Embed Size (px)
Citation preview

Systolic Hypertension in Hemodialysis Patients
Rajiv AgarwalDivision of Nephrology, Department of Medicine, Indiana University School of Medicine, Indianapolis, Indiana
ABSTRACT
Systolic hypertension with or without diastolic hypertension isa major problem in hemodialysis (HD) patients; isolateddiastolic hypertension is uncommon. Accelerated age-relatedchanges in vascular stiffness, together with factors peculiar touremia, lead to loss of large and small vessel distensibility andprofound changes in circulatory function that includes anincrease in systolic pressure and widening of the pulse pressure.Epidemiologic studies show a direct relationship of mortalitywith systolic blood pressure (BP) and an inverse relationshipwith diastolic BP. Thus systolic BP should be the focus oftreatment. In HD patients with systolic hypertension, diastolicBP is inversely related to cardiovascular risk. An accuratediagnosis of hypertension followed by nonpharmacologicmeasures (sodium restriction, exercise, dry weight) should be
the initial steps in BP reduction. The second step should be theuse of antihypertensive agents, particularly the use of angio-tensin converting enzyme (ACE) inhibitors and/or b-blockers.The use of these agents has been associated with betteroutcomes in observational studies in HD patients. Further-more, the administration of atenolol and lisinopril can besupervised three times a week to achieve improved BP control.Daily dialysis may improve BP and cardiovascular risk factors.Although more difficult to implement, it may emerge as afeasible alternative to conventional dialysis. Adequate systolicBP control with these available and emerging techniques shouldhelp stem the tide of cardiovascular mortality and mortality inHD patients.
The Joint National Committee on the Prevention,Detection, Evaluation, and Treatment of High BloodPressure (JNC VI 1997) stated in a clinical advisory, ‘‘thecommittee now recommends a major paradigm shift inurging that systolic BP become the major criterion for thediagnosis, staging, and therapeutic management ofhypertension, particularly in middle-aged and olderAmericans’’ (1). Based on our knowledge of hyperten-sion in patients with chronic kidney disease (CKD), therecommendations of JNC VI should be extrapolated toadult patients with end-stage renal disease (ESRD), alsoa major paradigm shift.
Pathophysiologically, CKD is a state of acceleratedvascular aging that leads to reduced capacitative com-pliance and increased systolic BP. Epidemiologically,systolic hypertension is more common in CKD and whenCKD progresses to end-stage renal disease (ESRD);systolic hypertension is nearly universal in these patientsirrespective of antihypertensive drug use. Cardiovascularoutcomes that are, in part, attributable to hypertensionin CKD or hemodialysis (HD) patients are many timeshigher compared to the general population (2). Increasedaortic stiffness, which is associated with systolic hyper-tension, is a strong independent predictor of all-cause(mainly cardiovascular) mortality in patients on chronic
HD (3). Thus an HD patient in the third or fourth decadeof life has a survival similar to a healthy person in theseventh or eighth decade of life. For the above reasons, aparadigm shift is needed in CKD where systolic, notdiastolic, hypertension becomes central to the manage-ment of the hypertensive patient.
Pathophysiology of Systolic Hypertension
General Population
In industrialized societies, systolic BP increases stead-ily with age, whereas diastolic BP increases till about 55years of age and then declines. Pulse pressure thereforewidens with age. Structural and functional changes inarterial circulation occur with aging, are accelerated withhypertension, and lead to a high prevalence of systolichypertension in the older population (4). Although theconcept of atherosclerosis and endothelial dysfunction iswell recognized, the concept of arteriosclerosis andresultant ‘‘adventitial dysfunction’’ has not received asmuch attention.
Arteriosclerosis is an age-related diffuse processcharacterized by replacement of elastin with collagen inthe walls of large arteries (5). Fibrosis and hypertrophy ofsmooth muscle of the arterial wall results in dilatationand lengthening of the aorta (6). The elastic properties ofthe blood vessels hydraulically filter the discontinuouspulsations of the heart to a steady stream in theperipheral vessels. The modified Windkessel modelconceives two compliances (7): the first is proximal,representing the storage capacity of the larger conduitarteries; the second is distal, representing the elasticity of
Address correspondence to: Rajiv Agarwal, MD, Division ofNephrology, Department of Medicine, Indiana Universityand RLR VA Medical Centre, 1481 West 10th St., 111N,Indianapolis, IN 46202, or e-mail: [email protected].
Seminars in Dialysis—Vol 16, No 3 (May–June) 2003pp. 208–213
208

smaller arteries and branch points involved in reflectionsand oscillations in the system. As arteries become lessdistensible, there is a quicker return of the backwardpressure wave from the reflection sites toward the heart,boosting pressure during late systole (rather thandiastole) by as much as 40–50 mmHg in central arteries(5). The second systolic peak becomes more prominent asarteries stiffen. The lack of aortic distensibility fails tomaintain steady flow in diastole and therefore attenuatesdiastolic pressure. Accordingly, widened pulse pressure isthe most robust clinical indicator of arteriosclerosis andcardiovascular risk. Nevertheless, systolic BP, ratherthan pulse pressure, is considerably simpler to useclinically in the management of hypertensive patientsand is the basis of the JNC VI clinical advisory (1).
HD Patients
Hypertension in HD patients, as in patients withessential hypertension, is associated with a number ofcardiac adaptations and maladaptations (8). Cardiacchanges, such as left ventricular hypertrophy (LVH) anddiastolic dysfunction, go hand-in-hand with vascularchanges such as increased pulse wave velocity, increasedcarotid intima media thickness, and widened pulsepressure (9).
Bothvolumeand pressureoverloadare seen inpatientswith ESRD. The causes of chronic flow overload are wellrecognized and include the presence of arteriovenous(AV) shunts, salt and water overload, and anemia.Pressure overload can occur from hypertension as well asloss of compliance of large arteries and increasedreflection from smaller arteries and branch points.
Factors peculiar to uremia that contribute to acceler-ated vascular stiffening include hyperparathyroidism,increased calcium · phosphorus product, increased cir-culating endothelin concentration (10), sympatheticactivation (11), and vascular inflammation; increases inintravascular volume and inappropriately high angio-tensin II further augment vascular stiffness (12). The lossof vessel compliance causes increased left ventricularafterload and impaired coronary perfusion and furthercompromise cardiac function. These pathologic changescause an impairment of circulatory function that isassociated with increased cardiovascular morbidity andmortality.
Epidemiology and Consequences of SystolicHypertension
General Population
Lloyd-Jones et al. (13) evaluated the differential effectof systolic and diastolic BP on JNC VI staging in ahypertensive population with a mean age 58 years. Whilethere was a 65% concordance for staging betweensystolic and diastolic BP, 32% were upstaged on the basisof systolic BP and only 4% were upstaged on the basis ofdiastolic BP. Overall systolic BP alone classified 99% ofall subjects, and 95% of those £60 years of age.
In the general population older than 60 years, it issystolic hypertension, not diastolic hypertension that is
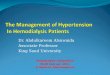
a major public health problem (14). In this population,high systolic BP and low diastolic BP are betterpredictors of cardiovascular outcomes (15). In fact,pulse pressure derived from ambulatory BP monitor-ing is the single best predictor of outcomes in elderlyhypertensive patients (16). Similarly pulse pressure wasfound to be the best predictor of outcomes in trialsassessing outcomes of therapy with calcium channelblockers (17) (Fig. 1). Mean arterial pressure whenadjusted for pulse pressure was a poor predictor.These data imply that treating systolic hypertension iscausally linked to improved outcomes in essentialhypertension.
CKD Population not on Dialysis
In patients with CKD, control of hypertension is ofparamount importance in preventing the progression ofrenal disease. Nonetheless, only 11% of people with renalfailure reach the JNC VI recommended goal of less than130/85 mmHg and only 27% achieve the less than 140/90mmHg goal (18), even though a higher proportion ofpeople with renal failure (75% compared to 49% withoutrenal failure) are treated with antihypertensive medica-tions. Thus only 14% of the treated people with CKDreach the JNC VI recommended goal.
Data from three large randomized controlled hyper-tension trials in patients with CKD are shown in Table 1(19–21). Judging from the reported mean values, poorlycontrolled systolic hypertension was highly prevalent inall the studies. In the RENAAL trial, 560 of 751 patients(75%) treated with placebo had a systolic BP ‡ 140mmHg. In the AASK trial only 36% of the visits in theusual BP group (<140/90 mmHg) achieved the statedgoal.
Fig. 1. Mortality and cardiovascular morbidity in trials of
isolated systolic hypertension treated with dihydropyridine calcium
channel blockers (in Syst-Eur and Syst-China trial) or diuretics (in
European Working Party on High Blood Pressure in the Elderly
Trial). Data are adjusted for sex, age, previous cardiovascular
complications, smoking, and active treatment. Pulse pressure
analyzes are adjusted for mean arterial pressure and mean arterial
pressure analyzes are adjusted for pulse pressure, Data demonstrate
the predictive value of pulse pressure, but not mean arterial pressure,
in predicting cardiovascular endpoints in elderly patients. (Data
adapted from Blacher J, et al. Arch InternMed 160:1085–1089, 2000.)
SYSTOLIC HYPERTENSION IN HEMODIALYSIS 209

HD Population
Hypertension in HD is mainly systolic in nature,reflecting the loss of aortic distensibility and acceleratedvascular aging (22). At any mean arterial pressure, HDpatients have a higher systolic BP and lower diastolic BPcompared to control subjects with normal renal function,matched for age, gender, diabetes mellitus, and bodymass index (23). When assessed using interdialyticambulatory BP monitoring, systolic hypertension ispresent with or without diastolic hypertension in themajority of the patients; only 3% of the patients haveisolated diastolic hypertension (24) (Fig. 2).
There are no outcome trials with hard cardiovascularendpoints in patients with hypertension in HD. The bestdata come from Japanese studies of patients who are newto dialysis (25). Although patient numbers were small,the duration of follow-up was more than a decade.Overall these studies show poorer outcomes in hyper-tensive patients, with the notable finding that initiallyhypertensive patients who became normotensive withtreatment had outcomes that were similar to normoten-sive controls.
The association of increased systolic BP and pulsepressure in HD patients with poor cardiovascularoutcomes is now emerging. Pulse pressure was found tobe the single best predictor of total mortality at 1 year in alarge U.S. HD cohort (26). Longer-term observationalstudies in the United States over 6 years also show that a
high systolic BP and low diastolic BP are associated withincreased total mortality (27). Thus a patient with a BP of170/70 mmHg has a poorer cardiovascular outcome thana patient with a BP of 170/100 mmHg. Nevertheless,most of the association of mortality and BP wasaccounted for in the concomitant comorbid factors suchas age, smoking, diabetes, and vascular disease. Japanesestudies, having the longest follow-up, show similarresults (28) (Fig. 3). Thus the epidemiology of hyperten-sion and outcomes are similar to that seen in the olderparticipants of the Framingham study, where a highsystolic but a low diastolic BP predicted cardiovascularoutcomes (15).
Treatment of Systolic Hypertension
General Population
In the late 1980s Cruickshank (29) pointed out that inlong-term studies of patients with hypertension, inclu-ding patients with severe hypertension and overt ische-mia, a J-shaped relationship existed between diastolic BPduring treatment and myocardial infarction; the lowestpoint (the J-point) was at a diastolic BP between 85 and90 mmHg. He speculated that subjects who have severecoronary artery stenosis have a poor coronary flowreserve, which makes the myocardium vulnerable toreductions in coronary perfusion pressure. He advised
-20
-10
0
10
20
30
Pulse Pressure
Mean Pressure
Adj
uste
d re
lativ
e %
incr
ease
(95
% C
I) in
haza
rd r
ate
asso
ciat
ed w
ith 1
0 m
m H
gin
crea
se in
Pul
se P
ress
ure
or M
ean
Art
eria
lPr
essu
re
TotalMortality
CardiovascularMortality
CardiovascularEnd Points
Stroke Coronary EndPoints
Fig. 2. Distribution of ambulatory systolic and diastolic hyper-
tension in chronic HD patients. Only 3% of the patients had isolated
diastolic hypertension. The major burden of hypertension in HD
patients is systolic. (Agarwal R, Lewis RR. Kidney Int 60:1982–1989,
2001.)
Fig. 3. Relationship of systolic and diastolic BP and34 cardiovas-
cular morbidity and total mortality in HD patients. High systolic BP
predicts increased events, but a low, not high diastolic BP predicts
increased total mortality, stroke, and acute myocardial infarctions.
(Adapted from Tozawa M, et al. Kidney Int 61:717–726, 2002.)
TABLE 1. Comparison of achieved systolic and diastolic BP control in randomized controlled trials in CKD
IDNT RENAAL AASK
Placebo Irbesartan Amiodipine Losartan PlaceboLower BP
(<125/75 mmHg)Usual BP
(<140/90 mmHg)
Number of participants 569 579 567 751 762 540 554Age (years) 58 59 59 60 60 55 55Whites (%) 73 76 69 48 50 0 0Serum creatinine 1.7 1.7 1.7 1.9 1.9 2.2 2.2Baseline BP (mmHg) 158/87 161/87 159/87 152/82 153/82 152/96 149/95Final BP (mmHg) 145/79 142/77 142/76 140/75 142/75 128/78a 141/85a
aAverage BP after the first 3 months.IDNT, Irbesartan Diabetic Neprhopathy Trial. RENAAL, Reduction in End-Points with Angiotensin II Antagonist Losartan; Aask,
African American Study of Kidney Disease.
Agarwal210

caution when treating very old patients (‡84 years old)and patients 60–79 years old who have isolated systolichypertension.
However, in a trial of 18,790 patients with essentialhypertension but minimal vascular disease at baseline,randomized to three different diastolic BP goals of 80, 85,and 90 mmHg diastolic BP, no increase in cardiovascularevents or cardiovascular mortality was seen in those withthe lowest achieved diastolic BPs (30), even among thosewith renal disease (31). In fact, in the 8% of thepopulation that was diabetic, a significant reduction inmyocardial infarctions and cardiovascular mortality wasseen in those randomized to the lowest diastolic BPgroups. These data demonstrate the safety and efficacy ofBP reduction and the lack of the J-curve in randomizedtrials in non-ESRD populations.
Several trials have shown the benefits of treating olderpatients with isolated systolic hypertension. In patientswithout renal disease, the benefits of pharmacologictherapy (chlorthalidone with or without atenolol orreserpine) was first established by the Systolic Hyperten-sion in the Elderly Program (32). Trials using newerdrugs like dihydropyridine calcium channel blocker inSyst-Eur (33) or an angiotensin II receptor blocker inLIFE (34) have also demonstrated the safety and efficacyof treating systolic hypertension in the elderly.
HD Patients
The absence of randomized controlled trials, butcompelling observational data to demonstrate the dele-terious effect of systolic hypertension in HD patients,makes the recommendations a matter of opinion. Thefirst step is to make an accurate diagnosis (as discussed inan earlier issue of this journal (35)), followed byinstitution of nonpharmacologic measures to control BP.
Sodium restriction clearly lowers BP in patientswithout renal failure (36). Its value in dialysis patientswas demonstrated 30 years ago (37). Other benefits ofsodium restriction may also occur. Sprague-Dawley ratsplaced on a high sodium diet have structural anddistensibility alterations of large arteries even in theabsence of BP changes (38). Limiting sodium intake inHD patients will reduce interdialytic weight gain andmake it easier to achieve dry weight. Observational datafrom the U.S. Renal Data System (USRDS) DialysisMorbidity and Mortality Study Waves 3 and 4 show thatpatients had an average interdialytic weight gain of 3.6%and that those gaining 4.8% or more had a 12% highermortality than those gaining less than 2.3% (27).Predominantly systolic hypertension was present in thispopulation, with an average predialysis BP of 152/80mmHg.
Exercise can improve systolic BP control in HDpatients (39). In a controlled trial, 40 HD patientsperformed stationary bicycle exercise during dialysis and35 nonexercising patients served as controls. BP averagedabout 160/80 mmHg. After 6 months, 54% of thepatients continuing to exercise had a decrease inantihypertensive medications, whereas only four patientsin the control group had their BP medications reduced(p < 0.001).
Assessment and adjustment of ‘‘dry weight’’ should bean ongoing process in HD patients (40). Poorly con-trolled hypertension is often attributable to chronicvolume overload (41); gentle reduction in postdialysisweight over a few weeks, along with salt restriction(41,42), longer dialysis (43), or extra dialysis sessions mayyield a significant benefit. Volume control with dialysismay not only improve BP control but also the autonomiccontrol of BP, thus limiting the systolic increases anddecreases in BP (44).
While antihypertensive agents should be used as a lastresort, they clearly have an important place in controllingsystolic hypertension. In a cohort study with a 3-yearfollow-up, we observed a BP reduction of 9.4/6.7 mmHgin association with an increase in the mean number ofantihypertensive medications from 0.91 to 1.41 (45).Overall BP medications in this population produced agreater reduction in systolic rather than diastolic pres-sure. In a double-blind study, London et al. (46) studied24 ESRD patients with LVH who were randomized toreceive 1 year of either the ACE inhibitor perindopril orthe calcium channel blocker nitrendipine. Both agentsinduced significant and similar decreases in BP, as well asimproving large-artery compliance and arterial wavereflections (augmentation index). ACE inhibition de-creased LVH independently of its antihypertensive effector its associated alterations in arterial hemodynamics.
Withholding antihypertensive therapy on days ofdialysis and use of submaximal antihypertensive therapyare significant barriers in BP control (47). Use ofantihypertensives is independently associated with abetter survival (48,49). Recent data show that b-blockershave the best outcomes (27), perhaps due to a greaterlowering of systolic compared to diastolic BP. Supervisedadministration of low-dose atenolol given three times aweek lowers interdialytic BP by 17 mmHg systolic and 11mmHg diastolic, thereby improving pulse pressure by 6mmHg (50). Furthermore, smooth interdialytic BPreduction is achieved with this regimen.
ACE inhibitors can be similarly used and result in a 22mmHg reduction in systolic pressure and an 11 mmHgreduction in diastolic pressure (51). The resultant 11mmHg lowering of pulse pressure may account forreports of better outcomes in users of ACE inhibitorsamong dialysis patients (52). Even low doses of ACEinhibitors, especially when accompanied by improvedintravascular volume, can improve vascular compliance(12).
On the basis of these limited data in HD patients,together with the extensive data in hypertensive anddiabetic individuals, ACE inhibitors and b-blockersshould be used in preference to calcium channel blockers;the latter are the most widely prescribed antihypertensiveclass in HD patients (22,53). Although dihydropyridinecalcium channel blockers may improve aortic stiffness(54,55), left ventricular dilatation is improved with long-term ACE inhibitors but not with dihydropyridinecalcium channel blockers (46).
Another strategy that is emerging as promising andrevolutionary is short daily or prolonged daily HD.Centers in which prolonged HD is performed reportexcellent control of BP without medications and a very
SYSTOLIC HYPERTENSION IN HEMODIALYSIS 211

low mortality rate (56,57). Hypertension control may bedue to the removal of sodium and water (58), but mayalso be due to removal of pressor substances such asasymmetric dimethylarginine (59) and mitigation ofautonomic activation. Furthermore, the cardiovascularrisk profile may be improved by a reduction in homo-cysteine levels (60). Nocturnal HD performed 8–10 hoursduring sleep at home, 6–7 days/week, allows BP controlwith fewer medications (61) as well as fewer episodes ofsleep apnea (62). Despite a reduction in BP to normo-tensive levels and improvements in LVH (58), the normalnocturnal dipping of BP is not restored (58,63). Non-dipping is associated with LVH (64), which, in essentialhypertension, is a strong risk factor for future cardio-vascular events. Thus the circadian rhythm of BP maynot be restored despite daily dialysis. However, thesedata provide hope that long-duration dialysis mayreduce cardiovascular risk factors and therefore cardio-vascular events in HD patients.
In conclusion, systolic hypertension is the majorproblem in HD patients should be the focus of treatment.An accurate diagnosis of hypertension followed bynonpharmacologic measures (sodium restriction, exer-cise, dry weight) should be the essential first step in BPreduction. The second step should be the use ofantihypertensive agents, particularly the use of ACEinhibitors and b-blockers in a supervised fashion threetimes a week to achieve improved BP control. Prolongeddialysis that may improve BP and cardiovascular riskfactors is more difficult to implement but will likelyemerge as a feasible alternative to conventional dialysis.Adequate systolic BP control should translate intoimproved cardiovascular morbidity and mortality inpatients on HD.
Acknowledgment
Supported by grant no. 1 RO1 DK062030-01A1 from National
Institute of Diabetes, Digestive and Kidney Disease.
References
1. Izzo JL Jr, Levy D, Black HR: Clinical advisory statement. Importance ofsystolic blood pressure in older Americans. Hypertension 35:1021–1024, 2000
2. Foley RN, Parfrey PS, Sarnak MJ: Clinical epidemiology of cardiovasculardisease in chronic renal disease. Am J Kidney Dis 32(suppl 3):S112–S119,1998
3. Blacher J, Guerin AP, Pannier B, Marchais SJ, Safar ME, London GM:Impact of aortic stiffness on survival in end-stage renal disease. Circulation99:2434–2439, 1999
4. McVeigh GE, Bratteli CW, Morgan DJ, Alinder CM, Glasser SP, Finkel-stein SM, Cohn JN: Age-related abnormalities in arterial compliance iden-tified by pressure pulse contour analysis. aging and arterial compliance.Hypertension 33:1392–1398, 1999
5. O’Rourke MF: Wave travel and reflection in the arterial system. J Hypertens17(suppl 5):S45–S47, 1999
6. van Bortel LM, Spek JJ: Influence of aging on arterial compliance. J HumHypertens 12:583–586, 1998
7. Black HR, Kuller LH, O’Rourke MF, Weber MA, Alderman MH, BenetosA, Burnett J, Cohn JN, Franklin SS, Mancia G, Safar M, Zanchetti A: Thefirst report of the Systolic and Pulse Pressure (SYPP) Working Group. JHypertens 17(suppl 5):S3–S14, 1999
8. Rostand SG, Brunzell JD, Cannon ROI, Victor RG: Cardiovascular com-plications in renal failure. J Am Soc Nephrol 2:1053–1062, 1991
9. Guerin AP, London GM, Marchais SJ, Metivier F: Arterial stiffening andvascular calcifications in end-stage renal disease. Nephrol Dial Transplant15:1014–1021, 2000
10. Demuth K, Blacher J, Guerin AP, Benoit MO, Moatti N, Safar ME, LondonGM: Endothelin and cardiovascular remodelling in end-stage renal disease.Nephrol Dial Transplant 13:375–383, 1998
11. Converse RL Jr, Jacobsen TN, Toto RD, Jost CMT, Cosentino F, Fouad-Tarazi F, Victor RG: Sympathetic overactivity in patients with chronic renalfailure. N Engl J Med 327:1912–1918, 1992
12. Tycho Vuurmans JL, Boer WH, Bos WJ, Blankestijn PJ, Koomans HA:Contribution of volume overload and angiotensin II to the increased pulsewave velocity of hemodialysis patients. J Am Soc Nephrol 13:177–183, 2002
13. Lloyd-Jones DM, Evans JC, Larson MG, O’Donnell CJ, Levy D: Differ-ential impact of systolic and diastolic blood pressure level onJNC-VI staging.Hypertension 34:381–385, 1999
14. Hyman DJ, Pavlik VN: Characteristics of patients with uncontrolledhypertension in the United States. N Engl J Med 345:479–486, 2001
15. Franklin SS, Larson MG, Khan SA, Wong ND, Leip EP, Kannel WB, LevyD: Does the relation of blood pressure to coronary heart disease risk changewith aging? The Framingham Heart Study. Circulation 103:1245–1249, 2001
16. Khattar RS, Swales JD, Dore C, Senior R, Lahiri A: Effect of aging on theprognostic significance ofambulatory systolic, diastolic, and pulse pressure inessential hypertension. Circulation 104:783–789, 2001
17. Blacher J, Staessen JA, Girerd X, Gasowski J, Thijs L, Liu L, Wang JG,Fagard RH, Safar ME: Pulse pressure not mean pressure determines car-diovascular risk in older hypertensive patients. Arch Intern Med 160:1085–1089, 2000
18. Coresh J, Wei GL, McQuillan G, Brancati FL, Levey AS, Jones C, Klag MJ:Prevalence of high blood pressure and elevated serum creatinine level in theUnited States: findings from the third National Health and NutritionExamination Survey (1988–1994). Arch Intern Med 161:1207–1216, 2001
19. Brenner BM, Cooper ME, deZeeuw D, KeaneWF, MitchWE, Parving HH,Remuzzi G, Snapinn SM, Zhang Z, Shahinfar S: Effects of losartan on renaland cardiovascular outcomes in patients with type 2 diabetes and nephrop-athy. N Engl J Med 345:861–869, 2001
20. Lewis EJ, Hunsicker LG, Clarke WR, Berl T, Pohl MA, Lewis JB, Ritz E,Atkins RC, Rohde R, Raz I: Renoprotective effect of the angiotensin-re-ceptor antagonist irbesartan in patients with nephropathy due to type 2diabetes. N Engl J Med 345:851–860, 2001
21. Wright JT, Jr., Bakris G, Greene T, Agodoa LY, Appel LJ, Charleston J,Cheek D, Douglas-Baltimore JG, Gassman J, Glassock R, Hebert L,Jamerson K, Lewis J, Phillips RA, Toto RD, Middleton JP, Rostand SG:Effect of blood pressure lowering and antihypertensive drug class on pro-gression of hypertensive kidney disease: results from the AASK trial. JAMA288:2421–2431, 2002
22. Rocco MV, Yan G, Heyka RJ, Benz R, Cheung AK: Risk factors for hy-pertension in chronic hemodialysis patients: baseline data from the HEMOstudy. Am J Nephrol 21:280–288, 2001
23. Tozawa M, Iseki K, Iseki C, Oshiro S, Yamazato M, Higashiuesato Y,Tomiyama N, Tana T, Ikemiya Y, Takishita S: Evidence for elevated pulsepressure in patients on chronic hemodialysis: a case-control study. Kidney Int62:2195–2201, 2002
24. Agarwal R, Lewis RR: Prediction of hypertension in chronic hemodialysispatients. Kidney Int 60:1982–1989, 2001
25. Tomita J, Kimura G, Inoue T, Inenaga T, Sanai T, Kawano Y, Nakamura S,Baba S, Matsuoka H, Omae T: Role of systolic blood pressure in determiningprognosis of hemodialyzed patients. Am J Kidney Dis 25:405–412, 1995
26. Klassen PS, Lowrie EG, Reddan DN, DeLong ER, Coladonato JA, SzczechLA, Lazarus JM, Owen WF, Jr: Association between pulse pressure andmortality in patients undergoing maintenance hemodialysis. JAMA287:1548–1555, 2002
27. Foley RN, Herzog CA, Collins AJ: Blood pressure and long-term mortalityin United States hemodialysis patients: USRDS Waves 3 and 4 study. KidneyInt 62:1784–1790, 2002
28. Tozawa M, Iseki K, Iseki C, Takishita S: Pulse pressure and risk of totalmortality and cardiovascular events in patients on chronic hemodialysis.Kidney Int 61:717–726, 2002
29. Cruickshank JM: Coronary flow reserve and the J curve relation betweendiastolic blood pressure and myocardial infarction. BMJ 297(6658):1227–1230, 1988
30. Hansson L, Zanchetti A, Carruthers SG, Dahlof B, Elmfeldt D, Julius, S,Menard J, Rahn KH, Wedel H, Westerling S: Effects of intensive blood-pressure lowering and low-dose aspirin in patients with hypertension: prin-cipal results of the Hypertension Optimal Treatment (HOT) randomisedtrial. HOT Study Group. Lancet 351(9118):1755–1762, 1998
31. Ruilope LM, Salvetti A, Jamerson K, Hansson L, Warnold I, Wedel H,Zanchetti A: Renal function and intensive lowering of blood pressure inhypertensive participants of the hypertension optimal treatment (HOT)study. J Am Soc Nephrol 12:218–225, 2001
32. Prevention of strokebyantihypertensive drug treatment in olderpersonswithisolated systolic hypertension. Final results of the Systolic Hypertension inthe Elderly Program (SHEP). SHEP Cooperative Research Group. JAMA265:3255–3264, 1991
33. Tuomilehto J, Rastenyte D, Birkenhager WH, Thijs L, AntikainenR, BulpittCJ, Fletcher AE, Forette F, Goldhaber A, Palatini P, Sarti C, Fagard R:Effects of calcium-channel blockade in older patients with diabetes and sys-tolic hypertension. Systolic Hypertension in Europe Trial Investigators [seecomments]. N Engl J Med 340:677–684, 1999
Agarwal212

34. Kjeldsen SE, Dahlof B, Devereux RB, Julius S, Aurup P, Edelman J, BeeversG, de Faire U, Fyhrquist F, Ibsen H, Kristianson K, Lederballe-Pedersen O,Lindholm LH, Nieminen MS, Omvik P, Oparil S, Snapinn S, Wedel H:Effects of losartan on cardiovascular morbidity and mortality in patients withisolated systolic hypertension and left ventricular hypertrophy: a LosartanIntervention for Endpoint Reduction (LIFE) substudy. JAMA 288:1491–1498, 2002
35. Agarwal R: Assessment of blood pressure in hemodialysis patients. SeminDial 15:299–304, 2002
36. Sacks FM, Svetkey LP, Vollmer WM, Appel LJ, Bray GA, Harsha D,Obarzanek E, Conlin PR, Miller ER, III, Simons-Morton DG, Karanja N,Lin PH: Effects on blood pressure of reduced dietary sodium and the DietaryApproaches to Stop Hypertension (DASH) diet. DASH-Sodium Collabor-ative Research Group. N Engl J Med 344:3–10, 2001
37. Chrysanthakopoulos SG, Kastagir BK, Jubiz W, Kolff WJ: Hypertension inpatients on maintenance hemodialysis: evaluation of peripheral renin activityand bilateral nephrectomy. Am J Med Sci 264:9–21, 1972
38. Simon G, Jaeckel M, Illyes G: Altered structure and distensibility of arteriesin salt-fed rats. J Hypertens 21:137–143, 2003
39. Miller BW, Cress CL, Johnson ME, Nichols DH, Schnitzler MA: Exerciseduring hemodialysis decreases the use of antihypertensive medications. Am JKidney Dis 39:828–833, 2002
40. Charra B: ‘‘Dry weight’’ in dialysis: the history of a concept. Nephrol DialTransplant 13:1882–1885, 1998
41. Chazot C, Charra B, Vo VC, Jean G, Vanel T, Calemard E, Terrat JC, RuffetM, Laurent G: The Janus-faced aspect of ‘‘dry weight.’’ Nephrol DialTransplant 14:121–124, 1999
42. Lins RL, Elseviers M, Rogiers P, Van Hoeyweghen RJ, De Raedt H, ZacheeP, Daelemans RA: Importance of volume factors in dialysis related hyper-tension. Clin Nephrol 48:29–33, 1997
43. Katzarski KS, Charra B, Luik AJ, Nisell J, Divino Filho JC, Leypoldt JK,Leunissen KM, Laurent G, Bergstrom J: Fluid state and blood pressurecontrol in patients treated with long and short haemodialysis. Nephrol DialTransplant 14:369–375, 1999
44. Weise F, London GM, Pannier BM, Guerin AP, Elghozi JL: Effect ofhemodialysis on cardiovascular rhythms in end-stage renal failure.Kidney Int47:1443–1452, 1995
45. Agarwal R: Strategies and feasibility of hypertension control in a prevalenthemodialysis cohort. Clin Nephrol 53:344–353, 2000
46. London GM, Pannier B, Guerin AP, Marchais SJ, Safar ME, Cuche JL:Cardiac hypertrophy, aortic compliance, peripheral resistance, and wavereflection in end-stage renal disease. Comparative effects of ACE inhibitionand calcium channel blockade. Circulation 90:2786–2796, 1994
47. Rahman M, Dixit A, Donley V, Gupta S, Hanslik T, Lacson E, Ogundipe A,Weigel K, Smith MC: Factors associated with inadequate blood pressurecontrol in hypertensive hemodialysis patients. Am J Kidney Dis 33:498–506,1999
48. Zager PG, Nikolic J, Brown RH, Campbell MA, Hunt WC, Peterson D, VanStone J, Levey A, Meyer KB, Klag MJ, Johnson HK, Clark E, Sadler JH,
Teredesai P: ‘‘U’’ curve association of blood pressure and mortality inhemodialysis patients. Medical Directors of Dialysis Clinic, Inc. Kidney Int54:561–569, 1998 [published erratum, Kidney Int 54:1417, 1998]
49. Salem MM: Hypertension in the haemodialysis population: any relationshipto 2-years survival? Nephrol Dial Transplant 14:125–128, 1999
50. Agarwal R: Supervised atenolol therapy in management of hemodialysishypertension. Kidney Int 55:1528–1535, 1999
51. Agarwal R, Lewis RR, Davis JL, Becker B: Lisinopril therapy for hemodi-alysis hypertension—hemodynamic and endocrine responses. Am J KidneyDis 38:1245–1250, 2001
52. Efrati S, Zaidenstein R, Dishy V, Beberashvili I, Sharist M, Averbukh Z,Golik A, Weissgarten J: ACE inhibitors and survival of hemodialysis pa-tients. Am J Kidney Dis 40:1023–1029, 2002
53. Zazgornik J, Biesenbach G, Forstenlehner M, Stummvoll K: Profile ofantihypertensive drugs in hypertensive patients on renal replacement therapy(RRT). Clin Nephrol 48:337–340, 1997
54. London GM, Marchais SJ, Guerin AP, Metivier F, Safar ME, Fabiani F,Froment L: Salt and water retention and calcium blockade in uremia. Cir-culation 82:105–113, 1990
55. Marchais SJ, Boussac I, Guerin AP, Delavaux G, Metivier F, London GM:Arteriosclerosis and antihypertensive response to calcium antagonists in end-stage renal failure. J Cardiovasc Pharmacol 18(suppl 5):S14–S18, 1991
56. Charra B: Control of blood pressure in long slow hemodialysis. Blood Purif12:252–258, 1994
57. Charra B, Calemard E, Ruffet M, Chazot C, Terrat J-C, Vanel T, et al:Survival as an index of adequacy of dialysis. Kidney Int 41:1286–1291, 1992
58. Fagugli RM, Reboldi G, Quintaliani G, Pasini P, Ciao G, Cicconi B, PasticciF, Kaufman JM, Buoncristiani U: Short daily hemodialysis. blood pressurecontrol and left ventricular mass reduction in hypertensive hemodialysispatients. Am J Kidney Dis 38:371–376, 2001
59. Kielstein JT, Boger RH, Bode-Boger SM, Schaffer J, Barbey M, Koch KM,Frolich JC: Asymmetric dimethylarginine plasma concentrations differ inpatients with end-stage renal disease: relationship to treatment method andatherosclerotic disease. J Am Soc Nephrol 10:594–600, 1999
60. Friedman AN, Bostom AG, Levey AS, Rosenberg IH, Selhub J, Pierratos A:Plasma total homocysteine levels among patients undergoing nocturnalversus standard hemodialysis. J Am Soc Nephrol 13:265–268, 2002
61. Pierratos A, Ouwendyk M, Francoeur R, Vas S, Raj DS, Ecclestone AM,Langos V, Uldall R: Nocturnal hemodialysis: three-year experience [seecomments]. J Am Soc Nephrol 9:859–868, 1998
62. Hanly PJ, Pierratos A: Improvement of sleep apnea in patients with chronicrenal failure who undergo nocturnal hemodialysis. N Engl J Med 344:102–107, 2001
63. Chazot C, Charra B, Laurent G, Didier C, Vo VC, Terrat JC, Calemard E,Vanel T, Ruffet M: Interdialysis blood pressure control by long haemodi-alysis sessions. Nephrol Dial Transplant 10:831–837, 1995
64. McGregor DO, Buttimore AL, Nicholls MG, Lynn KL: Ambulatory bloodpressure monitoring in patients receiving long, slow home haemodialysis.Nephrol Dial Transplant 14:2676–2679, 1999
SYSTOLIC HYPERTENSION IN HEMODIALYSIS 213