Embed Size (px)
Citation preview

Surviving Sepsis Campaing Resultados y futuro
Ricard Ferrer Intensive Care Department
Mutua Terrassa University Hospital Barcelona. SPAIN

Phase 1 Barcelona declaration Phase 2 Evidence based guidelines
Phase 3 Implementation and Education

Surviving Sepsis Campaign: Timeline
Barcelona Declara<on
SSC Guidelines
2010
Guidelines And bundles Revision
2005
NEJM editorial
2004
2002
Guidelines Revision
Phase III starts: IHI partnership
2008 2012
Results published 15,000 pts 20% RRR
2006 2014
Results published 30,000 pts 27% RRR

Surviving Sepsis Campaign (SSC) guidelines for management of severe
sepsis and septic shock
Dellinger RP, Carlet JM, Masur H, Gerlach H, Calandra T, Cohen J, Gea-Banacloche J, Keh D, Marshall JC, Parker MM, Ramsay G,
Zimmerman JL, Vincent JL, Levy MM Crit Care Med 2004;32:858-873
Intensive Care Med 2004;30:536-555

Surviving Sepsis Campaign: International guidelines for management of severe sepsis
and septic shock: 2008
Dellinger RP, Levy MM, Carlet JM, Bion J, Parker MM, Jaeschke R, Reinhart K, Angus DC, Brun-Buisson C, Beale R, Calandra T,
Dhainaut JF, Gerlach H, Harvey M, Marini JJ, Marshall J, Ranieri M, Ramsay G, Sevransky J, Thompson BT, Townsend S, Vender
JS, Zimmerman JL, Vincent JL.
Crit Care Med 2008; 36:296-327
Intensive Care Med 2008;30:536-555
Surviving Sepsis Campaign: Interna<onal guidelines for management of severe sepsis
and sep<c shock: 2012
R Phillip Delllinger MD1; Mitchell M. Levy MD2, Andrew Rhodes MD BS3; Djillali Annane MD4; Herwig Gerlach MD PhD5; Steven M. Opal MD6; Jonathan E. Sevransky MD7; Charles L. Sprung MD8; Ivor S. Douglas MD9; Roman Jaeschke MD10; Tiffany M. Osborn MD MPH11; Mark E. Nunnally MD12; Sean R. Townsend MD13; Konrad Reinhart MD14; Ruth M. Kleinpell
PhD RN-‐CS15; Derek C. Angus MD MPH16, Clifford S. Deutschman MD MS17; Flavia R. Machado MD PhD18, Gordon Dr. Rubenfeld MD19; Steven A. Webb MB BS PhD20; Richard J. Beale MB BS21; Jean-‐Louis Vincent MD PhD22; Rui Moreno MD PhD23; and the Surviving
Sepsis Campaign Guidelines Commi`ee including the Pediatric Subgroup*
Cri<cal Care Med. 2013 Feb;41(2):580-‐637 Intensive Care Med. 2013 Feb;39(2):165-‐228

Current Surviving Sepsis Campaign Guidelines Sponsors
• American Associa<on of Cri<cal-‐Care Nurses
• American College of Chest Physicians • American College of Emergency Physicians • Australian and New Zealand Intensive Care
Society • Asia Pacific Associa<on of Cri<cal Care
Medicine • American Thoracic Society • Brazilian Society of Cri<cal Care(AIMB) • Canadian Cri<cal Care Society • Chinese Society of Cri<cal Care Medicine • Chinese Society of Cri<cal Care Medicine
of Chinese Medical Associa<on • European Respiratory Society • European Society of Clinical Microbiology
and Infec<ous Diseases
• European Society of Intensive Care Medicine • European Society of Pediatric and Neonatal
Intensive Care • German Sepsis Society • Infec<ous Diseases Society of America • Indian Society of Cri<cal Care Medicine • Japanese Associa<on for Acute Medicine • Japanese Society of Intensive Care Medicine • La<n American Sepsis Ins<tute • Pan Arab Cri<cal Care Medicine Society • Pediatric Acute Lung Injury and Sepsis Inves<gators • Society Academic Emergency Medicine • Society of Cri<cal Care Medicine • Society of Hospital Medicine • Surgical Infec<on Society • World Federa<on of Cri<cal Care Nurses • World Federa<on of Socie<es of Intensive and
Cri<cal Care Medicine

Phase 1 Barcelona declaration Phase 2 Evidence based guidelines
Phase 3 Implementation and Education

SSC Methodology: International Multifaceted Intervention
• National/regional/network “launch meetings” – Identify local champions – Introduce sepsis bundles – Staff support for coordinating sites – Regular conference calls
• Educational tools • SSC manual • SSC slides
• Website – SSC and IHI website – Sepsis list-serve
• Interactive database – Automated uploading to SSC server – Technical support – Local audit and feedback capabilities

Crit Care Med 2010; 38(2):367-374
n= 15.022

Crit Care Med 2010; 38(2):367-374

SSC: Europe vs USA
Levy M et al. Lancet ID 2012
Mortality Organ dysfunc<ons

SSC: Europe vs USA
Origin of infec<on Pa<ent Loca<on at
Diagnosis
Levy M et al. Lancet ID 2012

ICU bed availability is higher in the USA

SSC Final Report of Phase III 7.5 year analysis of 30,000 patients
Effects: • Participation • Duration • Dose

SSC Mortality: Par<cipa<on effect
Levy et al; 2014 CCM/ICM
27.3% RRR in mortality P < 0.001

SSC DuraHon Effect
Levy et al; 2014 CCM/ICM
• The adjusted odds of hospital mortality is decreasing 1% per site quarter (p = 0.005)
• The longer a site participated, the greater the associated mortality reduction
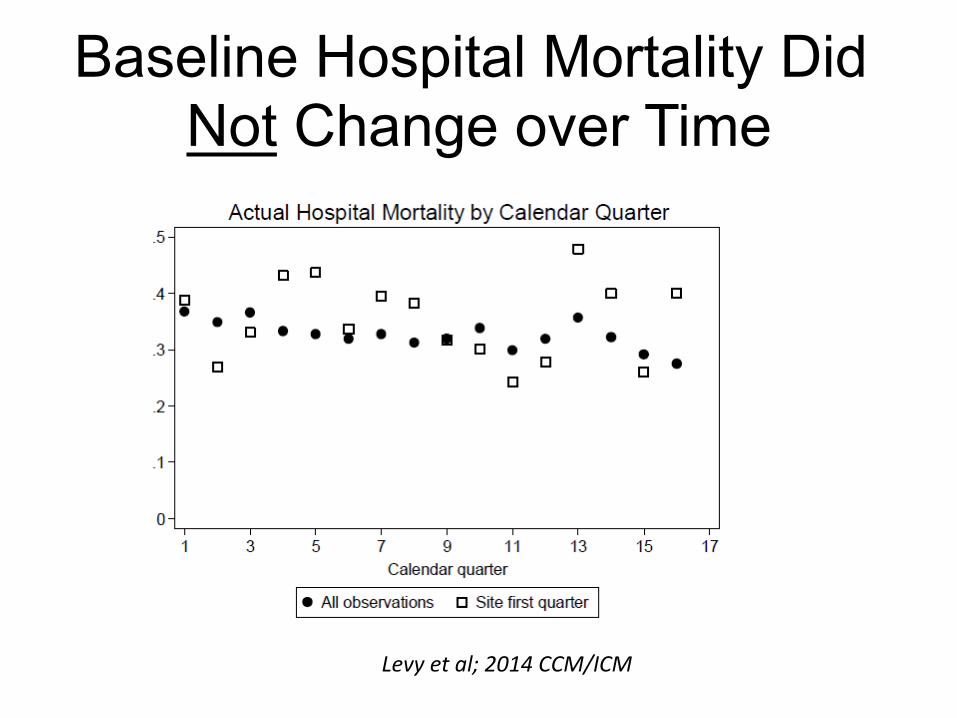
Baseline Hospital Mortality Did Not Change over Time
Levy et al; 2014 CCM/ICM

Mortality in HIGH COMPLIANCE Sites with at least 3 years of data collection
êMortality: 45.7% to 29.5% ARR: 16.5% P < 0.001 RRR: 36%

êMortality: 42.9% to 26.2% ARR: 16.7% P < 0.001 RRR: 39%
Mortality in HIGH COMPLIANCE Sites with at least 4 years of data collection

CCM 2014;42:1749-55
Severe Sepsis and Septic Shock
Empirical antibiotics after sepsis recognition

Predicted hospital mortality and 95% CIs for time to first antibiotic administration Results adjusted by the sepsis severity score, ICU admission source ([ED], ward, vs ICU), and geographic region (Europe, United States, and South America)

26.3% 68.6% 51.8% 78.2% 84.0% 87.5% 100%
Median time to empiric antibiotics

16935
18671
15000
16000
17000
18000
19000
20000
Euro
s
Hospital Costs
Preintervention Intervention
5.445.98
3.75 4.12
01234567
Years
LYG QALY
Preintervention Intervention
Adjusted ICER 4,435 euros per LYG Adjusted ICUR 6,428 euros per QALY

Published Data from SSC: 2006-2014
• All prospective cohort studies
• 40 published reports in peer-reviewed journals
• All demonstrated: – Increased compliance – Associated decreased
mortality
– United States (25) – Spain (1) – France (1) – Germany (1) – Portugal (1) – Netherlands (2) – UK (2) – China (3) – Iceland (1) – Korea (1) – Pan-Asia (1) – Latin America (1)
Challenges to SSC data • Uncontrolled data
– Interrupted Hme series – Before/aMer design
• Mortality benefit could be explained by: – Secular trends in sepsis mortality – Are sites shiMing less sick paHents into ICU who would have survived regardless: DiluHng mortality rate over Hme
• However, when adjusted for severity: Mortality benefit remains significant

Crit Care Med 2014; 42:1890–1898
CONTROL INTERVENTION

Mortality Change in Interven<on and Control Groups
CONTROL
INTERVENTION

INTERVENTION

Conclusions • With the adequate leadership, it is possible to do
international multifaceted interventions. • It is feasible to use data to audit and change
clinical behavior – Performance metrics can change clinical practice
• Increased compliance with performance metrics is associated with improved survival – 39% RRR with high compliance

Conclusions: Variability • Published studies demonstrate wide practice
variation: Poor compliance with known quality indicators
• Variability based on different weighting of relevant knowledge – EXPECTED
• Variability based on knowledge deficits, faulty application of knowledge or simple forgetting – UNACCEPTABLE

What’s Next? • Marked increased attention: SSC
recommendations are being implemented – Important american organizations are
incorporating SSC metrics: • National Quality Forum measure • CMS: Centers for Medicare & Medicaid Services
– Governments • New York System mandated reporting • Catalonia: 2015 Instruction
– Many hospital networks



Registry: including the SSC quality indicators
SEPTIC CODE
Patients Flow: SEP-I centers SEP-IIa centers SEP-IIb centers

What’s Next?
• SSC Guidelines • Sepsis Definition • IMPRESS study

SSC Guidelines 2016
• Timeline: October 2016 • Scope: Early management of severe sepsis and sepHc shock. Early is defined as within the first 24 hours.
• Target audience: Any healthcare worker in any healthcare se[ng who is caring for adult paHents with sepsis.
• Independent Pediatric Guidelines

SSC Guidelines 2016
• Results of studies PROCESS, ARISE are challenging current recommendaHons.
• New evidences in fluids: balanced crystalloids, albumin.
• New studies in specific subgroups like DIC or AKI.

Living Guideline Concept
• Living guidelines are systemaHcally developed, evidence based, and conHnually updated.
• Rigorous monitoring of published literature. • Electronic format vs Paper format. • EvaluaHon of the current state of the recommendaHon: no revision needed, revision possible, revision imperaHve.

Sepsis in Resource-Limited Nations Task Force report
• Leaders: M. Dünser/C. Farmer • Global task force to explore sepsis diagnosis and management
in resource-‐limited countries. • This task force has developed a conceptual approach, the
scan-‐teach-‐treat system. This approach has three steps: – Scan the region of interest for key elements that influence sepsis
detecHon, management, and outcome; – Teach through public awareness and healthcare provider educaHonal
programs on sepsis; – Treat by implemenHng a “sepsis first aid kit” into clinical pracHce.


SEPSIS DEFINITION Objectives
• Improve our ability to make early bedside detecHon of the disease, and thus allow early therapeuHc intervenHon and adequate paHent allocaHon.
• IdenHfy paHents with different condiHons but with the similar pathophisiology, so same therapeuHc targets.
• Select paHents with similar severity, according to a scoring system.
• Adequate tool for selecHng paHents for clinical trials promoHng the research of new drugs or devices.


Consequences of 1992 definition
• Definition has help to standardize the treatment and produce guidelines.
• Quality of treatment and mortality have improve.
• However, none innovative treatments showed benefit despite lots of trials using these definitions.
• Important epidemiological differences in different areas.

Main limitations of SIRS criteria
• Unspecific • Arbitrary cut-offs • Too sensitive:
– Not useful to alert sepsis outside the ICU: almost every viral infection could be confounded with sepsis
– SIRS criteria almost universal in the ICU • Not consistent in different consensus. • Not always present.

SIRS criteria at ICU admission
Outcome according SIRS criteria at ICU admission
87%

Am J Respir Crit Care Med Vol 171. pp 461–468, 2005
DEVELOPMENT OF THE RISSC FOR PROGRESSION FROM SEPSIS TO SEVERE SEPSIS OR SEPTIC SHOCK
BIVARIATE HR MULTIVARIATE HR

Crit Care Med 2005; 33:512–519
ApEn


Incidence of the four SIRS criteria on day 1 by variations in threshold criteria and mode of data recording: - Automatic (continuous) recordings of single occurrences - Automatic recordings of 60-min intervals above threshold - Manual (hourly) recordings of single occurrences - Manual recordings of 60-min intervals above threshold.

Infec<on + some of:

PIRO concept: Tool for Phenotyping sepsis
Predisposition
Insult (Infection)
Response
Organ Dysfunction
Genetic susceptibility Coexisting health complications
Pathogen, toxicity and sensitivity Location and compartmentalization
Increased biomarkers or biomediators Manifested physiologic symptoms
Number of failing organs

Use of biomarkers for diagnosing sepsis is premature
IL-6 CRP
PCT WBC
TNF-α erythrocyte sedimentation
Lactate


- The 2001 definition has not improved the 1992 definition. - The PIRO concept has not been incorporated. - In fact, most of the studies are still using the 1991 definition, with the known limitations
Consequences

L. Gattinoni, SCCM 2015

• Sepsis is a life threatening condition that arises when the body's response to an infection injures its own tissues and organs.
• Sepsis leads to shock, multiple organ failure and death especially if not recognized early and treated promptly.
• Sepsis remains the primary cause of death from infection despite advances in modern medicine, including vaccines, antibiotics and acute care.

KOL and Sepsis definition
• Unspecific, not useful for clinical trials. • Reserve the notion of sepsis for
conceptual purposes only. • Focus future clinical investigation on
specific biological targets or on patients with specific infectious diseases.
Crit Care Med 2008; 36:964–966

KOL and Sepsis definition
• Sepsis is the host’s deleterious, non-resolving inflammatory response to infection that leads to organ dysfunction.
• Sepsis should be defined as a systemic response to infection with the presence of some degree of organ dysfunction.

KOL and Sepsis definition
• A single universal definition – using validated variables – should support a more accurate
epidemiological characterization – appropriate power for interventional trials – appropriate benchmarks for providers and
hospitals.
2015

San Francisco Sepsis Definition ESICM/SCCM task force
• Sepsis 3.0 definiHon: updated in the future according the new evidence.
• Help to idenHfy paHents outside the ICU. • SIRS is DEAD. • SEPSIS: “Life-‐threatening organ dysfuncHon due host response to an infecHon”
• New “sepsis”= Old “severe sepsis”. SepHc shock, no change.
• Data-‐driven definiHon: definiHon of OD, shock will be based in “big data analysis”. “New 3”.

• 1 day world-‐wide point prevalence study • First study: 7th November 2013
An Interna<onal Mul<centre Prevalence Study on Sepsis.
The Impress Study

The IMPRESS-‐SSC Study An Interna<onal Mul<-‐Centre Prevalence Study of Sepsis
Aims • To assess pracHce gaps in care of paHents with sepsis by measuring compliance with SSC sepsis bundles in sites in both community and academic hospitals internaHonally.
• To evaluate the epidemiology of sepsis in different areas of the world.

The IMPRESS-‐SSC Study An Interna<onal Mul<-‐Centre Prevalence Study of Sepsis
Inclusion Criteria: • For the study day (0000 to 2400), consecuHve paHents presenHng to either the emergency department (ED) or being cared for in the ICU with severe sepsis or sepHc shock will be enrolled. To be eligible paHents must have all of the following: – Must be admiked or transferred to either the ED or ICU. – Have a high clinical suspicion of an infecHon – Have sepsis as defined by the presence (probable or documented) of infecHon together with systemic manifestaHons of infecHon
– Evidence of acute organ dysfuncHon and / or shock

The IMPRESS-‐SSC Study An InternaHonal MulH-‐Centre Prevalence Study of Sepsis
November 7th 2013 62 Countries from all conHnents 1794 PaHents
28.4% In hospital Mortality

0
100
200
300
400
500
600
700
800
North America
Europe Asia Other
November 7th 2013 62 Countries from all conHnents 1794 PaHents
1794 Pa<ents Enrolled in One Day.

Age years (SD) North America
Europe Asia Other1
<65 294 (55.4) 297 (43.0) 246 (65.8) 115 (59.0) 65 to 75 115 (21.7) 187 (27.1) 75 (20.1) 41 (21.0) >75 122 (23.0) 207 (30.0) 53 (14.2) 39 (20.0)
November 7th 2013 62 Countries from all conHnents 1794 PaHents
Age of Pa<ents by Region.
Significant at p<0.0001

Origin of sepsis N (%) North America
Europe Asia Other
Community acquired 344 (64.8) 377 (54.6) 242 (64.9) 102 (55.1) Health care acquired 131 (24.7) 102 (14.8) 35 (9.4) 23 (12.4) Hospital acquired 38 (7.2) 130 (18.8) 62 (16.6) 43 (23.2) ICU acquired 18 (3.4) 81 (11.7) 34 (9.1) 17 (9.2)
November 7th 2013 62 Countries from all conHnents 1794 PaHents
Origin of Sepsis by Region.
Significant at p<0.0001

Site of Infec<on N (%) North America
Europe Asia Other
Abdominal 88 (16.5) 184 (26.6) 88 (23.5) 42 (21.5) CNS infecHon 4 (0.8) 3 (0.4) 12 (3.2) 3 (1.5) Catheter 12 (2.3) 19 (2.8) 8 (2.1) 6 (3.1) Device 7 (1.3) 5 (0.7) 0 (0.0) 1 (0.5) Other infecHon 47 (8.8) 64 (9.3) 49 (13.1) 15 (7.7) Respiratory 203 (38.1) 273 (39.4) 160 (42.8) 80 (41.0) Unknown 60 (11.3) 58 (8.4) 43 (11.5) 26 (13.3) UTI 112 (21.0) 86 (12.4) 14 (3.7) 22 (11.3) November 7th 2013 62 Countries from all conHnents 1794 PaHents
Site of Infec<on by Region. Significant at p<0.0001

0
10
20
30
40
50
60
70
80
North America
Europe Asia Other
%
November 7th 2013 62 Countries from all conHnents 1794 PaHents
Propor<on of Pa<ents on Mechanical Ven<la<on.
P<0.0001

North America
Europe Asia Other
Chronic illness 263 (49.3) 266 (38.4) 108 (28.9) 94 (48.2) <2 Organ Failures 153 (28.8) 154 (22.2) 87 (23.3) 53 (27.2) Vasopressors, N (%) 76 (14.3) 19 (2.8) 20 (5.4) 11 (5.6) IntubaHon, N (%) 196 (36.8) 325 (47.0) 235 (62.8) 109 (55.9) Mechanical VenHlaHon 245 (47.7) 400 (57.8) 278 (74.3) 121 (62.0) SOFA, mean (SD) 6.5 (3.2) 6.9 (3.4) 8.0 (3.3) 7.4 (3.0) APACHE II, mean (SD) 22.0 (9.5) 21.6 (8.3) 21.9 (8.7) 22.3 (8.8)
November 7th 2013 62 Countries from all conHnents 1794 PaHents
Markers of Severity by Region.
All significant at p<0.0001 apart from APACHE II (p=0.8)

0 5
10 15 20 25 30 35 40 45 50
North America
Europe Asia Other
%
November 7th 2013 62 Countries from all conHnents 1794 PaHents
Propor<on of Pa<ents with Sep<c Shock.
P=0.034

N (%) or median (IQR)
North America
Europe Asia Other
ICU admission 469 (88.0) 556 (80.4) 356 (95.2) 164 (84.1) ICU LOS, days 5.9 (2-‐14) 9.5 (4-‐21) 9.0 (4-‐18) 8.5 (3-‐22) ICU mortality 102 (19.1) 150 (21.7) 89 (23.8) 64 (32.8) Hospital LOS, days 10.9 (5-‐20) 16.0 (7-‐29) 14.2 (7-‐23) 14.3 (7-‐26) Hospital mortality 131 (24.6) 194 (28.0) 114 (30.5) 71 (36.4)
Unadjusted Pa<ent Outcomes by Region.
ICU admission and ICU & hospital LOS significant at p<0.0001, ICU mortality p= 0.03, Hospital mortality p=0.013

Variable Hospital mortality odds ra<o1 95% CI p-‐value
North America (ref) 1.00 -‐-‐-‐ -‐-‐-‐ Europe 1.06 0.64 – 1.75 0.820 Asia 1.08 0.62 – 1.87 0.786
Rela<onship Between Hospital Mortality and Region.
1Adjusted for 3 hour bundle compliance, 6 hour bundle compliance, age, ICU admission (yes vs. no), sepsis status (severe vs. shock), locaHon (ED, ward, ICU, OR, unknown), sepsis origin (community, health care, hospital, or ICU acquired), and APACHE II
GEE popula<on-‐averaged logis<c regression model hospital mortality odds ra<os by region

November 7th 2013 62 Countries from all conHnents 1794 PaHents
3 Hour Bundle Compliance % Compliance Measurement of Lactate 56 Obtain Blood Cultures Prior to AnHbioHcs 49 Administer Broad Spectrum AnHbioHcs 94 Administer 30 mL/kg crystalloid for hypotension 57
6 Hour Bundle Compliance % Compliance Apply vasopressors 82 Measure CVP 67 Measure ScvO2 60
19% Overall Compliance
36% Overall Compliance
The IMPRESS-‐SSC Study An Interna<onal Mul<-‐Centre Prevalence Study of Sepsis

North America
Europe Asia Other
Lactate bundle, N (%) 332 (62.3) 413 (59.7) 178 (47.6) 79 (40.5) ABX bundle, N (%) 324 (60.8) 457 (66.0) 252 (67.4) 122 (62.6) Fluid bundle, N (%) 325 (60.1) 378 (54.6) 206 (55.1) 108 (55.4) Full bundle, N (%) 150 (28.1) 122 (17.6) 51 (13.6) 17 (8.7)
November 7th 2013 62 Countries from all conHnents 1794 PaHents
3 Hour Bundle Compliance by Region.
Lactate bundle and total bundle both significant at p<0.0001, Abx and Fluid bundle NS.

0
5
10
15
20
25
30
North America
Europe Asia Other
%
November 7th 2013 62 Countries from all conHnents 1794 PaHents
3 hour Bundle Compliance by Region. P<0.001

North America
Europe Asia Other
Lactate bundle, N (%) 302 (56.7) 479 (69.2) 204 (54.6) 92 (47.2) Vasopressor, N (%) 405 (76.0) 576 (83.2) 334 (89.3) 164 (84.1) CVP bundle, N (%) 332 (62.3) 472 (68.2) 276 (73.8) 129 (66.2) ScvO2 bundle, N (%) 306 (57.4) 417 (60.3) 233 (62.3) 114 (58.5) Full bundle, N (%) 172 (32.3) 281 (40.6) 134 (35.8) 50 (25.6)
November 7th 2013 62 Countries from all conHnents 1794 PaHents
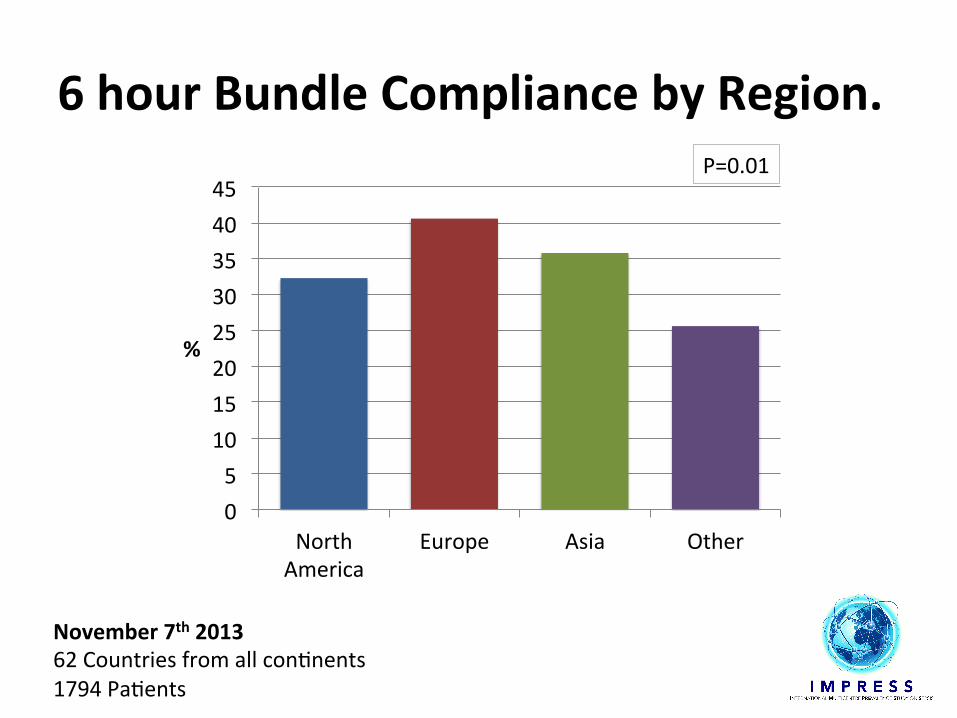
6 Hour Bundle Compliance by Region.
Lactate, vasopressor and CVP bundle significant at p<0.0001, Full bundle p=0.01, ScvO2 NS.
0 5
10 15 20 25 30 35 40 45
North America
Europe Asia Other
%
November 7th 2013 62 Countries from all conHnents 1794 PaHents
6 hour Bundle Compliance by Region. P=0.01
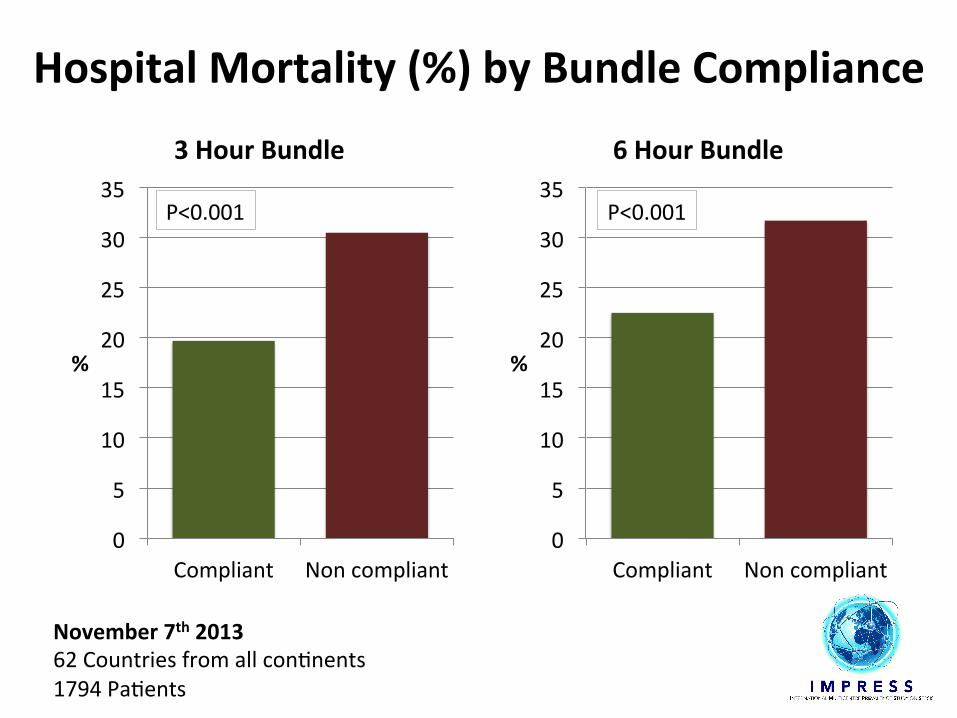
Hospital Mortality (%) by Bundle Compliance
0
5
10
15
20
25
30
35
Compliant Non compliant
%
3 Hour Bundle
0
5
10
15
20
25
30
35
Compliant Non compliant
%
6 Hour Bundle
P<0.001 P<0.001
November 7th 2013 62 Countries from all conHnents 1794 PaHents

Variable Hospital mortality odds ra<o1 95% CI p-‐value
Full 3 hour bundle 0.70 0.51 – 0.96 0.026 Full 6 hour bundle 0.75 0.58 – 0.96 0.020
November 7th 2013 62 Countries from all conHnents 1794 PaHents
Rela<onship Between Bundle Compliance and Outcome.
1Adjusted for ICU admission, sepsis status (severe vs. shock), locaHon (ED, ward, ICU, OR, unknown), and APACHE II
GEE popula<on-‐averaged logis<c regression model adjusted hospital mortality odds ra<os

• 1 day world-‐wide point prevalence study
Second study: World Sepsis Day 2016
An Interna<onal Mul<centre Prevalence Study on Sepsis.
The Impress Study

Conclusions • SSC has been a successful internaHonal mulHfaceted intervenHon.
• SSC registry and IMPRESS point prevalence study are sHll showing room for improvement.
• Many Knowledge Transfer iniHaHves based in the SSC guidelines are being implemented.
• SSC Guidelines: – Update the evidence every 4 years + living guideline concept.
– Specific guidelines: resource-‐limited, pediatrics,… • Sepsis definiHon 3.0 should help to beker idenHfy paHents, specially outside the ICUs.





























