Embed Size (px)
Citation preview

SwitchSwitch
SwitchSwitch
Safety and Efficacy of Crossover (Switch) from UFH/Enox to
Bivalirudin: Results from ACUITY
Safety and Efficacy of Crossover (Switch) from UFH/Enox to
Bivalirudin: Results from ACUITY
Dr. Harvey White
Green Lane Cardiovascular Service
Auckland City Hospital, Auckland, NZ
Dr. Harvey White
Green Lane Cardiovascular Service
Auckland City Hospital, Auckland, NZ

DisclosureDisclosure
Research Grants : Alexion Fournier Laboratories Sanofi Aventis
Johnson & Johnson Eli Lilly Proctor & Gamble Merck Sharpe & Dohme Schering Plough Roche The Medicines Company Glaxo Smith Kline Pfizer Neuren Pharmaceuticals NIH
Consultant: Sanofi Aventis The Medicines Company

BackgroundBackground ACS patients
87% of patients receive either UFH or Enox within 24 hours after admission1
72% of patients in Synergy and 50 % of patients in OASIS- 5 received prior antithrombin2,3
Published studies and perceptions Patients in Synergy who crossed over between UFH
and Enox had an increase in bleeding complications2
This activity occurred at various times through the study period: at times in response to clinical or clinician perception
Consistent therapy is better4
ACS patients 87% of patients receive either UFH or Enox within 24
hours after admission1
72% of patients in Synergy and 50 % of patients in OASIS- 5 received prior antithrombin2,3
Published studies and perceptions Patients in Synergy who crossed over between UFH
and Enox had an increase in bleeding complications2
This activity occurred at various times through the study period: at times in response to clinical or clinician perception
Consistent therapy is better4
1 CRUSADE( 1Q-2006 results); 2 Synergy results; JAMA 2004; 3 OASIS -5; Yusuf et al,NEJM 2006; 4 Cohen et al, JACC 2006;

Scope of AnalysisScope of Analysis This analysis will address the question of
the safety and efficacy of switching from indirect thrombin inhibition (UFH or Enox) to direct thrombin inhibition (bivalirudin) A protocol-driven activity of the ACUITY study
at the time of randomization
This analysis will address the question of the safety and efficacy of switching from indirect thrombin inhibition (UFH or Enox) to direct thrombin inhibition (bivalirudin) A protocol-driven activity of the ACUITY study
at the time of randomization

ACUITY: Primary resultsACUITY: Primary results
Heparin* + IIb/IIIa vs. Bivalirudin + IIb/IIIa vs. Bivalirudin Alone Heparin* + IIb/IIIa vs. Bivalirudin + IIb/IIIa vs. Bivalirudin Alone
7.3%5.7%
11.7%
7.7%
11.8%
5.3%
3.0%
10.1%
7.8%
Net clinical outcome Composite ischemia Major bleeding (non-CABG)
30 d
ay e
ven
ts (
%)
Heparin+IIb/IIIa (N=4603) Bivalirudin+IIb/IIIa (N=4604) Bivalirudin alone (N=4612)
PNI <0.001PSup = 0.015
PNI = 0.011 PSup = 0.32
PNI <0.001PSup <0.001
*Heparin=unfractionated or enoxaparin

UF Heparin Enoxaparin BivalirudinU/Kg mg/Kg mg/kg
Bolus 60 1.0 sc bid 0.1 iv
Infusion/h 121 0.25 iv
PCIACT
200-250s
0.30 iv bolus2
0.75 iv bolus3
0.50 bolus iv
1.75/h infusion iv4
CABG Per institution Per institution Per institution5
Medical mgt None6 None6 None6
Study MedicationsStudy Medications Anti-thrombin agents (started pre angiography) Anti-thrombin agents (started pre angiography)
1 Target aPTT 50-75 seconds2 If last enoxaparin dose ≥8h - <16h before PCI; 3 If maintenance dose discontinued or ≥16h from last dose4 Discontinued at end of PCI with option to continue at 0.25mg/kg for 4-12h if GPIIb/IIIa inhibitor not used5 Bivalirudin option for off-pump same as PCI dose. For on-pump bivalirudin discontinued 2 hours before6 Option to continue with pre-PCI anti-thrombotic regimen at physician discretion

Prior treatmentPrior treatment ACUITY Protocol requirements
Patients on an antithrombin (either UFH or Enox) prior to randomization:
Continued the same treatment if randomized into Heparin(s) + GP IIb/IIIa arm
Switched to bivalirudin if randomized to one of the bivalirudin arms
Following results of Synergy UFH was allowed in the trial Sites prospectively determined the preferred anti-
thrombin strategy of either UFH or Enox Switch between UFH and Enox was not permitted
ACUITY Protocol requirements Patients on an antithrombin (either UFH or Enox) prior
to randomization: Continued the same treatment if randomized into Heparin(s)
+ GP IIb/IIIa arm Switched to bivalirudin if randomized to one of the bivalirudin
arms
Following results of Synergy UFH was allowed in the trial Sites prospectively determined the preferred anti-
thrombin strategy of either UFH or Enox Switch between UFH and Enox was not permitted

Current AnalysisCurrent Analysis
Hypothesis Bivalirudin improves bleeding outcomes while
preserving ischemic protection for ACS patients even if the patients are switched from either UFH or enoxaparin to bivalirudin (monotherapy) at the time of presentation.
Is it better to switch to bivalirudin or remain on consistent therapy?
Hypothesis Bivalirudin improves bleeding outcomes while
preserving ischemic protection for ACS patients even if the patients are switched from either UFH or enoxaparin to bivalirudin (monotherapy) at the time of presentation.
Is it better to switch to bivalirudin or remain on consistent therapy?

Current AnalysisCurrent Analysis
Methods Patients on prior antithrombin
Consistent: No switching from pre-randomization anti-thrombin to randomized therapy:
Enox →Enox or UFH → UFH
Switch: Single switch to bivalirudin determined by randomization code
from Enox → bivalirudin or UFH →bivalirudin
Event rates at 30-days Net Clinical Outcome Ischemic Composite Major Bleeding
Methods Patients on prior antithrombin
Consistent: No switching from pre-randomization anti-thrombin to randomized therapy:
Enox →Enox or UFH → UFH
Switch: Single switch to bivalirudin determined by randomization code
from Enox → bivalirudin or UFH →bivalirudin
Event rates at 30-days Net Clinical Outcome Ischemic Composite Major Bleeding

ACUITY Primary Endpoints at 30 daysACUITY Primary Endpoints at 30 days
Net Clinical Endpoint Composite ischemic and non-CABG major bleeding endpoints
Ischemic Endpoint Death, MI, or unplanned revascularization
Non-CABG Major Bleeding Endpoint Intracranial, intraocular, or retroperitoneal bleeding Access site bleed requiring intervention/surgery Hematoma ≥5 cm Hgb ≥3g/dL with an overt source or ≥4g/dL w/o overt source Blood transfusion
Net Clinical Endpoint Composite ischemic and non-CABG major bleeding endpoints
Ischemic Endpoint Death, MI, or unplanned revascularization
Non-CABG Major Bleeding Endpoint Intracranial, intraocular, or retroperitoneal bleeding Access site bleed requiring intervention/surgery Hematoma ≥5 cm Hgb ≥3g/dL with an overt source or ≥4g/dL w/o overt source Blood transfusion
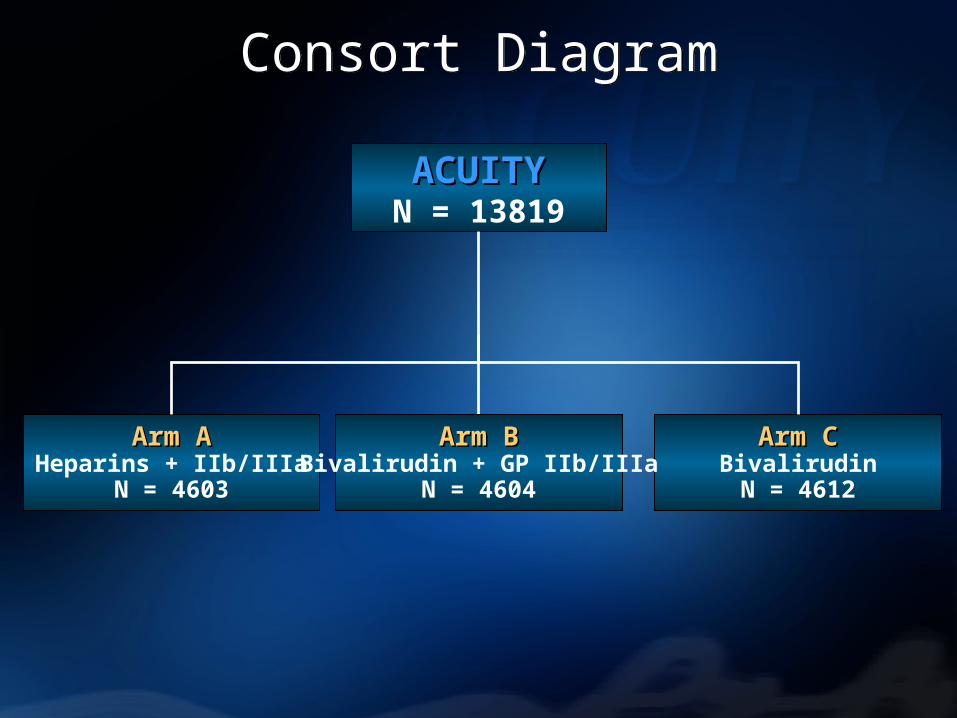
Consort DiagramConsort Diagram
ACUITYACUITYN = 13819
Arm AArm AHeparins + IIb/IIIa
N = 4603
Arm CArm CBivalirudinN = 4612
Arm BArm BBivalirudin + GP IIb/IIIa
N = 4604

Consort DiagramConsort Diagram
ACUITYACUITYN = 13819
Arm AArm AHeparins + IIb/IIIa
N = 4603
Arm CArm CBivalirudinN = 4612

Consort DiagramConsort Diagram
ACUITYACUITY13819
Arm A: CONSISTENTArm A: CONSISTENTHeparins + IIb/IIIa
N = 2223
Arm C: SWITCHArm C: SWITCHBivalirudinN = 2237
Pts on Prior ATN = 6606 ╪
•╪ excludes Arm B and pts. with multiple crossovers, missing data

Consort DiagramConsort Diagram
ACUITYACUITY13819
CONSISTENTCONSISTENTUFH/EnoxN = 2223
SWITCHSWITCHBivalirudin*
N = 2237
UFH→UFHN = 1294
Enox→EnoxN = 929
UFH→BivN = 1313
Enox→BivN = 857
Pts on Prior ATN = 6606 ╪
• * Includes 67 pts. who had UFH and Enox • ╪ excludes Arm B and pts. with multiple crossovers, missing data

Baseline Characteristics Consistent UFH/Enox vs. Switch to Biv
Baseline Characteristics Consistent UFH/Enox vs. Switch to Biv
* creatinine clearance <60 mL/min *Elevated cardiac markers and/or ST changes
ConsistentUFH/EnoxN = 2223
SwitchBivalirudinN = 2237
P-value
Age (median [range], yrs) 63 [23, 91] 62 [20, 92] 0.02Male (%) 71.6 70.0 NS
Weight (median [IQR], kg) 83 [73, 96] 84 [73, 96] NS
Diabetes(%) 27.6 25.0 0.05Hypertension (%) 64.5 63.8 NSHyperlipidemia (%) 54.6 54.0 NSCurrent smoker (%) 29.5 30.7 NSPrior MI (%) 31.0 30.4 NSPrior PCI (%) 36.8 36.8 NSPrior CABG (%) 18.4 18.1 NSThienopyridine exposure 63.8 66.1 NSRenal insufficiency* (%) 19.6 17.4 NSHigh Risk* (%) 77.6 74.6 0.02Troponin + (%) 65.4 63.6 NS

11.9%
7.3%5.8%
6.9%
9.1%
2.8%
Net Clinical Outcome Ischemic composite Major bleeding
30
da
y e
ve
nts
(%
)
Consistent UFH/Enox (N = 2223 )
Switch to Bivalirudin (N= 2237)
Comparing Consistent therapy on UFH/Enoxvs. Switch Bivalirudin Alone
Comparing Consistent therapy on UFH/Enoxvs. Switch Bivalirudin Alone
Consistent vs. SwitchConsistent vs. Switch
P=0.002
0.77 [0.63 – 0.91]
P=0.601
0.95 [0.76 – 1.17]
P<0.001
0.47 [0.35 – 0.64]

0 1 2
0.83 (0.67-1.02)
OR (95% CI)Odds ratio±95% CI
Switch to Bivalirudin alone betterSwitch to Bivalirudin alone better Consistent UFH/Enox betterConsistent UFH/Enox better
Major Bleeding
Ischemia
Net Clinical Outcome
1.10 (0.86-1.41)
0.47 (0.34-0.65)
P-value
0.073
0.464
<0.001
* Comparing consistent Hep/Enox vs Switch Bivalirudin* Comparing consistent Hep/Enox vs Switch Bivalirudin
Consistent vs. SwitchAll Patients - Adjusted
Consistent vs. SwitchAll Patients - Adjusted

Consistent vs. SwitchHigh Risk - Unadjusted
Consistent vs. SwitchHigh Risk - Unadjusted
Comparing Consistent UFH/Enox vs Switch Bivalirudin Comparing Consistent UFH/Enox vs Switch Bivalirudin
Consistent
UFH/Enox
N = 1654
Switch
Bivalirudin
N = 1623
RR
Net Clinical Outcome
13.1% 10.6% 0.81 [0.67-0.98]
Ischemia 8.0% 7.8% 0.97 [0.76-1.22]
Major Bleeding 6.6% 3.5% 0.52 [0.38-0.72]

0 1 2
0.86 (0.68-1.07)
OR (95% CI)Odds ratio±95% CI
Switch to Bivalirudin alone betterSwitch to Bivalirudin alone better Consistent UFH/Enox betterConsistent UFH/Enox better
Major Bleeding
Ischemia
Net Clinical Outcome
1.11 (0.85-1.46)
0.51 (0.36-0.72)
P-value
0.177
0.445
<0.001
Consistent vs. SwitchHigh Risk - Adjusted
Consistent vs. SwitchHigh Risk - Adjusted
Comparing Consistent UFH/Enox vs Switch Bivalirudin Comparing Consistent UFH/Enox vs Switch Bivalirudin

Consistent vs. SwitchPatients undergoing PCI - Unadjusted
Consistent vs. SwitchPatients undergoing PCI - Unadjusted
Comparing Consistent UFH/Enox vs Switch Bivalirudin Comparing Consistent UFH/Enox vs Switch Bivalirudin
Consistent
UFH/Enox
N = 1293
Switch
Bivalirudin
N = 1390
RR
Net Clinical Outcome
13.3% 11.8% 0.89 [0.73 -1.08]
Ischemia 8.1% 9.0% 1.06 [0.81 -1.40]
Major Bleeding 6.9% 3.5% 0.50 [0.36-0.71]

11.2%
7.0%
5.2%6.4%
9.1%
2.8%
Net Clinical Outcome Ischemic composite Major bleeding
30
da
y e
ve
nts
(%
)
Consistent Enox (N = 929 )
Switch from Enox to Bivalirudin (N= 857)
Comparing Consistent therapy on Enox vs. Switch from Enox to Bivalirudin Alone
Comparing Consistent therapy on Enox vs. Switch from Enox to Bivalirudin Alone
Consistent vs. SwitchConsistent vs. Switch
P=0.145
0.81 [0.61 – 1.07]
P=0.626
0.92 [0.65 – 1.30]
P=0.013
0.54 [0.34 – 0.88]

12.4%
7.6%6.3%
7.4%
9.4%
2.8%
Net Clinical Outcome Ischemic composite Major bleeding
30
da
y e
ve
nts
(%
)
UFH+ GP IIb/IIIa (N = 1294 )
UFH to Bivalirudin (N= 1313)
Comparing Consistent therapy on UFH vs. Switch from UFH to Bivalirudin Alone
Comparing Consistent therapy on UFH vs. Switch from UFH to Bivalirudin Alone
Consistent vs. SwitchConsistent vs. Switch
P=0.012
0.75[0.60 – 0.94]
P=0.857
0.98[0.74 – 1.28]
P<0.001
0.44[0.30 – 0.65]
0 1 2
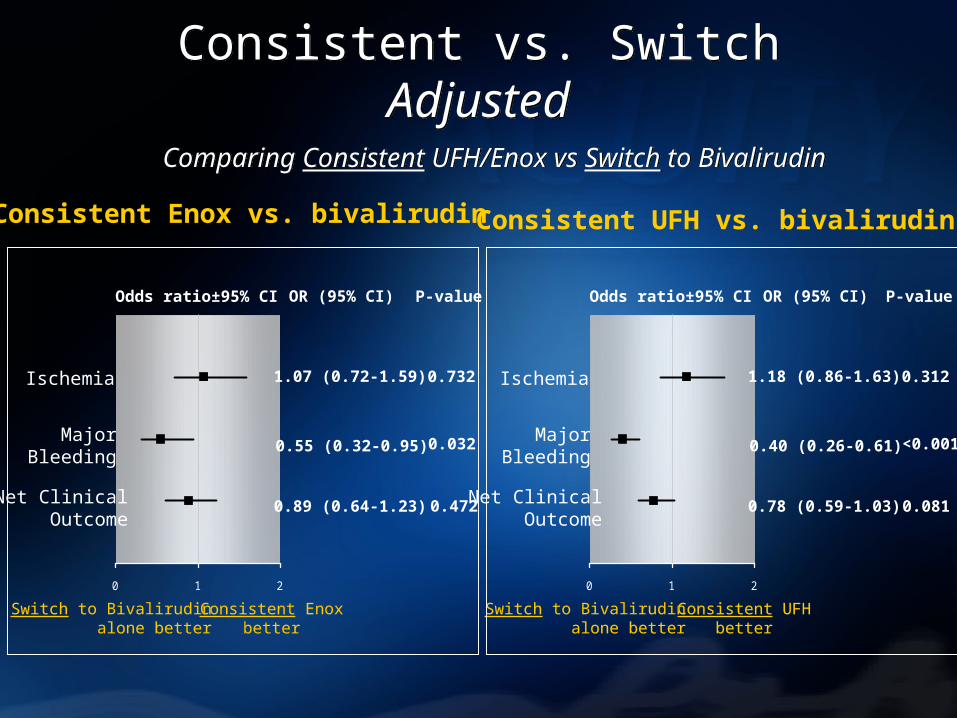
0.89 (0.64-1.23)
OR (95% CI)Odds ratio±95% CI
Switch to Bivalirudinalone better
Switch to Bivalirudinalone better
Consistent Enoxbetter
Consistent Enoxbetter
MajorBleeding
Ischemia
Net ClinicalOutcome
1.07 (0.72-1.59)
0.55 (0.32-0.95)
P-value
0.472
0.732
0.032
0 1 2
0.78 (0.59-1.03)
OR (95% CI)Odds ratio±95% CI
Switch to Bivalirudinalone better
Switch to Bivalirudinalone better
Consistent UFHbetter
Consistent UFHbetter
MajorBleeding
Ischemia
Net ClinicalOutcome
1.18 (0.86-1.63)
0.40 (0.26-0.61)
P-value
0.081
0.312
<0.001
Consistent vs. SwitchAdjusted
Consistent vs. SwitchAdjusted
Comparing Consistent UFH/Enox vs Switch to BivalirudinComparing Consistent UFH/Enox vs Switch to Bivalirudin
Consistent Enox vs. bivalirudin Consistent UFH vs. bivalirudin

LimitationsLimitations Post-hoc subgroup analysis
Pre-randomization use of anti-thrombin was not stratified
Timing and dose of last UFH and Enox was not collected in the CRF
Post-hoc subgroup analysis
Pre-randomization use of anti-thrombin was not stratified
Timing and dose of last UFH and Enox was not collected in the CRF

ConclusionsConclusions Switching to bivalirudin is safe
Switching from any heparin (either enoxaparin or UFH) to bivalirudin monotherapy is not associated with an increased risk for ischemic events.
Furthermore Switch to bivalirudin provides patients the
50% bleeding advantage of bivalirudin compared with consistent therapy on UFH or enoxaparin.
Switching to bivalirudin is safe Switching from any heparin (either enoxaparin
or UFH) to bivalirudin monotherapy is not associated with an increased risk for ischemic events.
Furthermore Switch to bivalirudin provides patients the
50% bleeding advantage of bivalirudin compared with consistent therapy on UFH or enoxaparin.




























