Embed Size (px)
Citation preview

Review
10.1586/17469899.3.3.279 © 2008 Expert Reviews Ltd ISSN 1746-9899 279www.expert-reviews.com
Systemic and ophthalmic manifestations of West Nile virus infectionExpert Rev. Ophthalmol. 3(3), 279–292 (2008)
Yos Priestley, Marcia Thiel and Steven B Koevary†
†Author for correspondenceDepartment of Biomedical Sciences and Disease, New England College of Optometry, 424 Beacon Street, Boston, MA 02115, USATel.: +1 617 587 5614Fax: +1 617 587 [email protected]
The first cases in the USA of infection with the mosquito vector-borne West Nile virus (WNV) –an enveloped, single-stranded RNA – occurred in 1999 in New York. Since then, it has movedwestward and now affects people in nearly every state, with most annual cases appearing inlate summer. Suspected infection can be confirmed by ELISA and reverse transcriptase PCR. Theincubation period of WNV prior to the onset of symptoms can be as long as 2 weeks. Threeclinical categories of infection have been defined: asymptomatic, West Nile fever (WNF) andWest Nile meningoencephalitis. The most common symptoms of WNF are flu-like and includefever, headache, myalgia, malaise, diarrhea, vomiting and fatigue. In less than 1% of cases,individuals develop severe, potentially fatal neurologic disease that has been variously classifiedas West Nile meningitis, West Nile encephalitis and West Nile poliomyelitis (acute flaccidparalysis). The most commonly reported ocular features of WNV infection are multifocal,bilateral chorioretinal lesions characteristically found in either a scattered or linear pattern.Other features include anterior uveitis, retinal vasculitis, optic neuritis and vitritis; lesscommonly, nystagmus, abducens nerve palsy, optic disc edema and absence of corneal reflexhave been reported. Patients were also reported to present with blurred vision, floaters,redness, visual field defects and diplopia. Ocular symptoms of WNV are generally self limited;however, in some notable cases, reduced visual acuity and field loss may persist. Many of theocular symptoms of WNV infection are associated with numerous viral, bacterial and parasiticdiseases, highlighting the importance of differential diagnosis in confirming WNV infection. Thefact that ophthalmic manifestations associated with WNV have only been recognized relativelyrecently makes the long-term prognosis in patients difficult to predict. However, most patientspresenting with chorioretinitis show improvement over time, with visual acuity returning tobaseline after a few months. There are currently no approved treatments for WNV, althoughrecombinant vaccines are under development.
KEYWORDS: anterior uveitis • chorioretinitis • encephalitis • meningitis • optic neuritis • retinal vasculitis • vitritis • West Nile virus
West Nile Virus (WNV) is a member of theJapanese encephalitis virus serocomplex and isan enveloped, single-stranded RNA virus of thegenus Flavivirus. The envelope (E)-glycoproteinof the virus mediates its attachment to the hostcell and also induces the production of virus-neutralizing antibodies. This serogroup ofviruses is associated with the development ofvarious types of encephalitis, including the Jap-anese, St Louis, Murray Valley and Australianvarieties; the latter of which is caused by Kunjinvirus, a subtype of WNV. Antigenic similaritiesamong these viruses and other Flavivirusesaccount for their serological cross-reactivity inlaboratory diagnostic testing [1].
West Nile disease is caused by viruses that dis-play one of two lineages, based on their nucleicacid sequence. Lineage 1 strains are distributedthroughout North America, Eastern Europe,the Middle East, West Africa and Australia. Incontrast to the worldwide distribution of line-age 1, lineage 2 strains have only been isolatedin sub-Saharan Africa and Madagascar [2].
Epidemiology & risk factors
West Nile virus was first isolated in the West Niledistrict of Uganda in 1937 from the blood of afebrile woman [3] and was first identified as acause of meningoencephalitis during an outbreak

280 Expert Rev. Ophthalmol. 3(3), (2008)
Review Priestley, Thiel & Koevary
in an Israeli nursing home in 1957. Since then, outbreaks havebeen reported throughout the world, with the first infection inthe USA reported in August 1999 in the New York City (NY,USA) area [4]. While it is not known with certainty how thevirus reached the western hemisphere, its close homology(>99.8%) to an isolate found in Israel suggests that it arrivedfrom the Middle East [5]. Furthermore, the only strains ofWNV found to be fatal in both birds and humans are found inthe USA and Israel [6].
Since its arrival in the USA, WNV has gradually spread west-ward. In 2000, 21 cases of disease were reported in three stateson the East Coast and, by the following year, 66 cases werereported in ten states. In 2002, the number of virus infectionsand states affected jumped dramatically to 4156 and 39, respec-tively [7]. According to the US Centers for Disease Control(CDC) website, there have been a total of 27,573 reported casesof WNV infections since its initial incursion in 1999 through2007, including 1083 fatalities in a total of 43 states [101]. It isestimated that over 750,000 have gone undiagnosed [101].
General risk factors for contracting WNV include the time ofyear and geographical region. In temperate regions, incidencepeaks in August or September owing to the high number ofmosquitoes, while those living in the South appear to be at riskyear-round because of their perennially warmer weather pat-terns. As mentioned previously, while the virus has beenreported in most states, it is generally thought that riskincreases for individuals who spend appreciable time in areaswhere mosquito-borne viruses are common, such as the EastCoast and the Midwest. Individuals who work outdoors arealso thought to be at an increased risk [6,8,102].
Patients with the following conditions were reported to havean increased risk of developing severe WNV disease: diabetesmellitus, hypertension, HIV, rheumatoid arthritis, coronary dis-ease, cancer, organ transplant recipients on immunosuppressivetherapy, patients on mechanical ventilation, history of stroke,and alcoholism [2,4,6,9–11]. Patients with diabetes were alsoreported to be at increased risk of developing ischemic macu-lopathy [12]. Advanced age has also been linked to severe WNVdisease [4,6,13]. A study by Chowers et al. found an elevated riskof neuroinvasive disease in patients 70 years of age or over [14].Children have also been shown to be at greater risk primarilybecause they tend to spend more time outdoors during high-risk times of the year [15]. In keeping with the association ofmore severe disease with increasing age, children generally seemto experience fewer complications and morbidity from WNVinfection than do adults greater than 18 years of age [15].
A study by Glass et al. suggested that there might be a geneticbasis for human susceptibility. A genetic mutation of CCR5, achemokine receptor, results in the creation of the CCR5∆32allele. While this mutation was shown to be beneficial in pro-tecting T cells from being infected by HIV [16], the study byGlass et al. suggests that it also increases the risk of fatal WNVinfection [17]. Among patients with confirmed WNV infection,4–8% were homozygous for CCR5∆32; by contrast, only
approximately 1% of the general population in the USA ishomozygous for the mutated allele [18]. Patients who arehomozygous for CCR5∆32 also had a higher mortality ratethan those who did not carry the mutation. This mutationappears most commonly in Caucasian populations. In light ofthe foregoing, patients with HIV-1 who receive CCR5 antago-nist therapy are at increased risk of developing severe WNVinfection [18].
Diagnostic tests
Suspected WNV infection is confirmed on the basis of the fol-lowing laboratory tests: IgM and IgG ELISAs, plaque reductionneutralization test (PRNT), immunoflourescence (IFA) and anucleic acid amplification test (NAT). When WNV is sus-pected, cerebrospinal fluid and serum samples can be tested forthe presence of WNV IgM antibodies using the IgM antibodycapture (MAC)-ELISA; this test is most accurate when per-formed 8–21 days postinfection. A more definitive diagnosiscan be made if the patient exhibits a fourfold or greater increasein their IgM antibody titer in serum samples collected 2–3weeks apart using the PRNT. In light of the fact that IgM levelsare only elevated for a brief period after infection, IgG-basedtest kits are more often used to confirm a diagnosis of WNV,since IgG antibodies are known to persist after infection; insuch an assay, a fourfold increase in IgG titer confirms a diag-nosis of WNV. Commercially produced IFA kits are also availa-ble to confirm WNV, which are easier to use than PRNT. Sincecross-reactivity of WNV with other flaviviruses is very commonin the aforementioned-mentioned assays, it may be necessary insome cases to confirm a diagnosis of WNV using the moredefinitive NAT reverse transcriptase (RT) PCR test. MRI isgenerally performed to assess the presence and/or extent ofWNV-induced lesions in patients with neuroinvasive disease,most notably paralysis [19–21].
Immune response to the virus
Data suggest that antibody, T-cell, dendritic cell and macrophageresponses play important roles in anti-WNV immunity [22]. Infact, it is the replication of the virus in dendritic cells at thesite of inoculation and its spread from there to regional lymphnodes that is thought to be the mode of establishment ofinfection in the body [23]. The binding of double-strandedWNV RNA to Toll-like receptor-3, resulting in the upregula-tion of TNF-α production and a subsequent increase inblood–brain barrier permeability, appears to play a role inviral penetration into the CNS [24]. The importance of anti-bodies was made clear in B cell-deficient mice that uni-formly died after WNV infection but were protected by pas-sive transfer of immune sera [25]. Consistent with animportant role for T cells, it was reported that individualswith hematologic malignancies and impaired T-cell functionhad an increased risk of developing neuroinvasive WNV

Systemic & ophthalmic manifestations of West Nile virus infection Review
www.expert-reviews.com 281
infection [22]. Fredericksen et al. reported that WNV inducedthe expression of IFN-β and several IFN-stimulated genes latein infection of cultured human cells but that despite this hostresponse, it was still able to replicate efficiently [26]. The fore-going notwithstanding, more recent data suggest that WNVinduces an antiviral state in retinal pigment epithelium(RPE) cells by a mechanism that seems to employ the IFNsignaling pathway [27]. Interestingly, through an unknownmechanism, flavivirus nonstructural proteins were reported tosuppress host antiviral immune responses [28].
Transmission
West Nile virus is a vector-borne disease that is transmittedthrough the bite of infected Culex mosquitoes. The mosquitoes actas a maintenance vector by infecting birds that act as amplifyinghosts. Birds that are most susceptible to WNV disease are crowsand blue jays of the family Corvidae. Infection in birds results in ahigh level of viremia, which facilitates the enzootic cycle of mos-quito transmission [6,29]. At any point during this cycle, an infectedmosquito can act as a ‘bridge vector’ by spreading the virus tohumans through a bite [6]. Viral amplification occurs during thesummer months in the enzootic cycle and culminates in the earlyfall when the mosquitoes begin to bite humans. Thus, upwards of85% of human infections occur during the months of August andSeptember [8]. Vectoral transmission of WNV by mosquitoes fromhuman to human is not thought to occur because of the lowreported levels of viremia in infected individuals [29]. However,WNV has been reported to have been passed on to others byblood transfusion, organ transplantation and vertically frommother to child.
The first cases of WNV that were acquired through bloodtransfusion and organ transplantation were reported in Augustof 2002 during a major outbreak in the USA. Of note was thereported case of transmission to four recipients of organs trans-planted from a common donor [30]. The organ donor hadreceived blood products from 63 donors before her death, one ofwhom had asymptomatic WNV. Following her last transfusion,her serum and plasma tested positive for the presence of WNVisolates. Three of the four organ recipients developed West Nileencephalitis (WNE) while the fourth developed symptoms ofWN fever (WNF; see later). More recently, additional cases ofviral transmission through tainted blood transfusions and organtransplants have been reported [31–33].
Shortly after reports surfaced that WNV could be transmit-ted by infected blood and transplanted organs, came reports oftransmission of the virus to the fetus and neonate through theplacenta and breast milk, respectively. In 2003, it was reportedthat a woman of 20 years of age contracted WNV 2 monthsbefore delivering a live infant at 38 weeks of gestation. Theinfant had normal physical features, but was found to havebilateral chorioretinitis, severe bilateral loss of white matter inboth temporal and occipital lobes of the brain, and cystic cere-bral tissue destruction in one temporal lobe [34]. The infant’s
serum and CSF tested positive for WNV-specific IgM [34].While additional complications have been reported followingWNV infection in utero, it remains unclear whether the virusplayed a role in their development. Data suggest that congenitalWNV infection can not be ruled out, based on a negative sero-logical finding of cord blood [35,103]. Though confirmed trans-mission of WNV through breast milk has only been reported inone case, it is perhaps prudent to counsel against this practicein mothers who have been diagnosed with WNV infection [102].
Prevention
Exposure to WNV can be limited in a variety of ways. Personalprotection, mosquito control programs, and screening of bloodand organs for transplantation are central to reducing risk. Per-sonal protection during the months of August and Septemberincludes staying indoors between dusk and dawn when mos-quitoes are most active, wearing protective clothing when out-doors (i.e., long sleeves and pants with socks and shoes), andusing mosquito repellants. The most effective mosquito repel-lant for use on skin is N,N-diethyl-m-toluamide (DEET) [36].Other substances can be used, including repellants containingpicaridin and oil of lemon eucalyptus [37]. The CDC recom-mends three types of mosquito control: larvicide, adulticideand breeding site reduction. Larviciding involves using chemi-cals that are toxic to mosquito larvae while adulticidinginvolves the use of chemicals which are toxic to adult mosqui-toes. Removal of standing water in barrels, buckets, gutters andflowerpots, which can be used as breeding sites, also helps toreduce the mosquito population [37].
In addition, as mentioned above, those receiving blood trans-fusions and organ transplants face the risk of acquiring the dis-ease from infected donors. The first US FDA-approved stand-alone test for screening the blood of donors was the Procleix®
WNV Assay, approved in 2005 [104]. The Procleix assay is ableto detect WNV RNA, and can therefore identify infected donorblood and tissues before antibodies are present. The Procleix®
TIGRIS® is a fully automated test approved in March of 2007for blood, tissue and organ screening [105]. As a fully automatedsystem, the TIGRIS is especially useful during times of highWNV activity and reduces the risk of human error. Shortlythereafter, the FDA approved the cobas TaqScreen WNV test, asecond test for screening donated tissues [106]. The cobasTaqScreen WNV test can detect viral RNA in plasma specimensfrom donors of whole blood and blood components as well asdonor cells and other tissues. Additionally, the test can be usedto test the plasma of organ donors, but only when specimens areobtained while the donor’s heart is still beating [106].
Systemic clinical features of infection
The incubation period of WNV prior to the onset of symp-toms ranges from 2 to 14 days. This said, most patientsinfected with WNV are asymptomatic and many cases go

282 Expert Rev. Ophthalmol. 3(3), (2008)
Review Priestley, Thiel & Koevary
unreported. Symptoms are estimated to develop in only20–40% of individuals who are infected by the virus [19]. Threeclinical categories of infection have been defined: asymptomatic,WNF, and WN meningoencephalitis (WNM). WNF occursmuch more frequently than WNM. The most common symp-toms of WNF are flu-like and include fever, headache, myalgia,malaise, diarrhea, vomiting and fatigue [4,6,21,38]. Other reported,but less common, features include a maculopapular rash on thechest, back and lower extremities, pharyngitis, arthralgias, seizuresand hearing loss [11,39–43]. Less-common organ involvementincludes hepatitis, pancreatitis, myocarditis and orchitis. Onepatient with diagnosed WNV presented with diffuse monomor-phic skin eruptions comprised of erythematous papules that spreadto the patient’s face, palms, and soles [44]. A maculopapular rash isseen most often in patients with WNF or WNM rather thanWNE [42]. Symptoms of WNF usually subside in less than a weekand patients generally recover within days to months [11,45,46].
In less than 1% of cases, individuals develop severe, potentiallyfatal neurologic disease that has been variously classified asWNM, WNE, and WN poliomyelitis (WNP; acute flaccidparalysis). TABLE 1 highlights the percentages of cases in each cate-gory of WNV disease in humans and the most common symp-toms of each. As evidenced, many symptoms overlap in givenindividuals, making diagnosis difficult; however, given the highmortality rate and more severe complications of the encephaliticform of the disease, settling on a correct diagnosis is critical.
WNM presents as would a typical meningitis, with symp-toms including fever, headache, stiff neck, nuchal rigidity andphotophobia [4,11,20,21]. Other symptoms may include respira-tory failure, limb weakness and cardiac arrhythmia [11]. WNEcan develop as the disease begins to involve the brain. Whenthis occurs, additional, serious symptoms may develop, includ-ing altered mental status and state of consciousness, dysarthria,seizures, tremor, ataxia, involuntary movements, parkinsonismand cranial nerve palsies [4,11,20,21]. In one reported case byBode et al. only 21% of patients with WNE who survived acutedisease returned to their original level of neurological functionfollowing hospitalization [11]. It is not clear why or how theinfection targets certain regions of the CNS; regions of thebrain that were shown to be susceptible include the medulla [6],basal ganglia [2,6,47,48] and thalamus [2,21,48].
A rare but clearly important neuroinvasive condition that hasbeen associated with WNV infection is acute flaccid paralysis,which develops as a result of a reduction in anterior horn motorresponse amplitudes [20]. Many of these patients initially presentwith the typical flu-like symptoms of WNF and go on to developmuscle weakness a week or two later [19]. Symptoms were reportedto range from weakness in one limb to flaccid quadriplegia[20,50–52]. At autopsy, a 41 year old patient with WNP was reportedto have severe neuronal loss and gliosis in his spinal cord anteriorhorns and substantia nigra; his anterior horn nerve roots and sub-stantia nigra also showed severe atrophy and neurofibrillary tangle
Table 1. Estimated percentage of overall infections, median ages affected, acute clinical features and estimated case fatality rate of the acute clinical syndromes associated with human West Nile virus infection*
Variable West Nile fever West Nile neuroinvasive disease
West Nile meningitis West Nile encephalitis West Nile poliomyelitis
Estimated percentage of overall infections
20 <1‡ <1‡ <1‡
Estimated percentage of WNND cases
Not applicable 35–40 55–60 Unknown but may be 5–10§
Acute clinical features Abrupt onset of fever, headache, malaise, fatigue, anorexia and nausea
Symptoms of WNF, plus meningismus (nuchal rigidity, photo and phonophobia); CSF with pleocytosis; white blood cell count generally < 500 cells/mm3
Symptoms of WNF, plus encephalopathy (altered mental status, lethargy), and/or focal neurologic signs (weakness, cranial nerve palsies); movement disorders, including tremor, parkinsonism and ataxia, may be frequent
Acute onset of limb weakness or paralysis; weakness is typically asymmetric and abrupt; involved limbs typically are flaccid and areflexic; respiratory muscles may be involved; WNP may occur in the absence of fever or other features suggestive of WNV infection
Estimated case fatality rate
<1 <1 20 10–50
*Syndromes include WNF, West Nile meningitis, West Nile encephalitis and WNP.‡Overall, WNND represents 1% of human WNV infections.§ WNP may occur in the context of any other manifestation of WNV infection or in isolation, without associated fever, meningitis, or encephalitis.Modified with permission from [47].WNF: West Nile fever; WNND: West Nile neuroinvasive disease; WNP: West Nile poliomyelitis.

Systemic & ophthalmic manifestations of West Nile virus infection Review
www.expert-reviews.com 283
formation, respectively [53]. While many patients with severe flac-cid paralysis due to WNP are misdiagnosed with Guillain–Barresyndrome (GBS), very few have had confirmed demyelinatingneuropathy in nerve conduction studies [6,19,20,54]. Prognosis is var-iable, with some patients recovering fully in weeks while othershave continued to suffer long-term complications [55]. Cranialnerve involvement, while uncommon, has also been reported inthese patients, with CN7 being preferentially affected, resulting infacial paralysis and weakness [20,56].
Differential diagnosis of systemic disease
In light of its rise in incidence in the USA, it behooves cliniciansto consider a diagnosis of WNV when patients display symptomsin common with Legionnaires disease, Mycoplasma meningeoen-cephalitis, listeria meningoencephalitis, rocky mountain spottedfever, ehrlichiosis, malaria, and herpes simplex virus 1 [57]. As men-tioned previously, WNP may be misdiagnosed as GBS, both ofwhich share severe flaccid paralysis as their most important symp-tom. Rash, abdominal and back pain preceding a proximal asym-metric flaccid weakness along with fever may help to distinguishWNP from GBS [20]. Symptoms of WNV can often mimic com-mon complications associated with other systemic diseases, result-ing in its under- or misdiagnosis in immunocompromizedpatients. Thus, patients with HIV who are susceptible to a host ofCNS complications may be misdiagnosed when they develop neu-roinvasive symptoms of WNV [58]. The fact that paralysis is a gen-erally uncommon symptom of viral infection makes a correct diag-nosis of WNV especially difficult in patients who do not presentwith meningitis or encephalitis. WNV has even been shown tomimic herpes simplex encephalitis when a patient presented with arare symptom of focal seizures in addition to meningoencephalitis.Only when a negative herpes test result was obtained did physi-cians consider other possibilities, including WNV – an epidemicof which was affecting patients in the area [41]. WNV can alsoaffect other organs and may manifest itself as hepatitis, pancreati-tis and myocarditis [29]. In one case, WNV was isolated from apatient who presented with hemorrhagic disease, highlighting thebroadening clinical spectrum of the disease [59]. WNV should beconsidered in the differential diagnosis of patients that presentwith any of the aforementioned symptoms, especially if they do soduring the summer and fall months.
Ocular manifestations of infection
While the systemic manifestations of WNV infections have beenwell studied, ocular involvement was only first identified in 2003.The most commonly reported ocular features of infection include:linearly arranged or scattered chorioretinal lesions, anterior uveitis,retinal vasculitis, optic neuritis and vitritis [29,56,59–61]. Less com-monly, patients exhibit neuroophthalmological findings such asnystagmus [21,62,63], abducens nerve palsy [56,62], optic discedema [55] and absence of a corneal reflex [21]. Patients werealso reported to present with blurred vision, floaters, redness,
visual field defects and diplopia [61,62]. Ocular symptoms ofWNV are generally self-limited, but in some notable casesreduced visual acuity and field loss may persist [12,60,61,64,65].
Chorioretinitis
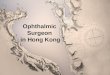
The most commonly reported ocular features of WNV infectionare multifocal, bilateral chorioretinal lesions characteristicallyfound in either a scattered or linear pattern [29,66,67]. A prospectivestudy conducted in Tunisia found that 20 out of 29 patients seenwith WNV had chorioretinal lesions [62]. The size of the lesionscan range from 100 to 1500 µm, with most being 200–500 µm.Active lesions have distinct margins, appear circular, flat, deep andwhitish/yellow in color upon ophthalmoscopy, are typically foundin the midzone and periphery of the temporal and superior nasalquadrants and may also involve the posterior pole [62,63]. Inactivelesions are partially atrophic and partially pigmented with a centralhypoflorescence and a peripheral hyperflorescence upon fluores-cence angiography, resulting in a target-like appearance. A studyby Khairallah et al. suggests that chorioretinal lesions are bestobserved using indocyanine green (ICG) (FIGURE 1) rather thanophthalmoscopy (FIGURE 2) and fluorescence angiography (FA)(FIGURE 3) [65]. While it was suggested that the virus causes chori-oretinitis by seeding the choroid by hematogenous disseminationduring viremia [29], other data indicate that that the characteristiclinear pattern seen in 80% of cases [62] develops in parallel with thepath of retinal nerve fibers, suggesting that the virus spreads fromthe CNS to the retina, RPE and choroid by way of the opticnerve [67]. Vitritis is often seen in patients with chorioretinitis;there has been only one reported case of stand-alone vitritis [29].
As indicated previously, patients may present with a range ofocular symptoms; however, it is important to note that most donot exhibit symptoms or display only a mild reduction in vision[29,51–58,60–62]. While most patients’ vision eventually returns tobaseline, the severity of their chorioretinitis certainly influencestheir outcome and recovery [65]. Diabetes has recently beenshown to be a risk factor for the development of more severe cho-rioretinitis and as such, these patients have a worse prognosis [68].Next, three cases of reported confirmed WNV associated chori-oretinitis of varying severity are described; in addition, a case isdescribed in which vitritis was the only ocular manifestation.
Case 1Myers et al. reported the case of a 68-year-old female with severevision loss due to extensive chorioretinitis [65]. The patient had ahistory of noninsulin-dependent diabetes, hypertension, conges-tive heart failure and coronary artery disease. She was hospitalizedwhen her fever, clear nasal discharge, headache, myalgia, fatigueand dry cough persisted for several days. Her condition soonworsened and she began to experience a change in mental status.Upon ocular examination, her visual acuity was light perceptionocular uterque (OU). Fundus examination revealed bilateral,multifocal chorioretinal lesions of variable sizes throughout themacula and mid-periphery. The vitreous was grossly clear and the

284 Expert Rev. Ophthalmol. 3(3), (2008)
Review Priestley, Thiel & Koevary
optic discs were pink and flat. Multiple small intraretinal hemor-rhages were observed OU, probably related to diabetic retino-pathy as the patient had a history of diabetes. No treatment wasgiven for the ocular symptoms. A total of 8 months later, thepatient’s health and mental status had recovered but visual acuityremained reduced to hand motions oculus dexter (OD) and lightperception oculus sinister (OS). The appearance of her fundi hadnot changed [65].
Case 2 Bains et al. reported the case of a patient with vitritis and chorio-retinitis [69]. This 62-year-old female, with a 2-week history offloaters in her left eye, as well as fatigue, headache and low grade afever, was found to have a visual acuity of 20/25 OD and 20/40OS. Slit lamp examination revealed a few anterior vitreous cellsOD and 2+ anterior cells OS. Ophthalmoscopy was significantwith chorioretinal lesions measuring 500–750 µm in the left eye;similarly, less extensive lesions were seen in the right eye. Lesionswere actively inflammatory and moderate vitritis was present in thesuperior retina of the left eye and overlying the optic disc. After2 weeks the patient’s vision improved to 20/30 OS, her vitritisimproved and her floaters diminished [69].
Case 3Garg and Jampol discussed the case of a patient with chori-oretinitis and long-term complications of subfoveal choroidalneovascularization [29]. The patient was a 73-year-old woman,with a history of well-controlled diabetes, who presented withfever, tremors, unintelligible speech, extreme lethargy andchanges in mental status which developed a few days after theonset of fatigue. At 1 week postadmission with supportive care,the patient reported blurry vision in her right eye. Acuity OD
was counting fingers (CF). Fluorescence angiography revealednumerous scattered white lesions ranging in size from 200 to500 µm. After 3 months, her visual acuity improved to 20/60OD. The authors suggested that a juxtafoveal chorioretinallesion may have caused the severe decrease in vision and that itsresolution over time led to improvement. After 18 months, thepatient’s visual acuity worsened again to CF OD due to thedevelopment of subfoveal choroidal neovascularization OD [29].
Case 4Yim et al. described an unusual case in which vitritis was the onlyocular manifestation in a 9-year-old Caucasian girl with confirmedWNV infection [70]. She presented with decreased vision in her lefteye that she had experienced since her initial diagnosis of acute oti-tis media and streptococcal pharyngitis 10 days earlier. Upon oph-thalmic examination, the patient displayed visual acuities of 20/20OD and 20/40 OS, with full visual fields and extraocular move-ments. Both of her anterior segments were normal. The posteriorsegment of her right eye revealed 1+ vitreous haze, 1+ vitreous cellswith 2 snowballs, and a small infratemporal area of snowbanking.The vitreous of her left eye showed 2–3+ vitreous haze with 2–3+cells with vitreous hemorrhage and possible snowbankinginfratemporally. The patient was treated with 1 drop of 1% pred-nisolone acetate every 2 h and showed slow improvement withcomplete recovery of vision within 6 months [70].
Anterior uveitis
Like vitritis, anterior uveitis is commonly seen along with cho-rioretinal lesions in patients with WNV. Often it is seen tran-siently early in the acute stage of ocular symptoms, whichaccounts for why it is easily missed [60]. Treatment of the uveitis
Figure 1. Indocyanine green angiography from a patient with confirmed West Nile virus infection. Late-phase indocyanine green angiograms of the (A) right eye and (B) left eye of a 58-year-old diabetic man with serologically confirmed West Nile virus infection show well-delineated hypofluorescent choroidal lesions that are more numerous than those appreciated by fluorescein angiography or clinically. Note the presence of a supramacular focal retinal arterial indocyanine green hyperfluorescence in the right eye.Reproduced with permission from [66].
A B

Systemic & ophthalmic manifestations of West Nile virus infection Review
www.expert-reviews.com 285
involves the use of topical anti-inflammatory drugs and, suchas other WNV ocular manifestations, is generally self limited[29,60–62]. The following are two cases of anterior uveitis thatwere reported in patients with confirmed WNV infection –first, a typical case of uveitis associated with chorioretinallesions [60] and, second, an unusual case of uveitis in theabsence of chorioretinal lesions [71].
Case 1In a case reported by Chan et al., a 71-year-old patient pre-sented in the emergency room (ER) with a history of fatigue,joint pain, diarrhea, malaise, confusion and fever for the previ-ous 10 days [60]. 1 month after presenting to the ER with symp-toms of WNV infection, the patient complained of blurryvision and floaters greater in OD than OS. Her visual acuitywas 20/40 OD and 20/30 OS. An examination of the anteriorsegment revealed mild cells in the anterior chambers of botheyes. Posterior segment evaluation showed moderate vitreouscells in the left eye. In addition, chorioretinal lesions wereobserved OU. Even though the patient was treated with topicalprednisolone acetate, the vision in her left eye worsened a fewweeks later to 20/200. Examination revealed normal anteriorsegments except for the presence of resolving cells in the ante-rior chambers. Examination of the left eye’s fundus revealedarterial narrowing, perivascular sheathing, and vascular occlu-sion consistent with retinal vasculitis. The dosage frequency oftopical prednisolone acetate was increased and the patient wasstarted on oral prednisolone treatment. At her most recentlyreported follow-up examination, her visual acuity hadimproved to 20/25 OD and 20/70 OS. Her reduced OS visionwas thought to be most likely due to ischemia due to retinalvasculitis and vascular occlusion [60].
Case 2In an interesting case presented by Kuchtey et al. [71], a 56-year-oldwoman with history of hypertension, coronary artery disease,Graves disease, Type 1 diabetes, hepatic and pancreatic insuffi-ciency, seizure disorder, and mitochondrial myopathy, presentedwith blurry vision, floaters, nausea, malaise and myalgias. She hadbeen bitten by mosquitoes 3 weeks prior to the development ofthese symptoms. Upon examination, her visual acuity was 20/25OD and 20/40 OS and she displayed bilateral nongranulomatousanient. She was treated with 1% prednisolone acetate hourly for1 week and her visual acuity improved to baseline. After 3 weeks,her uveitis and systemic symptoms resolved [71].
Retinal vasculitis
There have been several documented cases of occlusive retinal vas-culitis associated with confirmed WNV infection [12,60,72,73].Patients who develop vasculitis often have other associated ocularsymptoms such as chorioretinitis and optic neuritis; many of thesepatients also have a history of diabetes [12]. Development of WNVis known to accelerate the progression of diabetic retinopathy inthese individuals [12]. Patients typically present with complaints ofreduced central or peripheral vision in one or both eyes, suddenvision loss and floaters, in addition to other systemic symptoms.Ocular findings often include sheathing of the retinal vessels (mostcommonly veins), vitritis, anterior chamber cells, retinal hemor-rhages, vascular leakage on fluorescein angiography, cystoidmacular edema and optic nerve edema or atrophy [12,60,72].
In reported cases by Chan et al., ophthalmic examination inpatients with findings consistent with occlusive retinal vasculitisrevealed arterial narrowing, perivascular sheathing and vascularocclusion. One patient with a history of diabetic retinopathy and
Figure 2. Fundus photographs from a patient with confirmed West Nile virus infection. Fundus photographs of the (A) right eye and (B) left eye of the same patient as in FIGURE 1 demonstrating multiple chorioretinal lesions of various sizes that are partially atrophic and partially pigmented. Note the presence of nonproliferative diabetic retinopathy.Reproduced with permission from [66].
A B

286 Expert Rev. Ophthalmol. 3(3), (2008)
Review Priestley, Thiel & Koevary
clinically significant diabetic macular edema of the left eye alsoshowed diffuse optic nerve pallor and atrophy in both eyes, inaddition to the previously stated symptoms [60]. In anotherreported case by Garg and Jampol, a 57-year-old nondiabeticman presented with visual acuities of 20/50 OD and handmotion OS [29]. Upon fundus evaluation, he was found to havearterial attenuation, scattered intraretinal hemorrhages, diffuse cot-ton-wool spots and retinal neovascularization, which were indica-tive of severe hemorrhagic ischemic vasculitis. The patient under-went panretinal photocoagulation OU and a subsequent parsplana vitrectomy OD due to tractional retinal detachment and vit-reous hemorrhage. Vision was 20/100 OD and 20/200 OS at his18 month follow-up examination. In another case, a diabeticpatient presented with severe, permanent visual loss in his right eyeas a consequence of extensive nonperfusion macular capillary andassociated bilateral multifocal chorioretinitis and diabetic retinopa-thy [12]; owing to its unilateral involvement, it was suggested thathis vasculitis may have been the cause of his arteriolar occlusion.
Most documented cases involving the retinal vasculature wereassociated with additional retinal involvement including severe dia-betic retinopathy. Many of these patients have persistent areas ofischemia due to artery occlusion, permanent visual loss, neovascu-larization, vitreous hemorrhages and retinal detachments [72]. Asmentioned previously, diabetes has proven to be a significant riskfactor for development of severe retinal vasculitis in patientsinfected with the WNV.
Optic neuritis
Another rare, but notable, symptom of WNV is optic neuritis.Most patients that develop optic neuritis have WNM andpresent with ocular pain, blurred vision, and visual clouding or‘black fog’ in both eyes. In many of the reported cases of opticneuritis, patients described onset of ocular symptoms concomi-tantly with other systemic symptoms and had associated chori-oretinitis. Fundus examination of patients with optic neuritisrevealed bilateral pale, swollen optic nerves and in many cases afew vitreous cells [29,64,74]. An associated relative afferent papil-lary defect was noted, in addition to remarkable loss of periph-eral vision in many cases where the bilateral optic neuropathyhad an asymmetric presentation between the two eyes. Follow-up examinations revealed optic atrophy, visual acuity loss andvisual field loss [64,74].
Optic nerve involvement is seen in many conditions, high-lighting the importance of considering epidemiologic events aspart of the differential diagnosis, especially in cases wherepatients present with acute neurologic symptoms. It is worthnoting that in some cases of reported optic neuritis, patientshad previously received lumbar punctures but opening pres-sures were not reported. Thus, increased intracranial pressure,or papilledema, may have played a role in their optic nerveswelling [29]. Optic neuropathies are thought to develop sec-ondarily to primary occlusion of the posterior ciliary or retinalvessels [60].
Differential diagnosis of ophthalmic disease
Many of the ocular symptoms of WNV infection are associatedwith numerous viral, bacterial and parasitic diseases: highlightingthe importance of differential diagnosis in confirming WNV infec-tion. Patient history is an important first step in settling on a diag-nosis of WNV. Previous exposure to mosquitoes or current mos-quito bites associated with other systemic symptoms of WNVinfection, such as fever, malaise, fatigue, headache, nausea and rash,supports inclusion of WNV in the differential diagnosis.
The most common ocular finding in WNV infection is chorio-retinal lesions, which were shown in a small study to have 100%specificity and 73% sensitivity for the diagnosis of WNV infectionin patients with suspected WNV compared with WNV-negativepatients [75]. This said, of course chorioretinal lesions are notpathognomonic for WNV. Differential diagnosis of WNV chori-oretinitis includes presumed ocular histoplasmosis syndrome(POHS), idiopathic multifocal choroiditis (IMC), Vogt–Koyan-agi–Harada syndrome, Rift Valley fever, rubella, subacute scleros-ing panencephalitis, sarcoidosis, syphilis and tuberculosis[29,60,62,72]. IMC and POHS commonly occur in young popula-tions while WNV is more commonly seen in older individuals.Lesions in patients with IMC generally show hyperflourescencerather than hypofluorescence in the acute phase when observedwith FA [72]. Clinical features of POHS do not include cells in theanterior or posterior chamber, unlike WNV chorioretinitis. Addi-tionally, the lesions observed in patients with POHS are associatedwith peripapillary pigmentary changes and maculopathy [29]. Insarcoidosis, lesions are nodular granulomas, range in size from one-fourth to 1 disk diameter, and are found in clusters in the inferiorretina [29,76]. Syphilis is most easily differentiated based on its sys-temic and neurological findings. In addition, lesions associatedwith syphilis are midzonal, sectoral and are associated with perivas-culitis [29,77]. Unlike WNV lesions that appear and resolve together,the lesions in syphilis are recurrent and therefore found in differentstages of resolution. Finally, chorioretinal lesions found in tubercu-losis patients range from one-sixth to two disk sizes in diameterand have indistinct borders [29,78].
Other ocular manifestations of WNV, such as anterior uveitis,vitritis and vasculitis, have multiple causes. Some conditions thatshould be considered include tuberculosis, syphilis, sarcoidosis,collagen vascular diseases, herpes viruses, Epstein–Barr virus, Lymedisease, Rift Valley fever, Behçet disease, rubella, rickettsioses andsubacute sclerosing panencephalitis [60,73,76–78].
Long-term effects of systemic & ophthalmic disease
One of the most common symptoms reported by patients withWNF and neuroinvasive disease is extreme fatigue; others, asmentioned previously, include weakness, muscle pain, head-ache, memory problems, excessive sleepiness and problems con-centrating [79–82]. Patients recovering from WNM often sufferfrom many of these same symptoms. WNE is associated withthe highest mortality and morbidity rates compared with other

Systemic & ophthalmic manifestations of West Nile virus infection Review
www.expert-reviews.com 287
forms of the infection, with death due to disease occurring upto 1 year following diagnosis [47,82]. Some of the most commonlonger-lasting symptoms of WNE include persistent tremors,bradykinesia, parkinsonism and ataxia. Many patients requiremonths of intensive care and ventilator support, and rehabilita-tion may include intense physical, occupational and speechtherapy. The initial severity of WNE does not necessarily pre-dict neurological outcome; even patients who suffer severeencephalopathy and neurological symptoms may experiencefull recovery. In general, functional recovery following WNVtends to be more complete in younger patients [47,82].
Although rare, WNP is associated with the highest mortalityand morbidity among all WNV-infected individuals. Patients whowere successfully extubated following WNP may still experiencedyspnea and require supplemental oxygen for many years. Musclestrength usually returns after 6–8 months and may continue toimprove over time; the level of improvement following physicaland occupational therapy has been variable. Patients recoveringfrom neuroinvasive disease may continue to show motor impair-ment and compromised dexterity over time [82]. Finally, depressionhas also been a reported outcome in approximately a third ofpatients with WNV [83].
Ophthalmic manifestations associated with WNV have onlyrelatively recently been recognized, making the long-term prog-nosis in these patients difficult to predict. Most patients present-ing with chorioretinitis show improvement over time, with visualacuity returning to baseline after a few months. An interestingcase was reported of late-onset choroidal neovascularization(CNV) following a history of WNV chorioretinitis [84] in a manof 81 years of age with a history of diabetes, nonproliferativeretinopathy, hyperstension, coronary artery disease and pseudo-phaki who was diagnosed with serologically confirmed WNV
encephalitis. The patient developed bilateral mild vitritis andchorioretinal lesions characteristic of WNV. Within 4–5 months,the patient’s vision returned to baseline and chorioretinal scarsdeveloped. After 5 years, the patient presented with reducedvision to hand motion in his left eye at 60.96 cm. Fundoscopicexamination revealed the presence of a 2 disk-diameter area ofsubretinal fluid centered on the fovea OS with a subretinal hem-orrhage surrounding it. FA and ICG (FIGURE 4), as well as OCT allconfirmed the diagnosis of CNV. The patient was treated with1.25 mg of the anti-VEGF compound bevacizumab intravitreallyin his left eye. After 4 weeks, the patient’s intraretinal fluidresorbed but his visual acuity failed to improve. To date, therehave been only two other reported cases of CNV to our knowl-edge [12,29], both of whom had a history of diabetes and pre-sented with chorioretinitis. Presentation with CNV seems tooccur between 6 months and 5 years following the developmentof WNV chorioretinitis [84]. In light of this, CNV should be con-sidered as a possible late manifestation of WNV chorioretinitis,especially in patients with diabetes.
Treatment
There is no currently approved treatment for WNV. Sympto-matic patients are given supportive therapy such as intravenousfluids if they have experienced prolonged nausea, vomiting anddiarrhea, pain relievers, ventilator support as required, andtreatment for the prevention of secondary infections. Elderlypatients with functional damage as a result of WNE were foundto benefit from routine geriatric neurological rehabilitation [85].
There are a number of treatments under investigation forWNE and meningitis, including ribavirin, IFN-α2b, anti-WNVimmunoglobulin, antisense gene-targeted compounds, and
Figure 3. Fluorescein angiography from a patient with confirmed West Nile virus infection. Middle-phase fluorescein angiograms of the (A) right eye and (B) left eye of of the same patient as in FIGURE 1 show many more lesions that are observed clinically; these lesions are hypofluorescent centrally and hyperfluorescent peripherally.Reproduced with permission from [66].
A B

288 Expert Rev. Ophthalmol. 3(3), (2008)
Review Priestley, Thiel & Koevary
minocycline, a broad spectrum tetracycline antibiotic. In cases ofWNV infection with anterior chamber involvement, as men-tioned previously, topical steroids such as prednisolone have beenfound to be effective [61,63,69].
A vaccine developed by Acambis is currently in Phase IIclinical trials. The vaccine, called ChimeriVax™-WN02 is alive, attenuated recombinant vaccine produced by replacingpre-membrane and enveloped genes of an infectious yellowfever 17D virus with equivalent WNV genes [86,87]. After asingle dose, the vaccine was shown to produce a strongimmune response, characterized by the production of neutral-izing antibodies as well as CD4+ and CD8+ T cells against thevirus. In double-blind clinical trials, the immune responseoccurred in human participants within 14–28 days afterreceiving the vaccine [88].
A WNV recombinant protein vaccine is also under investiga-tion. This chimeric protein vaccine, being developed by the VaxIn-nate Corporation, is capable of eliciting both innate and adaptiveimmunity to the WNV. The vaccine was produced by fusing amodified version of bacterial flagellin to the domain III of theWNV envelope glycoprotein (E DIII) [89]. In mice, the vaccine wasshown to successfully induce protective immunity without use ofan adjuvant [89]. That said, inoculation with the WNV E DIII pro-tein along with an adjuvant was shown to induce a Th1 immuneresponse in mice, supporting its potential use in patients [90].Recently, mapping and analysis of WNV-specific monoclonalantibodies has been explored in an attempt to develop a safer,although less conventional, vaccine [91]. Vaccination of popula-tions at risk of developing severe WNV infection may reduce thenumber of fatalities due to WNV in the USA.
Figure 4. Late onset choroidal neovascularization in a patient with prior confirmed West Nile virus infection. (A) Red-free photograph of left fundus. (B) Early- and (C) late-phase fluorescence angiography shows late leakage perifoveally with hypofluorescence corresponding to hemorrhage, and late hyperfluorescence of the West Nile virus chorioretinal scars. (D) Late phase indocyanine green angiography showing foveal hyperfluorescence, and hypofluorescence of the West Nile virus chorioretinal scars.Reproduced with permission from [84].
A B
C D

Systemic & ophthalmic manifestations of West Nile virus infection Review
www.expert-reviews.com 289
Conclusion
West Nile virus infection can have serious systemic and oculareffects, both acute and chronic. Ocular symptoms may be treatedwith topical corticosteroids, but seem to be self-limited in mostcases. In rare cases, ocular involvement has led to a permanentdecrease in vision acuity and fields. Since there is currently noapproved treatment or vaccine for WNV, the CDC stronglyencourages preventative methods by communities and individualswho are at greatest risk of exposure. WNV should be included inthe differential diagnosis, especially during the months of Augustand September when infection rates are highest or if an outbreak isoccurring in the area. If WNV is confirmed or suspected as part ofthe differential diagnosis, a dilated fundus exam is extremelyimportant. Due to the high incidence of chorioretinal lesions inpatients with confirmed WNV infection, the presence of lesions ina patient with history of mosquito bites followed by fever, lethargy,malaise or rash strongly indicates WNV infection. However, otherocular symptoms such as anterior uveitis and vitritis may bepresent in the absence of lesions so a diagnosis of WNV should notbe ruled out if lesions are not present.
Expert commentary
As noted by Kramer et al., one way to improve the diagnosis ofWNV would be to use luciferase-reporting flaviviruses for thestandard antibody-mediated neutralizing assay [19]. Since the assaywould be able to identify the virus within 1 day of infection, thetime it would take to confirm a diagnosis of WNV would be short-ened considerably. The greatest challenge, however, for cliniciansstill remains the development of treatments for severe systemicneuropathological symptoms and for ocular symptoms that are notself-limiting.
Five-year view
As more becomes known about the significance of WNV in ocularpathology, it will become even more important to educate practi-tioners on the role of WNV as an etiologic factor in retinal lesions.Patient data suggest that chorioretinitis is highly specific and sensi-tive for WNV; in the coming years, this linkage will be strength-ened and confirmed. Research into the mechanism by which thispathogen causes ocular disease will also be likely to increase, aswill investigations into role of acquired immunity in virus ampli-fication. Finally, results of ongoing clinical trials may lead to thedevelopment of a clinically viable vaccine for at-risk individuals.
Current status of the field
While kits are currently available for diagnosing WNV, more sensi-tive methods for detecting the virus shortly after infection wouldbe helpful in individuals in whom differential diagnosis is difficult.More prospective ocular studies would help in solidifying the linkbetween chorioretinitis and possibly other ocular lesions, andWNV. Clearly, the greatest challenge for clinicians is the devel-opment of treatments for severe systemic neuropathologicalsymptoms and for ocular symptoms that are not self-limiting.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement withany organization or entity with a financial interest in or financialconflict with the subject matter or materials discussed in themanuscript. This includes employment, consultancies, honoraria, stockownership or options, expert testimony, grants or patents received orpending, or royalties. No writing assistance was utilized in the production of this manuscript.
Key issues
• Since its arrival in the USA, West Nile virus (WNV) has spread westward to a total of 43 states, resulting in 27,573 reported cases of infection.
• Patients with the following conditions/features were reported to have an increased risk of developing severe WNV disease: diabetes mellitus, hypertension, HIV and advanced age.
• Recent data suggest that WNV induces an antiviral state in retinal pigment epithelium cells via a mechanism that seems to involve the interferon signaling pathway.
• Transmission of WNV has been reported through the bite of infected mosquitoes, organ transplants, blood transfusions and vertical transmission through the placenta or breast milk.
• Most patients infected with WNV are asymptomatic; those that do present with symptoms usually develop WN fever and less than 1% go on to develop severe, potentially fatal neurologic disease that has been classified as West Nile meningoencephalitis, West Nile encephalitis and West Nile poliomyelitis.
• The most commonly reported ocular features of infection include: linearly arranged or scattered chorioretinal lesions, anterior uveitis, retinal vasculitis, optic neuritis and vitritis.
• Many of the ocular symptoms of WNV infection are associated with numerous viral, bacterial and parasitic diseases, highlighting the importance of differential diagnosis in confirming WNV infection.
• Functional recovery following WNV tends to be complete, though choroidal neovascularization should be considered as a possible late manifestation of WNV chorioretinitis, especially in patients with diabetes.

290 Expert Rev. Ophthalmol. 3(3), (2008)
Review Priestley, Thiel & Koevary
References
Papers of special note have been highlighted as:
• of interest
•• of considerable interest
1 Martin DA, Biggerstaff BJ, Allen B, Johnson AJ, Lanciotti RS, Roehrig JT. Use of immunoglobulin M cross-reactions in differential diagnosis of human flaviviral encephalitis infections in the United States. Clin. Diagn. Lab. Immunol. 9, 544–549 (2002).
2 Hayes EB, Sejvar JJ, Zaki SR, Lanciotti RS, Bode AV, Campbell GL. Virology, pathology, and clinical manifestations of West Nile virus disease. Emerg. Infect. Dis. 11, 1174–1179 (2005).
3 Smithburn KC, Hughes TP, Burke AW, Paul JH. A neurotropic virus isolated from the blood of a native of Uganda. Am. J. Trop. Med. 20, 471–492 (1940).
4 Nash D, Mostashari F, Fine A et al.; 1999 West Nile Outbreak Response Working Group. The outbreak of West Nile virus infection in the New York City area in 1999. N. Engl. J. Med. 344, 1807–1814 (2001).
5 Lanciotti RS, Roehrig JT, Deubel V et al. Origin of the West Nile virus responsible for an outbreak of encephalitis in the northeastern United States. Science 286, 2333–2337 (1999).
6 Petersen LR, Marfin AA. West Nile virus: a primer for the clinician. Ann. Intern. Med. 137, 173–179 (2002).
7 O’Leary DR, Marfin AA, Montgomery SP et al. The epidemic of West Nile Virus in the United States, 2002. Vector Borne Zoonotic. Dis. 4, 61–70 (2004).
8 Sampathkumar P. West Nile virus: epidemiology, clinical presentation, diagnosis, and prevention. Mayo Clin. Proc. 78, 1137–1143 (2003).
9 Batsis JA, Phy MP. West Nile virus meningitis in a chronic immunosuppressed patient with rheumatoid arthritis. Clin. Rheumatol. 24, 548–550 (2005).
10 Batalis NI, Galup L, Zaki SR, Prahlow JA. West Nile virus encephalitis. Am. J. Forensic Med. Pathol. 26, 192–196 (2005).
11 Bode AV, Sejvar JJ, Pape WJ, Campbell GL, Marfin AA. West Nile virus disease: a descriptive study of 228 patients hospitalized in a 4-county region of Colorado in 2003. Clin. Infect. Dis. 42, 1234–1240 (2006).
12 Khairallah M, Ben Yahia S, Attia S, Jelliti B, Zaouali S, Ladjimi A. Severe ischemic maculopathy in a patient with West Nile virus infection. Ophthalmic. Surg. Lasers Imaging 37, 240–242 (2006).
13 Berner YN, Lang R, Chowers MY. Outcome of West Nile fever in older adults. J. Am. Geriatr. Soc. 50, 1844–1846 (2002).
14 Chowers MY, Lang R, Nassar et al. Clinical characteristics of West Nile fever outbreak, Israel 2000. Emerg. Infect. Dis. 7, 675–678 (2001).
15 LaBeaud AD, Kile JR, Kippes C, King CH, Mandalakas AM. Exposure to West Nile virus during the 2002 epidemic in Cuyahoga County, Ohio: a comparison of pediatric and adult behaviors. Public Health Rep. 122, 356–361 (2007).
16 Liu R, Paxton WA, Choe S et al. Homozygous defect in HIV-1 coreceptor accounts for resistance of some multiply-exposed individuals to HIV-1 infection. Cell 86, 367–377 (1996).
17 Glass WG, McDermott DH, Lim JK, et al. CCR5 deficiency increases risk of symptomatic West Nile virus infection. J. Exp. Med. 203, 35–40 (2006).
18 Diamond MS, Klein RS. A genetic basis for human susceptibility to West Nile virus. Trends Microbiol. 14(7), 287–289 (2006).
19 Kramer LD, Li J, Shi PY. West Nile virus. Lancet Neurol. 6, 171–181 (2007).
20 Jeha LE, Sila CA, Lederman RJ, Prayson RA, Isada CM, Gordon SM. West Nile virus infection: a new acute paralytic illness. Neurology 61, 55–59 (2003).
21 Sejvar JJ, Haddad MB, Tierney BC et al. Neurologic manifestations and outcome of West Nile virus infection. JAMA 290, 511–515 (2003).
22 Samuel MA. Diamond MS. Pathogenesis of West Nile Virus infection: a balance between virulence, innate and adaptive immunity, and viral evasion. J. Virol. 80, 9349–9360 (2006).
23 Diamond MS, Shrestha B, Mehlhop E et al. Innate and adaptive immune responses determine protection against disseminated infection by West Nile encephalitis virus. Viral Immunol. 16, 259–278(2003).
24 Wang T, Town T, Alexopoulou L et al. Toll-like receptor 3 mediates West Nile virus entry into the brain causing lethal encephalitis. Nat. Med. 10, 1366–1373 (2004).
25 Diamond MS, Shrestha B, Marri A, Mahan D, Engle M. B cells and antibody play critical roles in the immediate defense of disseminated infection by West Nile encephalitis virus. J. Virol. 77, 2578–2586 (2003).
26 Fredericksen BL, Smith M, Katze MG, Shi PY, Gale M Jr. The host response to West Nile Virus infection limits viral spread through the activation of the interferon regulatory factor 3 pathway. J. Virol. 78, 7737–7747 (2004).
27 Cinatl J Jr, Michaelis M, Fleckenstein C et al. West Nile virus infection induces interferon signalling in human retinal pigment epithelial cells. Invest. Ophthalmol. Vis. Sci. 47, 645–651 (2006).
28 Kramer LD, Li J, Shi PY. West Nile virus. Lancet Neurol. 6, 171–181(2007).
29 Garg S, Jampol LM. Systemic and intraocular manifestations of West Nile virus infection. Surv. Ophthalmol. 50(1), 3–13. (2005).
• Detailed description of the systemic and ocular manifestations of West Nile virus (WNV) with case reports of the most commonly reported ocular diseases associated with WNV.
30 Iwamoto M, Jernigan DB, Guasch A et al. Transmission of West Nile virus from organ donor to four transplant recipients. N. Engl. J. Med. 348, 2196–2203 (2003).
• Describes the first case of WNV that was acquired through blood transfusions.
31 Centers for Disease Control and Prevention. West Nile Virus infections in organ transplant receipients – New York and Pennsylvania, August–September, 2005. MMWR Morb. Mortal. Wkly Rep. 54, 1021–1023 (2005).
32 Harrington T, Kuehnert MJ, Kamel H et al. West Nile virus infection transmitted by blood transfusion. Transfusion 43, 1018–1022 (2003).
33 Pealer LN, Marfin AA, Petersen LR et al. West Nile Virus Transmission Investigation Team. Transmission of West Nile virus through blood transfusion in the United States in 2002. N. Engl. J. Med. 349, 1236–1245 (2003).
34 Alpert SG, Fergerson J, Noel LP. Intrauterine West Nile virus: ocular and systemic findings. Am. J. Ophthalmol. 136, 733–735 (2003).
35 O’Leary DR, Kuhn S, Kniss KL et al. Birth outcomes following West Nile Virus infection of pregnant women in the United States: 2003–2004. Pediatrics 117, e537–e545 (2006).

Systemic & ophthalmic manifestations of West Nile virus infection Review
www.expert-reviews.com 291
36 Fradin MS, Day JF. Comparative efficacy of insect repellants against mosquito bites. N. Engl. J. Med. 347, 13–18 (2002).
37 Centers for Disease Control and Prevention (CDC). West Nile virus activity – United States, 2006. MMWR Morb. Mortal. Wkly Rep. 56, 556–559 (2007).
38 Hayes EB, Gubler DJ. West Nile virus: epidemiology and clinical features of an emerging epidemic in the United States. Annu. Rev. Med. 57, 181–194 (2006).
39 Peterson LR, Marfin AA, Gubler DJ. West Nile Virus. JAMA 290, 524–528 (2003).
40 Nasci RS, Savage HM, White DJ et al. West Nile virus in overwintering Culex mosquitoes, New York City, 2000. Emerg. Infect. Dis. 7, 742–744 (2001).
41 Rimon A, Straussberg R, Amir J. West Nile encephalitis mimicking herpes encephalitis. Pediatr. Neurol. 35, 62–64 (2006).
42 Francisco AM, Glaser C, Frykman E et al. 2004 California pediatric West Nile virus case series. Pediatr. Infect. Dis. J. 25, 81–84 (2006).
43 Tilley PA, Fox JD, Jayaraman GC, Preiksaitis JK. Maculopapular rash and tremor are associated with West Nile fever and neurological syndromes. J. Neurol. Neurosurg. Psychiatry 78, 529–531 (2007).
44 Jesitus, John. West Nile virus skin symptoms documented. Dermatol. Times 18, 22 (2005).
45 Watson JT, Pertel PE, Jones RC et al. Clinical characteristics and functional outcomes of West Nile Fever. Ann. Intern. Med. 141, 360–365 (2004).
46 Klee AL, Maidin B, Edwin B et al. Long-term prognosis for clinical West Nile virus infection. Emerg. Infect. Dis. 10, 1405–1411 (2004).
47 Sejvar JJ. The long-term outcomes of human West Nile virus infection. Clin. Infect. Dis. 44, 1617–1624 (2007).
• Good review of the long-term systemic outcomes of WNV infection.
48 Rosas H, Wippold FJ II. West Nile virus: case report with MR imaging findings. Am. J. Neuroradiol. 24, 1376–1378 (2003).
49 Sejvar JJ, Bode AV, Marfin AA et al. West Nile virus-associated flaccid paralysis. Emerg. Infect. Dis. 11, 1021–1027 (2005).
50 Sejvar JJ, Bode AV, Marfin AA et al. West Nile virus-associated flaccid paralysis outcome. Emerg. Infect. Dis. 12, 514–516 (2006).
51 Leis AA, Stokic DS, Webb RM, Slavinski SA, Fratkin J. Clinical spectrum of muscle weakness in human West Nile virus infection. Ann. Neurol. 28, 302–308 (2003).
52 Li J, Loeb JA, Shy ME et al. Asymmetric flaccid paralysis: a neuromuscular presentation of West Nile virus infection. Ann. Neurol. 53, 703–710 (2003).
53 Schafernak KT, Bigio EH. West Nile virus encephalomyelitis with polio-like paralysis and nigral degeneration. Can. J. Neurol. Sci. 33, 407–410 (2006).
54 Ahmed S, Libman R, Wesson K, Ahmed F, Einberg K. Guillain-Barré syndrome: an unusual presentation of West Nile virus infection. Neurology 55, 144–146. (2000).
55 Cao N, Ranganathan C, Kupsy W, Li J. Recovery and prognosticators of paralysis in West Nile virus infection. J. Neurol. Sci. 236, 73–80 (2005).
56 Cunha BA, Eisenstein LE, Wirkowski E, Klein NH, Johnson DH. West Nile encephalitis relapse presenting with abducens and facial nerve palsies. Am. J. Med. 119, e1–e2 (2006).
57 Cunha BA, Thermidor M, Mohan S, Ly H. West Nile viral encephalitis mimicking hepatic encephalopathy. Heart Lung 34, 72–75 (2005).
58 Jamison SC, Michaels SR, Ratard R, Sweet JM, Deboisblanc BP. A 41-year-old HIV-positive man with acute onset of quadriplegia after West Nile virus infection. South Med. J. 100, 1051–1053(2007).
59 Paddock CD, Nicholson WL, Bhatnagar J et al. Fatal hemorrhagic fever caused by West Nile virus in the United States. Clin. Infect. Dis. 42, 1527–1535 (2006).
60 Chan CK, Limstrom SA, Tarasewicz DG, Lin SG. Ocular features of west nile virus infection in North America: a study of 14 eyes. Ophthalmology 113, 1539–1546 (2006).
• Illustrates a variety of reported cases of WNV infection with ocular manifestations.
61 Bakri SJ, Kaiser PK. Ocular manifestations of West Nile virus. Curr. Opin. Ophthalmol. 15, 537–540 (2004).
62 Khairallah M, Ben Yahia S, Ladjimi A et al. Chorioretinal involvement in patients with West Nile virus infection. Ophthalmology 111, 2065–2070 (2004).
• Prospective study of the ocular symptoms of WNV.
63 Hershberger VS, Augsburger JJ, Hutchins RK, Miller SA, Horwitz JA, Bergmann M. Chorioretinal lesions in nonfatal cases of West Nile virus infection. Ophthalmology 110, 1732–1736 (2003).
64 Anninger W, Lubow M. Visual loss with West Nile virus infection: a wider spectrum of a ‘new’ disease. Clin. Infect. Dis. 38, e55–e56. (2004).
65 Myers JP, Leveque TK, Johnson MW. Extensive chorioretinitis and severe vision loss associated with West Nile virus meningoencephalitis. Arch. Ophthalmol. 123, 1754–1756 (2005).
66 Khairallah M, Ben Yahia S, Attia S et al. Indocyanine green angiographic features in multifocal chorioretinitis associated with West Nile virus infection. Retina 26, 358–359 (2006).
67 Khairallah M, Ben Yahia S, Attia S, Zaouali S, Ladjimi A, Messaoud R. Linear pattern of West Nile virus-associated chorioretinitis is related to retinal nerve fibres organization. Eye 21, 952–955 (2007).
• Postulates a new theory that accounts for the characteristic linear pattern of chorioretinitis seen in WNV patients.
68 Khairallah M, Ben Yahia S, Letaief M et al. A prospective evaluation of factors associated with chorioretinitis in patients with West Nile virus infection. Ocul. Immunol. Inflamm. 15, 435–439 (2007).
69 Bains HS, Jampol LM, Caughron MC, Parnell JR. Vitritis and chorioretinitis in a patient with West Nile virus infection. Arch. Ophthalmol. 121, 205–207. (2003).
70 Yim R, Posfay-Barbe KM, Nolt D, Fatula G, Wald ER. Spectrum of clinical manifestations of West Nile virus infection in children. Pediatrics 114, 1673–1675 (2004).
71 Kuchtey RW, Kosmorsky GS, Martin D, Lee MS. Uveitis associated with West Nile virus infection. Arch. Ophthalmol. 121, 1648–1649 (2003).
72 Teitelbaum BA, Newman TL, Tresley DJ. Occlusive retinal vasculitis in a patient with West Nile virus. Clin. Exp. Optom. 90, 463–467 (2007).
73 Kaiser PK, Lee MS, Martin DA. Occlusive vasculitis in a patient with concomitant West Nile virus infection. Am. J. Ophthalmol. 136, 928–930 (2003).
74 Gilad R, Lampl Y, Sadeh M, Paul M, Dan M. Optic neuritis complicating west nile virus meningitis in a young adult. Infection 31, 55–56 (2003).
75 Abroug F, Ouanes-Besbes L, Letaief M et al. A cluster study of predictors of severe West Nile virus infection. Mayo Clin. Proc. 81, 12–16 (2006).
• Underscores the significance of multifocal chorioretinitis in diagnosing WNV with specificity and sensitivity.

292 Expert Rev. Ophthalmol. 3(3), (2008)
Review Priestley, Thiel & Koevary
76 Wolfensberger TJ, Herbort CP. Indocyanine green angiographic features in ocular sarcoidosis. Ophthalmology 106, 285–289 (1999).
77 Gass JD, Braunstein RA, Chenoweth RG. Acute syphilitic placoid chorioretinitis. Ophthalmology 97, 1288–1297 (1990).
78 Thompson MJ, Albert DM. Ocular tuberculosis. Arch. Ophthalmol. 123, 844–849 (2005).
79 Rao N, Char D, Gnatz S. Rehabilitation outcomes of 5 patients with severe West Nile virus infection: a case series. Arch. Phys. Med. Rehabil. 86, 449–452 (2005).
80 Patnaik JL, Harmon H, Vogt RL. Follow-up of 2003 human West Nile virus infections, Denver, Colorado. Emerg. Infect. Dis. 12, 1129–1131.(2006).
81 Hayes EB, O’Leary DR. West Nile virus infection: a pediatric perspective. Pediatric 113, 1375–1381 (2004).
82 Carson PJ, Konewko P, Wold KS et al. Long-term clinical and neuropsychological outcomes of West Nile virus infection. Clin. Infect. Dis. 43, 723–730 (2006).
83 Murray KO, Resnick M, Miller V. Depression after infection with West Nile virus. Emerg. Infect. Dis. 13, 479–481(2007).
84 Seth RK, Stoessel KM, Adelman RA. Choroidal neovascularization associated with West Nile Virus chorioretinitis. Semin. Ophthalmol. 22, 81–84 (2007).
• Highlights the significance of possible long-term effects of ocular manifestations of WNV and describes a patient who exhibited late-onset choroidal neovascularization.
85 Berner Y, Feldman J, Spigel D, Chowers M, Finckeltov B. Rehabilitation of West Nile fever (WNF) encephalitis in elderly. Arch. Gerontol. Geriatr. 41, 15–21 (2005).
86 Arroyo J, Miller C, Catalan J et al. ChimeriVax – West Nile virus live-attenuated vaccine: preclinical evaluation of safety, immunogenicity, and efficacy. J. Virol. 78, 12497–12507 (2004).
87 Hall RA, Khromykh AA. ChimeriVax – West Nile vaccine. Curr. Opin. Mol. Ther. 9, 498–504 (2007).
88 Monath TP, Liu J, Kanesa-Thasan N et al. A live, attenuated recombinant West Nile virus vaccine. Proc. Natl Acad. Sci. USA 103, 6694–6699 (2006).
89 McDonald WF, Huleatt JW, Foellmer HG et al. A West Nile virus recombinant protein vaccine that coactivates innate and adaptive immunity. J. Infect. Dis. 195, 1607–1617 (2007).
90 Chu JH, Chiang CC, Ng ML. Immunization of flavivirus West Nile recombinant envelope domain III protein induced specific immune response and protection against West Nile virus infection. J. Immunol. 178, 2699–2705 (2007).
91 Throsby M, Ter Meulen J, Geuijen C, Goudsmit J, de Kruif J. Mapping and analysis of West Nile virus-specific monoclonal antibodies: prospects for vaccine development. Expert Rev. Vaccines 6(2), 183–191 (2007).
Websites
101 Centers for Disease Control and Prevention. West Nile Virus: Statistics, Surveillance and Control. www.cdc.gov/ncidod/dvbid/westnile/surv&control.htm
102 Centers for Disease Control and Prevention. Epidemic/Epizootic West Nile Virus in the United States: Guidelines for Surveillance, Prevention, and Control. (3rd Revision). (2003). www.cdc.gov/ncidod/dvbid/westnile/resources/wnv-guidelines-aug-2003.pdf
103 Centers for Disease Control and Prevention (CDC). West Nile Virus, Pregnancy and Breastfeeding. www.cdc.gov/ncidod/dvbid/westnile/qa/breastfeeding.htm
104 FDA News. FDA Clears First Test for West Nile Virus. July 9, 2003. www.fda.gov/bbs/topics/NEWS/2003/NEW00920.html
105 FDA News. FDA Approves First Fully Automated Test to Screen for West Nile Virus in Blood and Tissue Donors. www.fda.gov/bbs/topics/NEWS/2007NEW01578.html (2 February 2007)
106 FDA News. FDA Approves Second West Nile Virus Screening Test for Donated Blood and Organs. August 28, 2007. www.fda.gov/bbs/topics/NEWS/2007/NEW01691.html
Affiliations
• Yos Priestley, BSDepartment of Biomedical Sciences and Disease, New England College of Optometry, 424 Beacon Street, Boston, MA 02115, USATel.: +1 617 587 [email protected]
• Marcia Thiel, BSDepartment of Biomedical Sciences and Disease, New England College of Optometry, 424 Beacon Street, Boston, MA 02115, USATel.: +1 617 587 [email protected]
• Steven B Koevary, PhDDepartment of Biomedical Sciences and Disease, New England College of Optometry, 424 Beacon Street, Boston, MA 02115, USATel.: +1 617 587 5614Fax: +1 617 587 [email protected]


















![ICD-10 Clinical Close-up...• 250.53-Diabetes with ophthalmic manifestations, type I [juvenile type], uncontrolled . ICD-10-CM Codes . Examples • E10.311 =Type 1 diabetes mellitus](https://img.dokumen.tips/doc/110x75/5f4fcde205202b5e6a605343/icd-10-clinical-close-up-a-25053-diabetes-with-ophthalmic-manifestations.jpg)