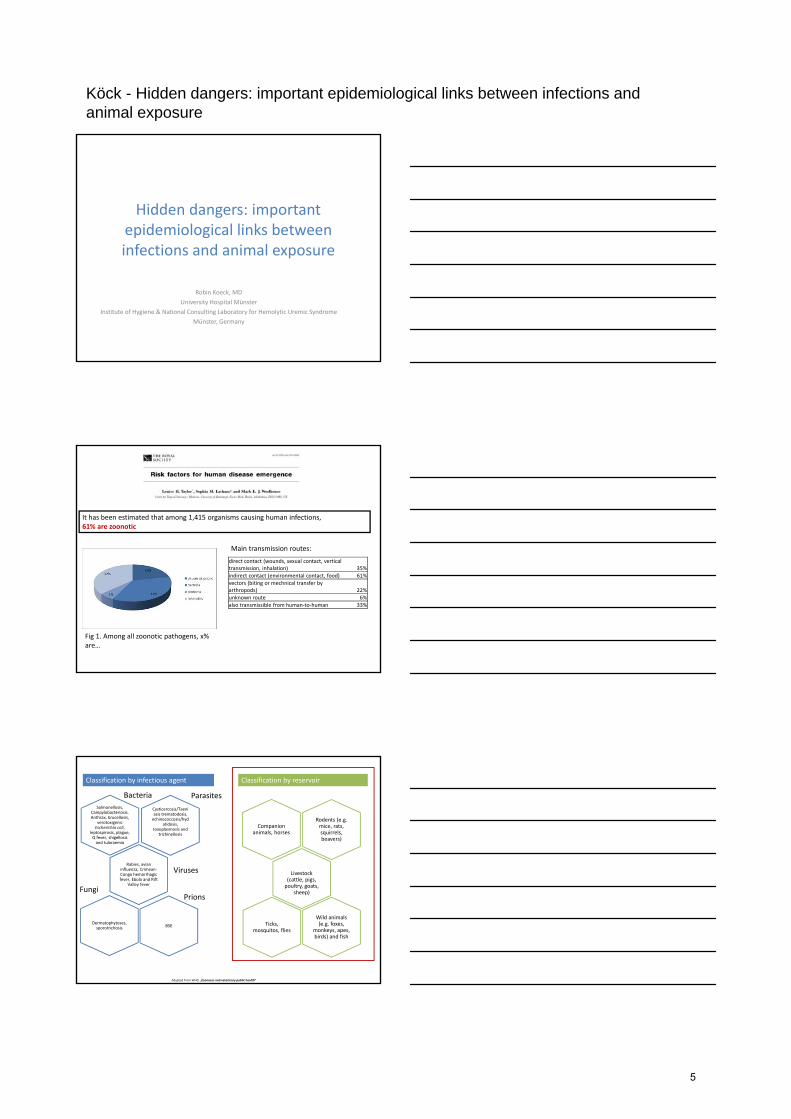
It has been estimated that among 1,415 organisms causing human infections, 61% are zoonotic
direct contact (wounds, sexual contact, vertical transmission, inhalation) 35%
indirect contact (environmental contact, food) 61%
vectors (biting or mechnical transfer by arthropods) 22%
unknown route 6%
also transmissible from human‐to‐human 33%
Main transmission routes:
Fig 1. Among all zoonotic pathogens, x% are…
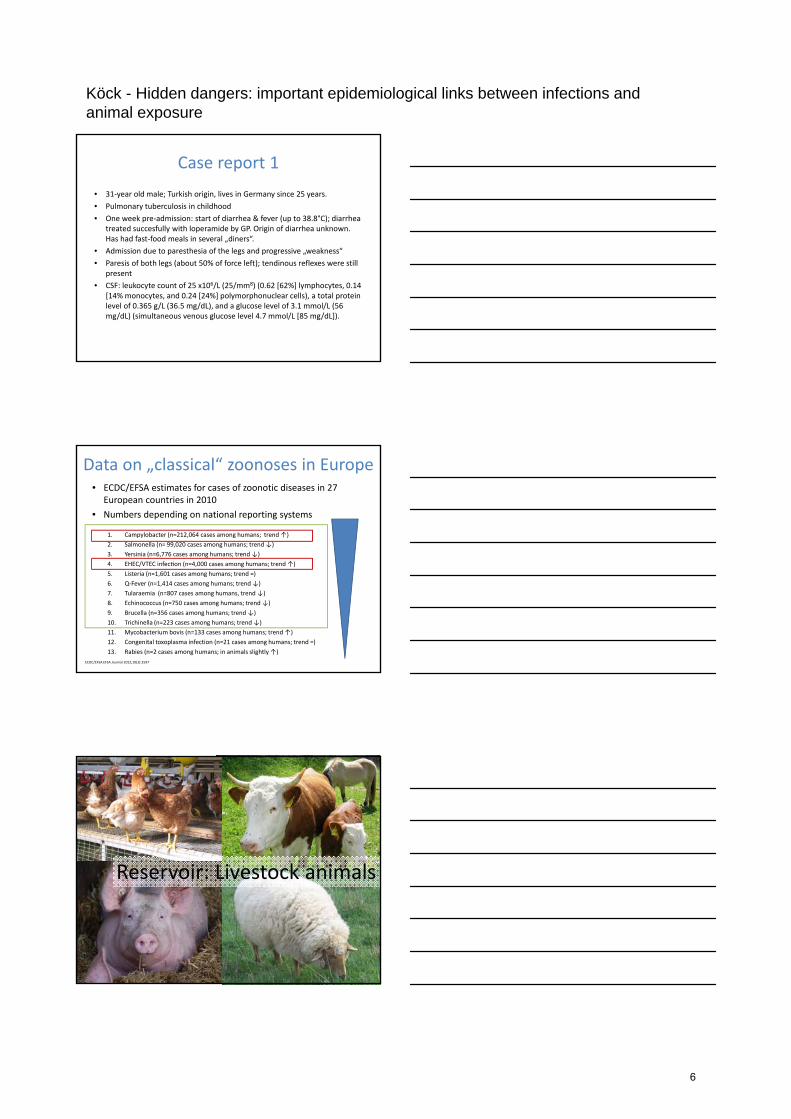
Classification by infectious agent Classification by reservoir
Salmonellosis, Campylobacteriosis. Anthrax, brucellosis,
verotoxigenicEscherichia coli,
leptospirosis, plague, Q fever, shigellosisand tularaemia
Bacteria
Cysticercosis/Taeniasis trematodosis, echinococcosis/hyd
atidosis, toxoplasmosis and
trichinellosis
Rabies, avian influenza, Crimean‐Congo hemorrhagic fever, Ebola and Rift
Valley fever
Dermatophytoses, sporotrichosis
Parasites
Viruses
Fungi
Adapted from WHO „Zoonoses and veterinary public health”
Ticks, mosquitos, flies
Wild animals(e.g. foxes,
monkeys, apes, birds) and fish
BSE
Prions
Companion animals, horses
Livestock (cattle, pigs, poultry, goats,
sheep)
Rodents (e.g. mice, rats, squirrels, beavers)
5
Köck - Hidden dangers: important epidemiological links between infections and animal exposure
Case report 1
• 31‐year old male; Turkish origin, lives in Germany since 25 years.
• Pulmonary tuberculosis in childhood
• One week pre‐admission: start of diarrhea & fever (up to 38.8°C); diarrhea treated succesfully with loperamide by GP. Origin of diarrhea unknown. Has had fast‐food meals in several „diners“.
• Admission due to paresthesia of the legs and progressive „weakness“
• Paresis of both legs (about 50% of force left); tendinous reflexes were still present
• CSF: leukocyte count of 25 x106/L (25/mm8) (0.62 [62%] lymphocytes, 0.14 [14% monocytes, and 0.24 [24%] polymorphonuclear cells), a total protein level of 0.365 g/L (36.5 mg/dL), and a glucose level of 3.1 mmol/L (56 mg/dL) (simultaneous venous glucose level 4.7 mmol/L [85 mg/dL]).
Data on „classical“ zoonoses in Europe• ECDC/EFSA estimates for cases of zoonotic diseases in 27
European countries in 2010
• Numbers depending on national reporting systems
1. Campylobacter (n=212,064 cases among humans; trend ↑)
2. Salmonella (n= 99,020 cases among humans; trend ↓)
3. Yersinia (n=6,776 cases among humans; trend ↓)
4. EHEC/VTEC infec on (n=4,000 cases among humans; trend ↑)
5. Listeria (n=1,601 cases among humans; trend =)
6. Q‐Fever (n=1,414 cases among humans; trend ↓)
7. Tularaemia (n=807 cases among humans, trend ↓)
8. Echinococcus (n=750 cases among humans; trend ↓)
9. Brucella (n=356 cases among humans; trend ↓)
10. Trichinella (n=223 cases among humans; trend ↓)
11. Mycobacterium bovis (n=133 cases among humans; trend ↑)
12. Congenital toxoplasma infection (n=21 cases among humans; trend =)
13. Rabies (n=2 cases among humans; in animals slightly ↑)
ECDC/EFSA EFSA Journal 2012;10(3):2597
Reservoir: Livestock animals
6
Köck - Hidden dangers: important epidemiological links between infections and animal exposure
Direct professional exposure to livestock
Direct exposure to livestock environment
Exposure to contaminated meat items (ingestion & handling)
Risk factors for transmission between humans and livestock
Poultry
• Salmonella: 1‐2% of the EU breeding flocks are positive (5 target serovars) 6% in laying hen flocks; trends downward.
• Campylobacter: at retail 30% of samples (range 3‐59%) are contaminated
• VTEC / EHEC: 0‐14% (Belgium) of meat samples VTEC positive; 0% positive for VTEC O157.
ECDC/EFSA EFSA Journal 2012;10(3):2597
Pigs
• Salmonella: 0.5‐1% of the animals; 6‐7% of the herds contaminated
• Campylobacter: at retail 0.6% of meat samples contaminated
• VTEC / EHEC: 1‐2% of meat samples VTEC positive; 0‐1% positive for VTEC O157.
• Yersinia: 2‐5% of the meat samples intended to be cooked were contaminated
ECDC/EFSA EFSA Journal 2012;10(3):2597
7
Köck - Hidden dangers: important epidemiological links between infections and animal exposure
Cattle
• Salmonella: 1% of the animals; 8% of the herds contaminated
• Campylobacter: at retail 0.4% of meat samples contaminated
• VTEC / EHEC: 0.5% of meat samples VTEC positive (range 0‐5.4%); 0.1% positive for VTEC O157. Raw‐milk: 3.3% (up to 18% in Germany)
ECDC/EFSA EFSA Journal 2012;10(3):2597
Livestock animals: Wolfs in sheep‘s clothing?
VTEC & food production animals:reliable detection vs. only „eyes of
the crocodile“?
8
Köck - Hidden dangers: important epidemiological links between infections and animal exposure
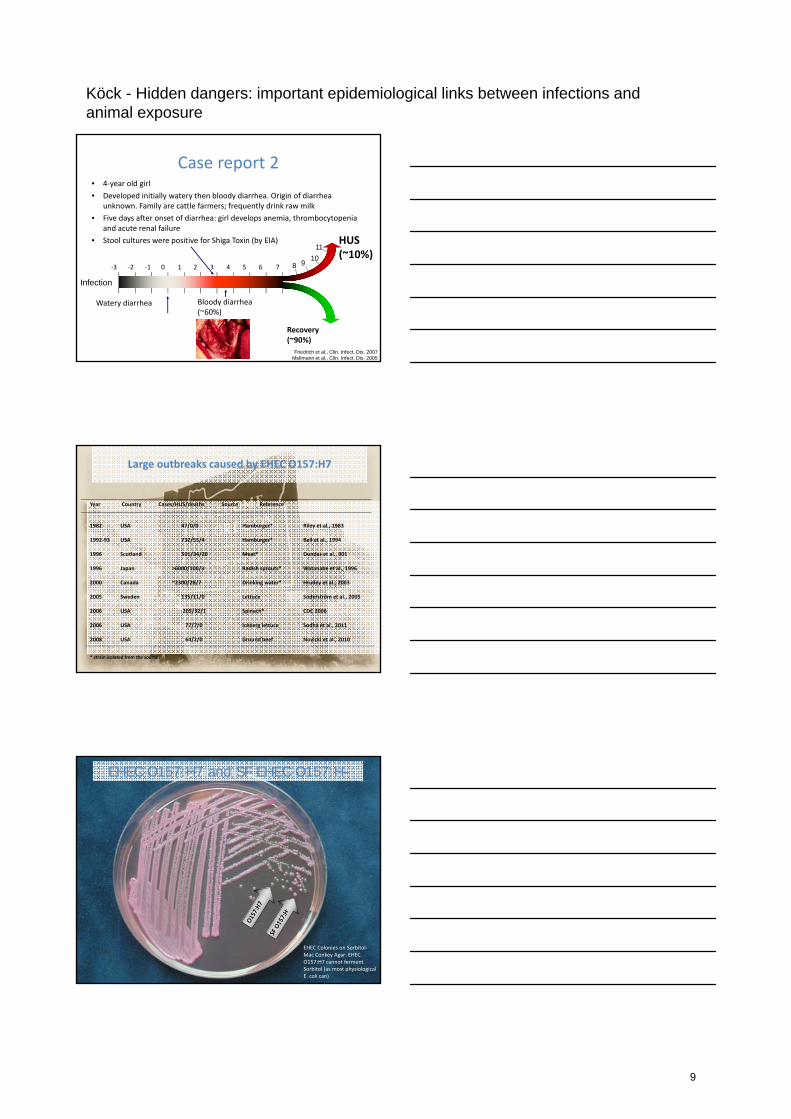
Case report 2• 4‐year old girl
• Developed initially watery then bloody diarrhea. Origin of diarrhea unknown. Family are cattle farmers; frequently drink raw milk
• Five days after onset of diarrhea: girl develops anemia, thrombocytopenia and acute renal failure
• Stool cultures were positive for Shiga Toxin (by EIA)
Recovery(~90%)
HUS(~10%)
Friedrich et al., Clin. Infect. Dis. 2007Mellmann et al., Clin. Infect. Dis. 2005
‐3 ‐2 ‐1 0 1 2 3 4 5 6 7 8 910
11
Watery diarrhea Bloody diarrhea(~60%)
Infection
Large outbreaks caused by EHEC O157:H7
Year Country Cases/HUS/deaths Source Reference
1982 USA 47/0/0 Hamburger* Riley et al., 1983
1992‐93 USA 732/55/4 Hamburger* Bell et al., 1994
1996 Scotland 501/34/20 Meat* Dundas et al., 001
1996 Japan >6000/100/3 Radish sprouts* Watanabe et al., 1996
2000 Canada ~2300/28/7 Drinking water* Hrudey et al., 2003
2005 Sweden 135/11/0 Lettuce Söderström et al., 2005
2006 USA 205/32/1 Spinach* CDC 2006
2006 USA 77/7/0 Iceberg lettuce Sodha et al., 2011
2008 USA 64/2/0 Ground beef Novicki et al., 2010
* strain isolated from the source
EHEC O157:H7 and SF EHEC O157:H-
EHEC Colonies on Sorbitol‐Mac Conkey Agar: EHEC O157:H7 cannot ferment Sorbitol (as most physiological E. coli can)
9

Köck - Hidden dangers: important epidemiological links between infections and animal exposure
EHECStx 1,2 +eae +/‐
STECStx 1,2 positiveeae negative
Mainly colonizing animals Subgroup of Shiga toxin-
producing E. coli (STEC)
380 EHEC serotypes isolated from humans with gastrointestinal disease (O157:H7, non-O157)
42 different strains of HUS-associated E. coli (HUSEC001 –HUSEC042) in Germany
6 confirmed HUS outbreaks in Germany (1988-2010)
EHEC vs STEC
Reliable detection of VTEC in food samples?
EFSA Journal 2009; 7(11):1366, Technical specifications for the monitoring and reporting ofverotoxigenic Escherichia coli (VTEC) on animals and food (VTEC surveys on animals and food)
Normal flora: green = variant susceptible to the selective stimulus; red = resistant to the selective stimulus
Selection process
Selective stimulus: e.g. antibiotics (disinfection, pH, temperature, metals…)
Predominance of resistant variant
Faciliated dissemination (high number of colony forming units) via direct and indirect transmission
Antibiotic use in animals & humans
Animal reservoir of antibiotic resistance
Human reservoir of antibiotic resistance
10

Köck - Hidden dangers: important epidemiological links between infections and animal exposure
ESBL in fecal/rectal samples from cattle, pigs, chickens
UK: 31/48 calves and 2/60 cows carry ESBL‐E. coli. Liebana JCM 2006
China: 3.1% of cattle ESBL‐E. coli positive. Duan RS Micro Drug Resist 2006
Japan: ESBL‐E. coli were in 12.5% of beef cattle. Hiroi M J Vet Med Sci. 2012
France: mastitis cases: 0.4% (6/1427) of E. coli/K. pneumoniae carried an ESBL gene. Dahmen S Vet Microbiol. 2013
Switzerland: 17.1% of fecal samples, mostly calves, ESBL positive. Geser N J Food
Prot 2011
Korea: 1/654 (0.2%) cattle fecal samples was positive for ESBL. Tamang MD
Foodborne Pathog Dis. 2013
Bavaria: n=196/598 (32.8%) ESBL E. coli positive; 39/45 farms 86.7%. Schmid A
Appl Environ Microbiol 2013
UK: ESBL‐E. coli were isolated from 54.5% of the broiler abattoirs and from 3.6% of individual broiler caecal samples . Randall LP JAC 2011
Poland: ESBL in 42.3% of samples from layers, 48.0% from turkey, and 54.5% from broilers. Wasyl D Microb Drug
Resist. 2012
Japan: ESBL‐carrying E. coli were isolated from 60.0% of individual broiler rectal samples, 5.9% of layers. Hiroi M J Vet Med Sci. 2012
Portugal: Cefotaxime‐resistant E. coli were recovered from 32 broiler fecal samples (42.1%). Costa D Vet Microbiol
2009
China: 2% of pigs had ESBL‐E. coli. Duan RS Micro Drug Resist 2006
China: faecal carriage rate of ESBL‐E. coli was 63.6% inpigs. Ho PL J Antimicrob Chemother. 2011
Poland: ESBL in 33.3% of samples from pigs. Wasyl D Microb Drug Resist. 2012
Japan: ESBL‐carrying E. coli in 3% of pigs. Hiroi M J Vet Med Sci. 2012
Czech Republic: 7/118 rectal samples from pigs were positive for ESBL‐E. coli. Bardon J Klin Mikrobiol Infekc Lek 2012
Switzerland: 15.2% of the porcine fecal samples yielded ESBL producers. Geser N J Food Prot 2011
Korea: 21.5% of swine fecal samples ESBL positive. Tamang MD Foodborne Pathog Dis. 2013
MRSA in samples from cattle, pigs, chickens
Belgium: MRSA carriage was 64% in calves, 5% in beef, 1% in dairy cows. Vandendriessche S JAC 2013
Germany: MRSA detected in nasal swabs of cows (7/15) and calves (4/7). Spohr M Zoonoses Public Health 2011
Netherlands: 50% of the beef calvesCarried LA‐MRSA in their nose. Vanderhaeghen W Epidemiol Infect 2010
Belgium: MRSA carriage 3% in broilers. Vandendriessche S JAC 2013
Germany: at farm level 18/20 (90%) of all urkey flocks were MRSA positive. Richter A Epidemiol Infect 2012
Belgium: Broiler flock prevalence 0‐28%. Plentickx LJ Infect Genet Evol. 2011
Netherlands: 7% of all broilers, 35% of all broiler farms MRSA positive. Mulders MN Epidemiol Infect 2010
Prevalence at farm level:
Netherlands: 23‐81% of the farms with MRSA positive pigs. Huijsdens XW Ann Cin Microbiol
Antimicrob 2006, van Duijkeren E Vet Microbiol 2008
Germany: 70% of the farms with MRSA positive pigs. Köck R EJMID 2010
Denmark: 66% of the farms with MRSA positive pigs. Guardabassi L Vet Microbiol 2007
Belgium: 68% of the farms with MRSA positive pigs. Willems G 2nd Symposium on Antimicrobial
Resistance in Animals and the Environment, 2007
Canada: 45% of the farms with MRSA positive pigs. Khanna T Vet Microbiol 2008
MRSA/ESBL contamination in food items at retail
Proportion of MRSA positive food items (%); German national Monitoring of zoonotic food pathogens 2009 and Dutch data (de Boer et al. 2009).
ESBL‐producing enterobacteria:
Chicken: 6‐38% ESBL‐producing enterobacteria positive (Kola A JAC 2012; German
National Institute for Risk Assessment (BfR) Nr. 002/2012 )
Pig meat: 2% ESBL‐E. coli positive (German National Institute for Risk Assessment (BfR) Nr. 002/2012 )
MRSA:
11
Köck - Hidden dangers: important epidemiological links between infections and animal exposure
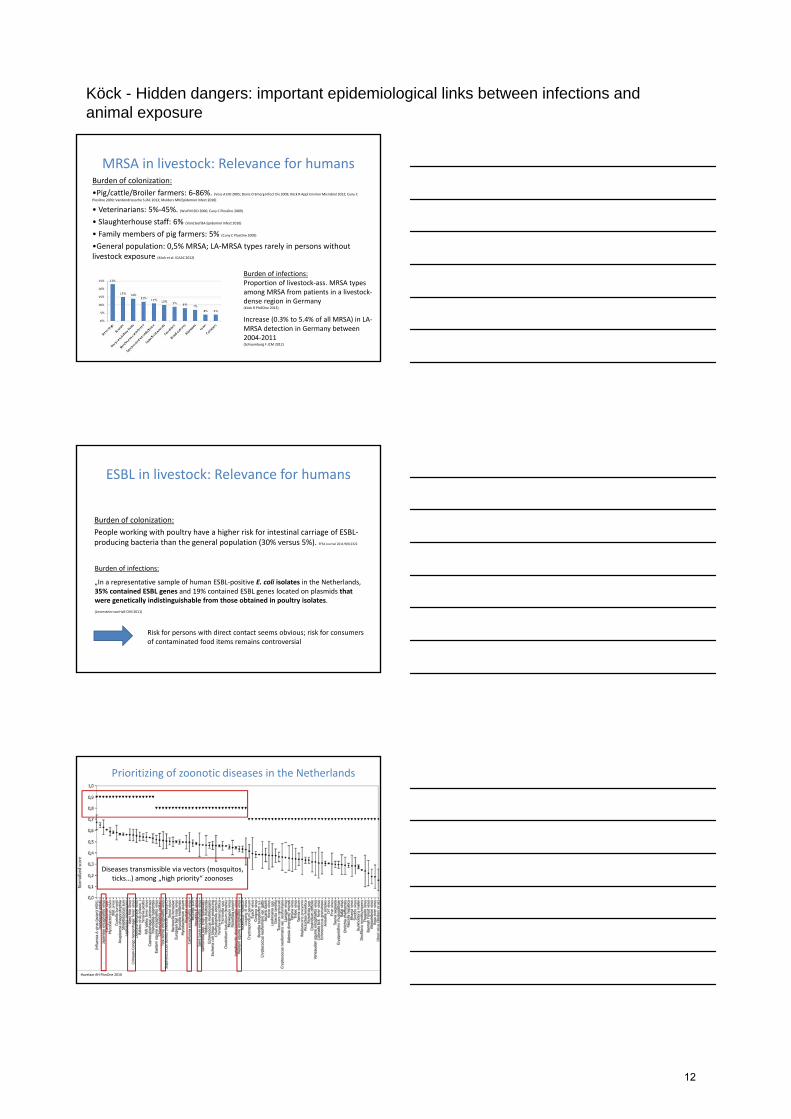
MRSA in livestock: Relevance for humansBurden of colonization:
•Pig/cattle/Broiler farmers: 6‐86%. (Voss A EID 2005; Denis O Emerg Infect Dis 2009; Köck R Appl Environ Microbiol 2012; Cuny C
PlosOne 2009; Vandendriessche S JAC 2013; Mulders MN Epidemiol Infect 2010)
• Veterinarians: 5%‐45%. (Wulf M EID 2006; Cuny C PlosOne 2009)
• Slaughterhouse staff: 6% (VanCleef BA Epidemiol Infect 2010)
• Family members of pig farmers: 5% (Cuny C PlosOne 2009)
•General population: 0,5% MRSA; LA‐MRSA types rarely in persons without livestock exposure (Köck et al. ICAAC 2012)
Burden of infections:Proportion of livestock‐ass. MRSA types among MRSA from patients in a livestock‐dense region in Germany(Köck R PloSOne 2013)
Increase (0.3% to 5.4% of all MRSA) in LA‐MRSA detection in Germany between 2004‐2011(Schaumburg F JCM 2012)
ESBL in livestock: Relevance for humans
Burden of colonization:
People working with poultry have a higher risk for intestinal carriage of ESBL‐producing bacteria than the general population (30% versus 5%). EFSA Journal 2011;9(8):2322
Burden of infections:
„In a representative sample of human ESBL‐positive E. coli isolates in the Netherlands, 35% contained ESBL genes and 19% contained ESBL genes located on plasmids thatwere genetically indistinguishable from those obtained in poultry isolates.
(Leverstein‐van Hall CMI 2011)
Risk for persons with direct contact seems obvious; risk for consumers of contaminated food items remains controversial
Havelaar AH PlosOne 2010
Diseases transmissible via vectors (mosquitos, ticks…) among „high priority“ zoonoses
Prioritizing of zoonotic diseases in the Netherlands
12
Köck - Hidden dangers: important epidemiological links between infections and animal exposure
Mosquito‐borne transmission
Climate Change mean temperature;extreme temperatures;precipitation;
may have influence on the occurence of both vectors and hosts
GlobalisationInternational travel; International transport; Human population growth /aggregation;
may faciliatate dissemination of vectors / and infected humans
Conclusions
• Huge burden of zoonotic diseases in European countries by livestock / food‐producing animals
• Link between burden of antimicrobial resistance in humans and animals
• Climate change and internationalisation impact on occurrence of vector‐borne diseases
Consider the positive aspects of climate change….
Thank you for your attention
13
Grossi - Surgical site infections - ID perspective
Paolo Grossi
SURGICAL SITE INFECTIONS – ID PERSPECTIVE
Infectious & Tropical Diseases UnitDepartment of Transplantation
Ospedale di Circolo e Fondazione Macchi –University of Insubria, Varese,Italy
TAE TRAINEES DAYECCMID 2013 ‐ BERLIN
Clinical presentations of SSTIs
• ~0.1% of adult population requires hospital treatment for SSTIs each year • SSTIs may become complicated if require hospitalisation, surgery, involve
deeper tissues, co-morbidities or systemic symptoms
Eron LJ, et al. J Antimicrob Chemother 2003; 52 Suppl1:i3–17
Skin and soft tissue infections
Infectedulcer
Infectedwound
Diabetic footinfection
Surgical siteinfection
Necrotising SSTI
Cellulitis
Abscess
Surgical Site Infections (SSI)
• Third most common nosocomial infection (14%–16%)
• Most common nosocomial infection among surgical patients (38%)
– 2/3 incisional
– 1/3 organs or spaces accessed during surgery
• 7.3 additional postoperative days at cost of $3,152 in extra charges
Mangram AJ et al. Infect Control Hosp Epidemiol. 1999;20:250‐278.
14
Grossi - Surgical site infections - ID perspective
Surgical Site Infection (SSI)
• A surgical site infection is an infection that occurs aftersurgery in the part of the body where the surgery tookplace.
• Surgical site infections can sometimes be superficialinfections involving the skin only.
• Other surgical site infections are more serious and can involve tissues under the skin, organs, or implantedmaterial.
• CDC provides guidelines and tools to the healthcarecommunity to help end surgical site infections and resources to help the public understand these infectionsand take measures to safeguard their own health whenpossible.
Surgical site infections include:
• Those occurring post‐operatively and those severe enough to require surgical intervention for diagnosis and treatment.
• Surgical site infection rarely occurs during the first 48 h after surgery, and fever during that period usually arises from noninfectious or unknown causes.
• In contrast, after 48 h, surgical site infection is a more common source of fever, and careful inspection of the wound is indicated.
• Most SSIs have no clinical manifestations for at least 5 days after the operation, and many may not become apparent for up to 2 weeks.
Surgical site infections• For patients with a temperature <38.5°C and without
tachycardia, observation, dressing changes, or opening the incision site suffices.
• Patients with a temperature >38.5°C or a heart rate >110 beats/min generally require antibiotics as well as opening of the suture line.
• Infections developing after surgical procedures involving nonsterile tissue, such as colonic, vaginal, biliary or respiratory mucosa, may be caused by a combination of aerobic and anaerobic bacteria. These infections can rapidly progress and involve deeper structures than just the skin, such as fascia, fat, or muscle.
15
Grossi - Surgical site infections - ID perspective
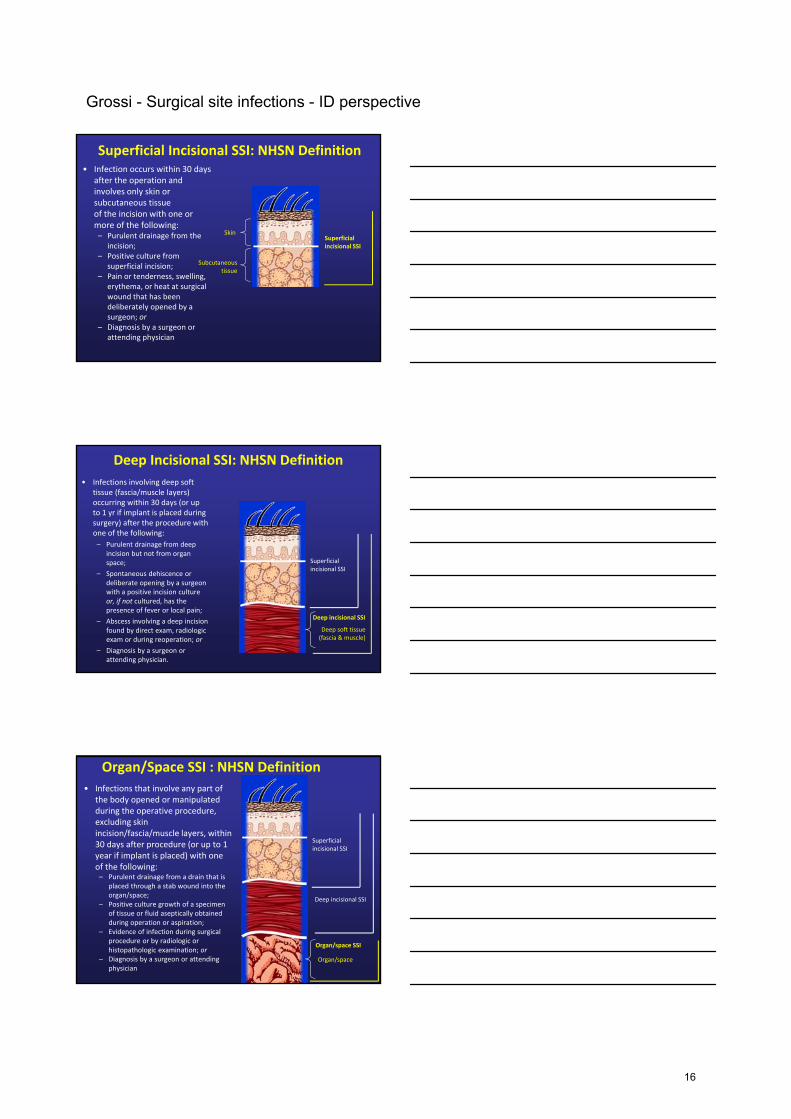
Superficial Incisional SSI: NHSN Definition• Infection occurs within 30 days
after the operation and involves only skin or subcutaneous tissue of the incision with one or more of the following:– Purulent drainage from the
incision;– Positive culture from
superficial incision;– Pain or tenderness, swelling,
erythema, or heat at surgical wound that has been deliberately opened by a surgeon; or
– Diagnosis by a surgeon or attending physician
Subcutaneous tissue
SkinSuperficial incisional SSI
Deep Incisional SSI: NHSN Definition
• Infections involving deep soft tissue (fascia/muscle layers) occurring within 30 days (or up to 1 yr if implant is placed during surgery) after the procedure with one of the following:
– Purulent drainage from deep incision but not from organ space;
– Spontaneous dehiscence or deliberate opening by a surgeon with a positive incision culture or, if not cultured, has the presence of fever or local pain;
– Abscess involving a deep incision found by direct exam, radiologic exam or during reoperation; or
– Diagnosis by a surgeon or attending physician.
Deep soft tissue (fascia & muscle)
Deep incisional SSI
Superficial incisional SSI
Organ/Space SSI : NHSN Definition
• Infections that involve any part of the body opened or manipulated during the operative procedure, excluding skin incision/fascia/muscle layers, within 30 days after procedure (or up to 1 year if implant is placed) with one of the following:– Purulent drainage from a drain that is
placed through a stab wound into the organ/space;
– Positive culture growth of a specimen of tissue or fluid aseptically obtained during operation or aspiration;
– Evidence of infection during surgical procedure or by radiologic or histopathologic examination; or
– Diagnosis by a surgeon or attending physician
Deep incisional SSI
Superficial incisional SSI
Organ/space SSI
Organ/space
16
Grossi - Surgical site infections - ID perspective
SSI – Risk FactorsOperation Factors
• Duration of surgical scrub• Maintain body temp• Skin antisepsis• Preoperative shaving• Duration of operation• Antimicrobial prophylaxis• Operating room ventilation• Inadequate sterilization of
instruments
Mangram AJ et al. Infect Control Hosp Epidemiol. 1999;20:250‐278.
• Foreign material at surgical site
• Surgical drains• Surgical technique
– Poor hemostasis– Failure to obliterate dead space
– Tissue trauma
SSI – Risk FactorsPatient Characteristics
• Age
• Diabetes– HbA1C and SSI
– Glucose > 200 mg/dL postoperative period (<48 hours)
• Nicotine use: delays primary wound healing
• Steroid use: controversial
• Malnutrition: no epidemiological association
• Obesity: 20% over ideal body weight
Mangram AJ et al. Infect Control Hosp Epidemiol. 1999;20:250‐278.
• Prolonged preoperative stay: surrogate of the severity of illness and comorbid conditions
• Preoperative nares colonization with Staphylococcus aureus: significant association
• Perioperative transfusion: controversial
• Coexistent infections at a remote body site
• Altered immune response
SSI – Wound Classification
• Class 1 = Clean
• Class 2 = Clean contaminated
• Class 3 = Contaminated
• Class 4 = Dirty infected
Mangram AJ et al. Infect Control Hosp Epidemiol. 1999;20:250-278.
Prophylactic antibiotics indicated
Therapeutic antibiotics
17
Grossi - Surgical site infections - ID perspective
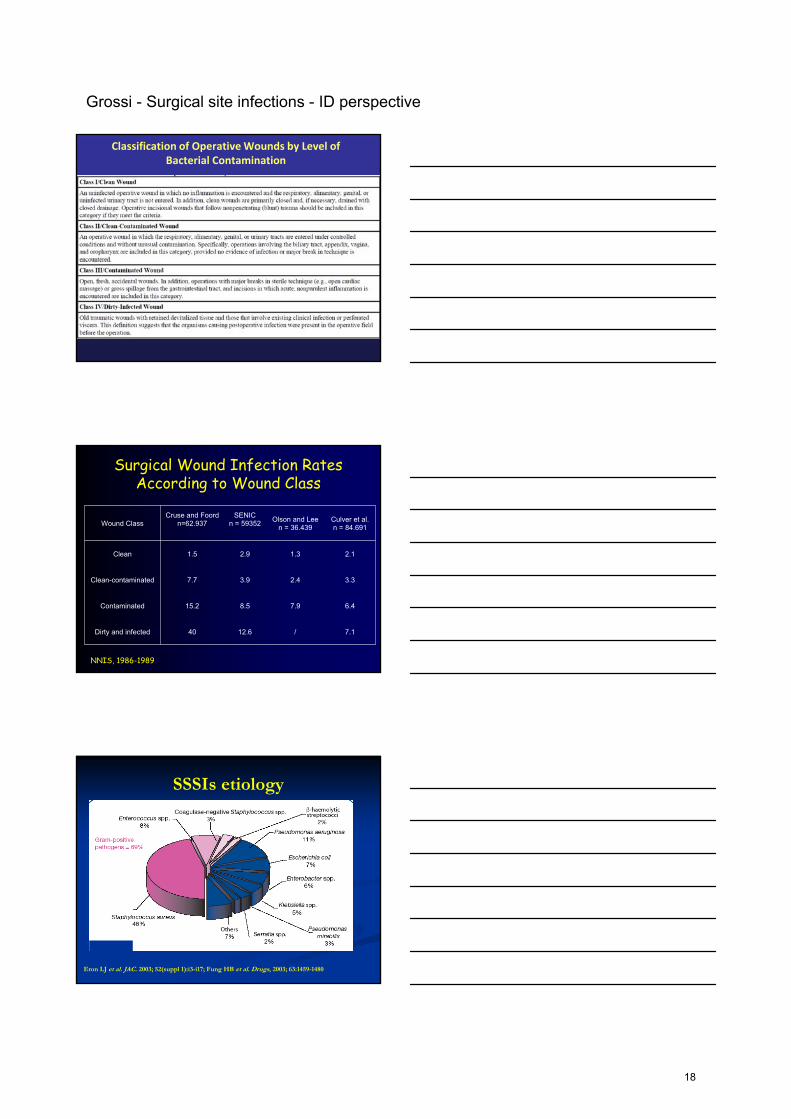
Classification of Operative Wounds by Level of Bacterial Contamination
Surgical Wound Infection Rates According to Wound Class
Wound ClassCruse and Foord
n=62.937SENIC
n = 59352Olson and Lee
n = 36.439Culver et al.n = 84.691
Clean 1.5 2.9 1.3 2.1
Clean-contaminated 7.7 3.9 2.4 3.3
Contaminated 15.2 8.5 7.9 6.4
Dirty and infected 40 12.6 / 7.1
NNIS, 1986-1989
SSSIs etiology
Eron LJ et al. JAC. 2003; 52(suppl 1):i3-i17; Fung HB et al. Drugs, 2003; 63:1459-1480
18
Grossi - Surgical site infections - ID perspective
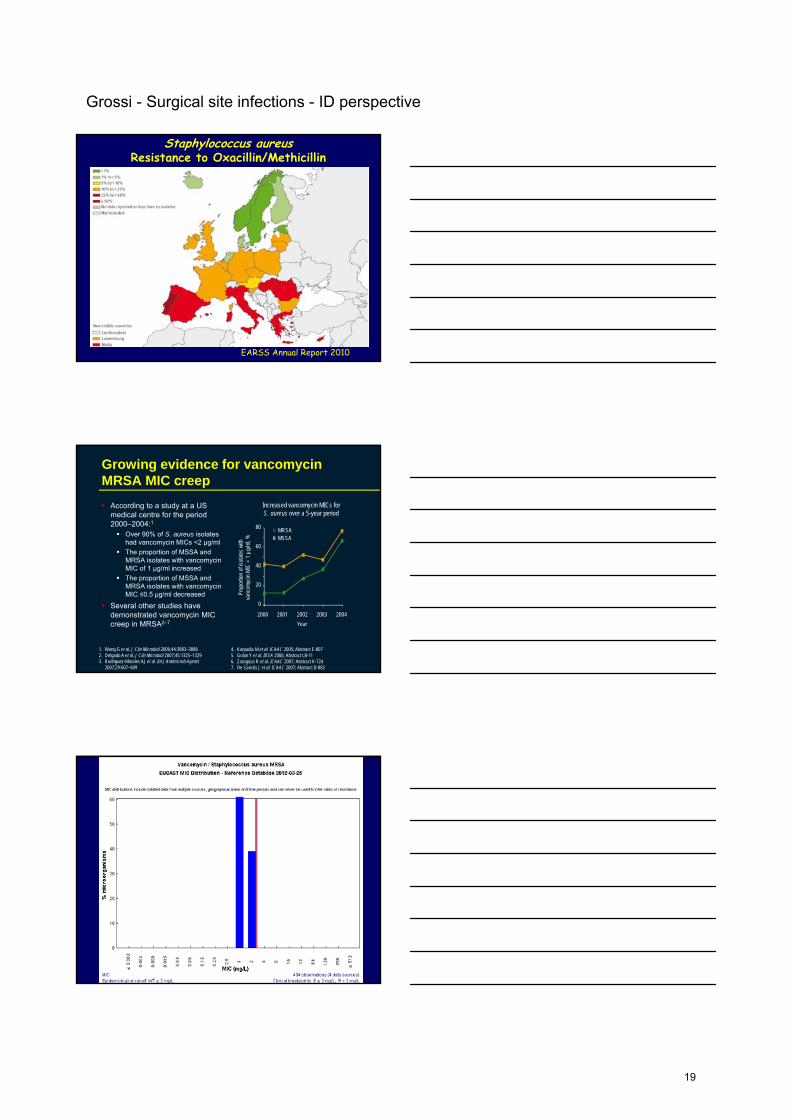
Staphylococcus aureusResistance to Oxacillin/Methicillin
EARSS Annual Report 2010
Growing evidence for vancomycin MRSA MIC creep
According to a study at a US medical centre for the period 2000–2004:1
Over 90% of S. aureus isolates had vancomycin MICs <2 μg/ml
The proportion of MSSA and MRSA isolates with vancomycin MIC of 1 µg/ml increased
The proportion of MSSA and MRSA isolates with vancomycin MIC ≤0.5 µg/ml decreased
Several other studies have demonstrated vancomycin MIC creep in MRSA2–7
Increased vancomycin MICs for S. aureus over a 5-year period
80
60
40
20
0
MRSAMSSA
2000 2001 2002 2003 2004
Prop
ortio
n of
isol
ates
with
va
ncom
ycin
MIC
= 1
µg/
ml,
%
Year
1. Wang G et al. J Clin Microbiol 2006;44:3883–38862. Delgado A et al. J Clin Microbiol 2007;45:1325–13293. Rodriguez-Morales AJ et al. Int J Antimicrob Agents
2007;29:607–609
4. Karpadia M et al. ICAAC 2005; Abstract E-807 5. Golan Y et al. IDSA 2006; Abstract LB-116. Zaragoza R et al. ICAAC 2007; Abstract K-7247. De Sanctis J et al. ICAAC 2007; Abstract D-882
19
Grossi - Surgical site infections - ID perspective
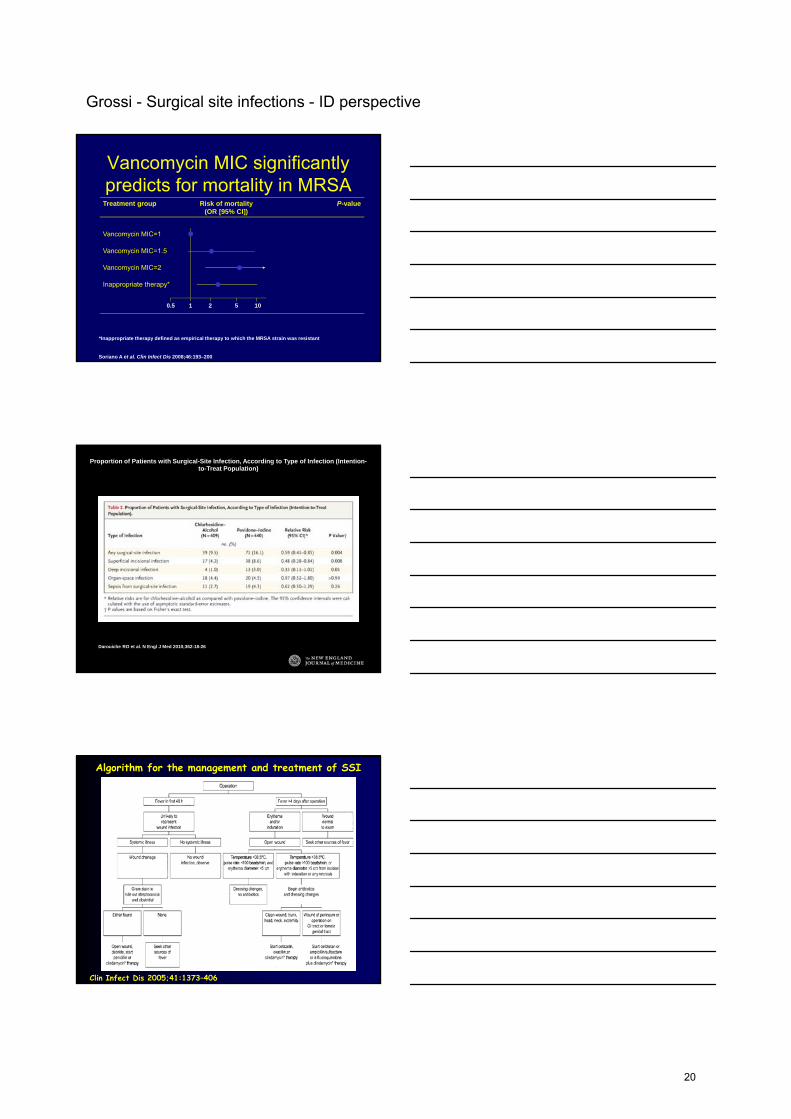
Vancomycin MIC significantly predicts for mortality in MRSA
Soriano A et al. Clin Infect Dis 2008;46:193–200
Treatment group Risk of mortality (OR [95% CI])
P-value
Vancomycin MIC=1 1
Vancomycin MIC=1.5 2.86 (0.87, 9.35) 0.08
Vancomycin MIC=2 6.39 (1.68, 24.3) <0.001
Inappropriate therapy* 3.62 (1.20, 10.9) <0.001
0.5 1 2 5 10
*Inappropriate therapy defined as empirical therapy to which the MRSA strain was resistant
Proportion of Patients with Surgical-Site Infection, According to Type of Infection (Intention-to-Treat Population)
Darouiche RO et al. N Engl J Med 2010;362:18-26
Algorithm for the management and treatment of SSI
Clin Infect Dis 2005;41:1373–406
20
Grossi - Surgical site infections - ID perspective
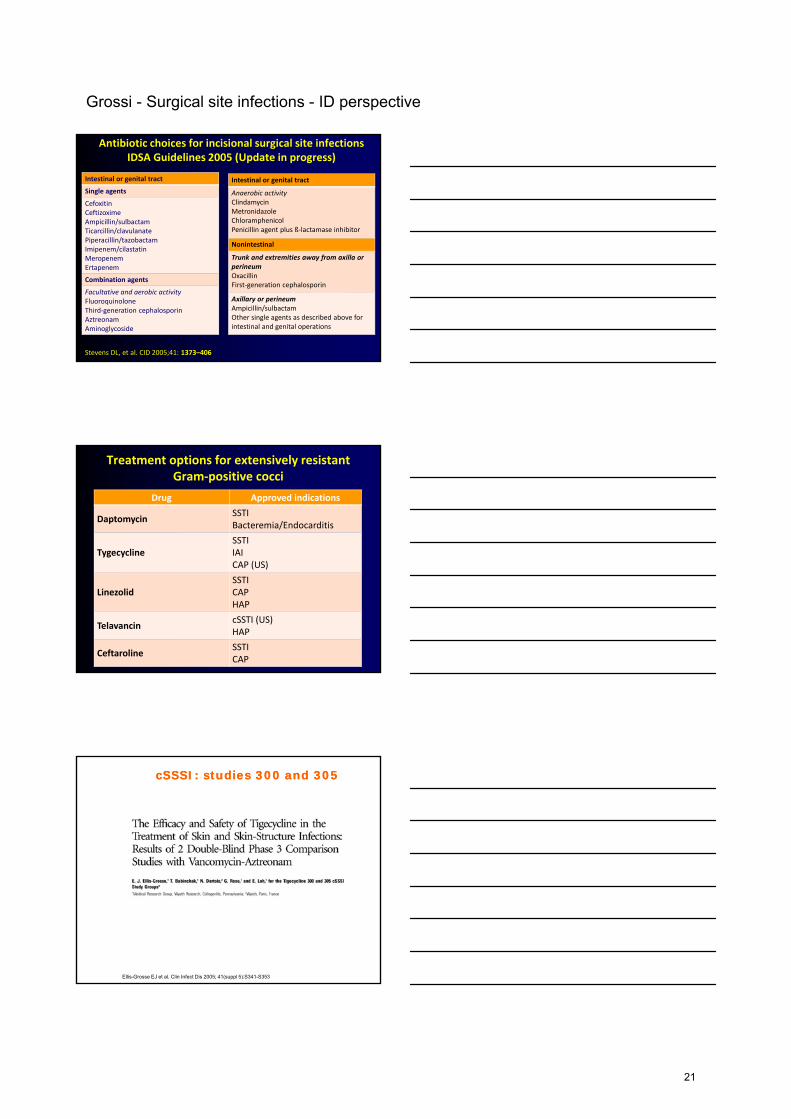
Antibiotic choices for incisional surgical site infectionsIDSA Guidelines 2005 (Update in progress)
• Cefoxitin
Intestinal or genital tract
Single agents
CefoxitinCeftizoximeAmpicillin/sulbactamTicarcillin/clavulanatePiperacillin/tazobactamImipenem/cilastatinMeropenemErtapenem
Combination agents
Facultative and aerobic activityFluoroquinoloneThird‐generation cephalosporinAztreonamAminoglycoside
Intestinal or genital tract
Anaerobic activityClindamycinMetronidazoleChloramphenicolPenicillin agent plus ß‐lactamase inhibitor
Nonintestinal
Trunk and extremities away from axilla or perineumOxacillinFirst‐generation cephalosporin
Axillary or perineumAmpicillin/sulbactamOther single agents as described above for intestinal and genital operations
Stevens DL, et al. CID 2005;41: 1373–406
Treatment options for extensively resistantGram‐positive cocci
Drug Approved indications
DaptomycinSSTIBacteremia/Endocarditis
TygecyclineSSTIIAICAP (US)
LinezolidSSTICAPHAP
TelavancincSSTI (US)HAP
CeftarolineSSTICAP
cSSSI: studies 300 and 305cSSSI: studies 300 and 305
Ellis-Grosse EJ et al. Clin Infect Dis 2005; 41(suppl 5):S341-S353
21
Grossi - Surgical site infections - ID perspective
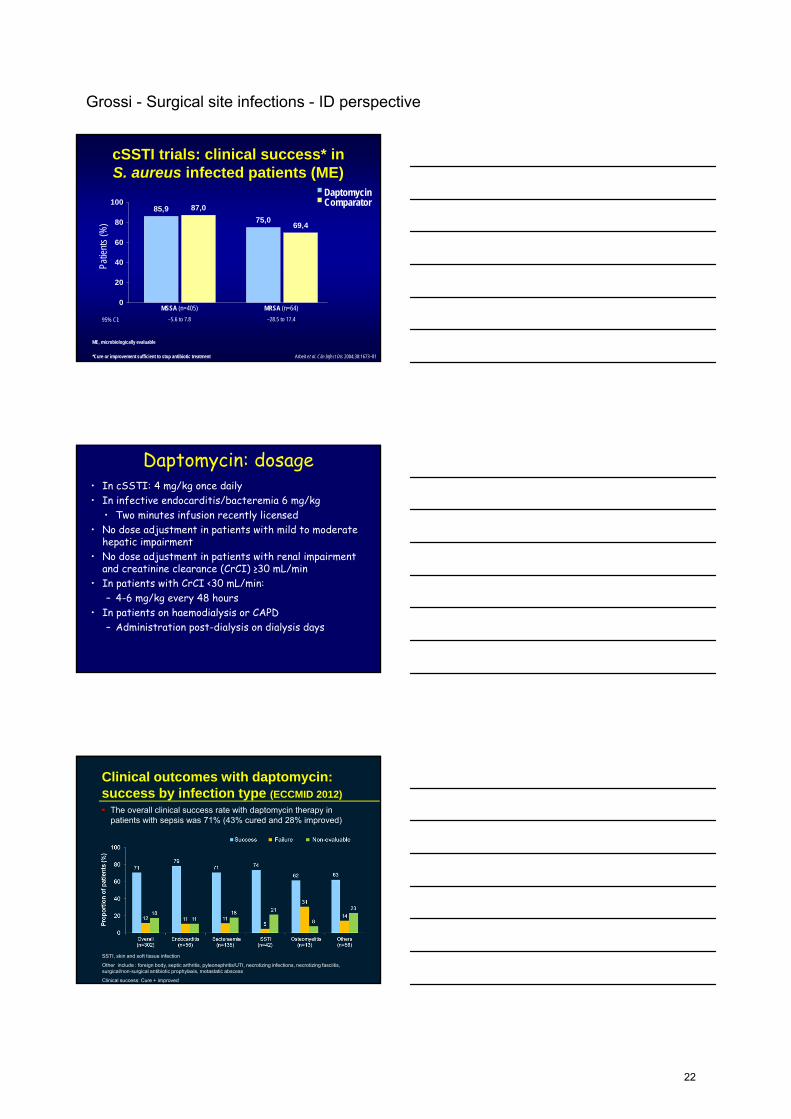
cSSTI trials: clinical success* inS. aureus infected patients (ME)
85,9
75,069,4
87,0
0
20
40
60
80
100
MSSA (n=405)
–5.6 to 7.8
MRSA (n=64)
–28.5 to 17.4
ME, microbiologically evaluable
Arbeit et al. Clin Infect Dis 2004;38:1673–81
95% CI:
Patie
nts
(%)
*Cure or improvement sufficient to stop antibiotic treatment
DaptomycinComparator
Daptomycin: dosage• In cSSTI: 4 mg/kg once daily• In infective endocarditis/bacteremia 6 mg/kg
• Two minutes infusion recently licensed• No dose adjustment in patients with mild to moderate
hepatic impairment• No dose adjustment in patients with renal impairment
and creatinine clearance (CrCI) ≥30 mL/min• In patients with CrCI <30 mL/min:
– 4-6 mg/kg every 48 hours• In patients on haemodialysis or CAPD
– Administration post-dialysis on dialysis days
Clinical outcomes with daptomycin: success by infection type (ECCMID 2012)
The overall clinical success rate with daptomycin therapy in patients with sepsis was 71% (43% cured and 28% improved)
SSTI, skin and soft tissue infection
Other include : foreign body, septic arthritis, pyleonephritis/UTI, necrotizing infections, necrotizing fasciitis, surgical/non-surgical antibiotic prophylaxis, metastatic abscess
Clinical success: Cure + improved
22
Grossi - Surgical site infections - ID perspective
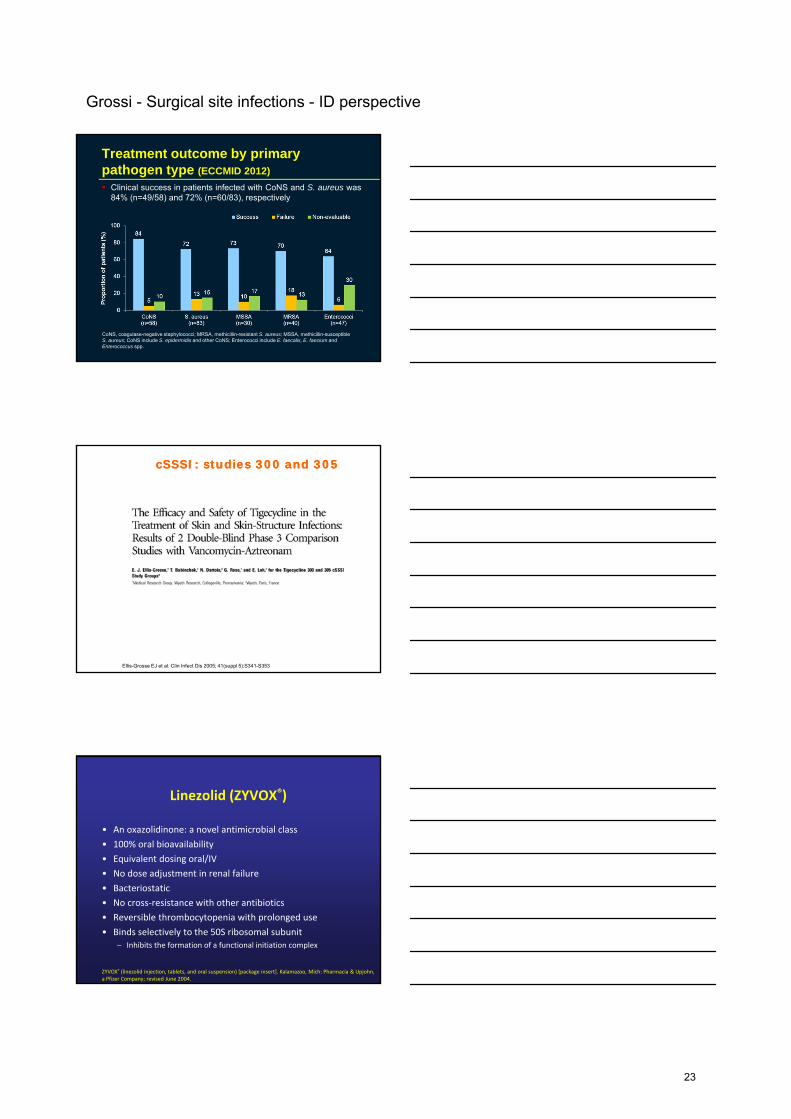
Treatment outcome by primary pathogen type (ECCMID 2012)
CoNS, coagulase-negative staphylococci; MRSA, methicillin-resistant S. aureus; MSSA, methicillin-susceptible S. aureus; CoNS include S. epidermidis and other CoNS; Enterococci include E. faecalis, E. faecium and Enterococcus spp.
Clinical success in patients infected with CoNS and S. aureus was84% (n=49/58) and 72% (n=60/83), respectively
cSSSI: studies 300 and 305cSSSI: studies 300 and 305
Ellis-Grosse EJ et al. Clin Infect Dis 2005; 41(suppl 5):S341-S353
Linezolid (ZYVOX®)
• An oxazolidinone: a novel antimicrobial class
• 100% oral bioavailability
• Equivalent dosing oral/IV
• No dose adjustment in renal failure
• Bacteriostatic
• No cross‐resistance with other antibiotics
• Reversible thrombocytopenia with prolonged use
• Binds selectively to the 50S ribosomal subunit– Inhibits the formation of a functional initiation complex
ZYVOX® (linezolid injection, tablets, and oral suspension) [package insert]. Kalamazoo, Mich: Pharmacia & Upjohn, a Pfizer Company; revised June 2004.
23
Grossi - Surgical site infections - ID perspective
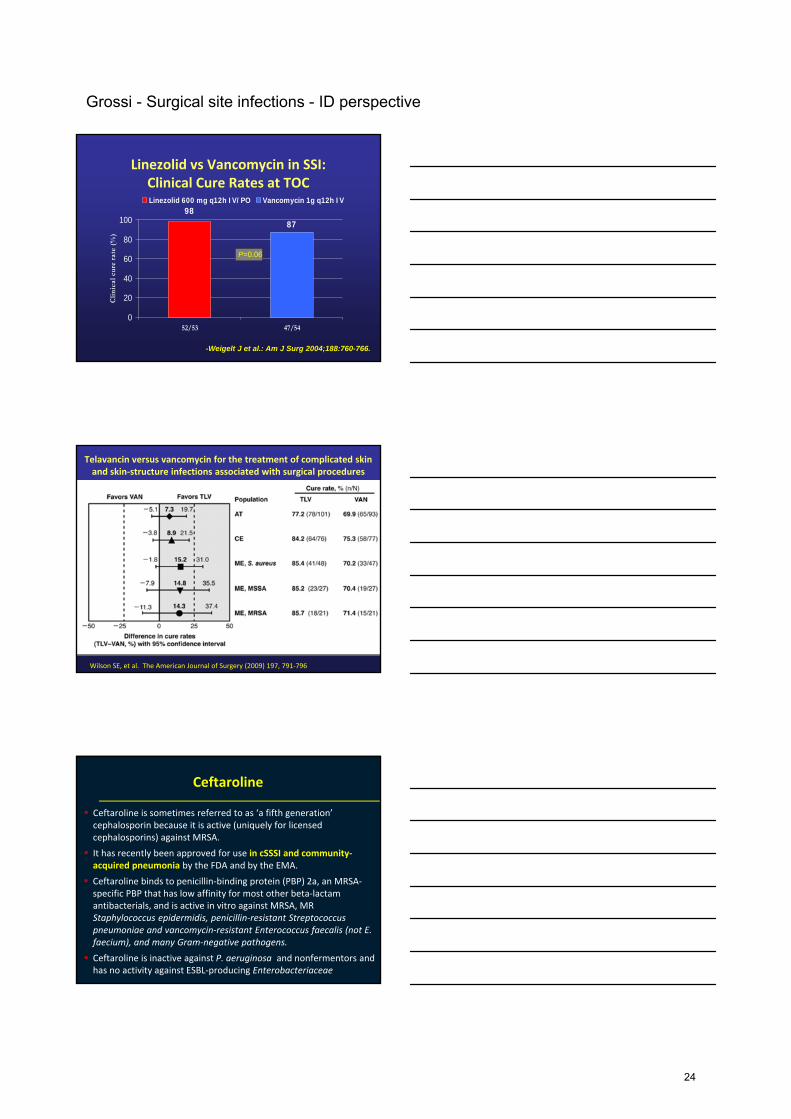
Linezolid vs Vancomycin in SSI:Clinical Cure Rates at TOC
8798
0
20
40
60
80
100
52/53 47/54
Clin
ical
cur
e ra
te (
%)
Linezolid 600 mg q12h IV/PO Vancomycin 1g q12h IV
P=0.06
-Weigelt J et al.: Am J Surg 2004;188:760-766.
Telavancin versus vancomycin for the treatment of complicated skin and skin‐structure infections associated with surgical procedures
Wilson SE, et al. The American Journal of Surgery (2009) 197, 791‐796
Ceftaroline
Ceftaroline is sometimes referred to as ‘a fifth generation’ cephalosporin because it is active (uniquely for licensed cephalosporins) against MRSA.
It has recently been approved for use in cSSSI and community‐acquired pneumonia by the FDA and by the EMA.
Ceftaroline binds to penicillin‐binding protein (PBP) 2a, an MRSA‐specific PBP that has low affinity for most other beta‐lactamantibacterials, and is active in vitro against MRSA, MR Staphylococcus epidermidis, penicillin‐resistant Streptococcuspneumoniae and vancomycin‐resistant Enterococcus faecalis (not E. faecium), and many Gram‐negative pathogens.
Ceftaroline is inactive against P. aeruginosa and nonfermentors and has no activity against ESBL‐producing Enterobacteriaceae
24
Grossi - Surgical site infections - ID perspective
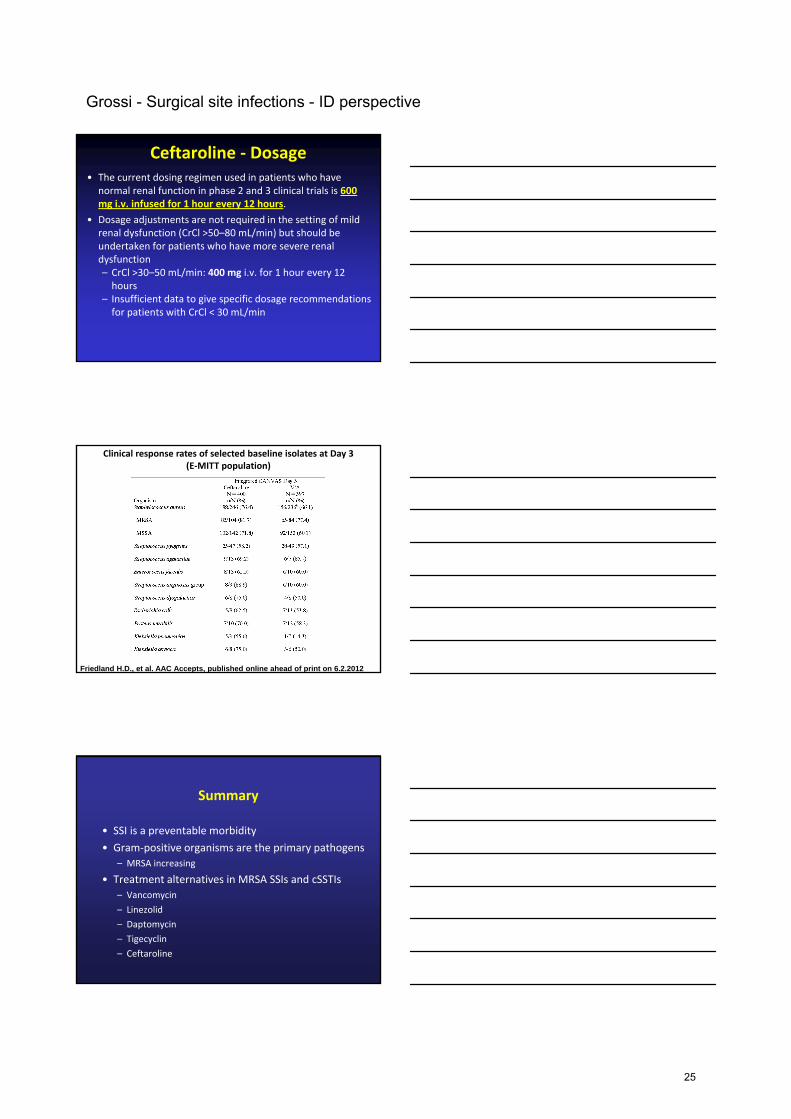
Ceftaroline ‐ Dosage• The current dosing regimen used in patients who have
normal renal function in phase 2 and 3 clinical trials is 600 mg i.v. infused for 1 hour every 12 hours.
• Dosage adjustments are not required in the setting of mild renal dysfunction (CrCl >50–80 mL/min) but should be undertaken for patients who have more severe renal dysfunction – CrCl >30–50 mL/min: 400 mg i.v. for 1 hour every 12 hours
– Insufficient data to give specific dosage recommendations for patients with CrCl < 30 mL/min
Clinical response rates of selected baseline isolates at Day 3 (E‐MITT population)
Friedland H.D., et al. AAC Accepts, published online ahead of print on 6.2.2012
Summary
• SSI is a preventable morbidity
• Gram‐positive organisms are the primary pathogens
– MRSA increasing
• Treatment alternatives in MRSA SSIs and cSSTIs
– Vancomycin
– Linezolid
– Daptomycin
– Tigecyclin
– Ceftaroline
25
Graf - Surgical site infections - CM perspective
26
Graf - Surgical site infections - CM perspective
27
Graf - Surgical site infections - CM perspective
28
Graf - Surgical site infections - CM perspective
29
Graf - Surgical site infections - CM perspective
30
Graf - Surgical site infections - CM perspective
31

Graf - Surgical site infections - CM perspective
32
Graf - Surgical site infections - CM perspective
33
Graf - Surgical site infections - CM perspective
34
Graf - Surgical site infections - CM perspective
35
Graf - Surgical site infections - CM perspective
36
Graf - Surgical site infections - CM perspective
37
Graf - Surgical site infections - CM perspective
38





























