Embed Size (px)
Citation preview

1037
Synthetic Bioabsorbable Barrierfor Regeneration in HumanPeriodontal DefectsJ. Caton,* G. Greenstein/ and U. Zappa*
Guided tissue regeneration (GTR) may result in the formation of new bone, cemen-
tum, and periodontal ligament. The purpose of this study was to assess the efficacy of a
resorbable synthetic material, which has been used extensively in general surgery forwound support, to promote GTR. Forty healthy patients with adult Periodontitis, eachhaving a Class II furcation defect, participated in the study. After initial therapy, mu-
coperiosteal flaps were elevated and furcations debrided with hand and rotary instruments.In 20 patients the molar Class II furcation defects were treated with a GTR procedureusing the resorbable synthetic material (experimental), and 20 patients received a mu-
coperiosteal flap debridement procedure without barrier placement (control). Probingdepth and attachment level measurements were taken immediately before surgery, at 6weeks, and 2, 3, 4, 5, and 6 months after surgery. All areas healed uneventfully. Com-parison of clinical attachment level measurements indicated significantly greater gain ofattachment at sites receiving barriers. Fifteen of 20 Class II furcations in the syntheticbarrier group, but only one of 20 in the control group, were converted to Class I defects.Barriers were still clinically detectable at 4 weeks, but were absent at 6 weeks. Thesynthetic barriers enhanced gain of clinical attachment in human Class II furcation de-fects. J Periodontol 1994; 65:1037-1045.
Key Words: Membranes, artificial; membranes, barrier; furcation/therapy; guided tissueregeneration; clinical trials; periodontal attachment.
The main objective of traditional periodontal treatment isto resolve the inflammatory lesion in the periodontal tis-sues. This therapy involves the elimination of plaque andcalculus from tooth surfaces, either with scaling and rootplaning alone or combined with periodontal surgery. Withproper postoperative maintenance care, periodontal therapyresults in resolution of gingival inflammation and in thearrest of disease progression.12
A contemporary goal of periodontal therapy, however,has become the regeneration of the lost attachment appa-ratus. This includes the formation of new cementum, peri-odontal ligament, and alveolar bone. Studies in animals andhumans have demonstrated that it is possible to promoteregeneration of a new connective tissue attachment to de-nuded root surfaces by selectively favoring regrowth of theperiodontal ligament tissue.3 4 This technique, guided tissueregeneration (GTR), is accomplished by placing a barrierbetween the gingiva and the root surface which preventsthe gingival tissues from reaching contact with the root dur-
* Department of Periodontology, Eastman Dental Center, Rochester, ny.'Private practice, Freehold, nj.*School of Dental Medicine, University of Zürich, Zürich, Switzerland.
ing healing and gives preference to cells originating fromthe periodontal ligament to repopulate the root surface.
Nonresorbable barriers prevented epithelial migration andpromoted new connective tissue attachment, however, theynecessitated secondary surgical procedures for removal, re-
ducing their practicality during routine patient management.For these reasons, an absorbable barrier would appear more
practical. A bioabsorbable material should first permit se-
lective repopulation of the exposed root surface by peri-odontal ligament cells, and when this process is complete,be absorbed.
Recently, a resorbable synthetic material8 was success-
fully used to enhance new connective tissue attachment indogs5 and monkeys.6 Others employed it in conjunctionwith bone grafts to promote regeneration in human peri-odontal defects.7 This resorbable synthetic barrier also fa-cilitated a gain of clinical attachment in humans.8
Long-term follow-up of periodontal therapy indicatesthat the majority of periodontal lesions will respond wellto treatment. An exception are lesions in multi-rooted teeththat have advanced into the furcation area between the
§Vicryl, Ethicon, Inc., Somerville, nj.
1038 BIOABSORBABLE MEMBRANES AND REGENERATIONJ Periodontol
November 1994
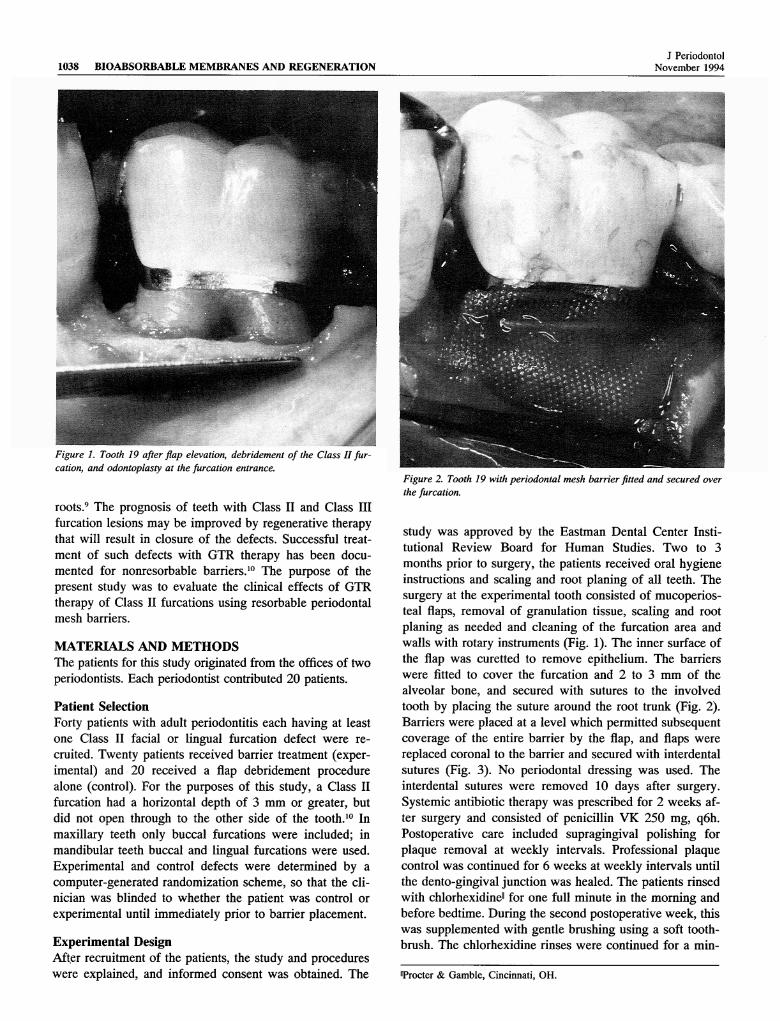
Figure 1. Tooth 19 after flap elevation, debridement of the Class II fur-cation, and odontoplasty at the furcation entrance.
roots.9 The prognosis of teeth with Class II and Class IIIfurcation lesions may be improved by regenerative therapythat will result in closure of the defects. Successful treat-ment of such defects with GTR therapy has been docu-mented for nonresorbable barriers.10 The purpose of thepresent study was to evaluate the clinical effects of GTRtherapy of Class II furcations using resorbable periodontalmesh barriers.
MATERIALS AND METHODSThe patients for this study originated from the offices of twoperiodontists. Each periodontist contributed 20 patients.Patient SelectionForty patients with adult Periodontitis each having at leastone Class II facial or lingual furcation defect were re-cruited. Twenty patients received barrier treatment (exper-imental) and 20 received a flap debridement procedurealone (control). For the purposes of this study, a Class IIfurcation had a horizontal depth of 3 mm or greater, butdid not open through to the other side of the tooth.10 Inmaxillary teeth only buccal furcations were included; inmandibular teeth buccal and lingual furcations were used.Experimental and control defects were determined by a
computer-generated randomization scheme, so that the cli-nician was blinded to whether the patient was control or
experimental until immediately prior to barrier placement.Experimental DesignAfter recruitment of the patients, the study and procedureswere explained, and informed consent was obtained. The
Figure 2. Tooth 19 with periodontal mesh barrier fitted and secured over
the furcation.
study was approved by the Eastman Dental Center Insti-tutional Review Board for Human Studies. Two to 3months prior to surgery, the patients received oral hygieneinstructions and scaling and root planing of all teeth. Thesurgery at the experimental tooth consisted of mucoperios-teal flaps, removal of granulation tissue, scaling and root
planing as needed and cleaning of the furcation area andwalls with rotary instruments (Fig. 1). The inner surface ofthe flap was curetted to remove epithelium. The barrierswere fitted to cover the furcation and 2 to 3 mm of thealveolar bone, and secured with sutures to the involvedtooth by placing the suture around the root trunk (Fig. 2).Barriers were placed at a level which permitted subsequentcoverage of the entire barrier by the flap, and flaps were
replaced coronal to the barrier and secured with interdentalsutures (Fig. 3). No periodontal dressing was used. Theinterdental sutures were removed 10 days after surgery.Systemic antibiotic therapy was prescribed for 2 weeks af-ter surgery and consisted of penicillin VK 250 mg, q6h.Postoperative care included supragingival polishing forplaque removal at weekly intervals. Professional plaquecontrol was continued for 6 weeks at weekly intervals untilthe dento-gingival junction was healed. The patients rinsedwith Chlorhexidine11 for one full minute in the morning andbefore bedtime. During the second postoperative week, thiswas supplemented with gentle brushing using a soft tooth-brush. The Chlorhexidine rinses were continued for a min-
"Procter & Gamble, Cincinnati, OH.

Figure 3. Tooth 19 after flap closure and suturing with interdental sutures.
imum of 6 weeks, and the patients continued normal me-
chanical plaque control for the remainder of the study.
Control ProcedureIdentical surgical and maintenance procedures were per-formed at control sites, with the exception that barriers were
not placed.
MeasurementsMeasurements were taken immediately prior to surgery andat 6 weeks and 2, 3, 4, 5 and 6 months following surgery.These measurements included plaque, visual signs of in-flammation, probing depth, recession, clinical attachmentlevel, and horizontal and vertical furcation depths. A 6-month evaluation period was chosen because several stud-ies showed that dimensional alteration of the periodontaltissues resulting from surgical therapy occurs within 6months (Fig. 4).U13
Pre- and Postsurgical Measurements1. Visual signs of inflammation: The presence or absence
of color change at the gingival margin was evaluated at thefurcation.
2. Plaque: The presence or absence of plaque at gingivalmargin was assessed at the furcation.
3. Bleeding after probing was assessed as presence orabsence of bleeding within 30 seconds after measuring theprobing depth.14
4. Probing depth was measured from the gingival margin
Figure 4. Tooth 19 at 6 months after the GTR operation.
to the bottom of the pocket at the furcation with a peri-odontal probe.
5. Gingival margin location: The distance between thegingival margin and the cemento-enamel junction (CEJ)measured with a periodontal probe at the furcation.
6. Clinical attachment level was calculated using the dis-tance between gingival margin and the CEJ, and probingdepth at the furcation.
7. Furcation involvement was measured at the midfur-cation site as horizontal and vertical defect depth.
The vertical defect depth was measured as the distancefrom the furcation roof to the bottom of the pocket. Thehorizontal defect depth was measured using the buccal/Iin-gual surface of the roots as the reference level. All meas-
urements were made at the middle of the furcation.Probing measurements were made using a periodontal
probe calibrated in 1 mm increments and an end diameterof 0.4 mm. Measurements falling between markings were
rounded to the next higher millimeter.
Statistical MethodsSince all patients were enrolled under the same protocol,and since there were no demographic or clinical observa-tions that contraindicated pooling over the study centers,the data from both offices were combined and presented as
a comparison of control and experimental groups of 20 mo-lars each.
All analyses of differences between groups were two-sided and employed a 0.05 level of significance. Compar-ison of demographic distributions employed either analysisof variance or a chi square test. Consistency between the

1040 BIOABSORBABLE MEMBRANES AND REGENERATIONJ Periodontol
November 1994
Table 1. Patients Included in the Study Table 2. Tooth Types Included in the StudyOffice 1 Office 2
Sex Control Experimental Control Experimental Total
FemaleMaleTotals
46
10
73
10
55
10
64
10
221840
two study centers was demonstrated by means of a repeatedmeasures analysis of variance in the case of ordinal data(parameters 1, 2, 3) and log-linear model techniques in thecase of nominal data (parameters 4, 5, 6, 7). Similarly,group comparisons at each examination used either r-test or
Fisher's exact test. Missing data were encountered for one
patient in one experimental group at 4 months and one pa-tient in the control group at 5 months. This was ignoredsince there was no evidence that the missing data were re-
lated to either the periodontal disease process or treatmentdifferences. Analyses'were run with and without these pa-tients with no apparent differences in the results.
Measurement ErrorIntraexaminer and interexaminer errors were determined forthe probings using repeated measurements made 1 hourapart on 10 patients. The following summarizes the resultsof these determinations for intraexaminer errors: 0 differ-ence
-
78%; + 1mm- 20%; ± 2 mm-
2%. For inter-examiner errors the values were: 0 difference 72%; ± 1mm
—
26%; ± 2 mm—
2%. These errors were consideredwithin reason for the purposes of this study.
RESULTS
PatientsTwenty patients were available from each of two offices(11 female and 9 male patients in each office). The mean
age in the patients of the first office was 55.1 (± 3.25)years in the control group and 48.5 (± 3.25) years in theexperimental group. In the second office the mean age inthe control group was 49.3 (± 3.25) years and in the ex-
perimental group 46.7 (± 3.25) years.The number of teeth treated and evaluated are shown in
Table 1. Of the total of 40 teeth included in the study 13were maxillary molars, and 27 were mandibular molars(Table 2).
The percentage of sites with visual signs of inflammationwas the same for both control and experimental groups 6weeks after surgery (Fig. 5). At all other time points, thepercentage of sites with visual signs of inflammation was
numerically higher at control sites as compared to the ex-
perimental sites. These differences were statistically signif-icant at months 2, 3, 4, and 6 after surgery.
The percentage of sites with supragingival plaque at thegingival margin was the same in control and experimentalgroups prior to surgery at month 0. At all time points aftersurgery, the percentage of sites with plaque was numeri-
Office Office 2
Tooth Control Experimental Control Experimental Total
2 03 1
14 015 017 018 119 330 431 1Totals 10
111o01312
10
010212130
10
2 30 30 14 60 11 50 71 92 5
10 40
Percentage of sites with visual signsof inflammation
(Mean, SE)100^
Office 1 Office 2 Combined
0 1.5 > 3 4
MonthFigure 5. Percentage of sites with visual signs of inflammation at thesurgical sites, shown for each examination.
cally greater in the control group (Fig. 6). These differenceswere statistically significant at months 2 and 3 after surgery(P <0.05).
Prior to surgery, bleeding on probing occurred at controland experimental sites in virtually the same percentage ofsites (Fig. 7). These values were reduced to half at 6 weeksafter surgery in both groups. Thereafter the percentage ofsites with bleeding on probing was markedly lower at ex-
perimental sites than at control sites. These differences were
statistically significant at months 2, 3, 4, and 6 aftersurgery.
Probing depth prior to surgery was significantly (P<0.05) greater in experimental sites (7.3 mm) as comparedto control sites (6.5 mm) (Fig. 8). Six weeks after surgery,these values were reversed, and control sites (6.2 mm) were

Volume 65Number 11 caton, greenstein, zappa 1041
Percentage of sites with supragingival plaque(Mean,SE)
Office 1 Office 2 Combined
MonthFigure 6. Percentage of sites with supragingival plaque at the surgicalsites, shown for each examination.
significantly deeper than experimental sites (4.0 mm).These differences were maintained at all time points aftersurgery (P <0.001).
At most sites and time points, the gingival margin lo-cation was apical to the CEJ. The results are expressed as
mean recession in Figure 9. Recession was greater at con-
trol sites at all time points. Also, recession was greater atall postsurgical time points as compared to presurgicalmeasurements.
The mean loss of attachment prior to surgery was similarat control and experimental sites (7.9 mm) (Fig. 10). At allpostsurgical time points loss of attachment was significantlylower in experimental sites (P <0.002), as compared tobaseline and to control sites.
Presurgically, the mean horizontal furcation depth was
significantly (P = 0.004) greater in experimental sites (4.0mm) compared to control sites (3.2 mm) (Fig. 11). At 6weeks after surgery the experimental sites were numericallyless deep than the controls, but this effect was not signifi-cant. At later time points (2 to 6 months) experimental siteswere significantly less deep than control sites (P <0.03).
The mean vertical depth of furcations presurgically was
higher in experimental sites (5.3 mm) compared to controlsites (4.5 mm) (Fig. 12) and this difference was statisticallysignificant (P = 0.02). However, at all postsurgical timepoints, the vertical furcation depth was significantly less atexperimental sites (P <0.01) than in control sites.
Initially, all sites had Class II involvement. However, 6
Percentage of sites with bleeding on probing(Mean, SE)
ro.*—«a E
100^
80
60
40-I CL lu 20
2 20
I 40
60-
80-
100
Office 1 Office 2 Combined
0 1.5
I2
4
MonthFigure 7. Percentage of sites with bleeding after probing at surgical sites,shown for each examination.
Probing depth at the furcations(Mean, SE)
mm7
c 6E 5
"fe8-3
LU 21
—
01
ö 234567
£=Oü
Office 1Il Office 2 Combined
0 1.5 3 4 5
MonthFigure 8. Mean probing depth at surgical sites at each examination.
weeks after surgery, 40% of the experimental sites had pro-gressed to Class I and this figure increased to 75% at 6months. At all postsurgical time points the percentage ofClass I furcations was significantly higher in experimentalsites (P <0.001). At control sites the percentage of Class Ifurcations remained zero at 2 and 3 months, and reachedonly 5 to 6% of the sites at months 4 to 6 (Fig. 13).

1042 BIOABSORBABLE MEMBRANES AND REGENERATIONJ Periodontol
November 1994
egeCDEi—CD -
LU
erOO
Recession (mm)(Mean, SE)
Office 1H Office 2 Combined
i i
k i
Ti
li
LIO
0 1.5 2
HT6
MonthFigure 9. Mean recession at surgical sites at each examination.
Horizontal depth of furcation involvement(Mean, SE)
mm
4cd
-4—'
CD JECD 2Q_X
LU -I
-0
Ö 1
2Ü
3
4
ft Office 1 Office 2 Combined
ffl m
,
-
riii rhl
"I I I I 0 1.5 2 3 4
" 6
MonthFigure 11. Mean horizontal depth of furcation involvement at surgicalsites, shown for each examination.
Attachment loss at the furcations(Mean, SE)
mm8
le<B 5 c 4CD oQ. ° o
1
—
01
II:§ 4O 5
67j8
îirhl
Office 1 Office 2
Combined
1.5 3
ib A
5 6
MonthFigure 10. Mean probing attachment loss at surgical sites at each ex-
amination.
Vertical depth of furcation involvement(Mean, SE)
mm
5
4co
A—»
CD JE 2 -
LU
2 1-*—»
§ 2^O
3·- 4
5
Office 1M Office 2 Combined
tàl
IT
I0 1.5
3
Month4 5
" 6
Figure 12. Mean vertical depth offurcation involvement at surgical sitesat each examination.

Volume 65Number 11 CATON, GREENSTEIN, ZAPPA 1043
Percentage of patients with class I furcations(Mean, SE)
100-,
Sc: E -
CL
LU
80-
60
40J
20
ÍZoO
-
0
20
40
60
80
100
Office 1 Office 2 Combined
o 1.5 5 6
MonthFigure 13. Percentage of patients with Class I furcation involvement at
surgical sites, shown for each examination.
DISCUSSIONThe purpose of the present study was to evaluate the clin-ical healing effects after treatment of Class II furcation de-fects using resorbable periodontal mesh barriers. The most
important observation of this study was that at 6 monthsafter the GTR surgery, 75% of the sites treated with theperiodontal mesh barriers improved from a Class II to ClassI furcation while only 5% of the control sites showed thesame improvement. From these results, it appears that theprinciples of guided tissue regeneration also work whenresorbable barriers are used.
The changes in clinical parameters at experimental andcontrol teeth were significantly different at postsurgicaltime points. Experimental barrier-treated sites showed lesssupragingival plaque, visual signs of inflammation, andbleeding on probing. Probing depth, recession, loss of at-
tachment, and vertical and horizontal depth of the furca-tions were significantly less in the experimental sites. Thisconfirms the notion that conversion of Class II to Class Ifurcation involvement improves the clinical periodontalstatus, probably by facilitating oral hygiene and prophylac-tic measures at these sites. It therefore appears that the GTRprocedures offer a distinct advantage for the patient as com-
pared to conventional surgical treatment alone.The results obtained using a resorbable periodontal mesh
in the present study compare favorably with the results ofother studies which evaluated clinical results after usage ofnonresorbable barriers. Pontonero10 evaluated 21 patientsfor 6 months. Postsurgically, plaque levels at control and
test sites were not different, while the GI measurementswere lower at experimental sites, as were the number ofsites bleeding on probing. As in the present study, probingdepth, was more reduced in experimental sites which re-
ceived a barrier. Furthermore, vertical and horizontal prob-ing attachment levels in the furcation of experimental siteswere significantly improved compared to control sites.These improvements achieved with nonresorbable barriersare similar to the results obtained in the present study usingthe resorbable periodontal mesh.
Other authors have shown that new attachment can beformed to previously exposed root surfaces. These authorsused nonresorbable barriers1516 or treated the root surfaceswith citric acid.17 The clinical results from the present studyare consistent with the conclusion of the previous studies,namely that a biologically resorbable barrier can also leadto formation of a new attachment apparatus by the processof GTR.18 21 Efficacy studies in monkeys that evaluated theresorbable periodontal mesh support this conclusion.6
The clinical effects of GTR therapy using resorbableperiodontal mesh include reduction of furcation involve-ment from Class II to Class I. These changes reflect reduc-tion of horizontal interradicular probe penetration. The rea-
son for this effect can either be formation of newconnective tissue attachment or of a long junctional epithe-lium between the root surfaces and the newly formed densesoft tissues.9-22 Even if the reduction of involvement is dueto a long junctional epithelium, the patients seem to havebenefited from the GTR therapy. All indices measuring ef-fect of oral hygiene measures were significantly lower at
experimental sites, suggesting that the patients' hygiene ef-forts were more successful at the GTR-treated sites. In ad-dition, it is known that a long junctional epithelium is ofvalue, because the seal between root surface and soft tissuesprovided by it may be as resistant and durable as the den-togingival structures present prior to the onset ofPeriodontitis.23-24
The barriers used for GTR should disappear at the endof wound healing or at a point during wound healing whenthe critical cellular events have occurred. From this pointof view bioabsorbable polymers may be best suited for pro-viding an appropriate barrier effect for a limited period oftime, without imposing additional strain on patient and ther-apist. Considerable recent evidence suggests that resorbablebarriers are effective in promoting new attachment. Animalstudies6-25 30 showed that the incidence of new attachmentformation after use of these materials is 2 to 3 times higherthan at control sites. These animal studies used observationperiods of 3 months or less. In humans, several reportsdocumented clinical attachment gain at barrier treatedsites.3135 One report documented histologically in humansthe formation of new cementum, bone and periodontalligament.36
Biodegradation of barriers could introduce problemssuch as local inflammatory responses.35-37 In addition, thetiming of degradation of the barrier relative to completion

1044 BIOABSORBABLE MEMBRANES AND REGENERATIONJ Periodontol
November 1994
of periodontal regeneration is probably crucial.35 36 The bi-odegradable material should first permit selective repop-ulation of the exposed root surface by periodontal ligamentcells, and degrade only when this process is complete. Po-lyglactin 910 was reported to degrade within 30 to 50days,5-38 and these times were confirmed by the results ofthe present study, where the barriers had disappeared at 4to 6 weeks.
The in vivo absorption of synthetic polymers such as
polyglactin 910 is easy to control, because degradation isnot achieved by enzymes, but by hydrolyzation of esterbonds.39"41 In contrast, resorbable collagen membranes re-
quire enzymatic processes, and this seems to limit the bar-rier function due to colonization with epithelial andfibroblast cells.32 Normally, apical migration of the epithe-lium occurs within 2 weeks after surgery,37-42 and root ré-
sorption and bone ankylosis become active 2 to 3 weekspostoperatively. Therefore it appears necessary that the bar-rier structure be maintained to protect the root surface forat least 3 to 4 weeks. The resorbable periodontal mesh usedin our study seems to maintain its structure for this timeperiod.6 Thereafter, it is absorbed within 60 days withoutany evidence of chronic inflammatory reactions.38
The present study showed that the use of resorbable peri-odontal mesh barriers for GTR therapy at Class II furca-tions resulted in significant reduction of furcation involve-ment. The improvements are comparable with the resultsobtained with nonresorbable barriers. Therefore it appearsthat a patient with Class II furcation involvements benefitsfrom barrier treatment, because results are superior to con-
ventional treatment without barriers. The use of resorbablebarriers provide the patient with the additional advantagethat no second surgical procedure is necessary for removalof the barrier.
AcknowledgmentThis study was supported by Johnson & Johnson, Inc.,Skillman, NJ.
REFERENCES1. Badersten A. Non-surgical periodontal therapy [Thesis], Department
of Periodontology, Faculty of Odontology, University of Lund,Malmö, Sweden, 1984.
2. Westfeit E. Effect of periodontal therapy [Thesis]. Department ofPeriodontology, Faculty of Odontology, University of Gothenburg,Sweden, 1984.
3. Nyman S, Lindhe J, Karring T. Reattachment-
new attachment. In:Lindhe J, ed. Textbook of Clinical Periodontology. Copenhagen:Munksgaard; 1983; 409^129.
4. Gottlow J, Nyman S, Lindhe J, Karring T, Wennström J. New at-tachment formation in the human periodontium by guided tissue re-
generation. Case reports. J Clin Periodontol 1986; 13:604—616.5. Fleisher N, Waal HD, Bloom A. Regeneration of lost attachment ap-
paratus in the dog using Vicryl absorbable mesh (polyglactin 910).Int J Periodontics Restorative Dent 1988; 8(2):45-54.
6. Quiñones CR, Catón JG, Mota LF, Poison AM, Wagener CJ. Eval-uation of a synthetic biodegradable barrier to facilitate guided tissue
.
regeneration. J Dent Res 1990; 69(Spec. Issue)275(Abstr. 1336).7. Schultz AJ, Gager AH. Guided tissue regeneration using an absorb-
able membrane (polyglactin 910) and osseous grafting, hit J Perio-dontics Restorative Dent 1990; 10:8-17.
8. Caton JG, Frantz B, Greenstein G, Hoffman B, Poison AM, ZappaU. Synthetic biodegradable barrier for regeneration in human perio-dontal defects. J Dent Res 1990; 69(Spec. Issue):275(Abstr. 1335).
9. Hamp SE, Hyman S, Lindhe J. Periodontal treatment of multirootedteeth. Results after 5 years. J Clin Periodontol 1975; 2:126-135.
10. Pontoriero R, Lindhe J, Nyman S, Karring T, Rosenberg E, LanaviF. Guided tissue regeneration in degree II furcation involved mandib-ular molars. A clinical study. J Clin Periodontol 1988; 15:247-254.
11. Rosling B, Nyman S, Lindhe J, Jern B. The healing potential of theperiodontal tissues following different techniques of periodontal sur-
gery in plaque-free dentitions. A 2-year clinical study. J Clin Perio-dontol 1976; 3:233-250.
12. Lindhe J, Westfeit E, Nyman S, Socransky SS, Heijl L, Bratthall G.Healing following surgical/non-surgical treatment of periodontal dis-ease. A clinical study. J Clin Periodontol 1982; 9:115-128.
13. Westfelt E, Bragd L, Socransky SS, Haffajee AD, Nyman S, LindheJ. Improved periodontal conditions following therapy. J Clin Perio-dontol 1985; 12:283-293.
14. Van der Veiden U. Probing force and the relationship of the probetip to the periodontal tissues. J Clin Periodontol 1979; 6:106-114.
15. Nyman S, Gottlow J, Karring T, Lindhe J. The regenerative potentialof the periodontal ligament. An experimental study in the monkey. JClin Periodontol 1982; 9:257-265.
16. Nyman S, Lindhe J, Karring T, Rylander H. New attachment follow-ing surgical treatment of human periodontal disease. J Clin Perio-dontol 1982; 9:290-296.
17. Cole RT, Crigger M, Bogle G, Egelberg J, Selvig KA. Connectivetissue regeneration to periodontally diseased teeth. A histologicalstudy. J Periodont Res 1980; 15:1-9.
18. Becker W, Becker BE, Prichard JF, Caffesse R, Rosenberg E, Gian-Grasso J. Root isolation for new attachment procedures
-
A surgicaland suturing method: Three case reports. J Periodontol 1987; 58:819-826.
19. Melcher AH. Healing wounds in the periodontium. In: Melcher AG,Bowen WH, eds. Biology of the Periodontium. London: AcademicPress; 1969.
20. Line SE, Poison A, Zander H. Relationship between periodontal in-jury, selective cell repopulation and ankylosis. J Periodontol 1974;45:725-730.
21. Boyko GA, Melcher AG, Brunmette DM. Formation of new perio-dontal ligament by periodontal ligament cells implanted in vivo afterculture in vitro. J Periodont Res 1981; 16:73-88.
22. Pontoriero R, Lindhe J, Nyman S, Karring T, Rosenberg E, LanaviF. Guided tissue regeneration in the treatment of furcation defects inmandibular molars. A clinical study of degree III involvements. J ClinPeriodontol 1989; 16:170-174.
23. Magnusson I, Runstad L, Nyman S, Lindhe J. A long junctional ep-ithelium
-
A locus minoris resistentia in plaque infection? J Clin Per-iodontol 1983; 10:333-340.
24. Beaumont RH, O'Leary TJ, Kafrawy AH. Relative resistance of longjunctional epithelial adhesion and connective tissue attachments to
plaque-induced inflammation. J Periodontol 1984; 55:213-223.25. Pitaru S, Tal H, Soldinger M, AzarAvidan O, Noff M. Collagen mem-
branes prevent the apical migration of epithelium during periodontalwound healing. J Periodont Res 1987; 22:331-333.
26. Magnusson I, Batich C, Collins BR. New attachment formation fol-lowing controlled tissue regeneration using biodegradable membranes.J Periodontol 1988; 59:1-7.
27. Pitaru S, Tal H, Soldinger M, Grosskopf A, Noff M. Partial regen-eration of periodontal tissues using collagen barriers. Initial obser-vations in the canine. J Periodontol 1988; 59:380-386.
28. Blumenthal NM. The use of collagen membranes to guide regenera-tion of new connective tissue attachment in dogs. J Periodontol 1988;59:830-836.
29. Pitaru S, Tal H, Soldinger M, Noff M. Collagen membranes prevent

Volume 65Number 11 CATON, GREENSTEIN, ZAPPA 1045
apical migration of epithelium and support new connective tissue at-
tachment during periodontal wound healing in dogs. J Periodont Res1989; 24:247-253.
30. Card SJ, Caffesse RG, Smith BA, Nasjleti CE. New attachment fol-lowing the use of a resorbable membrane in the treatment of Perio-dontitis in dogs. Int J Periodontics Restorative Dent 1989; 9:59—69.
31. Gantes , Martin M, Garrett S, Egelberg J. Treatment of periodontalfurcation defects. (II). Bone regeneration in mandibular class II de-fects. J Clin Periodontal 1988; 15:232-239.
32. Garrett S, Loos B, Chamberlain D, Egelberg J. Treatment of intraos-seous periodontal defects with a combined adjunctive therapy of citricacid conditioning, bone grafting, and placement of collagenous mem-
branes. J Clin Periodontal 1988; 15:383-389.33. Busschop J, De Boever J. Clinical and histological characteristics of
lyophilized allogenic dura mater in periodontal bony defects in hu-mans. J Clin Periodontal 1983; 10:399-411.
34. Blumenthal NM. The use of collagen materials in bone grafted defectsto enhance guided tissue regeneration. Periodont Case Reports 1987;9:16-22.
35. Iglhaut J, Suggs C, Borjesson B, Aukhil I. Apical migration of oralepithelium in experimental dehiscence wounds. J Clin Periodontal1987; 14:508-514.
36. Zappa U. Resorbierbare Membranen (II). Parodontale Geweberege-neration unter Verwendung von resorbierbaren Membranen
-
Histo-
logische Aspekte. Schweiz Monatsschr Zahnmed 1991; 101:1321—1326.
37. Dahlin C, Lindhe J, Gottlow J, Nyman S. Healing of bone defects byguided tissue regeneration. Plast Reconstr Surg 1988; 81:672-676.
38. Conn J, Oyasu R, Welsh M, Beai JM. Vicryl (polyglactin 910) syn-thetic absorbable sutures. Am J Surg 1974; 128:19-23.
39. Cutright DE, Perez B, Beasley JD, Larson WJ, Posey WR. Degra-dation rates of polymers and copolymers of polylactic and polygly-colic acids. Oral Surg Oral Med Oral Pathol 1974; 37:142-152.
40. Miller RA, Brady JM, Cutright DE. Degradation rates of oral resorb-able implants (polylactates and polyglycolates): Rate modificationwith changes in PLA/PGA copolymer ratios. J Biomed Mater Res1977; 11:711-719.
41. Brady JM, Cutright DE, Miller RA, Battistone GC, Hunsuck EE. Re-sorption rate, route of elimination, and ultrastructure of the implantsite of polylactic acid in the abdominal wall of the rat. J Biomed MaterRes 1973; 7:155-166.
42. Karring T, Nyman S, Lindhe J, Sirirat M. Potentials for root résorp-tion during periodontal wound healing. J Clin Periodontal 1984; 11:41-52.
Send reprint requests to: Dr. Jack Caton, Eastman Dental Center, De-partment of Periodontology, 625 Elmwood Avenue, Rochester, NY 14620.
Accepted for publication June 4, 1994.




![Bioabsorbable Stents - · PDF fileCompany Picture Polymer/Drug Features Bioabsorbable Vascular Solutions (BVS) [Guidant] All biodegradable polymers (PLLA) with everolimus Igaki-Tamai](https://img.dokumen.tips/doc/110x75/5a70b7c97f8b9ab1538c312d/bioabsorbable-stents-summitmdcomwwwsummitmdcompdfpdf060526lec6pdfpdf.jpg)
























