Embed Size (px)
Citation preview


Table of Contents
Original articles
diet, Physical activity, Marital Status and risk of Cancer: a Case Control Study of adults from riyadh, Saudi arabia .......................06Eyad Fawzi AlSaeed and Mutahir A. Tunio
Clinico-hematological Profile of 184 Patients with non-Hodgkin’s lymphoma: an experience from Southern Pakistan ...................11Sadia Sultan, Syed Mohammed Irfan, Anila Rashid, Saira Parveen and Neesha Nawaz
ambiguity of Whole Body PeT CT Scans in diagnosis of Co-existing Tuberculosis and Malignancy: is Histopathological Confirmation Mandatory? .........................................................................................................................................15Prekshi Chaudhary, Sweety Gupta, Nitin Leekha, Ravi S. Rajendra, Shiv S. Mishra, Vandana Arora, Sudarsan De and Sandeep Agarwal
epidemiology and Outcomes with Platinum-Based Chemotherapy in recurrent or Metastatic Carcinoma Cervix in a developing Country: experience from a Tertiary Oncology Centre in Southern india ......................................................................20K.C. Lakshmaiah, Aditi Harsh Thanky, D. Lokanatha, K. Govind Babu, Linu Jacob, Suresh Babu, A.H. Rudresha, K.N. Lokesh, L.K. Rajeev and Aparna Sridharmurthy
disclosure of adverse Cancer news: The Public’s Perspective in a Middle eastern Country .................................................................27Jamal Zekri, Mohamed E. El Sayed and Youssef Nauf
Second Primary Tumors associated with Breast Cancer: Kuwait Cancer Control Center experience ....................................................35Salah Fayaz, Gerges Attia Demian, Heba El-Sayed Eissa and Sadeq Abuzalouf
implications of Observer variation in Gleason Scoring of Prostate Cancer on Clinical Management: a Collaborative audit ...............41A. Harbias, E. Salmo and A. Crump
Squamous Cell Carcinoma of the Buccal Mucosa: a Single institute retrospective analysis of nodal involvement and Survival ...........................................................................................................................................................46Vivek Tiwari and Rakesh Mahawar
Clinical and Pathological Characteristics of Triple Positive Breast Cancer among iraqi Patients ..........................................................51Nada A.S. Alwan, Faisal H. Mualla, Munawar Al Naqash, Saad Kathum, Furat N. Tawfiq and Sana Nadhir
Pre-Treatment nutritional Status and radiotherapy Outcome in Patients with locally advanced Head and neck Cancers ...............61Amit Bahl, Arun Elangovan, Satinder Kaur, Roshan Verma, Arun Singh Oinam,Sushmita Ghoshal, Naresh K Panda
evaluation of BrCa1 large Genomic rearrangements in Group of egyptian female Breast Cancer Patients Using MlPa ...................................................................................................................................................................................64Ola M. Eid, Eman A. El Ghoroury, Maha M. Eid, Rana M. Mahrous, Mohamed I. Abdelhamid, Zahra I. Aboafya, Esmat A. Abdel Ghaffar and Amany H. Abdelrahman
Case reportsBrain Metastasis from Colorectal adenocarcinoma: a Case report ........................................................................................................70Jaroslav Nemec, Abdulsalam Alnajjar, Jasem Albarrak , Shaban A, Mariam Al Otaibi and Asit Mohanty
leiomyosarcoma of Penis: an aggressive and exceptionally rare entity ...............................................................................................73Vinita Trivedi, Muneer A, Rita Rani, Richa Chauhan, Usha Singh and Naveen Kuna
review articlesChemotherapy-induced febrile neutropenia in Solid Tumours ...............................................................................................................77Ayman Rasmy, Mohammed Al Mashiakhi and Amal Ameen
Conference Highlights/Scientific Contributions• NewsNotes ............................................................................................................................................................................................85
• Advertisements .....................................................................................................................................................................................88
• ScientificeventsintheGCCandtheArabWorldfor2017 ..................................................................................................................89
Cancer Aware NationP.O.BOX 26733 Safat 13128 Kuwait
Tel. (+965) 22250226 - Fax:(+965) [email protected]
2225 0226www.cancampaign.com
twitter can_campaign facebook cancampaignkw

6
Corresponding author: Mutahir A. Tunio, MBBS, FCPS (Radiation Oncology), Radiation Oncology,
Comprehensive Cancer Center, King Fahad Medical City, Riyadh-59046, Saudi Arabia. Tel: +96612889999,
Email: [email protected]
introductionModifiable risk factors including poor nutritional
habits, physical inactivity, and smoking are known to be associated with 20% of annual mortality globally.(1) Approximately 50% of all malignancies especially breast, colon, endometrium, stomach, prostate and kidneys are associated with these modifiable risk factors.(2,3) Dietary habits, life style, smoking, drinking coffee and marital status may not only fuel a rise in various cancers, but may also affect the treatment outcomes especially survival.(4,5)
Recent data has shown that lifestyle changes and pharmacologic interventions may reduce the risk of cancer.(6) For example, maintenance of a healthy weight and adhering to fiber rich and low fat diet reduces the risk of breast cancer, (7) and taking aspirin daily reduces the risk of colon cancer.(8) Recently an interesting large prospective study found a small, though not significant
abstract
Objectives: We aimed to compare the dietary habits, engagement in various sports, smoking habits, marital status and other demographic characteristics, between cancer patients and healthy adults (control) at our institute, Riyadh, Saudi Arabia.
Patients and methods: A cross-sectional descriptive study was conducted on 500 participants (237 cancer patients and 263 healthy adults). A well-structured questionnaire was given to these participants regarding the life style, dietary habits, and marital status through interviews.
results: Mean age of whole cohort was 39.3 years (range: 14-85). Among the cancer patients, breast cancer was predominant (45.6%). Compared to controls, higher percentage of married (72.6% vs. 55.5%) and divorced (10.2% vs.4.2%) was noticed in cancer patients (P =
0.002). In cancer patients, majority were unemployed (housewives = 49.3%; retired = 16.0%) as compared to controls (housewives = 14.1%; retired = 2.0%) P = 0.0001. Use of computer laptops/tablets and internet surfing was significantly higher in controls as compared to cancer patients (80.3% vs. 42.2%) P = 0.0001. Similarly, cancer patients started smoking at early age and were relatively heavy smokers with P = 0.03 and P = 0.001 respectively. Cancer patients consumed > 3 cups of coffee/day as compared to control (42.4% vs. 21.5%) P = 0.02. More cancer patients got married at early age between 11-20 years (58.7% vs. 37.7%) P = 0.01.
Conclusion: Unemployment, marital status, lack of nutritional knowledge through internet, heavy smoking, heavy coffee consumption and early age at marriage were associated with the risk of various cancers in both genders.
Keywords: Diet, physical activity, marital status, risk of cancer, case control study
Original Article
diet, Physical activity, Marital Status and risk of Cancer: a Case Control Study of adults from riyadh, Saudi arabia
Eyad Fawzi AlSaeed1,2, Mutahir A. Tunio3
1Faculty of Medicine, King Saud University, 2Consultant Radiation Oncology, King Khalid University Hospital, Riyadh, Saudi Arabia,
3Radiation Oncology, Comprehensive Cancer Center, King Fahad Medical City, Riyadh-59046, Saudi Arabia.
reduction in risk of endometrial cancer with intentional weight loss of at least 20 pounds (relative risk (RR) =0.96; 95% confidence interval (CI) 0.61–1.52.(9) Another prospective trial in ovarian cancer found risk reduction in ovarian cancer with a low-fat diet with a hazard ratio (HR) of 0.60 (95% CI: 0.38–0.96) at 8 years post-intervention.(10) Similarly, in one Japanese trial involving 41,761 adults, green tea consumption was found to be associated with a reduced risk of liver cancer.(11) Coffee is found rich source of various polyphenols containing antioxidant properties which may be beneficial against various malignancies, however results of various studies are controversial.(12)
7
G. J. O. Issue 25, 2017
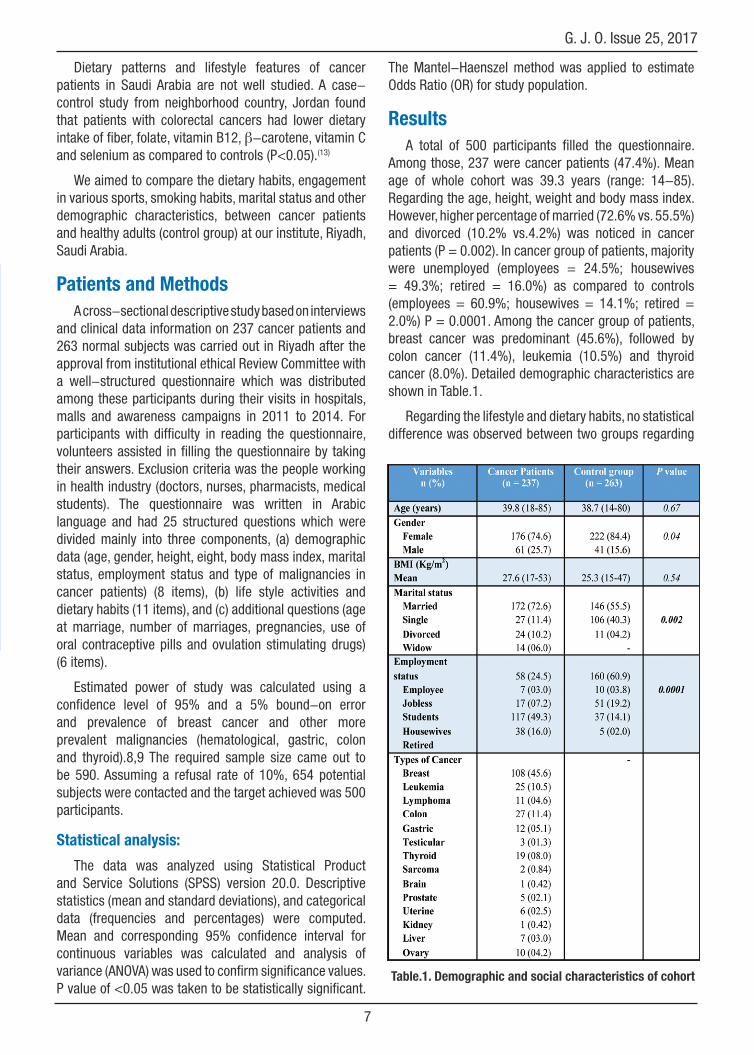
Dietary patterns and lifestyle features of cancer patients in Saudi Arabia are not well studied. A case-control study from neighborhood country, Jordan found that patients with colorectal cancers had lower dietary intake of fiber, folate, vitamin B12, β-carotene, vitamin C and selenium as compared to controls (P<0.05).(13)
We aimed to compare the dietary habits, engagement in various sports, smoking habits, marital status and other demographic characteristics, between cancer patients and healthy adults (control group) at our institute, Riyadh, Saudi Arabia.
Patients and MethodsA cross-sectional descriptive study based on interviews
and clinical data information on 237 cancer patients and 263 normal subjects was carried out in Riyadh after the approval from institutional ethical Review Committee with a well-structured questionnaire which was distributed among these participants during their visits in hospitals, malls and awareness campaigns in 2011 to 2014. For participants with difficulty in reading the questionnaire, volunteers assisted in filling the questionnaire by taking their answers. Exclusion criteria was the people working in health industry (doctors, nurses, pharmacists, medical students). The questionnaire was written in Arabic language and had 25 structured questions which were divided mainly into three components, (a) demographic data (age, gender, height, eight, body mass index, marital status, employment status and type of malignancies in cancer patients) (8 items), (b) life style activities and dietary habits (11 items), and (c) additional questions (age at marriage, number of marriages, pregnancies, use of oral contraceptive pills and ovulation stimulating drugs) (6 items).
Estimated power of study was calculated using a confidence level of 95% and a 5% bound-on error and prevalence of breast cancer and other more prevalent malignancies (hematological, gastric, colon and thyroid).8,9 The required sample size came out to be 590. Assuming a refusal rate of 10%, 654 potential subjects were contacted and the target achieved was 500 participants.
Statistical analysis:
The data was analyzed using Statistical Product and Service Solutions (SPSS) version 20.0. Descriptive statistics (mean and standard deviations), and categorical data (frequencies and percentages) were computed. Mean and corresponding 95% confidence interval for continuous variables was calculated and analysis of variance (ANOVA) was used to confirm significance values. P value of <0.05 was taken to be statistically significant.
Table.1. demographic and social characteristics of cohort
The Mantel-Haenszel method was applied to estimate Odds Ratio (OR) for study population.
resultsA total of 500 participants filled the questionnaire.
Among those, 237 were cancer patients (47.4%). Mean age of whole cohort was 39.3 years (range: 14-85). Regarding the age, height, weight and body mass index. However, higher percentage of married (72.6% vs. 55.5%) and divorced (10.2% vs.4.2%) was noticed in cancer patients (P = 0.002). In cancer group of patients, majority were unemployed (employees = 24.5%; housewives = 49.3%; retired = 16.0%) as compared to controls (employees = 60.9%; housewives = 14.1%; retired = 2.0%) P = 0.0001. Among the cancer group of patients, breast cancer was predominant (45.6%), followed by colon cancer (11.4%), leukemia (10.5%) and thyroid cancer (8.0%). Detailed demographic characteristics are shown in Table.1.
Regarding the lifestyle and dietary habits, no statistical difference was observed between two groups regarding

8
Diet, Physical Activity, Marital Status and Risk of Cancer, Eyad Fawzi AlSaeed, et. al.
Table 2. life style activities and dietary habits of cohort
Table 3. Marital characteristics of cohort
the playing sports, types of sports and sports hours (P = 0.16; P = 0.96; and P = 0.21 respectively). Similarly, no significant difference was noticed between two groups in terms of watching television and hours spent in front of television (P = 0.95). However, use of laptops, tablets and internet surfing was significantly higher in controls as compared to cancer patients (80.3% vs. 42.2%) P = 0.0001. Regarding smoking, no statistical difference was observed between two groups (P = 0.60); however, cancer patients started smoking at early age and were relatively heavy smokers with P = 0.03 and P = 0.001 respectively. Regarding the use of hot beverages especially coffee, cancer patients consumed > 3 cups per 24 hours as compared to control (42.4% vs. 21.5%) P = 0.02. Details are shown in Table.2.
More cancer patients got married at early age between 11-20 years (58.7% vs. 37.7%) P = 0.01.
However, no significant difference was seen between two groups regarding the number of marriages, number of pregnancies and age at first pregnancy (P = 0.47; P = 0.51 and P = 0.90 respectively). Cancer patients reported more use of oral contractive pills (OCP) as compared to controls (90.6% vs. 66.4%) P = 0.0001, while in contrast, healthy control reported more use of ovulation stimulating drugs (20.6% vs. 11.2%) P = 0.01. The details are shown in Table 3. OR for various risk factors are mentioned in Fig.1.
discussionOur study showed some interesting findings. Firstly,
majority of cancer patients were found to have low socio-economic status (unemployed and retired), which is consistent with findings of other epidemiological studies.(14) However, in contrast to other studies, protective effect of marriage against cancer risk which is likely related to spousal support was not observed in our study.(15,16)
Exact explanation could not be explained, but it is likely associated with low socio-economic status and selection bias as majority of cancer cohort was with breast cancer.
Secondly, non-significant difference was observed between cancer patients and controls regarding the playing sports, types of sports and sports hours, which can be explained by heterogeneity of our cohort. Current evidence of lack of physical activity in malignancies especially breast cancer is controversial, though physical activity appear promising, but further studies are warranted to establish their efficacy.(17)

9
G. J. O. Issue 25, 2017
Thirdly, use of laptops, tablets and internet surfing were found significantly less in cancer patients, which reflected the educational background of cancer patients and lack of nutritional and life style knowledge. Various studies have shown that internet access and availability of online information is associated with dietary and life style changes, thus cancer prevention.(18)
Fourthly, related to smoking, although non-significant difference was observed between cancer patients and controls, cancer patients started smoking at very young and were relatively heavy smokers, which is in agreement with reported data.(19) Similarly, consumption of coffee > 3 cups per day was significantly higher in cancer patients as compared to controls. This could be due to our heterogeneous population, but evidence is controversial, as many of studies have found a protective effect of high coffee consumption with respect to malignancies especially colon cancer, others have found either no effect or a rise in risk of cancer. (20, 21)
Fifthly, it was seen that majority of cancer patients got married at early age between 11-20 years as compared to their counterpart, which can be explained by the religious and cultural traditions in country.(22)
Sixthly, regarding the use of OCP, cancer patients reported more use these pills as compared to controls, which is also in agreement with other studies. (23) Possible explanation could be our breast cancer predominant cohort. Lastly, no strong correlation between the use of ovarian stimulating drugs and cancer risk was seen,
which was also in agreement with reported data; (24) however, this needs further investigation.
Strengths of present study were (a) large sample size, (b) case-control study, (c) a well-structured questionnaire in Arabic version and limitations of study were (a) heterogeneous cancer patients and (b) lack of analysis regarding impact of these modifiable risk factors on treatment outcomes.
In conclusion, there is very scanty data regarding the impact of dietary habits, life style, marital status and risk of cancer in Saudi Arabia. Results of present study showed that unemployment, low socioeconomic status, marital status (married, divorced and young age at marriage), lack of nutritional knowledge through internet, heavy smoking, and heavy coffee consumption were associated with the risk of various cancers in our population. However, further similar studies are warranted.
references1. Beavis AL, Smith AJ, Fader AN. Lifestyle changes and
the risk of developing endometrial and ovarian cancers: opportunities for prevention and management. Int J Womens Health 2016; 8:151-67. doi: 10.2147/IJWH.S88367.
2. Colditz GA, Atwood KA, Emmons K, Monson RR, Willett WC, Trichopoulos D, Hunter DJ. Harvard report on cancer prevention volume 4: Harvard Cancer Risk Index. Risk Index Working Group, Harvard Center for Cancer Prevention. Cancer Causes Control 2000; 11:477-88
fig.1. forest plot showing odds ratio for various risk factors
LCL = lower confidence limit, UCL = upper confidence limit, OCP = oral contraceptive pills

10
Diet, Physical Activity, Marital Status and Risk of Cancer, Eyad Fawzi AlSaeed, et. al.
3. Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med 2003; 348:1625-38
4. Reeves GK, Pirie K, Beral V, Green J, Spencer E, Bull D; Million Women Study Collaboration. Cancer incidence and mortality in relation to body mass index in the Million Women Study: cohort study. BMJ 2007; 335:1134
5. Hendifar A, Osipov A, Khanuja J, Nissen N, Naziri J, Yang W, Li Q, Tuli R. Influence of Body Mass Index and Albumin on Perioperative Morbidity and Clinical Outcomes in Resected Pancreatic Adenocarcinoma. PLoS One 2016; 11:e0152172. doi: 10.1371/journal.pone.0152172
6. Schmandt RE, Iglesias DA, Co NN, Lu KH. Understanding obesity and endometrial cancer risk: opportunities for prevention. Am J Obstet Gynecol 2011; 205:518-25. doi: 10.1016/j.ajog.2011.05.042
7. Kotepui M. Diet and risk of breast cancer. Contemp Oncol (Pozn) 2016; 20:13-9. doi: 10.5114/wo.2014.40560
8. Parker ED, Folsom AR. Intentional weight loss and incidence of obesity-related cancers: the Iowa Women’s Health Study. Int J Obes Relat Metab Disord 2003; 27:1447-52
9. Li H, Zhu F, Boardman LA, Wang L, Oi N, Liu K, Li X, Fu Y, Limburg PJ, Bode AM, Dong Z. Aspirin Prevents Colorectal Cancer by Normalizing EGFR Expression. EBioMedicine 2015; 2:447-455
10. Prentice RL, Thomson CA, Caan B, Hubbell FA, Anderson GL, Beresford SA, Pettinger M, Lane DS, Lessin L, Yasmeen S, Singh B, Khandekar J, Shikany JM, Satterfield S, Chlebowski RT. Low-fat dietary pattern and cancer incidence in the Women’s Health Initiative Dietary Modification Randomized Controlled Trial. J Natl Cancer Inst 2007; 99:1534-43
11. Ui A, Kuriyama S, Kakizaki M, Sone T, Nakaya N, Ohmori-Matsuda K, Hozawa A, Nishino Y, Tsuji I. Green tea consumption and the risk of liver cancer in Japan: the Ohsaki Cohort study. Cancer Causes Control 2009; 20:1939-45. doi: 10.1007/s10552-009-9388-x.
12. Ren JS, Freedman ND, Kamangar F, Dawsey SM, Hollenbeck AR, Schatzkin A, Abnet CC. Tea, coffee, carbonated soft drinks and upper gastrointestinal tract cancer risk in a large United States prospective cohort study. Eur J Cancer 2010;46:1873-81
13. Arafa MA, Waly MI, Jriesat S, Al Khafajei A, Sallam S. Dietary and lifestyle characteristics of colorectal cancer in Jordan: a case-control study. Asian Pac J Cancer Prev 2011; 12:1931-6
14. Vanthomme K, Vandenheede H, Hagedoorn P, Gadeyne S. Socioeconomic disparities in lung cancer mortality in Belgian men and women (2001-2011): does it matter who you live with? BMC Public Health 2016; 16:493. doi: 10.1186/s12889-016-3139-1.
15. Jin JJ, Wang W, Dai FX, Long ZW, Cai H, Liu XW, Zhou Y, Huang H, Wang YN. Marital status and survival in patients with gastric cancer. Cancer Med 2016 Jun 5. doi: 10.1002/cam4.758
16. Shi RL, Qu N, Lu ZW, Liao T, Gao Y, Ji QH. The impact of marital status at diagnosis on cancer survival in patients with differentiated thyroid cancer. Cancer Med 2016 Jun 5. doi: 10.1002/cam4.778
17. Chan RJ, McCarthy AL, Devenish J, Sullivan KA, Chan A. Systematic review of pharmacologic and non-pharmacologic interventions to manage cognitive alterations after chemotherapy for breast cancer. Eur J Cancer 2015; 51:437-50. doi: 10.1016/j.ejca.2014.12.017
18. Silva PR, Castiel LD, Ferreira FR. Patterns of cancer-related internet searches: reactiveness; risks; the role of affect. Cien Saude Colet 2016; 21:861-870
19. Taghizadeh N, Vonk JM, Boezen HM. Lifetime Smoking History and Cause-Specific Mortality in a Cohort Study with 43 Years of Follow-Up. PLoS One 2016; 11:e0153310. doi: 0.1371/journal.pone.0153310
20. Zhang X1, Albanes D, Beeson WL, van den Brandt PA, Buring JE, Flood A, et al. Risk of colon cancer and coffee, tea, and sugar-sweetened soft drink intake: pooled analysis of prospective cohort studies. J Natl Cancer Inst 2010; 102:771-83. doi: 10.1093/jnci/djq107
21. Yamada H, Kawado M, Aoyama N, Hashimoto S, Suzuki K, Wakai K, Suzuki S, Watanabe Y, Tamakoshi A; JACC Study Group. Coffee consumption and risk of colorectal cancer: the Japan Collaborative Cohort Study. J Epidemiol 2014; 24:370-8
22. Al-Zaben FN, Sehlo MG, Koenig HG. A cross-sectional study of anxiety and marital quality among women with breast cancer at a university clinic in western Saudi Arabia. Saudi Med J 2015; 36:1168-75. doi: 10.15537/smj.2015.10.12254
23. Al-Amri FA, Saeedi MY, Al-Tahan FM, Ali AM, Alomary SA, Arafa M, Ibrahim AK, Kassim KA. Breast cancer correlates in a cohort of breast screening program participants in Riyadh, KSA. J Egypt Natl Canc Inst 2015; 27:77-82. doi: 10.1016/j.jnci.2015.04.002
24. Bjornholt SM, Kjaer SK, Nielsen TS, Jensen A. Risk for borderline ovarian tumours after exposure to fertility drugs: results of a population-based cohort study. Hum Reprod 2015; 30:222-31. doi: 10.1093/humrep/deu297