Embed Size (px)
Citation preview

914
BRIEF REPORT
SYNOVIAL LYMPHOCYTE RESPONSE TO CHLAMYDIAL STIMULATION ASSOCIATED WITH INTRASYNOVIAL CHLAMYDIAL ANTIGEN IN A PATIENT WITH “RHEUMATOID ARTHRITIS”
DENYS K. FORD, GRAHAM D. REID, SATHISH MAGGE, and H. RALPH SCHUMACHER
A 48-year-old man with “rheumatoid arthritis” of 3 years duration was found to have synovial fluid lympho- cytes that were maximally stimulated in vitro by chlamyd- ial antigen, on 5 of 6 tests over 18 months. Immunocyto- chemical staining of a synovectomy specimen, using the peroxidase-antiperoxidase technique, subsequently re- vealed chlamydial antigen in the synovium. The possibility that Chlamydia in the synovium may produce features of rheumatoid arthritis is discussed.
The 3H-thymidine uptake response of synovial lymphocytes to microbial antigen stimulation appears to suggest the origin of the arthritis in enteric and sexually transmitted Reiter’s syndrome (1-4). The finding that the synovial lymphocytes of Lyme disease patients react to Borreliu burgdorferi antigens to a greater extent than do their peripheral blood lympho- cytes ( 5 ) lends evidence to support the validity of this approach.
Studies in patients with rheumatoid arthritis (RA) have raised the possibility that the response of synovial lymphocytes to microbial antigen stimulation might also be helpful for research into that disease. Over 70 patients with RA have been studied and the
From the Department of Medicine, University of British Columbia, Vancouver, British Columbia, Canada, and the Depart- ment of Medicine, University of Pennsylvania, Philadelphia.
Denys K. Ford, MD: Professor of Medicine, University of British Columbia: Graham D. Reid, MB: Clinical Assistant Profes- sor of Medicine, University of British Columbia; Sathish Magge, MD: Research Fellow, University of Pennsylvania; H. Ralph Schu- macher, MD: Professor of Medicine, University of Pennsylvania.
Address reprint requests to Denys K. Ford, MD, The Arthritis Centre, 895 West 10th Avenue, Vancouver, British Colum- bia, V5Z 1L7, Canada.
Submitted for publication September 29, 1987: accepted in revised form January 18, 1988.
results reported, either as observations on “controls” for the findings in patients with Reiter’s syndrome (2,3) or as observations on RA patients whose synovial lymphocytes reacted maximally to a particular antigen (6-10). We report the association of a repeated syno- vial lymphocyte response to chlamydial stimulation with the presence of chlamydial antigen in a surgically removed synovial specimen from a patient diagnosed as having RA.
Case report. The patient injured his right knee while playing soccer in 1953, when he was 16 years old. Surgery was performed, and he had 3 episodes of “water on the knee” over the next 10 years. In 1982, at the age of 45, he had an episode of pain and swelling at the base of his right thumb. About 2 months later, he noted generalized stiffness, fatigue, and weight loss of approximately 7 kg. He developed pain in the fingers, wrists, shoulders, neck, and knees, and his right knee became swollen.
The patient was referred to one of us (GDR) 5 months after the onset of his polyarthritis. At that time he had pain and swelling of several finger joints, both wrists, both shoulders, and both knees. There was a large effusion in the right knee. All of the metatarso- phalangeal joints were tender, and both fifth toes were swollen and red; in addition, there was tenderness beneath the left heel. Based on the clinical assessment, it was concluded that the patient had an asymmetric polyarthritis. It was noted in his chart that, “in view of the swelling of the little toes and the heel pain, one might suspect that this will be a seronegative type.” The patient denied having diarrhea or genitourinary symptoms.
Over the next 2 years, the polyarthritis per- sisted; the right knee was always the most involved
Arthritis and Rheumatism, Vol. 31, No. 7 (July 1988)

BRIEF REPORTS
PHA
joint. Rheumatoid factor was found (titer 1:640 by latex fixation). Radiographs showed erosions in the hands and feet, and normal sacroiliac joints. Gold treatment for rheumatoid arthritis was started in March 1984 and continued at varying dosages up to the present. Various nonsteroidal antiinflammatory drugs were also given.
The patient demonstrated 3 types of skin le- sions during the 3-year observation period. He was referred to a dermatologist who noted scattered scal- ing plaques typical of psoriasis, tinea versicolor of the trunk, and stasis eczema of both lower legs. Significant lymphadenopathy of the hilar, axillary, and epitroch- lear nodes was also noted, but only reactive hyperpla- sia was shown on biopsy. HLA typing revealed A2,29;B7,49;DR1,4.
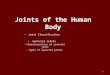
Synovial fluid was obtained from the patient’s right knee on 6 occasions between August 1983 and January 1985, as shown in Figure 1. In 5 of the 6 studies, the synovial lymphocytes were stimulated maximally by chlamydial antigen, while once (August 1984) there was no significant stimulation from any
a
Ureaplasma
Chlamydia
Salmonella Candida
Rubella
Mumps
Adenovirus Parainfluenza
Resp. Syn.
Reovirus
Coxsackie
Varicella
Measles CMV
S T I M U L A T I O N I N D I C E S
20 40 2040 60 A-
I -F Mar *a4
915
antigen. On the first test (August 1983), reactivity with phytohemagglutinin was also studied; it, too, elicited less of a stimulation response than the chlamydial antigen. In August 1985, similar testing was performed with the patient’s peripheral blood lymphocytes. These lymphocytes also responded to a chlamydial antigen more than to other antigens; the stimulation index was twice that obtained from the antigen with the next highest stimulation index. These lymphocyte studies were performed using techniques that have been standard for the last 8 years and have been extensively described in earlier reports (1-4,641).
In May 1985, a total right knee replacement was performed, and the synovial tissue removed was dis- sected to select hypertrophied villous synovium, both for electron microscopy and for the freezing of ali- quots. The routine pathology report stated, “the sy- novium is heavily inflamed with chronic inflammatory cells including many plasma cells-consistent with rheumatoid arthritis.” A frozen aliquot was forwarded to Dr. Wanda Wenman (Division of Pediatrics, Infec- tious Diseases, University of Alberta, Edmonton, Al-
2040 60 a0100120 111111
20 1
Mar. May Aug. Jan. 384 ’a4 984 ’a5
Figure 1. ’H-thymidine uptake response of the patient’s synovial fluid lymphocytes to various antigens, on 6 occasions between August 1983 and January 1985. Resp. Syn. = respiratory syncytial virus; CMV = cytomegalovirus; PHA = phytohemagglutinin.

916 BRIEF REPORTS
berta, Canada), who had developed a DNA hybridiza- tion probe for chlamydial nucleic acid. She was unable to demonstrate any chlamydial nucleic acid in this frozen specimen. Another sample of synovium was fixed in 1% glutaraldehyde and forwarded to one of the authors (HRS) in Philadelphia for ultrastructural and immunocytochemical studies.
Routine transmission electron microscopy showed proliferation of types A and B synovial lining cells, scattered lymphocytes and plasma cells, and vessels with endothelial proliferation and multilamina- ted basement membrane. There were many macro- phage-like cells with phagocytic vacuoles containing finely granular and particulate material, but no sugges- tion of any identifiable microorganisms. Some of the vacuoles contained typical aurosomes (12); energy dispersive elemental analysis ( I 3) confirmed that these contained gold. Some dense inclusions contained both gold and small, round, darker particles with indistinct margins.
Portions of tissue were processed for immuno- cytochemical studies to search for chlamydial antigen. Endogenous peroxidase was blocked by incubation in 0.03% H,O, for 30 minutes. The specimen was next incubated in normal goat globulin and then in 0.01% saponin to permeabilize membranes. This was fol- lowed by incubation in rabbit antichlamydial antibody (Abbott, Chicago, IL) diluted 1: 100 (previously deter- mined to be the optimum dilution) for 1 hour at room temperature. After washing, goat anti-rabbit IgG (1 :20) was added in excess, so that binding sites were avail- able for the peroxidase-antiperoxidase complex, which was added in 1 :40 concentration after a further wash. The tissue was finally incubated in Tris buffer, H,O,, and diaminobenzidine, which would produce a dark reaction if chlamydial antigen was present. This procedure revealed marked dark staining of the parti- cles in many vacuoles of the macrophage-like cells. No reaction product was seen in any other sites.
Control procedures, consisting of replacement of the antichlamydial antibody with normal rabbit globulin, elimination of the peroxidase-antiperoxidase complex, and absorption of the antibody with Chla- mydia yielded totally negative results or showed only very rare and irregular suggestions of a reaction prod- uct. Positive control procedures were also performed, using synovia from 2 patients with Reiter’s syndrome and cultured chlamydial organisms (14). Similar find- ings of chlamydial reactivity in synovial tissue and cells of Reiter’s syndrome patients have recently been described by Keat et al, who used a fluorescein- labeled monoclonal antibody to Chlamydia trachoma-
tis (15). Three other synovial membranes from patients with RA were negative for chlamydial reactivity.
Despite the above-described findings, a sample of the patient’s serum, which was forwarded to Dr. Robert C. Brunham (Department of Medical Microbi- ology, University of Manitoba, Winnipeg, Manitoba, Canada), did not reveal either IgM or IgG antibody against C trachomatis.
Discussion. The results of several studies (6-10) suggest that rheumatoid arthritis may be a clinical syndrome caused by an aberrant immune response to a variety of common infectious agents, and that the microbiologic cause of a particular patient’s RA may be designated by the response of synovial lympho- cytes to that particular antigen, as compared with the response to antigens of other, nonrelevant agents. This viewpoint has recently been expressed in greater detail ( 16,17).
The demonstration of a maximal synovial lym- phocyte response to a particular antigen is not, in itself, sufficient evidence that the organism plays an etiologic role in the patient’s disease; further docu- mentation of a relationship between that particular agent and the arthritis is needed. Earlier studies in Vancouver have shown that, in each of 3 cases, the finding of a maximal synovial lymphocyte response to rubella antigen was associated with the isolation of rubella virus from the patient (8,9). In the present case, chlamydial antigen was found in the synovium, following the observation that the patient’s synovial lymphocytes responded maximally to stimulation with chlamydial antigen on successive occasions. Although an attempt was made to demonstrate chlamydial nu- cleic acid in the removed synovial specimen, it was unsuccessful. The sensitivity of the hybridization tech- nique employed and the suitability of the frozen spec- imen shipped to Edmonton are uncertainties in trying to relate this negative finding to the finding of synovial chlamydial antigen by the immunoperoxidase method employed in the Philadelphia laboratory.
This patient had “rheumatoid arthritis,” with radiographically evident erosions and positive rheu- matoid factor. He also had scattered skin lesions, which a dermatologist confidently diagnosed as psori- asis; moreover, he had “dactylitis” and some heel pain. In the opinion of the 2 rheumatologists respon- sible for his medical care, his disease did not fulfill criteria for psoriatic arthritis; both treated him for “rheumatoid arthritis.” The hilar, axillary, and epi- trochlear lymphadenopathy showed only reactive hy- perplasia on lymph node biopsy. At no time was there any indication that his arthritis was related to genito-

BRIEF REPORTS 917
urinary or intestinal symptoms, and he denied having any such symptoms.
Only this patient and one other patient with “rheumatoid arthritis” have shown a significant syno- vial lymphocyte response to chlamydial antigen; the study group now includes 70 patients with RA. Thus, if synovial lymphocyte response can suggest t he underly- ing causative agents in RA, Chlamydia is likely to be related to the disease in only a small percentage of cases. Previous evidence that Chlamydia might be related to unexplained knee arthritis (18), an entity which is clinically distinct from sexually acquired reac- tive arthritis, seems to have received recent confirma- tion (19), and there is thus no a priori reason why Chlamydia could not be responsible for the clinical syndrome of rheumatoid arthritis in some cases. The demonstration of gold in the same inclusions as the chlamydial antigen is of interest and may have implica- tions for the mechanism of action of gold as a treatment. The failure to demonstrate serum antibody against chlamydial antigen in our patient is perhaps not unex- pected, in view of similar findings in 13 patients with failed rubella immunization, of whom 3 had arthritis (20). Studies of the synovial lymphocyte responses in additional patients with RA are needed to further elu- cidate the possible role of infectious agents in this disease.
Acknowledgments. We thank Doreen da Roza, Susan Rothfuss, and Marie Sieck for technical assistance, and Dr. W. R. Bowie of the Division of Infectious Diseases, Univer- sity of British Columbia, for providing the chlamydial antigen.
REFERENCES 1. Ford DK, da Roza DM, Shah P, Wenman W: Cell-
mediated immune responses of synovial mononuclear cells in Reiter’s syndrome against ureaplasmal and chla- mydial antigens. J Rheumatol 7:751-755, 1980
2. Ford DK, da Roza DM, Shah P: Cell-mediated immune responses of synovial mononuclear cells to sexually transmitted, enteric and mumps antigens in patients with Reiter’s syndrome, rheumatoid arthritis and ankylosing spondylitis. J Rheumatol 8:220-232, 1981
3. Ford DK, da Roza DM, Schulzer M: The specificity of synovial mononuclear cell responses to microbiological antigens in patients with arthritis. J Rheumatol 9561- 567, 1982
4. Ford DK, da Roza DM, Schulzer M: Lymphocytes from the site of disease but not blood lymphocytes indicate the cause of arthritis. Ann Rheum Dis 44:701-710, 1985
5. Sigal LH, Steere AC, Freeman DH, Dwyer JM: Prolif-
erative responses of mononuclear cells in Lyme disease: reactivity to Borrelia burgdorferi antigens is greater in joint fluid than in blood. Arthritis Rheum 29:761-769, 1986
6. Ford DK, da Roza DM: Observations on the response of synovial lymphocytes to viral antigens in rheumatoid arthritis and Reiter’s syndrome. J Rheumatol 10:643- 646, 1983
7. Ford DK, da Roza DM: Further observations on the responses of synovial lymphocytes to viral antigens in rheumatoid arthritis. J Rheumatol 13: 113-1 17, 1986
8. Ford DK, da Roza DM, Reid GD, Chantler JK, Tingle AJ: Synovial mononuclear cell responses to rubella antigen in rheumatoid arthritis and unexplained persist- ent knee arthritis. J Rheumatol 9:420-423, 1982
9. Chantler JK, da Roza DM, Bonnie ME, Reid GD, Ford DK: Sequential studies on synovial lymphocyte stimu- lation by rubella antigen, and rubella virus isolation in an adult with persistent arthritis. Ann Rheum Dis 44:564- 568, 1985
10. Ford DK, da Roza DM, Schulzer M, Reid GD, Denegri JF: Persistent synovial lymphocyte responses to cyto- megalovirus antigen in some patients with rheumatoid arthritis. Arthritis Rheum 30:700-704, 1987
11. Ford DK: Synovial lymphocyte responses in the spon- dyloarthropathies. Adv Inflamm Res 9: 189-202, 1985
12. Oryshak AF, Ghadially FN: Aurosome formation in articular tissues after parenteral administration of gold. J Pathol 119:183-185, 1976
13. Bardin T , Schumacher HR, Lansaman J, Rothfuss S, Dryll A: Transmission electron microscopic identifica- tion of silicon containing particles in synovial fluid. Ann Rheum Dis 43:624-627, 1984
14. Schumacher HR Jr, Cherian PV, Sieck M, Clayburne G: Ultrastructural identification of chlamydial antigens in synovial membrane in acute Reiter’s syndrome (abstract). Arthritis Rheum 29 (suppl 4):S31, 1986
15. Keat A, Dixey J , Sonnex C, Thomas B, Osborn M, Taylor-Robinson D: Chlamydia trachomatis and reac- tive arthritis: the missing link. Lancet I:72-74, 1987
16. Ford DK: Reactive arthritis: a viewpoint rather than a review. Clin Rheum Dis 12:389-401, 1986
17. Ford DK: One syndrome-many infectious agents. J Rheumatol 14:650-652, 1987
18. Ford DK, da Roza DM, Ward RH: Arthritis confined to knee joints: synovial lymphocyte responses to microbial antigens correlate with distribution of HLA. Arthritis Rheum 27: 1157-1 164, 1984
19. Dixey J, Thomas B , Taylor-Robinson D, Osburn M, Keat A: Chlamydia trachomatis and unexplained knee synovitis in women (abstract). Arthritis Rheum 30 (suppl 4):S42, 1987
20. Tingle AJ, Chantler JK, Kettyls GD, Larke RPB, Schulzer M: Failed rubella immunization in adults: association with immunologic and virologic abnormali- ties. J Infect Dis 151:330-336, 1985