Embed Size (px)
Citation preview

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 1/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory Effective Date: 2/28/08
Dallas County Institute of Forensic Sciences
Forensic Laboratory
QUALITY MANAGEMENT PROGRAM
Quality Manual, Version 2.3
Authorized by:
Jeffrey J. Barnard, M.D.
Director and Chief Medical Examiner
Chris Heartsill
Quality Manager (Acting)
Timothy J. Sliter, Ph.D.
Chief, Physical Evidence
Elizabeth Todd, Ph.D.
Chief, Forensic Chemistry
Effective date: February 28, 2008
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 2/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory i Effective date: 2/28/2008
Summary of Changes from Previous Version
Previous version: Quality Manual, Version 1.0
Current version: Quality Manual, Version 2.X
1. Corrections of various typographical and grammatical errors.
2. Various non-substantive changes in wording and format to improve clarity.
3. Revision of Distribution List page and §3.4 to reflect electronic distribution of the
manual through the Quality Management System Portal.
4. Addition of §5.4.1.1.2.1, §5.5.8, §17.4.4.1, and §17.4.4.2 to clarify responsibilities of the
Executive Committee and Director in instances of alleged serious negligence or
misconduct by staff or subcontractors.
5. Revision of §9.1.2 to clarify Custodian of Records responsibilities.
6. Addition of §9.2.3.1.1 to address case number identification of administrative documents
in the case file.
7. Addition of §9.2.3.2.4 to clarify responsibility of report signers to initial pages of
supporting documentation package.
8. Addition of §9.2.8 concerning policies regarding bench notes.
9. Addition of §11.2.1 concerning distribution of hardcopy and electronic manuals.
10. Addition of § 13.9 concerning individual characteristic database samples.
11. Revisions of §16.3 concerning technical/peer review of case records.12. Revisions of §21 to clarify policies related to media contacts and disclosure of
information.
13. Revision to Peer/Technical Review Form to eliminate routine forwarding to Quality
Manager.
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 3/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory ii Effective date: 2/28/2008
Revisions & Corrections
Quality Management Program – Quality Manual, Version 2.X
Effective
Date
Description Authorized by
10/8/2007 Addition of section: Summary of Changes From Previous
Version
TJS
10/8/2007 Changes to §16.3 to clarify technical/peer review practices:
revisions of §16.3.4 & §16.3.7; additions of §16.3.3.1,
§16.3.4.1-8; §16.3.5, §16.3.6, §18.3.8.1, and technical/peer
review form
TJS
10/8/2007 Revisions of page numbers. TJS
1/13/2008 Addition: §4.4 (re: type and extent of laboratory
examinations)
TJS
1/13/2008 Addition: §7.1.1 (re: minimum education requirements) TJS
1/13/2008 Revision: §9.3.3.2 (re: distribution of analytical reports) TJS1/13/2008 Addition: §10.6 (re: measurement standards TJS
1/13/2008 Addition: §14.1.1.1 (re: standards for equipment
maintenance & calibration)
TJS
1/13/2008 Various non-substantive changes in wording and formatting
to improve clairity
TJS
1/13/2008 Revisions of page numbering TJS
2/27/2008 Addition of 9.4.2 clarifying that case records are maintained
indefinitely
ELT
2/27/08 Revision of 10.6 to clarify that certain measurement
standards are verified annually against traceable standards
ELT
2/27/08 Revision of page numbering ELT
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 4/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory iii Effective date: 2/28/2008
Dallas County Institute of Forensic Sciences
Forensic Laboratory
QUALITY MANUAL
DISTRIBUTION LIST
The Quality Management Program Quality Manual is maintained as an electronic document that
is accessible to all staff through the Quality Management System Portal web page.
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 5/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 1 Effective date: 2/28/2008
Table of Contents
Section Page
1. Policy Statement and Purpose of the Laboratory.................................................................... 3
2. Objectives of the Quality Management Program ................................................................... 3
3. Purpose of the Manual ............................................................................................................ 4
4. Scope and Organization of the Forensic Laboratory .............................................................. 5
5. Quality Management Responsibilities:................................................................................... 5
6. Job Descriptions...................................................................................................................... 9
7. Educational Background and Training Records..................................................................... 9
8. Training Programs ................................................................................................................ 10
9. Case Record Management and Control ................................................................................ 12
10. Quality Assurance of Standards, Controls, and Reagents .................................................... 20
11. Procedure Manual Control and Maintenance ....................................................................... 22
12. Development, Validation, and Verification of New Testing Methods................................. 23
13. Evidence Handling................................................................................................................ 25
14. Instrument Operation, Calibration, and Maintenance........................................................... 29
15. Facility Security and Maintenance ....................................................................................... 30
16. Quality Assurance/Quality Control ...................................................................................... 31
17. Self-Critical Review and Corrective Action......................................................................... 36
18. Review of Testimony............................................................................................................ 40
19. Departure from Documented Policies and Procedures ......................................................... 41
20. Addressing Complaints......................................................................................................... 42
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 6/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 2 Effective date: 2/28/2008
21. Disclosure of Information..................................................................................................... 42
22. Reviews and Audits .............................................................................................................. 42
23. Annual Quality System Review............................................................................................ 44
Appendices
Peer Technical Review Form
Request for Review (RFR) Form
Corrective Action Request (CAR) Form
This is a non-controlled copy of a controlled document
8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 7/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 3 Effective date: 2/28/2008
Dallas County Southwestern Institute of Forensic Sciences
Forensic Laboratory
Quality Management Program
1. Policy Statement and Purpose of the Laboratory
1.1. The Forensic Laboratory of the Dallas County Southwestern Institute of Forensic
Sciences (IFS or SWIFS) is committed to serving the needs of the Dallas County
Office of the Medical Examiner, submitting agencies, and the citizens of Dallas
County by providing a broad spectrum of forensic analyses performed accurately,
impartially, and in a timely manner.
1.2. To support this commitment, a quality management program has been developed to
ensure the ongoing quality, integrity, and reliability of analyses performed, reports
generated, and testimony provided by IFS personnel. IFS staff acknowledge the
unique responsibility inherent in conducting forensic analyses and the expectation
that all work performed will be of exemplary caliber.
1.3. Ensuring a competent and accurate work product requires a personal dedication to
quality and an active participation in this quality management program by every
employee.
1.4. The components of the program include
1.4.1. quality control (QC) - activities used to monitor the quality of analytical
data and to ensure that it satisfies specified criteria such as positive and
negative controls, standards, and blanks, and1.4.2. quality assurance (QA) – planned and systematic actions necessary to
provide sufficient confidence that a laboratory’s work product satisfies
specified quality requirements, for example, peer review, proficiency
tests, instrument calibration, assay verification, reviews and audits, etc.
2. Objectives of the Quality Management Program
2.1. IFS staff support this Quality Management Program designed to provide:
2.1.1. Accurate and relevant testing procedures which are scientifically sound
and adequately documented utilizing commonly accepted instrumentationand equipment in proper working order;
2.1.2. Analytical procedures which are based upon sound scientific principles
and which have been validated as to accuracy and reliability;
2.1.3. Acceptable operational performance of procedures, critical reagents, and
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 8/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 4 Effective date: 2/28/2008
instrumentation;
2.1.4. Testimony which is truthful, complete, and impartial provided in a
professional manner;
2.1.5. Hiring and training of qualified staff with verification of acceptable
competency and provision of ongoing training and professionaldevelopment for staff as appropriate;
2.1.6. Periodic evaluation of procedures and analysts through participation in
internal and/or external proficiency testing and peer review;
2.1.7. Use of quality analytical standards of known purity and/or composition
from reputable manufacturers where available and appropriate;
2.1.8. Evidence handling processes which provide care, custody, and control of
evidence and case records;
2.1.9. Participation as applicable in the Annual Internal Review, ASCLD/LAB
Annual Accreditation Audit Report, Annual Quality System Review, and
other audits and reviews; and
2.1.10. Maintenance of ASCLD/LAB accreditation.
2.2. Due to the nature of work performed, not all aspects of this program apply to the
Breath Alcohol Section; this Program will comply with this program as applicable.
3. Purpose of the Manual
3.1. The purpose of this manual is as follows:
3.1.1. To establish a mechanism to assure that activities conducted by the
Forensic Laboratory of the Dallas County Southwestern Institute of Forensic Sciences meet the quality management objectives listed above
which are designed to ensure a quality work product,
3.1.2. To establish quality control and quality assurance processes as an integral
and necessary component in providing competent forensic analyses,
3.1.3. To communicate expected quality management activities to laboratory
staff; and
3.1.4. To ensure a consistent approach to quality management throughout the
Forensic Laboratory.
3.2. Implementation of this manual requires written authorization by the Director,Section Chiefs, and the Quality Manager.
3.3. The Quality Manual is reviewed annually by the Quality Manager.
3.3.1. The Director, Section Chiefs, and Quality Manager must approve changes
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 9/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 5 Effective date: 2/28/2008
to the Manual prior to implementation.
3.3.2. Out-dated Manuals are archived by the Quality Manager.
3.4. The Quality Manual is readily available to Forensic Laboratory staff.
3.4.1. The official copy of the Quality Manual is kept by the Quality Manager.
3.4.2. The Quality Management Program Quality Manual is maintained as an
electronic document that is accessible to all staff through the Quality
Management System Portal web page.
4. Scope and Organization of the Forensic Laboratory
4.1. The Forensic Laboratory is a division of the Dallas County Southwestern Institute of
Forensic Sciences and was established by the Dallas County Commissioners Court
in a joint effort with UT-Southwestern Medical School.
4.1.1. The Forensic Laboratory is an independent laboratory, and the Director of
the Institute reports directly to the Dallas County Commissioners Courtand the Chair of the Pathology Department of UT-Southwestern Medical
School.
4.1.1.1. With respect to operation of the Forensic Laboratory, funding,
operation and reporting responsibilities rest with the Dallas
County Commissioners Court.
4.1.2. Selected senior science staff also serve as faculty at UT - Southwestern
Medical School.
4.2. A current organizational chart is maintained by the Director.
4.3. The Laboratory operates on a fee-for-service basis, and its services are available toanyone paying the fees authorized by the Dallas County Commissioners Court
within the policies and guidelines established by the Dallas County Commissioners
Court and the Director of the Institute.
4.3.1. A list of current disciplines and sub-disciplines in the Crime Laboratory is
maintained by the Quality Manager.
4.4. Type and extent of laboratory examinations.
4.4.1. The criminal investigation laboratory performs evidence examinations and
testing in the following analytical disciplines: Firearms & Toolmarks,
Trace Evidence, and Forensic Biology (Serology & DNA), Toxicology,
and Controlled Substances.
4.4.2. The specific analyses performed by each analytical unit can be found in
the technical procedure manuals of the units.
5. Quality Management Responsibilities:
This is a non-controlled copy of a controlled document
8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 10/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 6 Effective date: 2/28/2008
5.1. Employees. Employees have the following responsibilities:
5.1.1. To actively participate in the quality management program and follow
policies and procedures outlined in this Manual, applicable procedure
manuals, and other policy and procedure documents;
5.1.2.
To diligently and accurately perform the duties of their position;5.1.3. To immediately bring to the attention of their Supervisor, Section Chief,
or Director any situation which potentially compromises the integrity of
work performed or reported by Institute personnel;
5.1.4. To perform proficiency tests in the same manner as regular casework;
5.1.5. To complete proficiency tests, peer reviews, and courtroom monitoring in
a timely manner and as applicable; and
5.1.6. To review results of QC/QA activities with Supervisor or Section Chief,
provide written comment if applicable, and implement corrective action as
necessary.
5.2. Section Chiefs. Section Chiefs have the following responsibilities:
5.2.1. To support and implement the Quality Management Program;
5.2.2. To communicate quality management policies and procedures to
employees;
5.2.3. To ensure that all personnel receive necessary training and are qualified to
perform assigned work;
5.2.4. To ensure completeness of case records and reports;
5.2.5. To ensure active and timely participation by staff in proficiency tests, peer
reviews, courtroom monitoring, and other QC/QA activities;
5.2.6. To establish criteria for acceptable performance on proficiency tests, peer
reviews, courtroom monitoring, and other QC/QA activities;
5.2.7. To approve the selection and use of analytical procedures;
5.2.8. To review and update methods and procedures;
5.2.9. To establish criteria for method and procedure validation;
5.2.10. To implement corrective action as appropriate, review QC/QA
performance with the appropriate staff, and provide written comment as
necessary to the Quality Manager;
5.2.11. To assist the Quality Manager in review and evaluation of quality
processes including the Annual Internal Review, ASCLD/LAB Annual
Accreditation Audit Report, Annual Quality System Review, and other
audits and reviews; and
5.2.12. To delegate quality management responsibilities as applicable.
This is a non-controlled copy of a controlled document
8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 11/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 7 Effective date: 2/28/2008
5.3. Quality Manager. The Quality Manager reports directly to the Director and has
primary responsibility and oversight for implementation, documentation, and
assessment of the quality management program described in this manual. The
Quality Manager has the following responsibilities:
5.3.1. To maintain and update the quality manual;
5.3.2. To monitor laboratory practices to verify continuing compliance with
policies and procedures;
5.3.3. To maintain official copies of manuals;
5.3.4. To ensure documentation of routine instrument calibration, maintenance,
and repair;
5.3.5. To periodically assess the adequacy of report review activities including
peer review; ensure that peer review and courtroom monitoring are
conducted and evaluated in a timely manner;
5.3.6. To ensure the validation of new technical procedures and instrumentation;
5.3.7. To investigate technical problems, propose remedial actions, and verify
their implementation;
5.3.8. To ensure that appropriate proficiency tests (internal and/or external) are
ordered, performed in a timely manner, and evaluated;
5.3.9. To select, train, and evaluate internal inspectors;
5.3.10. To schedule, coordinate, and conduct the Annual Internal Review,
Annual ASCLD/LAB Accreditation Audit, Annual Quality System
Review, and other audits and reviews;
5.3.11.
To maintain applicable training and educational records of laboratorypersonnel;
5.3.12. To recommend training to improve the quality of laboratory staff;
5.3.13. To oversee the Request for Review (RFR) and Corrective Action
Response (CAR) processes;
5.3.14. To maintain a current listing of employees, signatures, and initials;
5.3.15. To propose corrections and improvements in the quality system;
5.3.16. To communicate with ASCLD/LAB and the Texas Department of Public
Safety (DPS) as applicable; and
5.3.17. To delegate quality management issues as applicable.
5.4. Quality Committees
5.4.1. At the discretion of the Quality Manager, ad hoc committees and working
groups may be established to assist in maintaining and improving
laboratory quality and maintaining ASCLD/LAB accreditation. Standing
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 12/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 8 Effective date: 2/28/2008
committees include:
5.4.1.1. Executive Committee
5.4.1.1.1. Membership includes the Quality Manager, Section
Chiefs, Forensic Coordinator, and other staff as
identified by the Director.5.4.1.1.2. Duties include managing the request for review and
corrective action processes, identifying new quality
initiatives, assessing overall effectiveness and
compliance with the quality program, ensuring
applicability of quality program for all laboratories,
participation in the ASCLD/LAB Annual Accreditation
Audit Report, Annual Internal Review, Annual Quality
System Review and other audits and reviews, providing
assistance to the Quality Manager, etc.
5.4.1.1.2.1.
The Executive Committee has theresponsibility to investigate alleged incidents
of serious negligence or misconduct by staff
or subcontractors that substantially affect the
integrity of the scientific analyses performed
and reported by the Institute; to report such
incidents to the Director for review and
referral to the accrediting bodies, the Texas
Department of Public Safety, the Dallas
County District Attorney’s Office, and other
agencies as appropriate.
5.4.1.2. Institute Quality Committee
5.4.1.2.1. Membership includes Quality Manager, Section Chiefs,
Supervisors, one analyst from each laboratory, EHS
Manager, Deputy EHS Manager, and other staff as
identified by the Director.
5.4.1.2.2. Duties include identification of quality related issues
requiring action, implementation of new quality
initiatives, dissemination of quality related information
to respective laboratories, participation in proposing
changes to the Quality program, etc.
5.5. Director. The Director has the following responsibilities:
5.5.1. To ensure an active quality management program within the Forensic
Laboratory, investigate concerns regarding QC/QA processes that are
brought to his attention, and review QC/QA reports prepared by the
Quality Manager;
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 13/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 9 Effective date: 2/28/2008
5.5.2. To support and promote implementation of the quality management
program;
5.5.3. To review and respond as applicable to the Annual Accreditation Audit
and Annual Quality System Review;
5.5.4.
To seek adequate funding to maintain a quality laboratory operation;5.5.5. To identify a Quality Manager to oversee implementation of the quality
management program;
5.5.6. To resolve disputed quality issues;
5.5.7. To delegate quality management responsibilities as applicable.
5.5.8. To review allegations received from the Executive Committee of serious
negligence or misconduct by staff or subcontractors that substantially
affects the integrity of the scientific analyses performed and reported by
the Institute; when warranted, to refer such allegations to accrediting
bodies, the Texas Department of Public Safety, the Dallas County District
Attorney’s Office, and other agencies as appropriate.
5.6. Suggestions for improving the Quality Management Program can be made to the
Quality Manager, Section Chief, and/or Director.
6. Job Descriptions
6.1. The Director maintains currently available job descriptions of employees in the
Forensic Laboratory which have been approved by the Dallas County
Commissioners Court.
6.2.
The Director may approve use of a more detailed statement of job functions, asnecessary.
7. Educational Background and Training Records
7.1. The educational background of each Laboratory employee at in-hire is documented
on the Dallas County employment application and/or in-hire curriculum vitae which
are maintained by the Director.
7.1.1. The minimum educational requirements for each laboratory position are
established in accordance with applicable accreditation standards
(ASCLD-LAB) and Dallas County employment policies, and are
documented on the official Dallas County job description for each
position.
7.2. Documentation of job prerequisites, such as academic degrees or specific course
work, may be required; failure to provide this documentation may result in
disciplinary action including termination in accordance with Dallas County policies.
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 14/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 10 Effective date: 2/28/2008
7.3. Each analyst will develop a curriculum vitae, resume, or statement of qualifications
summarizing education, training, publications, presentations, and other pertinent
information which is maintained by the Quality Manager.
7.3.1. This resume is updated annually as necessary by the analyst and under the
direction of the Quality Manager.
7.3.2. It is the employee’s responsibility to provide the Quality Manager with
documentation of all educational and/or training experiences related to the
employee’s job duties at the Institute.
7.4. The Quality Manager is responsible for maintaining the following portions of the
employee’s personnel file: documentation of academic degree and/or other
educational or training requirements, training records, current resume, and
competency testing documentation.
7.4.1. Only the current version of an employee’s resume is kept.
8. Training Programs
8.1. Professional Training
8.1.1. Employees must receive appropriate training prior to conducting
independent casework.
8.1.2. Training programs are developed under the direction of the appropriate
Section Chief and reviewed by the Quality Manager.
8.1.3. The Quality Manager is the official custodian of training records.
8.1.4. The purpose of the training program is to ensure that each trainee
demonstrates a basic proficiency in the following as applicable:8.1.4.1. applicable methods used by the Laboratory,
8.1.4.2. academic basis for methods used,
8.1.4.3. the use and basic troubleshooting of equipment,
8.1.4.4. the general theory of the analytical techniques and
instrumentation,
8.1.4.5. evidence handling,
8.1.4.6. expectations of a forensic examiner,
8.1.4.7.
skills of testimony, and8.1.4.8. other components of the job duties.
8.1.5. The training program is utilized for
8.1.5.1. training new employees prior to conducting casework,
8.1.5.2. training current employees who are newly assigned or
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 15/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 11 Effective date: 2/28/2008
reassigned, and
8.1.5.3. retraining of current employees as needed.
8.1.6. Competency testing is an integral part of a training program and should
include evaluation of knowledge of appropriate literature, examination
and identification of known and unknown materials, written and/or oralexamination, and moot court as applicable.
8.1.6.1. Competency testing protocols are a part of the training program
within each Section, and the areas for demonstration of
competency are covered in the training manual.
8.1.6.2. Competency test results are reviewed by the Section Chief and
forwarded to the Quality Manager for review.
8.1.6.3. Once competency is established, acknowledgement of successful
completion is included in the training documents held by the
Quality Manager. Individual test results are not required to be
kept as long as the specific areas covered are included in thetraining manual, check list, or other related document.
8.1.7. Regardless of academic qualifications or prior employment, new
employees and current employees who are reassigned or newly assigned
must successfully demonstrate competency in each applicable area of
examination prior to performing independent case-connected
examinations.
8.1.8. When an employee requires retraining, the Section Chief, Supervisor, and
Quality Manager will determine the appropriate portions of the training
program to be completed. Independent casework in the designated
training area may not be performed during a retraining period.
8.2. Continuing Education and Ongoing Training
8.2.1. It is important that analysts maintain technical qualifications through
participation in continuing education and/or training programs.
8.2.1.1. Continuing education and training activities must be documented
and may include reading current scientific literature,
participation in educational lab meetings, and/or attending
seminars, courses, professional meetings, training sessions
and/or classes in relevant subject areas.8.2.2. The Director and Section Chief determine appropriate use of training
funds and training resources.
8.2.2.1. Funding for training and continuing education is made available
by the Dallas County Commissioners Court during the annual
budget process.
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 16/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 12 Effective date: 2/28/2008
8.2.2.2. Employees may request training by providing a written request
to their Section Chief.
8.2.2.3. Supervisors may also identify and recommend appropriate
training opportunities for staff.
8.2.2.4.
The Quality Manager may recommend training.8.2.2.5. Training requests are evaluated based upon history of previous
training, need of the individual and Institute, availability and
location of training, employee performance, availability of funds,
recommendation of the Quality Manager, and/or other applicable
criteria.
8.2.3. The Quality Manager maintains documentation of continuing education
and training activities.
8.2.3.1. Training activities are included as a part of the employee’s
annual resume update.
8.3. Environmental Health and Safety Training
8.3.1. It is the responsibility of each employee to attend environmental, health,
and safety training.
8.3.2. Details of the safety training program may be found in the Institute of
Forensic Sciences Environmental Health and Safety Manual.
8.3.3. It is the responsibility of each employee to bring safety concerns
immediately to the attention of their supervisor.
9. Case Record Management and Control
9.1. Definitions
9.1.1. Case Record (Case File) – Files containing administrative and
examination documentation generated or received by a laboratory
pertaining to a particular case and used in reaching the conclusions
reported.
9.1.1.1. Administrative Documentation – Non-technical or non-analytical
records such as case related conversations, evidence receipts,
request/submission forms, description of evidence packaging and
seals, subpoenas, correspondence, investigative reports, peer
review documentation, case reports, and other related
information.
9.1.1.2. Examination Documentation – Technical and analytical records
such as notes, reference to procedures followed, tests conducted,
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 17/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 13 Effective date: 2/28/2008
standards and controls used, data, worksheets, instrument
output/chromatograms, spectra, graphs, sketches, diagrams,
printouts, photographs, observations and results of examinations,
and other related information.
9.1.1.2.1. Notes – The documentation of procedures, standards,
controls and instruments used, observations made,results of tests performed, charts, graphs, photos, and
other documents generated which are used to support
the examiner’s conclusions.
9.1.2. Records Custodian (Custodian of Records) – Individual(s) designated by
the Section Chief with responsibility for maintaining care, custody, and
control of case records including but not limited to
9.1.2.1. Institute Custodian of Records – Director
9.1.2.2. Custodian of Records for Section – applicable Section Chief and
Deputy Section Chief 9.1.2.3. Custodian of Records for a Laboratory – applicable Supervisor
9.1.2.4. Deputy Custodian of Records for Section or a Laboratory –
applicable Evidence Registrar(s), applicable Senior Analysts,
and others as designated by Section Chief. Analysts are Deputy
Custodians of Records for cases in which they performed work.
9.2. Preparation of Case Records
9.2.1. The case record, i.e. case file, should contain adequate information so that
another competent analyst or supervisor can independently evaluate and
interpret the data.
9.2.2. The Laboratory maintains case documentation in a case file denoted by a
unique laboratory case number.
9.2.2.1. Case numbers include a letter designator specific to a particular
laboratory or Section: P (Physical Evidence), C (Drug Analysis
Laboratory), M or no letter designation (Medical Examiner
Toxicology), D (DWI/DUID Toxicology), H (Other
Toxicology), B (Breath Alcohol).
9.2.2.2. Case numbers include a year designator.
9.2.2.3. Case numbers within a specific year and letter combination are
assigned sequentially.
9.2.2.4. Examples include 98C1234, 03P0011, etc. Medical Examiner
cases may be designated as 03M1234 or 1234-03 to allow for
historical numbering in the Office of the Medical Examiner.
9.2.3. Case records must be identified.
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 18/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 14 Effective date: 2/28/2008
9.2.3.1. Administrative Documentation –
9.2.3.1.1. The case number must appear on the first page of an
administrative document packet; multi-page
administrative documents which are bound together
may be identified by placing a case number on the front
page of the packet.
9.2.3.1.2. It is recommended that all pages of administrative
documentation are marked with the case number.
9.2.3.1.3. All pages of the case report must be signed or initialed
by the appropriate analyst.
9.2.3.2. Examination Documentation –
9.2.3.2.1. The laboratory case number and analyst’s signature
and/or initials must appear on each page of the
examination documentation.
9.2.3.2.2. It is acceptable for the laboratory case number to be
printed by an analytical instrument; the analyst’s
initials and/or signature must be handwritten.
9.2.3.2.3. When examination documentation is prepared by a
trainee or individual other than the one(s) with
responsibility for interpretation of the findings,
reporting of results, and/or testimony concerning the
documentation, both individuals must sign or initial
each page of the documentation.
9.2.3.2.4. The signer(s) of reports must initial each page of the
examination documentation package.
9.2.3.2.5. If an individual other than a signer of the report is
called to testify regarding a case report, the individual
must review the case file prior to testimony and sign or
initial each page of the documentation.
9.2.4. Entries into the case record must be made at or near the time of
occurrence.
9.2.4.1. Dates must be recorded throughout the case documentation to
indicate when work was performed.
9.2.5. All case records must be permanent in nature.
9.2.5.1. Where records or work product are inherently unstable, some
type of permanent record should be made as appropriate - for
example, thermal paper which fades over time should be copied,
photographs can be made, etc.
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 19/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 15 Effective date: 2/28/2008
9.2.5.2. Manual entries onto case records must be in ink, not pencil,
unless specific applications are required by procedures.
9.2.5.2.1. It is recommended that manual entries are made in blue
or other non-black ink to assist in distinguishing
between photocopies and original documents.
9.2.5.3. Nothing in the examination documentation may be obliterated or
erased. Corrections, changes, alterations, and additional
notations made in examination documentation must be initialed
by the individual making the change or addition.
9.2.5.3.1. Correction fluids like White-Out cannot be used.
9.2.5.3.2. “Post-it” type notes are not recommended and, if used,
must be taped securely to prevent accidental loss.
9.2.6. Original records are included in the case file where possible.
9.2.6.1. When batch instrument reports are generated, a copy of the
instrument report may be included in the individual case files,
and the original instrument report must be maintained in a
designated location.
9.2.6.2. Staff generated paperwork such as work lists may be
photocopied and initialed by staff.
9.2.6.3. By initialing, staff attests that photocopied paperwork is an exact
duplicate of the original and as such is considered equivalent to
the original.
9.2.6.4. Original casework which cannot reasonably be included in a case
file, may be stored in a designated location with appropriatenotation made in the case file or procedure.
9.2.6.5. “Original records” are the hard copy materials contained in the
case file or other designated location. Original case records may
be originally generated by computer but are not stored or
archived permanently in this manner.
9.2.7. Abbreviations and symbols may be used within the case record provided
that their meaning is readily comprehensible to a knowledgeable reviewer.
9.2.7.1. Scientifically accepted abbreviations and symbols may be used
without further explanation.
9.2.7.2. Other abbreviations and symbols must be documented in
laboratory procedures or other laboratory manuals.
9.2.8. Bench notes
9.2.8.1. Bench notes are original records made contemporaneously with
laboratory testing that describe observations, results and
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 20/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 16 Effective date: 2/28/2008
measurements that are integral to the examination and data
collection process. Bench notes are a type of raw data that
document processes and are utilized in forming final
conclusions.
9.2.8.2. Bench notes may take the following forms: handwritten entries
on designated forms and worksheets; handwritten notes onpaper; electronic forms and worksheets.
9.2.8.2.1. Electronic forms and worksheets are considered bench
notes only if completed contemporaneously with the
examination, and without an intermediate handwritten
record.
9.2.8.3. Bench notes must be legible and understandable to another
qualified examiner.
9.2.8.3.1. The use of personal abbreviations and short-hand
notations is not permitted.
9.2.8.3.2. Laboratory approved abbreviations/short-hand
notations may be used if they have been documented in
a procedure manual or other laboratory manual.
9.2.8.3.3. Personal abbreviations/short-hand notations may be
used if an explanation has been provided on the actual
bench notes.
9.2.8.3.4. Handwritten bench notes must be written with a pen,
not a pencil.
9.2.8.3.4.1. It is recommended that blue ink be used rather
than black in order to easily distinguish between
original documents and photocopies.
9.2.8.3.4.2. Additional color coded notations may be used
when appropriate.
9.2.8.3.5. Laboratories are encouraged to design and utilize
appropriate worksheets for the recording of handwritten
bench notes.
9.2.8.3.6. The use of scratch paper (e.g., Post-it notes, envelopes,
napkins, paper towels) is greatly discouraged. Scratch
paper should only be used under exceptional
circumstances beyond the control of the analyst, and
are considered bench notes
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 21/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 17 Effective date: 2/28/2008
9.2.8.4. Bench notes are part of the examination record and must be
retained in the official case file.
9.2.8.4.1. The original version of all handwritten bench notes is
retained in the case file as part of the supporting
documentation package for individual reports.
9.2.8.4.2. If scratch paper is used for making notes due to
exceptional circumstances, then the scratch paper must
be taped to standard 8½” x 11” paper for retention in
the case file.
9.2.8.4.3. If the original bench notes cannot be retained due to
some extenuating circumstances such as contamination
by a biological material, then the bench notes will be
placed in clear plastic and photocopied. The examiner
will verify that the copy is complete, accurate and
legible; and will make a notation that the copy is beingretained in lieu of the original. The photocopy will
then be retained. The original will be disposed of
appropriately.
9.2.8.4.4. Under some circumstances it may be necessary for the
sake of clarity to rewrite an entire sheet of bench notes.
9.2.8.4.4.1. In this situation, the entire original sheet must
be struck through and initialed, and a note
should be added to the struck-through sheetto indicate that the corrections are on a
separate sheet.
9.2.8.4.4.2. The new form or note should be marked to
indicate that it is a corrected sheet.
9.2.8.4.4.3. The original struck-through bench notes must
be retained.
9.2.8.4.5. A printout of electronic bench notes is retained as the
official case record in the hardcopy case file.
9.2.8.4.5.1. The electronic document is not considered an
official case record, and is not retained.
9.3. Report Generation
9.3.1. Laboratory reports are written and reviewed by the applicable analyst(s)
This is a non-controlled copy of a controlled document
8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 22/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 18 Effective date: 2/28/2008
and/or supervisor(s).
9.3.2. Results and conclusions must be fully supported by data in the case file.
9.3.3. The specific content of reports and the mechanism of report distribution
are specified by each Laboratory.
9.3.3.1. At a minimum, reports include identity of the examininglaboratory, case identifier, date of receipt, date of the report,
identity of the submitter, items analyzed, results and/or
conclusions, signature of the person(s) accepting responsibility
for the content of the report.
9.3.3.2. A copy of the final report is sent to the agency or individual
requesting the analysis. In criminal cases this will typically be
the investigating agency.
9.3.3.2.1. As appropriate to particular case circumstances, copies
of the final report may be sent to prosecutors assigned
to the case, or to other individuals authorized by therequesting agency/individual or by court order.
9.3.3.2.2. Under some circumstances reports may be released in
accordance with state law regarding government open
records.
9.3.3.3. Distribution of reports to other entities is noted in the case
record.
9.3.3.4. Additions or corrections to final reports are included in the case
file. They are appropriately marked (“Corrected Report,”
“Supplemental Report,” “Amended Report,” etc.), and copies are
provided to all entities receiving the original report.
9.3.3.4.1. Corrected Report – A report in which a change is made
to correct an error in the written portion of the original
report.
9.3.3.4.2. Supplemental and Amended Reports – Reports
detailing either a) new information not covered on the
original report and in which findings from the original
report are not repeated, or b) new testing information
not covered on the original report in combination with
a repetition of the original report contents.
9.3.3.5. A copy of all corrected reports is sent to the Quality Manager for
review. The Quality Manager determines if an RFR should be
initiated.
9.3.4. In some areas the report is routinely signed by more than one analyst,
usually one primary analyst and one reviewing analyst. If the two signing
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 23/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 19 Effective date: 2/28/2008
analysts cannot agree on the content of the report, it is their responsibility
to bring this situation immediately to the supervisor. The supervisor will
review the situation and attempts to resolve the disagreement by various
means which may include seeking consensus and/or reanalysis. If
resolution still cannot be reached, the Section Chief is advised. The
Section Chief then reviews the situation and offers suggestions forresolution. If consensus cannot be reached, it is ultimately the
responsibility of the Section Chief to determine the final course of action
which may include reassigning the case, reanalysis, and/or issuing and
signing the case report.
9.4. Case Record Storage, Security, and Disposition
9.4.1. The original contents of the case file must remain at the Institute, in the
possession of Institute personnel, or under direction of the Dallas County
Records Manager.
9.4.1.1. When it is determined that case reports and other records should
be released or provided in court proceedings, only a copy of applicable case contents may be provided.
9.4.1.2. Case records may be maintained on-site at the Institute or off-
site under the direction of the Dallas County Records Manager.
9.4.2. Case records are not disposed but are maintained indefinitely.
9.4.3. Case records are stored in secure areas inaccessible to the general public.
9.4.4. Proficiency tests and other quality assurance tests may receive a case
number; however, proficiency case records are maintained by the Quality
Manager.
9.4.5. Case records are maintained in accordance with Dallas County policy as
implemented by the Dallas County Records Manager.
9.5. Release of Case Records and Case Information
9.5.1. Work performed by the Forensic Laboratory is provided on a fee-for-
service basis. The agency or entity purchasing the services is the owner
of the work product.
9.5.2. Typically case results are provided to the submitting agency and/or their
designee or in response to proper legal direction.
9.5.3. Requests for disclosure of case related information falling outside routine
release practices are directed to the submitting agency and/or submitted tothe Civil Section of the Dallas County District Attorney’s Office for
review and direction. This may include responses to subpoenas, court
orders, freedom of information requests and other inquiries.
9.5.3.1. When the Office of the Medical Examiner (OME) is the
submitting agency, requests to release information must follow
This is a non-controlled copy of a controlled document
8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 24/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 20 Effective date: 2/28/2008
direction established by OME and/or be reviewed by the OME
prior to release.
9.5.3.2. Requests to release information submitted by other Dallas
County Departments must be reviewed by the Civil Section of
the Dallas County District Attorney’s Office prior to action.
10. Quality Assurance of Standards, Controls, and Reagents
10.1. Definitions
10.1.1. Critical Reagent - Reagent for which small changes in concentration or
activity of ingredients will produce significant changes in assay outcome.
10.1.2. Standard or Reference Standard – A preparation which has known
concentration and/or physical or chemical composition used for the
purpose of calibrating equipment and/or as an experimental control.
10.1.3. Control – A standard of comparison for verifying or checking the findingof an experiment. Positive controls verify the presence of analytes or
conditions; negative controls verify the absence of analytes or conditions.
10.2. Reagent Labels
10.2.1. Prepared reagents must be labeled with the identity of the reagent and the
date of preparation or lot number.
10.2.2. Special storage and handling requirements and expiration dates should
also be noted on the label if applicable.
10.3. Reagent Log
10.3.1. A record must be kept of reagent preparation including the individualpreparing the reagent and that it was tested and worked as expected.
10.3.2. Records may include other information such as how the reagent was
prepared, lot number, chemical form of the ingredients, etc.
10.4. Critical Reagents
10.4.1. Critical reagents must be of acceptable quality for the intended purpose
and of known purity and chemical form.
10.4.2. A log must be kept of all critical reagents prepared including the name of
the reagent, initials of preparing analyst, date prepared, lot number of
principal component(s), and a notation that the reagent worked asexpected. Method of preparation should be included if not covered
elsewhere, such as the procedure manual.
10.4.3. Details of critical reagents prepared and used only in a single analysis
may be included in the appropriate case file.
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 25/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 21 Effective date: 2/28/2008
10.4.4. Critical reagents are identified in procedure manuals.
10.5. Standards
10.5.1. Standards should be obtained from reputable suppliers and be of known
purity and/or chemical or physical composition.
10.5.2. A certificate of analysis will serve to establish the quality of a chemicalstandard and should be obtained from the chemical supplier where
possible. When a certificate of analysis is not available from the
manufacturer, standard composition should be verified internally by an
applicable analytical technique.
10.5.2.1. A log must be kept of all standard solutions prepared including
the name of the standard, the initials of preparing analyst, date of
preparation, method of preparation, and lot number.
10.5.2.2. Newly prepared standard solutions must meet quality control
criteria established by each laboratory to ensure proper response.
10.6. Measurement Standards
10.6.1. Critical measurements will be made using calibrated devices traceable to
NIST or other appropriate standards.
10.6.2. The following devices are verified against NIST-traceable standards at
least once per year:
10.6.2.1. Weights
10.6.2.2. Pipetters
10.6.2.3. Balances
10.6.2.4. Ruler for barrel length
10.6.2.5. Gauge blocks
10.6.2.6. Stage micrometer
10.6.2.7. Calipers
10.6.2.8. Thermometers
10.6.3. The records of yearly calibration checks are maintained by the Quality
Manager.
10.6.4. Other measurement standards and devices specific to particular analytical
units are defined in the technical procedures of those units.10.7. Controls
10.7.1. As applicable, controls, positive and negative, are analyzed on a routine
basis according to quality control procedures established by each
laboratory.
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 26/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 22 Effective date: 2/28/2008
10.7.2. Acceptable response of controls is further verification that the assay -
including reagents and standards - is functioning properly.
11. Procedure Manual Control and Maintenance
11.1. The types of examinations conducted at the Institute are listed in the proceduremanual for each laboratory.
11.2. All procedures routinely used by a laboratory are written and readily available to
analysts in that laboratory.
11.2.1. Procedure manuals are maintained either as hardcopy documents, or as
electronic documents
11.2.1.1. For hardcopy procedure manuals, the official manual is
maintained by the Quality Manager, and duplicate copies are
distributed to functional units as required.
11.2.1.2. For electronic procedure manuals, the official manual is theelectronic version accessed through the Quality Management
System Portal web page.
11.3. Components of Technical Procedures - As appropriate, procedures will include
assay title, principle and/or scope, equipment used, use and preparation of reagents
and controls and standards, assay specific instrument parameters, analytical
procedures, calculations, corrective action, interferences and other possible sources
of error, interpretation and reporting guidelines, safety precautions, references, date
of implementation, and other relevant information.
11.4. Revision of Procedures
11.4.1. Administrative revisions to procedures, including typographical errors orclarification of language, typically do not require additional validation.
11.4.2. Material technical revisions to procedures require additional validation.
11.4.3. Revisions and corrections to procedures are summarized in the front of
each manual including effective date of revision, description of the
change, and initials of individual authorizing the change.
11.4.4. Revisions may be made by memo or by updating procedures; the effective
date of implementation must be noted.
11.4.5. Prior to implementation of a revision, the update must be approved by the
Supervisor and Section Chief and reviewed by all applicable analysts andthe Quality Manager.
11.4.6. Archived procedures are maintained by the Quality Manager.
11.4.7. Out-dated procedures are immediately removed from general
accessibility.
This is a non-controlled copy of a controlled document
8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 27/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 23 Effective date: 2/28/2008
11.5. Implementation of New Procedures
11.5.1. New procedures must be properly validated prior to implementation.
11.5.2. The written procedure must be reviewed by all applicable analysts and the
Quality Manager and approved by the appropriate Section Chief and
Supervisor. The effective date of implementation must be noted on theprocedure.
11.5.3. Out-dated procedures must be removed from the procedure manual and
archived by the Quality Manager for future reference.
11.6. Procedure manuals are approved annually by the applicable Section Chief.
11.7. The Quality Manager maintains the official copy of each procedure manual.
12. Development, Validation, and Verification of New Testing Methods
12.1. For purposes of this section, “new testing method” is used in a broad sense to
include new or revised testing procedures or techniques, new or upgradedinstruments or equipment, and/or non-administrative changes to existing written
procedures. For example changing the manufacturer of a GC column (DB1 to HP1)
is considered an administrative change; changing from one type of GC column to
another (DB1 to DB5) requires validation.
12.2. All new testing methods - including material modifications to existing procedures –
must be validated after development and prior to use in casework.
12.2.1. Method development is the experimental process of devising, revising, or
applying a new method for routine use. The end process of method
development is a proposed method which must be validated prior to
routine implementation in the laboratory.
12.2.2. Method validation is the process of testing an analytical method,
technique, or instrument to determine its suitability for meeting its
intended purpose and to document its reliability under expected conditions
of use. Generally the validation process is expected to
12.2.2.1. Evaluate whether a new testing method meets identified
analytical needs and current scientific practices;
12.2.2.2. Compare the new test method’s performance with existing
laboratory methodology;
12.2.2.3. Describe the conditions under which a testing method willproduce valid results;
12.2.2.4. Predict possible sources of error;
12.2.2.5. Determine limitations of a testing method; and
12.2.2.6. Establish baseline characteristics of the testing method (linearity,
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 28/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 24 Effective date: 2/28/2008
accuracy, etc.) which serve as benchmarks to evaluate future
method performance.
12.3. Validation Process
12.3.1. The validation process is performed after method development and once a
proposed testing method has been finalized.12.3.1.1. The validation process may identify the need to make changes in
the testing method being validated. In this case, the modified
testing method must undergo validation.
12.3.2. A written procedure, validation plan, and proposed timetable are
developed prior to beginning the validation process and are submitted by
the supervisor or Section Chief to the Quality Manager for approval.
12.3.2.1. The complexity and comprehensiveness of the validation process
should be consistent with the magnitude of proposed testing
method changes. The validation plan is based upon the
following:
12.3.2.1.1. The type of method, technique, or analytical instrument
or equipment being validated.
12.3.2.1.2. The complexity of the new testing method and whether
it is a minor modification of an existing assay, major
modification of an existing assay, or development of a
new assay or technique.
12.3.2.1.3. The Laboratory’s experience and familiarity with
similar methods, techniques, or analytical instruments
or equipment.
12.3.2.2. Method validation must include the testing of known samples.
12.3.2.2.1. To the extent possible, known samples should resemble
actual specimens to allow evaluation of matrix effects,
specimen aging, specimen degradation, and sample
homogeneity.
12.3.2.2.2. Known samples may be obtained internally (for
example, split samples), externally (for example,
reference samples), collaboratively (for example,
exchange of blind or reference samples with another
competent laboratory).12.3.2.3. Where applicable, old and new methods should be run in parallel
on split samples and results compared.
12.3.2.4. Validation of quantitative methods should include an assessment
of accuracy and precision at concentrations expected in case
work.
This is a non-controlled copy of a controlled document
8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 29/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 25 Effective date: 2/28/2008
12.3.3. At the conclusion of the validation study, a validation report is generated,
reviewed/approved by the Supervisor and Section Chief, and submitted to
the Quality Manager for review.
12.3.3.1. The validation report contains a copy of the validated method, a
compilation of specific validation results, summary of validation
parameters identified in the validation plan, a discussion of method applicability and possible limitations, the date of method
implementation, etc.
12.3.3.2. The Quality Manager retains the original validation plan and
validation report.
12.3.3.3. Once the validation report is reviewed by the Quality Manager,
instrumental records may be discarded provided that the results
are adequately summarized in the validation report.
12.3.4. The Quality Manager places the new or revised procedure in the official
procedure manual.12.3.5. The Supervisor ensures that the new procedure is released for routine
work, and that training, as needed, is conducted. The Supervisor ensures
that any outdated procedure is immediately removed from use.
13. Evidence Handling
13.1. Procedures. Each Section or Laboratory specifies procedures for proper submission,
packaging, documentation, preservation, storage, and release of evidence.
13.2. Evidence Seals - Where feasible, all evidence is stored in a sealed condition.
13.2.1. A container is properly sealed when the container is secured in apermanent manner to prevent undetected access to the contents, when its
contents cannot readily escape, and when its contents are not subject to
external contamination.
13.2.2. The seal must be marked with an identifying mark or the initials of the
person sealing the evidence.
13.2.3. Ideally, evidence which is delivered in person and is not properly sealed
will be properly sealed by the submitter prior to receipt by the Evidence
Registrar.
13.2.4.
It is the responsibility of the Evidence Registrar or other individualreceiving evidence to ensure that all evidence accepted by the laboratory
is stored under proper seal and to repackage and/or seal evidence as
necessary.
13.2.5. Items of evidence which are impractical, inappropriate, or too large to be
placed in a sealed container are marked or identified in a permanent
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 30/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 26 Effective date: 2/28/2008
manner for future identification. Markings may be made using indelible
pens/markers, permanent tags, engraving, or using unique numbers
permanently affixed to the item such as serial numbers.
13.2.6. Evidence which is packaged in a manner that may affect the ability of the
Laboratory to analyze it should be repackaged properly.
13.2.6.1. Ideally repackaging should be performed by the submitting
agency prior to submission to the Laboratory when possible.
13.2.7. If evidence can only be recorded or collected by photograph – for example
with an impression – the image or photograph must be recoverable from a
computer otherwise a print or negative must be treated as evidence.
13.3. Evidence Receipt
13.3.1. Evidence may be submitted in person, by mail, by package delivery
service, by lock-box, or other method.
13.3.2. Evidence is stored in a manner and environment that preserves the
integrity of the evidence to the extent possible.
13.3.3. Case Numbering
13.3.3.1. Each case is assigned a unique case number which is placed on
the outside of each evidence container.
13.3.3.2. Item numbers may also be assigned and placed on the outside of
evidence containers.
13.3.4. As applicable, evidence is logged into a computer tracking system.
13.4. Chain of Custody – Each evidence transfer must be acknowledged at the time that
the evidence is transferred.13.4.1. Transfer of evidence between individuals must be acknowledged by both
parties at the time of evidence transfer.
13.4.2. Transfer of evidence between an individual and a primary evidence
storage area must be acknowledged at the time of evidence transfer.
13.4.3. Evidence located in a personal evidence storage locker is deemed to be in
the personal possession of the locker assignee; therefore, documentation
of chain of custody between a personal evidence locker and the locker
assignee is not required.
13.4.4. Location of evidence in a primary evidence storage area or in the
possession of an authorized Evidence Registrar or other individual with
authorized access to the primary evidence storage area is deemed to be
one and the same for purposes of evidence tracking. Therefore, transfer of
evidence among these authorized entities is not required during the
performance of routine Evidence Registration duties.
This is a non-controlled copy of a controlled document
8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 31/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 27 Effective date: 2/28/2008
13.4.5. Electronic tracking of chain of custody is acceptable as long as the
computerized data is reasonably secure, accessible, and able to be
committed to hard copy when needed.
13.4.5.1. Individual, secure personal identifiers are acceptable in lieu of
personal signatures.
13.4.6. In Texas, legal precedent establishes that chain of custody within the
laboratory goes to the weight of the evidence and not to its admissibility:
13.4.6.1. Norris vs. Texas, 507 S.W. 2d 796 (Tx. Cr. App. 1974) – “Where testimony
established chain of custody up to point that heroin was delivered to criminal
investigation laboratory, testimony by employee of the laboratory that he
received the exhibits in question from officers of the police department for
laboratory analysis, logged them in, and turned them over to a chemist for
analysis was sufficient to establish the chain of custody and any objection to
absence of chemist as a witness to testify as to receiving the exhibits went
only to the weight of that evidence and not to its admissibility.”
13.4.6.2. Medellin vs. State 617 S.W. 2d 229 (Tx. Cr. App. 1981) – “The chain of
custody was completed to inside the laboratory, thus any further objectiongoes to the weight of evidence, rather than to its admissibility.”
13.4.6.3. Bueno vs. State 677 S.W. 2d 261 (Tx. App. 13 Dist. 1984) – “Once the chain
of custody is completed to inside the laboratory any further objection goes to
the weight of the testimony rather than to its admissibility.”
13.5. Evidence Identification
13.5.1. Institute staff inventory and mark evidence as outlined in applicable
laboratory procedures.
13.5.2. Evidence or the evidence container must be marked with a unique
identifier such as a laboratory case number.
13.5.3. When a case consists of multiple items of evidence, the individual items
or samples analyzed or examined must be marked with a unique item
designator.
13.5.3.1. Evidence should be adequately marked to ensure that it can be
identified and to aid in ensuring the integrity of case evidence.
13.5.3.2. In some cases, evidence cannot be marked because marking will
alter its evidentiary or intrinsic value.
13.5.3.2.1. This evidence must be identified by some other means
such as placing a permanent tag, placing in a sealed
secondary container, etc.
13.5.4. Significant discrepancies or variations between a submitter’s description
of evidence and that of the examiner are noted; the submitting agency is
notified as outlined in procedures of the specific laboratories or sections.
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 32/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 28 Effective date: 2/28/2008
13.6. Evidence Security
13.6.1. Evidence received into the Laboratory is maintained in a secure manner at
all times; this may include the personal possession of the examiner or
evidence registrar, a designated personal secure storage area, a primary
evidence storage area, a secure refrigerator, a restricted area with access
limited to authorized staff, or similar area.
13.6.1.1. A restricted or limited-access area is accessible to staff who have
been authorized by the Director (permanent assignment) or
Section Chief (temporary assignment) and given a key to the
area.
13.6.1.1.1. Restricted or limited-access areas are locked when not
attended by authorized staff.
13.6.1.1.2. Unauthorized individuals are allowed in a restricted or
limited-access area only if escorted by authorized
personnel or in an emergency documented in the GrandMaster Key Log.
13.6.1.1.3. Assignment of keys is documented in the Institute Key
Log or on sign-out sheets under the direction of a
Section Chief.
13.6.1.1.4. Some areas are controlled both by key and by security
code.
13.6.1.1.4.1. Staff assigned a key and security code are
authorized unrestricted access to that area.
13.6.1.1.4.2. Staff assigned only a key are authorized
access only when staff noted in 13.6.1.1.4.1
are present in the building; typically routine
business hours.
13.7. In-Process Evidence
13.7.1. Evidence in the process of examination may be stored unsealed in a secure
area with limited access.
13.7.2. At all times, in-process evidence must be protected from loss, cross-
transfer, contamination and/or deleterious change.
13.7.3. Evidence must be properly sealed in a timely fashion once examination or
analysis is complete even if the evidence is stored in a personal evidencelocker.
13.7.3.1. Because it is common to receive additional testing requests in
Toxicology after production of the initial report, the Laboratory
has determined that evidence will be sealed within one month of
case completion.
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 33/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 29 Effective date: 2/28/2008
13.8. Evidence Release
13.8.1. The examiner reseals the evidence, initials (or otherwise marks) the seal
for later identification, and returns evidence to Evidence Registration.
13.8.2. The Evidence Registrar prepares evidence for disposition and notifies the
submitter that the evidence is available for release if appropriate.13.8.3. Evidence is released to the submitting agency in person, by mail, or by
package delivery; placed in long term storage; or disposed as outlined in
specific procedures for each section.
13.8.3.1. Transfer of evidence to long term storage or disposal of evidence
is tracked using appropriate chain of custody.
13.8.3.2. Release of evidence to the submitting agency is documented
using appropriate chain of custody.
13.8.4. Evidence may only be released to the submitting agency or an entity
approved by the submitting agency or in response to subpoena or other
legal procedure.
13.8.5. If the agent present to receive evidence is not known by the IFS employee,
then the IFS employee must require verification of the identity and
affiliation of the representative prior to releasing evidence.
13.8.6. If a submitting agency does not respond to notification that evidence is
ready for release, the Evidence Registrar may send evidence to the
submitter via mail or package delivery service per procedures identified
by each section.
13.9. Individual Characteristic Database Samples
13.9.1. The laboratory tests the following evidence sample types for inclusion inindividual characteristic databases:
13.9.1.1. Questioned and exemplar biological samples (for CODIS
databases)
13.9.1.2. Questioned cartridge cases (for NIBIN databases)
13.9.1.3. Exemplar cartridge cases generated from submitted firearms (for
NIBIN databases)
13.9.2. Samples processed for inclusion in individual characteristic databases are
handled in the same manner as any other evidence item.
14. Instrument Operation, Calibration, and Maintenance
14.1. Instrumentation is calibrated and maintained, as appropriate, to ensure that the
instrument/equipment remains in proper working order.
This is a non-controlled copy of a controlled document
8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 34/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 30 Effective date: 2/28/2008
14.1.1. Analytical instrumentation and equipment that have an effect on the
accuracy or validity of casework are routinely checked with applicable
reference measurement standards - for example, proper operation of a
GC/MS is usually verified using perfluorotributylamine (FC-43 or
PFTBA), an IR by using polystyrene, and a balance by using certified
weights.14.1.1.1. Appropriate calibration and maintenance for each instrument are
determined by the manufacturer’s specifications, quality control
ranges, device tolerances, etc., and are detailed in section
specific technical manuals.
14.1.2. Documentation of all calibration, maintenance, and repair must be made
and kept near the instrumentation/equipment for use as needed by the
analyst.
14.1.3. New instruments and equipment or instruments and equipment that have
undergone repair or maintenance must have proper operation and/or
calibration verified prior to analysis of casework.
14.2. Manufacturer’s operating and/or repair manuals must be kept readily available to all
analysts.
15. Facility Security and Maintenance
15.1. Security
15.1.1. The success of any security system depends upon employee commitment
to the security plan; therefore, it is each employee’s responsibility to
actively participate in the Institute security program as described in the
Institute of Forensic Sciences Security Manual.
15.1.2. The Institute is equipped with numerous security devices including secure
keys and locks, magnetic card locks, and door contacts and motion
detectors in critical areas.
15.2. Building Maintenance and Repair
15.2.1. General Building Maintenance and Repair
15.2.1.1. It is the responsibility of Dallas County Facilities Management
to conduct building maintenance and repair activities.
15.2.1.2.
Standard operating procedures for the Institute of ForensicSciences and relevant maintenance records are maintained on-
site by Facilities staff assigned to the Institute.
15.2.1.3. Building issues identified by IFS staff are forwarded to Facilities
Management usually through IFS Administration.
15.2.2. Laboratory Housekeeping
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 35/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 31 Effective date: 2/28/2008
15.2.2.1. Laboratory areas must be kept clean and free of relevant
contamination.
15.2.2.2. General building cleaning and non-regulated trash removal is the
responsibility of Facilities Management.
15.2.2.3.
Lab specific cleaning and/or decontamination is theresponsibility of knowledgeable IFS staff.
15.2.2.4. Each laboratory is responsible for developing, implementing,
and documenting applicable cleaning/decontamination
procedures.
16. Quality Assurance/Quality Control
16.1. The Institute has developed various quality assurance and quality control procedures
to provide ongoing verification that the technical procedures used in the Laboratory
are valid and that the quality of each examiner’s work is maintained at an acceptable
level.
16.1.1. Components of the Quality Assurance/Quality Control program include
but are not limited to: administrative review, technical/peer review,
proficiency testing, inter-laboratory comparisons, reanalysis of casework,
assay controls, reviews and audits, etc. Used as a whole, these tools are
valuable in assessing laboratory and analyst performance; however, a
single event is not the sole indicator of laboratory or analyst competence.
16.1.2. The goals of a quality assurance/quality control program are as follows:
16.1.2.1. To verify that technical procedures are valid and working
properly;16.1.2.2. To ensure that quality work is being produced;
16.1.2.3. To identify areas where additional training would be beneficial;
16.1.2.4. To evaluate effectiveness and appropriateness of analytical
methodology; and
16.1.2.5. To demonstrate current competence of the laboratory and the
individual analysts.
16.2. Administrative Review of Reports
16.2.1. Administrative review is a procedure used to check for consistency with
laboratory policy and procedures and for editorial correctness.
16.2.2. An administrative review is conducted on all laboratory reports to ensure
that all reports are complete, concise, and consistent with laboratory
policy.
16.2.3. Administrative review is conducted at the time of final report review and
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 36/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 32 Effective date: 2/28/2008
signature; by signing the case report, an individual documents that an
administrative review has been conducted.
16.2.4. An administrative review may also be conducted by others including a
peer reviewer.
16.3.
Technical/Peer Review of Case Records16.3.1. Peer/technical review is a review of the analytical report and supporting
documentation package for technical correctness by an individual - other
than the primary analyst - who has expertise in a specific functional area
gained through documented training and expertise.
16.3.1.1. The technical reviewer may be either an individual appropriately
qualified as a casework analyst in the discipline /subdiscipline
under review, or an individual qualified by appropriate training
and expertise but who does not perform casework analysis in the
discipline /subdiscipline under review.
16.3.2. Peer/technical review provides a second evaluation of bench notes, data,and other documents which form the basis for the scientific conclusion
described in the report.
16.3.3. Technical/peer review must be conducted on a minimum of 20% or six
(whichever is fewer) completed cases per examiner per month.
16.3.3.1. At the discretion of the section chief, technical/peer review in
specific disciplines/subdisciplines may be performed as a routine
review activity for all technical reports.
16.3.3.2. Technical/peer review is typically completed prior to the release
of a report and following completion of all relevant quality
control and administrative review activities.
16.3.3.3. In some disciplines/subdisciplines, technical/peer review may
occur following release of a report.
16.3.4. For each case that receives peer/technical review, the reviewer will
determine if the following elements have been satisfied:
16.3.4.1. The requested examinations are addressed, and the results are
clearly communicated to the reader.
16.3.4.2. The format of the report is consistent with laboratory practice,
and the report is editorially and typographically correct.
16.3.4.3. The report adequately describes the evidence.
16.3.4.4. The case number and signing analyst’s (or analysts’) initials
appear on all pages of the report’s supporting documentation
package.
16.3.4.5. The chains of custody for evidence items examined (including
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 37/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 33 Effective date: 2/28/2008
internal transfers) are current and adequately documented.
16.3.4.6. The examination results are supported by applicable analytical
documentation (graphs, charts, etc.)
16.3.4.7. The tests performed conform to accepted techniques, and
appropriate standards and/or control samples were used andadequately documented.
16.3.4.8. The conclusions drawn are fully supported by the data, and are
reasonable and within the range of acceptable opinions of peers
within the discipline.
16.3.5. Conformance to the elements described in section 16.3.4 may be
documented by completion of the Peer/Technical Review form.
16.3.5.1. When used, the Peer/Technical Review form is retained in the
case file.
16.3.5.2. Alternatively, disciplines/subdisciplines may incorporate the
technical/peer review into routine case review activities without
use of the Peer/Technical Review form provided that the
technical/peer review process is documented in technical or
other manuals.
16.3.6. Non-conformance to the elements described in section 16.3.4 will be
documented by completion of the Peer/Technical Review form.
16.3.6.1. On the Peer/Technical Review form the technical reviewer must
provide a description of all instances of non-conformance.
16.3.7. If a non-conformance to the elements described in section 16.3.4 is
detected during technical/peer review, and if the non-conformance is nototherwise resolved as part of the routine casework quality control process,
then it is reported to the Section Chief by the Technical Reviewer. The
Section Chief then:
16.3.7.1. Determines the appropriate course of action to resolve the
variance and documents this on the Peer Review Form.
16.3.7.2. Forwards the Peer Review Form to the Quality Manager for
review.
16.3.7.3. As appropriate, initiates a Request for Review (see the Self-
Critical Review and Corrective Action section of this Manual).
16.3.8. In any laboratory which has only one qualified examiner in a
discipline/subdiscipline, the Section Chief will make arrangements with
another forensic laboratory to perform a peer or technical review on the
required number of cases; where feasible, the laboratory should be
accredited.
This is a non-controlled copy of a controlled document
8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 38/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 34 Effective date: 2/28/2008
16.3.8.1. For an external review, components of the completed case file
necessary to reach final conclusions are copied and sent to a
qualified external reviewer with the Peer Review Form
16.3.9. The Quality Manager is responsible for tracking participation in the
technical/peer review process.
16.4. Proficiency Testing Program
16.4.1. Proficiency testing is a process in which analysts perform testing on
specimens of unknown composition to the analyst but of known
composition to selected Institute staff (internal) or to an independent
agency (external).
16.4.1.1. The following information is required for each proficiency test –
internal or external:
16.4.1.1.1. How samples were obtained or prepared
16.4.1.1.2. Who participated in testing
16.4.1.1.3. Time frame of testing
16.4.1.1.4. Responsible supervisor
16.4.2. Proficiency testing requirements apply to forensic examiners and to
forensic disciplines. A discipline or functional area is a major area of
casework for which a laboratory may seek accreditation - for example,
Trace Evidence, Drug Analysis, Firearms, etc. A subdiscipline is
specialized area of analysis included within a discipline or functional area
- for example, hair analysis, fiber identification, and arson are sub-
disciplines of Trace Evidence.
16.4.3. The following minimum proficiency testing standards must be met:
16.4.3.1. All forensic examiners must complete at least one proficiency
test (internal or external) annually for each sub-discipline in
which they perform frequent analyses.
16.4.3.2. Each discipline or functional area must participate annually in at
least one external proficiency test for each forensic discipline in
which it provides services.
16.4.3.2.1. Where available, at least one proficiency test for each
discipline must be from an ASCLD/LAB approved
provider with results released to ASCLD/LAB.16.4.3.2.2. At a minimum, DNA examiners and technical support
personnel performing DNA analytical techniques will
comply with ASCLD/LAB and DAB standards
regarding external proficiency tests.
16.4.4. Response to Proficiency Test Results
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 39/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 35 Effective date: 2/28/2008
16.4.4.1. Proficiency test results are assessed as successful, successful
with corrective action, or unsuccessful.
16.4.4.1.1. “Successful” proficiency results occur when results are
deemed acceptable by the external proficiency program
or when written criteria for successful completion
established by the Section Chief are met.
16.4.4.1.2. Inconsistent proficiency results occur when results fall
outside the acceptable range as defined by the external
proficiency provider or the range identified by the
Section Chief for in-house proficiencies or when
identified as such by ASCLD/LAB. Inconsistent
proficiency results are investigated using the Institute’s
Critical Review and Corrective Action Program.
Results are evaluated as follows:
16.4.4.1.2.1. “Successful with corrective action” denotes
that an RFR and/or CAR was successfullycompleted as judged by the ASCLD/LAB
Proficiency Review Committee or the
Institute’s Executive Committee.
16.4.4.1.2.2. “Unsuccessful” proficiency results occur
when inconsistent proficiency results are not
successfully resolved.
16.4.4.1.3. The Section Chief, Supervisor, and/or Quality Manager
will review inconsistent proficiency results with the
analyst.
16.4.4.1.4. The Quality Manager has authority to reject or render
invalid any internal proficiency test samples that are
improperly documented, prepared, or otherwise
rendered unsuitable for the purpose of proficiency
testing.
16.4.5. Proficiency testing documentation including any associated corrective
action requests is maintained by the Quality Manager.
16.4.6. Results of proficiency testing are reported to the Director on an annual
basis by the Quality Manager.
16.4.7. The Quality Manager is the point of contact between the Institute andASCLD/LAB as it relates to proficiency test issues.
16.5. Inter-laboratory Comparisons
16.5.1. Laboratories may choose to establish exchange programs with other
laboratories for external proficiencies, sample validation of new
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 40/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 36 Effective date: 2/28/2008
procedures, etc.
16.6. Blind Testing and/or Reanalysis of Casework
16.6.1. Laboratories may choose to develop methods for submission and testing
of blind samples submitted as normal casework.
16.6.2. Laboratories may also choose to have a second analyst reanalyzepreviously completed casework as a means of assessing quality and
providing training.
16.7. Quality Control Samples
16.7.1. Quality control procedures, used routinely in assays, provide a frequent
assessment of the performance of analytical methods and the application
of these methods by the analyst.
16.7.2. Specific quality control procedures are included as a part of individual
analytical procedures or described in other documents prepared by a
Section or laboratory.
17. Self-Critical Review and Corrective Action
17.1. Self-critical review of laboratory procedures, processes, and results is a fundamental
and routine expectation of a scientific laboratory and an integral component in
maintaining consistency with best practices in forensic sciences.
17.1.1. Self-critical review occurs routinely during the normal performance and
review of case work, quality control/quality assurance activities including
proficiency testing and peer review, reanalysis of casework, training or
retraining activities, audits and reviews, etc.
17.1.2. Certain issues identified through self-critical review are readily
anticipated and guidance for response is addressed in routine practices,
policies, and procedures.
17.1.3. Other issues identified through self-critical review may not be addressed
in routine practices, policies, and procedures; action on these issues may
be initiated by submitting a Request for Review (RFR) to the Executive
Committee.
17.1.3.1. Every isolated variance from policy and procedure does not
require an RFR.
17.1.3.2. Isolated administrative errors do not usually require an RFR.
17.1.3.3. The RFR document is an administrative, working document
which is not retained once an appropriate course of action is
established by the Executive Committee.
17.2. Requests for Review (RFR) Process
This is a non-controlled copy of a controlled document
8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 41/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 37 Effective date: 2/28/2008
17.2.1. Internal review of an issue is initiated using the RFR process.
17.2.1.1. A RFR is used to a request review of an issue by the Quality
Manager and the Executive Committee.
17.2.1.2. The issue in question may relate to any aspect of Laboratory
operation including quality, EHS, personnel, security, etc17.2.2. It is the responsibility of each employee to immediately notify a
Supervisor, Quality Manager, EHS Manager, Section Chief and/or the
Director if they become aware of any issue that may impact the quality,
security, and/or safety of work performed or reported by the Institute.
17.2.3. Once advised, any supervisor or manager will evaluate the issue of
concern. On the basis of that evaluation, the issue may be forwarded to
the Quality Manager as a RFR; the appropriate Section Chief should also
be advised.
17.2.4. The Quality Manager assesses the RFR with respect to Institute policies
and procedures. The RFR is then forwarded to the appropriate SectionChief or Manager for initial evaluation and development of a proposed
response.
17.2.5. The Section Chief or Manager presents the RFR to the Executive
Committee.
17.2.6. Executive Committee determines the appropriate course of action such as
requesting further information or action, accepting resolution proposed or
conducted as part of the RFR, initiating the Corrective Action Response
(CAR) process, referring the issue to a more appropriate process such as
Human Resources, EHS Manager, Security Manager, determining that no
action is necessary, etc.
17.3. Corrective Action Request (CAR)
17.3.1. When an issue raised in an RFR is determined by the Executive
Committee to be substantive, it will be investigated, tracked, and resolved
through the CAR process.
17.3.1.1. An issue is defined as being “substantive” if it has the potential
to significantly impact the quality of the work of the laboratory –
even if for a short time.
17.3.1.2. Determination that an issue is “substantive” should consider the
significance, substance, and time-span of the issue.17.3.2. The CAR is a record of the formal investigation and resolution of RFRs
deemed substantive by the Executive Committee.
17.3.3. To assist in developing a response, the Executive Committee classifies the
severity of the issue of concern addressed by the CAR. The Class
assignment may be reviewed and reevaluated during the CAR process.
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 42/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 38 Effective date: 2/28/2008
The categories of classification are:
17.3.3.1. Class I – The issue is systemic, and the nature and cause of the
issue raises immediate concern regarding the quality of a
laboratory’s work product.
17.3.3.2.
Class II - The issue is not persistent or serious enough to causeimmediate concern for the over-all quality of the laboratory’s or
individual analyst’s work product.
17.3.3.3. Class III - The issue is determined to be unlikely to recur, is not
systemic, and does not significantly affect the fundamental
reliability of the laboratory’s or individual analyst’s work.
17.3.3.4. Class IV – The issue is primarily administrative or clerical and
does not affect the reliability of the laboratory’s or analyst’s
work.
17.3.4. The CAR is forwarded to the appropriate Section Chief or Program
Manager (i.e. EHS Manager, Quality Manager, etc.) for response and/oraction.
17.3.5. As appropriate, the Manager and/or Section Chief may delegate the
responsibility for formal evaluation of the finding and development of a
corrective action plan.
17.3.6. Once actions are complete, the CAR is forwarded to the Section
Chief/Manager for review and approval.
17.3.7. The CAR and applicable documentation is reviewed, evaluated, and
verified by the Executive Committee. Once the Executive Committee
accepts response to a CAR, it is closed out by the Quality Manager.
17.3.8. The Quality Manager is responsible for oversight of the corrective action
process including correspondence with accrediting agencies
(ASCLD/LAB and Texas DPS) as appropriate.
17.3.9. Completed CARs are retained through the next ASCLD/LAB inspection
or as required by ASCLD/LAB and/or Texas DPS standards.
17.4. Response to RFRs and CARs
17.4.1. The scope of corrective action should be commensurate with the
magnitude of the issue at hand.
17.4.1.1.
For example, a situation which questions the quality of alaboratory’s work product may warrant taking a procedure or
even a discipline out of service with extensive revalidation of
procedures whereas a non-systemic, one-time occurrence may
warrant a corrected report.
17.4.2. Once an issue is identified, an appropriate course of action is initiated
This is a non-controlled copy of a controlled document
8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 43/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 39 Effective date: 2/28/2008
based on the severity (CAR Class) and type of the situation.
17.4.2.1. Types of errors may include
17.4.2.1.1. Administrative Error - repetitive clerical errors, sample
confusion, improper storage, etc.
17.4.2.1.2. System Error - variance due to methodological,equipment, or environmental factors.
17.4.2.1.3. Analytical/Interpretive Error - variance due to the
choice, use, or implementation of an analytical
procedure and/or inaccurate or incomplete
interpretation of analytical results.
17.4.2.2. Examples of action include but are not limited to the following
which may be performed for a single analyst, multiple analysts,
or laboratory-wide as appropriate:
17.4.2.2.1. Review of the discrepancy with the analyst(s) involved
17.4.2.2.2. Retraining
17.4.2.2.3. Performance of a new proficiency test
17.4.2.2.4. Review of past casework for analyst(s) or a lab usually
back to the last successful proficiency
17.4.2.2.5. Reanalysis of casework with generation of corrected
reports as applicable
17.4.2.2.6. Removal of an analyst from applicable casework
17.4.2.2.7. Temporary or permanent discontinuation of a
procedure or use of equipment
17.4.2.2.8. Modification of an existing procedure or development
of a new procedure with appropriate validation
17.4.2.2.9. Validation of a method using different equipment
17.4.3. If an issue of concern is procedure or equipment related, all applicable
analysts must be advised of the corrective action taken to minimize
recurrence of the situation.
17.4.4. Minor issues and/or discrepancies that individually do not warrant a CAR
may require increasingly stringent action if they occur repeatedly.
17.4.4.1. If the Executive Committee determines that a quality concerninvolves serious negligence or misconduct by staff or
subcontractors that substantially affects the integrity of the
scientific analyses performed and reported by the Institute, then
in addition to any other corrective actions taken, a report of the
investigation of the concern will be forwarded to the Director for
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 44/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 40 Effective date: 2/28/2008
review.
17.4.4.2. In the event that the Director determines that the quality concern
involves serious negligence or misconduct by staff or
subcontractors that substantially affects the integrity of the
scientific analyses performed and reported by the Institute, then
the Director will report the concern to the Texas Department of Public Safety, the Dallas County District Attorney’s Office, and
other agencies as appropriate
17.5. Oversight of RFR and CAR Processes
17.5.1. The Quality Manager has oversight of the RFR and CAR process.
17.5.2. The Quality Manager keeps the Director informed regarding RFR and
CAR processes.
17.5.3. The Quality Manager oversees reporting of RFR and/or CAR issues to
ASCLD/LAB and/or Texas DPS as appropriate.
17.5.4. In the event that the Executive Committee is unable to reach consensus
regarding resolution of a RFR or CAR, then the issue is forwarded by the
Quality Manager to the Director for review and action.
18. Review of Testimony
18.1. Testimony by Forensic Laboratory employees should provide
18.1.1. Accurate presentation of the analyst’s credentials including academic
background, training, research, etc.;
18.1.2.
An accurate and complete description of the employee’s involvement inthe case;
18.1.3. A truthful, clear, straightforward, relevant, and objective response to all
questions on both direct and cross-examination;
18.1.4. Conclusions that follow logically from the underlying data and analytical
results;
18.1.5. Clear articulation of the reliability of results, analytical limitations, and
conclusions; and
18.1.6. Expert opinion that is within the area of expertise of the analyst.
18.2. Court testimony of each examiner must be evaluated at least once in any calendaryear in which the examiner testifies.
18.2.1. Courtroom monitoring is necessary to evaluate the delivery of the
examiner’s testimony and to ensure that the testimony is scientifically
consistent with the findings documented in the case file.
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 45/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 41 Effective date: 2/28/2008
18.2.2. Each examiner must ensure that his/her testimony is monitored at least
once during each calendar year in which testimony is provided.
18.2.3. It is strongly recommended that this review be done through direct
observation by a supervisor, Quality Manager, or other knowledgeable
individual identified by the Section Chief.
18.2.4. If supervisory or peer personnel are not available to personally observe
the testimony, the examiner is responsible for making contact with the
district attorney’s office, defense attorney, or judge to solicit written
feedback on the analyst’s testimony. Feedback should be sent to the
Quality Manager.
18.2.5. Employees with new responsibility for court testimony should receive
court monitoring repeatedly during their first several experiences as an
expert witness as outlined in the applicable training manuals.
18.3. It is recommended that court testimony of support staff is monitored annually.
18.4. Reviewers complete the Court Testimony Monitoring Form which details the areasto be evaluated including appearance, poise, performance under cross-examination,
ability to present scientific information in an understandable manner to a lay jury,
and most importantly a determination that the testimony given is scientifically
consistent with the work documented in the case file.
18.4.1. These forms are submitted to the Supervisor or Section Chief who
reviews them with the testifying analyst.
18.4.2. The testifying employee may make comments on the review.
18.4.3. Court Monitoring forms are maintained by the Quality Manager and
summarized annually.
18.5. If indicated by the review, the Section Chief will implement corrective action.
19. Departure from Documented Policies and Procedures
19.1. Although most of the evidence submitted to the Forensic Laboratory is handled by
standard policies and procedures, occasionally evidence is submitted that requires
deviation from standard procedures due to the unique nature of evidence, the
uncontrolled and unpredictable type and condition of materials taken into custody,
the limited amount of evidence, and the inability to resample evidence once
collected.
19.2. With permission from the Section Chief or Supervisor, it is acceptable for an analyst
to deviate from standard policies and procedures.
19.2.1. It is imperative in these cases that clear documentation be made in the
case file detailing the exact procedures used in the analysis.
19.2.2. Any limitations placed on conclusions due to deviations in policy and
This is a non-controlled copy of a controlled document
8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 46/53
8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 47/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 43 Effective date: 2/28/2008
compliance with ASCLD/LAB accreditation standards, this Quality
Management Program, and other laboratory requirements.
22.1.2. The Annual Internal Review is conducted under the direction of the
Quality Manager.
22.1.2.1.
The Quality Manager selects an inspection team and developsthe format for the review.
22.1.2.2. At a minimum, the review covers the standards and criteria of
the ASCLD/LAB manual in effect at the time of the review, and,
at a minimum, the scope of the review includes current
ASCLD/LAB requirements for an Annual Accreditation Audit
Report and the current IFS Quality Management Program,
Quality Manual.
22.1.2.3. The review is scheduled and announced well in advance.
22.1.2.4. The review includes the following operational areas:
22.1.2.4.1. The staffs’ awareness of the quality manual
22.1.2.4.2. Analytical procedure selection, control, and validation
22.1.2.4.3. Control of reagents and standards
22.1.2.4.4. Equipment calibration and maintenance of records
22.1.2.4.5. Adequacy of case reports and notes and their
disposition
22.1.2.4.6. Evidence handling procedures
22.1.2.4.7. Proficiency testing and inter-laboratory comparison
studies
22.1.2.4.8. Personnel training records
22.1.2.4.9. Handling of deficiencies and remedial action
22.1.2.4.10. Laboratory orderliness and health and safety measures
22.1.3. Soon after the conclusion of the review, the Quality Manager with
assistance from the inspection team prepares a draft report with
recommendations for investigation and action.
22.1.4. The Quality Manager with assistance from the Executive Committee
initiates applicable RFRs and/or CARs.
22.1.4.1. Major findings should be immediately communicated to the
Section Chief, Executive Committee, and/or Director at the time
of the review.
22.1.4.2. Substantive non-compliance with essential criterion must be
specifically addressed using the CAR process.
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 48/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 44 Effective date: 2/28/2008
22.1.5. The Quality Manager is responsible for generation of the written Annual
Internal Review Report which is provided to the Director.
22.1.6. The results of the Annual Internal Review are reviewed with the Institute
Quality Committee.
22.1.7.
The Annual Internal Review is maintained by the Quality Manager.22.2. ASCLD/LAB Annual Accreditation Audit Report
22.2.1. The Annual Internal Review is relied upon in part for completion of the
ASCLD/LAB Annual Accreditation Report.
22.2.2. By March 12 of each year, the Quality Manager, with assistance from the
Executive Committee, completes the Annual Accreditation Audit Report
for the prior year for review and signature by the Director.
22.2.3. A copy of the Annual Accreditation Audit Report is submitted to
ASCLD/LAB as described in the current ASCLD/LAB accreditation
manual.
22.2.4. The Annual Accreditation Audit Report is maintained by the Quality
Manager.
22.2.5. The results of the ASCLC/LAB Annual Accreditation Audit Report are
reviewed with the Institute Quality Committee.
22.3. Other Reviews and Audits
22.3.1. Other reviews and audits may be conducted as needed under the oversight
of the Quality Manager.
22.3.1.1. Where applicable, other reviews and audits may be concurrent
with and/or satisfy portions of the Annual Internal Review.Examples include the DAB Review in Forensic Biology and the
annual EHS Audit.
23. Annual Quality System Review
23.1. By March 12 of each year, the Quality Manager and Executive Committee performs
an Annual Quality System Review with assistance from the inspection teams and the
Institute Quality Committee.
23.1.1. The goal of the review is to assess the effectiveness of the quality system
by identifying ways to improve laboratory quality, ensuring that
procedures and policies reflect standard accepted practices in forensic
laboratories and current legal requirements, and ensuring compliance and
consistency with ASCLD/LAB accreditation standards.
23.1.2. The Quality Manager solicits recommendations for changes in the quality
system from the inspection teams, Institute Quality Committee, and other
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 49/53
Dallas County Institute of Forensic Sciences Quality Manual, Version 2.3
Forensic Laboratory 45 Effective date: 2/28/2008
applicable sources.
23.1.3. The Annual Quality System Review is developed by the Quality Manager
and Executive Committee and forwarded to the Director for review and
action.
23.2.
The Quality Manager implements identified changes to the Quality ManagementProgram as authorized by the Director.
23.3. The Annual Quality System Review is maintained by the Quality Manager and
made available during an ASCLD/LAB inspection as requested.
This is a non-controlled copy of a controlled document
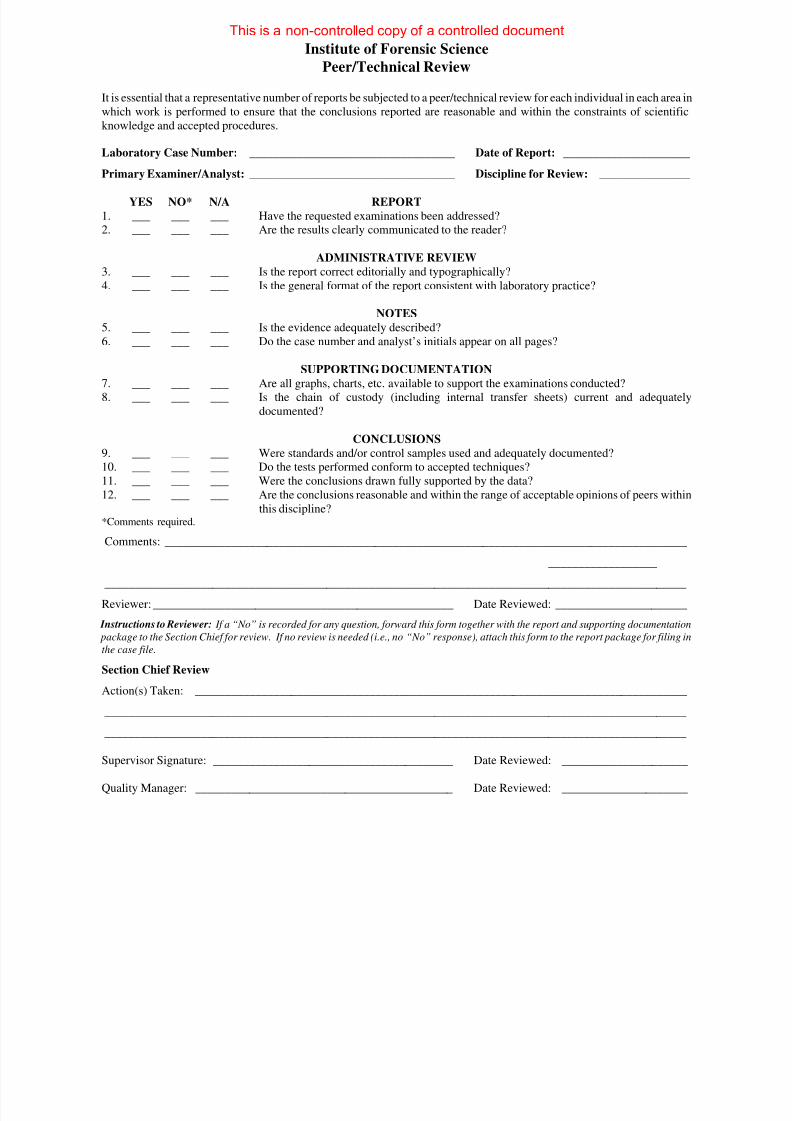
8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 50/53
Institute of Forensic Science
Peer/Technical Review
It is essential that a representative number of reports be subjected to a peer/technical review for each individual in each area in
which work is performed to ensure that the conclusions reported are reasonable and within the constraints of scientific
knowledge and accepted procedures.
Laboratory Case Number: __________________________________ Date of Report: _____________________
Primary Examiner/Analyst: __________________________________ Discipline for Review: _______________
YES NO* N/A REPORT
1. ___ ___ ___ Have the requested examinations been addressed?
2. ___ ___ ___ Are the results clearly communicated to the reader?
ADMINISTRATIVE REVIEW
3. ___ ___ ___ Is the report correct editorially and typographically?
4. ___ ___ ___ Is the general format of the report consistent with laboratory practice?
NOTES
5. ___ ___ ___ Is the evidence adequately described?
6. ___ ___ ___ Do the case number and analyst’s initials appear on all pages?
SUPPORTING DOCUMENTATION
7. ___ ___ ___ Are all graphs, charts, etc. available to support the examinations conducted?
8. ___ ___ ___ Is the chain of custody (including internal transfer sheets) current and adequately
documented?
CONCLUSIONS
9. ___ ___ ___ Were standards and/or control samples used and adequately documented?
10. ___ ___ ___ Do the tests performed conform to accepted techniques?
11. ___ ___ ___ Were the conclusions drawn fully supported by the data?
12. ___ ___ ___ Are the conclusions reasonable and within the range of acceptable opinions of peers withinthis discipline?*Comments required.
Comments: _______________________________________________________________________________________
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Reviewer: __________________________________________________ Date Reviewed: ______________________
Instructions to Reviewer: If a “No” is recorded for any question, forward this form together with the report and supporting documentatio
package to the Section Chief for review. If no review is needed (i.e., no “No” response), attach this form to the report package for filing i
the case file.
Section Chief Review
Action(s) Taken: __________________________________________________________________________________
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Supervisor Signature: ________________________________________ Date Reviewed: _____________________
Quality Manager: ___________________________________________ Date Reviewed: _____________________
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 51/53
RFR #: _________
RFR Form#2.doc
Institute of Forensic SciencesMonitoring Court Testimony
(To be completed by monitor)
Monitoring is necessary to evaluate the delivery of the examiner/analyst’s testimony and to ensure that the
testimony is scientifically consistent with the findings documented in the case file.
Witness: Discipline:
Laboratory Case Number: Date(s) of Appearance:
Court: Offense Charged: Time on Witness Stand:
Jury Trial: Trial Before the Court: _________ Other: _______________________
Rating Scale: 5 Excellent – 4 Commendable – 3 Competent – 2 Adequate – 1 Poor
Area Rating Scale CommentsAppearance
Demeanor – control,
alertness, posture
Presentation Style - clear,
professional, directed to jury
Professional Qualifications
Evidence Identification
Description of analysis or
examination
Testimony consistent with
case record and expertise
Nature of Attorneys Rapid Fire Personal
Attacks
Repetitive Confusing
Questions
Insinuating
Questions
‘Yes or No’
Questions
Prosecution Style
Defense Style
Comments
Comments by Monitor:
Monitor Signature/Date: ______________________ Supervisor Signature/Date:________________________
Additional comments attached: Monitor: Y / N Supervisor: Y / N
Analyst signature: I received a complete copy of the evaluation. _______________________ Date: _________
Analyst Comments:__________________________________________________________________________
Additional analyst comments attached: Y / N
This form must be returned to the Quality Manager for the Institute of Forensic Sciences.
This is a non-controlled copy of a controlled document
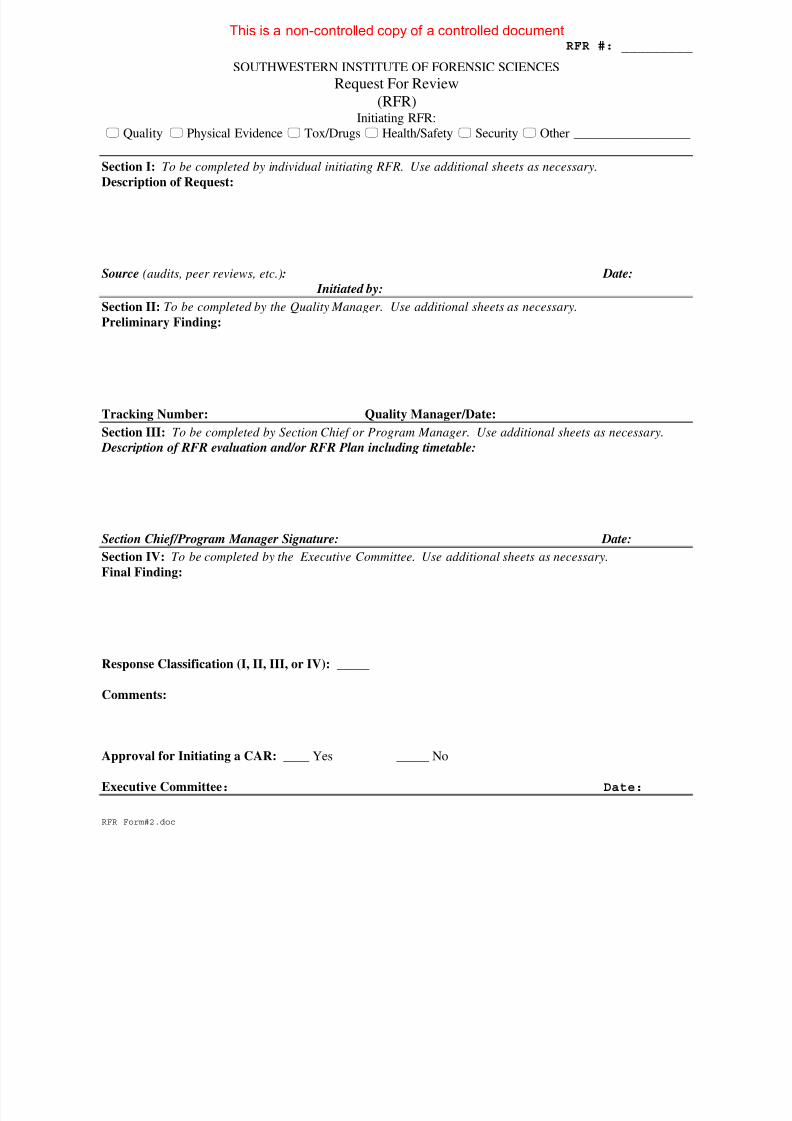
8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 52/53
RFR #: _________
RFR Form#2.doc
SOUTHWESTERN INSTITUTE OF FORENSIC SCIENCES
Request For Review
(RFR)Initiating RFR:
Quality Physical Evidence Tox/Drugs Health/Safety Security Other __________________
Section I: To be completed by individual initiating RFR. Use additional sheets as necessary.Description of Request:
Source (audits, peer reviews, etc.): Date:
Initiated by:
Section II: To be completed by the Quality Manager. Use additional sheets as necessary.
Preliminary Finding:
Tracking Number: Quality Manager/Date:
Section III: To be completed by Section Chief or Program Manager. Use additional sheets as necessary.
Description of RFR evaluation and/or RFR Plan including timetable:
Section Chief/Program Manager Signature: Date:
Section IV: To be completed by the Executive Committee. Use additional sheets as necessary.
Final Finding:
Response Classification (I, II, III, or IV): _____
Comments:
Approval for Initiating a CAR: ____ Yes _____ No
Executive Committee: Date:
This is a non-controlled copy of a controlled document

8/2/2019 SWIFS Quality Management Program Quality Manual v2.3 (02.28.2008) 53 Pages
http://slidepdf.com/reader/full/swifs-quality-management-program-quality-manual-v23-02282008-53-pages 53/53
CAR #: _________
SOUTHWESTERN INSTITUTE OF FORENSIC SCIENCES
Corrective Action Request
(CAR)Initiating CAR:
Quality Physical Evidence Tox/Drugs Health/Safety Security Other __________________
Section I: To be completed by individual initiating CAR. Use additional sheets as necessary.Description of Request:
Source (audits, peer reviews, etc.): Date:
Initiated by:
Section II: To be completed by the Quality Manager. Use additional sheets as necessary.
Description of Finding:
Executive Committee Approved:
Response Class (I, II, III, or IV): Initiating a CAR Date:
Tracking Number: Quality Manager Date:
Section III: To be completed by Section Chief or Program Manager. Use additional sheets as necessary.
Responsible for Corrective Action: Response Due Date:
Description of CAR evaluation and/or CAR Plan including timetable:
Plan Accepted by:
Section IV: To be completed by the individual responsible for corrective action. Use additional sheets as
necessary.
Description of Actions Taken:
Completed by: Date:
Section V: When CAR is complete, include evidence of completion with response and return to the initiating
S ti Chi f/M b th d d t
This is a non-controlled copy of a controlled document





























