Embed Size (px)
Citation preview

Survey of Neurology
Eric Kraus, MD
WAPA
4/22/17
NCCPA List
Diseases of nerves
» Peripheral neuropathy
» CRPS
» GBS
Movement D/Os
» Parkinson Dis
» Huntington Dis
» Essential tremor
» Tourette syndrome
Seizures
Syncope
Multiple sclerosis
Myasthenia gravis
Cerebral palsy
Altered mental status
» Dementia
» Delirium
Head injury
» Concussion
» Post-concussion syndrome
Covered elsewhere
» Stroke
» Headache
» Infections
ARS Question
This is a 22 yo woman with sensory loss in the right hand that spread
to her right trunk and leg over 2 weeks. No weakness. Last year she
had numbness in her left face for 4 weeks. Her exam reveals the
sensory loss to pinprick.
What test is likely to confirm your diagnostic suspicion?
A. Brain MRI
B. Spinal fluid evaluation
C. Lumbar MRI
D. Electrodiagnostic testing
E. Tibial evoked potentials

Multiple Sclerosis
CNS disease
Primarily demyelinating
» Axonal loss is also present
Females/white > males/non-white
Sex 2-3:1 = F:M
Prevalence 5-250/100,000 population
Associated with Vit D deficiency and EBV
exposure

MS: Types
Relapsing-remitting MS
(RRMS)
» 60-80%
» Secondary progressive
» Progressive relapsing
Primary progressive MS
(PPMS)
» 20-30%
» Older, cervical disease

MS: Clinical
Optic neuritis » Blurry, color desaturation
» Painful eye movement
Weakness, spasticity
Sensory » most common initial
presentation
Ataxia, tremor
Cognitive
Lhermitte’s sign
Fatigue
Heat and exercise
intolerance
Bladder
Sexual dysfunction

MS: Testing
MRI
CSF (Oligoclonal bands)
Evoked potentials

MRI
90-95% sensitive at
first presentation
Visual detection of
plaques
» Demyelination
» Gliosis
» Inflammation
Location
» Periventricular
» Corpus callosum
» Cerebellum
» Brain stem
Acute lesions
enhance (Gd+)
MacDonald Criteria

MRI MRI
Axial flair Coronal T1 with Gad Sagittal flair

MS: Treatment
Acute
» Glucocorticoids
Chronic (Disease modifying drugs)
» Interferon beta-1b (Betaseron, Extavia): SC qod
» Interferon beta-1a (Avonex): IM weekly
» Interferon beta-1a (Rebif): SC 3x/wk
» Glatiramir acetate (Copaxone): SC daily
» Nataluzimab (Tysabri): IV monthly
» Fingolimod (Gilenya): oral, new in 2010
» Teriflunomide (Aubagio): oral, new in 2012
» Dimethyl fumarate (Tecfidera): oral, new in 2013
» Mitoxantrone (worsening RRMS and SPMS)

ARS Question
A 48 yo man presents with 5 years of trouble eating
and writing. Your exam reveals a tremor with
outstretched hands R>L.
You make a presumptive diagnosis and suggest:
A. Medication review
B. Alcohol
C. Propranolol
D. Lab work-up
E. All of the above

Essential Tremor
Most common movement d/o
Postural and kinetic
Slowly progressive
Prevalence increases with age
» Mean age of presentation 35-45
» Adolescence onset
» 0.5-5% population
» F:M 1:1
Genetic - AD
» FH (+) 50-60%
Distribution
» Hands (symmetric)
» (30%) head, voice, jaw, face
» Legs
» Trunk
Worsened by:
» Emotion
» Hunger
» Fatigue
» Temperature
» Drugs/toxins

Action Tremor Work-up
Review medications
Ask about alcohol (response and abuse), illicit drugs
Labs » M7, LFTs, TSH, B12
» Ceruloplasmin and serum Cu
» Urine tox screen
» Rare: Vit E, heavy metals
Consider MRI for unilateral tremor and acute onset
Review psychiatric history

Drugs/Toxins
Steroids
Thyroid hormone
Lithium
Valproic acid
Cyclosporine
Tricyclics
Beta agonists
Theophyline
Neuroleptics
SSRIs
Caffeine
Nicotine
Arsenic
Lead
Cocaine/amphetamines
Alcohol withdrawal
Benzo withdrawal
Other drug withdrawal

ARS Question
A 56 yo man presents with trouble walking, small
hand writing, and a resting tremor.
You make a presumptive diagnosis and suggest:
A. Sinemet trial
B. Head MRI
C. Propranolol for essential tremor
D. Stroke work-up

Parkinson’s Disease
Loss of dopaminergic neurons in the
substantia nigra
Lewy bodies
Differentiate from broader classification
of parkinsonism
Mean age of onset 55yo

Parkinsonism
Parkinson’s Disease
Neuroleptic side effect
Post-encephalitic
Toxins (Mn, CO, MPTP)
Dementia
Wilson’s disease
Basal ganglia
calcifications
Parkinson-plus
syndromes
» Progressive supranuclear
palsy
» Corticobasoganglionic
degeneration
» Multisystem atrophy
– Autonomic
– Cerebellar
» Diffuse Lewy body
disease

PD: Clinical
Slow progressive course
4 cardinal features
» Resting tremor
» Bradykinesia
» Rigidity (cogwheel)
» Postural reflex impairment
Other: dementia, depression, autonomic

PD: Treatment
Sinemet = carbidopa/levodopa
» Levodopa converts to dopamine
» Most potent drug for PD
Dopamine agonists
» Act directly on dopamine receptors
» Synergy with levodopa
» Ex. Pramipexole, Ropinirole
COMT inhibitors
» Block COMT metabolism of levodopa to DA
» Ex. Entacapone
Other

Treatment Flow Chart

ARS Question
This 19 year-old male complains of excessive
blinking and the need to clear his throat. Onset
was at the age of 8.
You make a presumptive diagnosis and ask
questions about:
A. Sexual abuse
B. Attention deficit d/o
C. Numbness
D. Exercise program
E. Smoking

Tourette Syndrome
Clinical
» Tics: motor and vocal
» Involuntary but
suppressible
» Daily > 1 year
» Onset before age 21
(median age = 7)
» Lifelong, decline with age
» OCD
» ADHD
Prevalence 40/100k
Genetics
» 4:1 M:F
» AD with incomplete
penetrance
» MZ twins 80%

ARS Question
This 42 year-old female complains of a progressive
inability to keep her arms and legs still. She has
had depression for 10 years.
You make a presumptive diagnosis and ask
questions about:
A. Sexual abuse
B. Alcohol use
C. Family history
D. Exposure to lead
E. Smoking

Huntington Disease
Genetics
» CAG repeat
» AD
» Chrom 4
Pathology
» Loss of GABA
neurons in striatum
» Diffuse atrophy
Clinical
» Chorea
» Dementia
» Psychiatric
Treatment
» Neuroleptics
» Clonazepam
» Tetrabenazine
» Antidepressants

ARS Question
This 24 year-old man began having tingling
in his toes 3 days ago. Rapidly, it has
moved to the whole body accompanied by
weakness such that he can’t get out of bed
and is having trouble breathing and
swallowing. Reflexes are absent.
The most likely cause of this neuropathy is:
A.Vasculitis
B.Diabetes
C.B12 deficiency
D.Complex regional pain syndrome
E.Guillain-Barre syndrome

ARS Question
This 64 year-old man began having burning
pain in his toes 3 years ago. Slowly, it has
moved to the knee. The hands became
dysesthetic 1 year ago. No weakness.
Reflexes are absent at the ankles.
The most likely cause of this neuropathy is:
A. Vasculitis
B. Diabetes
C. B12 deficiency
D. Complex regional pain syndrome
E. Guillain-Barre syndrome

ARS Question
This 54 year-old has had stepwise
progression of sensory and motor
symptoms over the last 3 weeks. First in
the right hand (median), followed by the left
leg (sural), right leg (peroneal), and left
hand (ulnar).
The most likely cause of this neuropathy is:
A. Vasculitis
B. Diabetes
C. B12 deficiency
D. Complex regional pain syndrome
E. Guillain-Barre syndrome
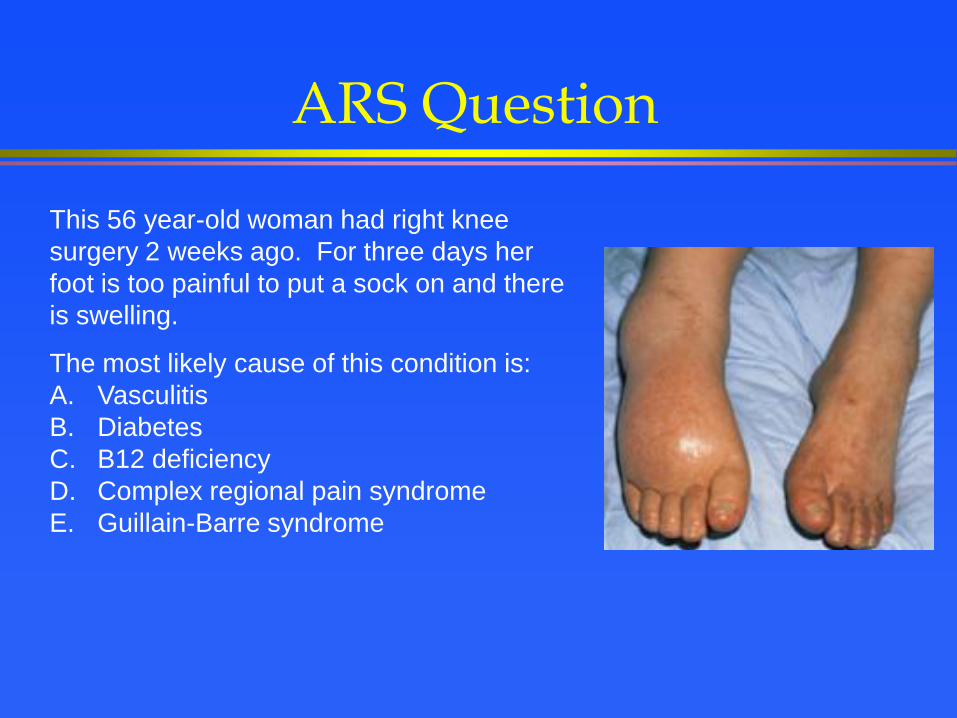
ARS Question
This 56 year-old woman had right knee
surgery 2 weeks ago. For three days her
foot is too painful to put a sock on and there
is swelling.
The most likely cause of this condition is:
A. Vasculitis
B. Diabetes
C. B12 deficiency
D. Complex regional pain syndrome
E. Guillain-Barre syndrome

Guillain-Barre Syndrome
AIDP: Acute Inflammatory Demyelinating
Polyneuropathy (80-90%)
AMAN: Acute Motor Axonal Neuropathy
AMSAN: Acute Motor Sensory Axonal
Neuropathy
MFS: Miller Fisher Syndrome

Guillain-Barre Syndrome
Clinical (AIDP, AMSAN)
» Paresthesias
» Ascending weakness
» Face
» Mostly symmetric
» Absent DTRs
» Autonomic
Studies
» High CSF protein
» Slow nerves
Course
» Max weakness < 4wks
» Slow recovery
» 85% do very well
» 10% disabled
» 5% die
Treatment
» Avoid complications
» Plasmapheresis
» IVIG

Diabetic Neuropathy
Symmetric
» Distal sensory
» Autonomic
» Proximal lower limb
» Acute cachectic
» Treatment induced
Focal
» Cranial nerve
– Pupil sparing 3rd
» Mononeuropathy
– Limb
– Trunk
» Proximal lower limb

AAN Consensus
Conclusion: Patients with distal symmetric sensory polyneuropathy have a relatively high prevalence of diabetes or pre-diabetes (impaired glucose tolerance), which can be documented by blood glucose, or GTT (Class III).
Recommendation: When routine blood glucose testing is
not clearly abnormal, other tests for pre-diabetes (impaired
glucose tolerance) such as a GTT may be considered in
patients with distal symmetric sensory polyneuropathy,
especially if it is accompanied by pain (Level C).

Neuropathy Work-up
Diabetes
B12 + methylmalonic acid
SPEP
JD England, et.al. Practice Parameter: Evaluation of distal symmetric
polyneuropathy: Role of laboratory, genetic, and autonomic testing;
nerve biopsy; and skin biopsy (an evidence-based review).
Neurology 2009;72:185

Treatment
V Bril, et. al. Evidence-based guideline: Treatment of painful
diabetic neuropathy. Neurology. 2011; 76:1758
Recommendation
Level A 2+ class 1 studies Pregabalin
Level B 1 class 1 study or Gabapentin, Sodium valproate
2 class 2 studies Duloxetine, Venlafaxine,
Amitriptyline, Tramadol, Opiates,
Capsaicin, TENS
Level U No class 1-3 studies Topiramate, SSRI, nortriptyline,
Insufficient evidence Lidocaine, Alpha lipoic acid
Not helpful Evidence against Lamotrigine, Oxcarbazepine,
Lacosamide, Mexilitine, Laser

Complex Regional Pain Syndrome
A chronic, progressive disease often limited to one
body region (arm, leg), following a noxious event and
characterized by severe pain (allodynia), autonomic
dysregulation, swelling, skin and bony changes.
Types
» I = No demonstrable nerve injury (90%) (formally called reflex
sympathetic dystrophy)
» II = Nerve injury (formally called causalgia)
Best treatment is early and often use of the limb

ARS Question
This 38 year-old man has SOB, trouble smiling and chewing, and mild
proximal arm weakness. Both diplopia and ptosis are present. The
symptoms are better in the morning and after rest. They are worse
when reading, walking, and lifting.
Which two tests will help confirm your diagnosis?
A. CPK and brain MRI
B. Repetitive nerve stimulation and CPK
C. Repetitive nerve stimulation and brain MRI
D. Ach Rec Abs and brain MRI
E. Repetitive nerve stimulation and Ach Rec Abs

Myasthenia Gravis
Definition: autoimmune
disease of the
neuromuscular junction
characterized by fatigable
weakness
Antibodies against multiple
epitopes on the muscle side
» Acetylcholine Rec
» MuSK (Muscle Specific
Kinase)
Types
» Generalized 85%
» Ocular 15%
» Neonatal
– Abs from mother

Myasthenia Gravis
Clinical
» Fatigability
» Ptosis and diplopia
» Sensory normal
» Reflexes maintained
» Bedside maneuvers
Diagnosis
» H&P
» Repetitive stimulation
» Antibodies
» Tensilon test
» Chest imaging

Myasthenia Gravis
Treatment
» Thymectomy (not MuSK)
» Anticholinesterase agents
» Immunosuppression
» Immunomodulation (plasmapheresis, IVIG)

ARS Question
This 39 year-old woman has recurrent
episodes of staring with inability to get her
attention. Duration ~30 secs. Started one
month ago after a car accident in which she
hit her head.
How should we classify her seizures?
A. Myoclonic
B. Complex partial
C. Simple partial
D. Absence
E. Generalized
EEG

ARS Question
A 53 yo man presents with loss of consciousness
and is witnessed to have whole body shaking for
10 secs and is sweaty. He wakes up immediately
and can talk.
You make a presumptive diagnosis and suggest a
work-up for:
A. Syncope
B. Alcohol withdrawal
C. Seizure
D. Conversion d/o
E. Illicit drug use

Classification
Partial onset
» Simple partial
» Complex partial
» Secondarily
generalized tonic-
clonic
Generalized onset
» Absence
» Myoclonic
» Atonic
» �Tonic
» Clonic
» Tonic-clonic
Partial Onset Seizure
Partial = focal
Simple
» Consciousness normal
» Smell, taste, vertigo, fear,
etc.
Complex
» Consciousness altered
» Blinking, lip smacking,
vocalizations, etc.

Partial Onset Seizure
Secondarily
generalized
Tonic-clonic

Generalized Onset Seizure
Source?
» Deep structure
EEG
» Bilateral synchronous
discharges
Genetic
Onset usually before
age 20

Differential Diagnosis
Syncope
» Definition: Loss of
consciousness due to
insufficient blood flow to
the brain
Migraine
Sleep d/o and
narcolepsy
TIA
Movement disorder
Psychiatric
Cardiac arrhythmia
Blood flow obstruction
» Structural cardiac dis
» Structural
cerebrovascular dis
Orthostatic hypotension
Neurally-mediated

Syncope vs. Seizure
Syncope
» LOC
» Tonic-clonic
– 5-15 sec.
» Urinary incontinence
» Tongue bite
» Low BP
» No post-ictal period
Seizure
» LOC
» Tonic-clonic
– 10-120 sec.
» Urinary incontinence
» Tongue bite
» High BP
» Post-ictal period

ARS Question
A 25 year-old male was brought to the ER after dropping
in the hallway in front of co-workers who describe tonic-
clonic activity. Four more seizures occurred while in
transport and you witness another in the ER. He never
regains consciousness in between.
You make a presumptive diagnosis and order what
emergent intervention first:
A. Benzodiazepines
B. MRI head
C. ABG
D. Neurology consult
E. Tox screen

Status Epilepticus
ABCs
IV
Labs
» ABG
» Toxicology
» Drug levels
» CBC, M7
Head CT?
Immediate drugs
» Benzos (diazepam,
lorazepam)
» Followed by…(phenytoin,
phenobarbital)
Refractory status
» Intubate
» Paralyze
» Continuous EEG
» Other drugs
ARS Question
A 16 yo female was hit in the head playing soccer.
Brief LOC if at all. She is dizzy on the sideline and
can’t answer questions about the score.
Can she go back in the game?
A. Now
B. Next game
C. Next year
D. Never
E. Only when her symptoms have improved.

Concussion
GCS of 13-15, measured at 30 min after acceleration, deceleration or contact forces to head
Loss of consciousness (<10%)
Typically with grossly normal imaging
Symptoms » Amnesia (post-traumatic, retrograde)
» Attention deficit
» HA, dizziness, blurred vision

Management
Sports » Graded return to play.
No symptoms at rest mild activity full contact.
Medications » None specific
» Symptomatic
Acute
» ABC’s
» Spine immobilization
» Head CT rules
Subacute
» Physical and mental rest

Prognosis
Post concussive syndrome
» Variable definition: symptoms remaining (7 days, 4 weeks, 3
months) after the mild TBI
» More prevalent in pts w/ depression or anxiety prior to injury
» Uncommon in children
» Longer duration of sx when involved in litigation
Vast majority (85-90%) better by 3 months

Question?
Early in the disease process
Dementia
» Normal level of consciousness
» Decreased content of consciousness
Delirium
» Altered level of consciousness (sleepy, obtunded or hyperactive)
» Acute or subacute
» Fluctuating
» Disorientation to place and time
» Hallucinations
» Large differential
What is the level of consciousness?
Dementia Delirium
Next question

Question?
Depression
» Screen
» Medication trial
» Neuropsychological testing
Is the patient depressed?
Dementia Pseudodementia
Next question
Example Case
This is an 64 year-old male who comes to the office alone to
discuss memory loss. His wife died 2 years ago of breast cancer.
His children live on the east coast. He used to like playing golf but
rarely joins his friends for a round. Sleep is disrupted and he wants
a sleeping pill. On exam he sighs a lot and doesn’t try to answer
the “day”.
Pseudodementia (depression)
Question?
Not easy to tell the difference. Time may be needed.
Normal changes » Forgetfulness » Small pupils » Decreased upgaze » Increased muscle tone » Impaired vision, smell, hearing, taste
Dementia definition » Decline in cognitive functioning severe
enough to impair activities of daily life or independence.
» Memory loss is almost always an early feature. Plus….
» Disorder of language, apraxia (motor function), agnosia (recognition), executive function (behavior, directions).
Could it be normal aging?
Dementia Age-related
Next question
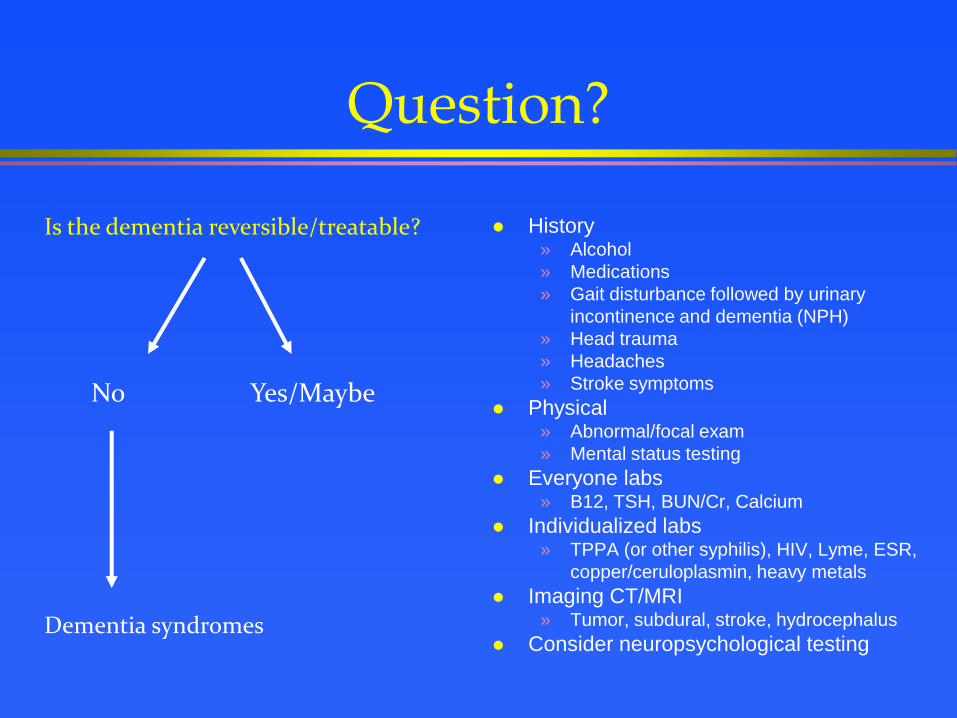
Question?
History » Alcohol
» Medications
» Gait disturbance followed by urinary
incontinence and dementia (NPH)
» Head trauma
» Headaches
» Stroke symptoms
Physical » Abnormal/focal exam
» Mental status testing
Everyone labs » B12, TSH, BUN/Cr, Calcium
Individualized labs » TPPA (or other syphilis), HIV, Lyme, ESR,
copper/ceruloplasmin, heavy metals
Imaging CT/MRI » Tumor, subdural, stroke, hydrocephalus
Consider neuropsychological testing
Is the dementia reversible/treatable?
No Yes/Maybe
Dementia syndromes

AAN Dementia Workup Recommendations
B12
Thyroid function testing
Dementia Screening
Neuroimaging

Example Case
This is a 77 year old female who is brought to the clinic by her
family. They are greatly concerned because the patient has been
talking about gremlins climbing the walls in her apartment for three
weeks. The family investigated but found nothing out of the
ordinary. On further questioning the family reports memory difficulty,
increased sleep, and walking trouble with two falls in the last 4
months. On exam she needs to push to get out of the chair, has a
slow walk, and there is mild arm cogwheel rigidity.
Diffuse Lewy-body disease

Example Case
This is a 53 year old female who is brought to the clinic by her
family because of change in personality over 1 year. She used to
be a quiet church going woman, but has recently been growing
more vulgar, and the other day began cursing in the middle of a
church service when her tic-tacs spilled out of her purse. Her family
reminds her to shower or she won’t for days. Her apartment is
always a mess. The patient is frustrated, and says there is nothing
wrong with her, and doesn’t know why her family is treating her so
poorly. She says she is sharp as a tack, spitting out the day, week,
month, season, and year without any difficulty.
Frontotemporal dementia: behavioral variant

Example Case
This is an 82 year-old male who is brought to your office by his son.
The son reports that there has been a gradual decline in his
father’s memory over the past three years. One month ago while
out on a walk he got lost, and was found by police wandering a
rough part of the neighborhood. Recently the family has taken over
financial responsibilities for him, after he wrote a check for $10,000
to his cable company. The MMSE score is 18/30, but he is
otherwise physically well.
Alzheimer disease

Alzheimer: Treatment
Neuro protection: NONE
Cholinesterase inhibitors:
» Mechanism: augment cholinergic function
» Donepezil: mild/moderate/severe dementia
» Rivastigmine, Galantamine: mild/moderate dementia
NMDA receptor antagonist
» Mechanism: antagonizes glutamate at NMDA receptor, may
improve signal transmission
» Memantine: moderate/severe dementia
Modest effects
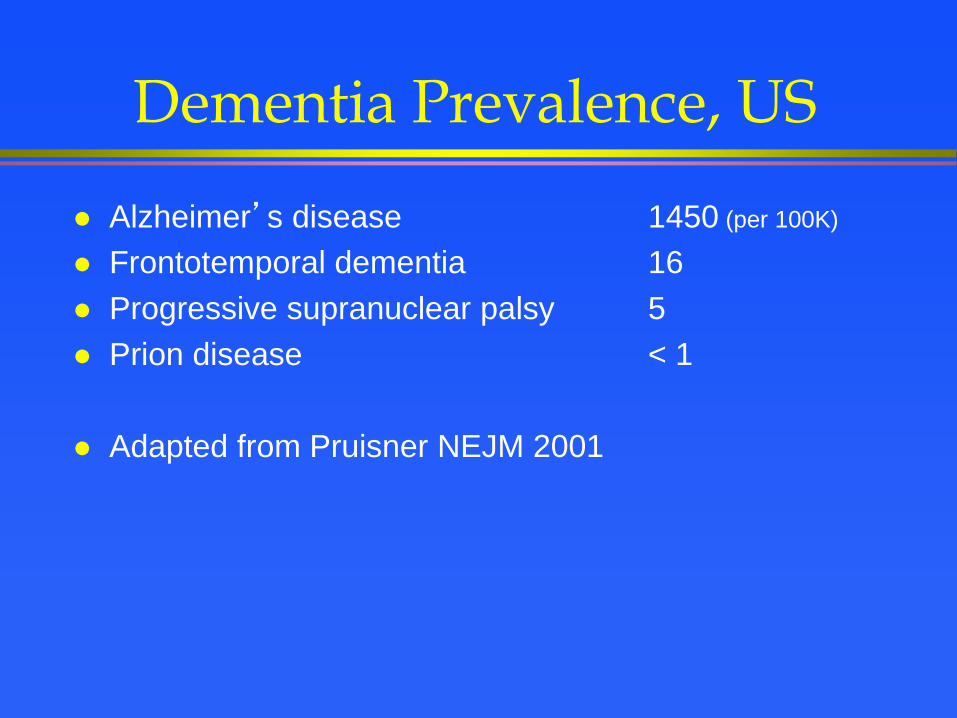
Dementia Prevalence, US
Alzheimer’s disease 1450 (per 100K)
Frontotemporal dementia 16
Progressive supranuclear palsy 5
Prion disease < 1
Adapted from Pruisner NEJM 2001

ARS Question
A 16 month-old boy is not meeting motor milestones. He
sat late and is not yet scooting on the floor. Your exam
shows spastic legs with increased DTRs.
You make a presumptive diagnosis and ask questions
about:
A. Prematurity
B. Language delays
C. Head circumference
D. Kernicterus
E. All of the above
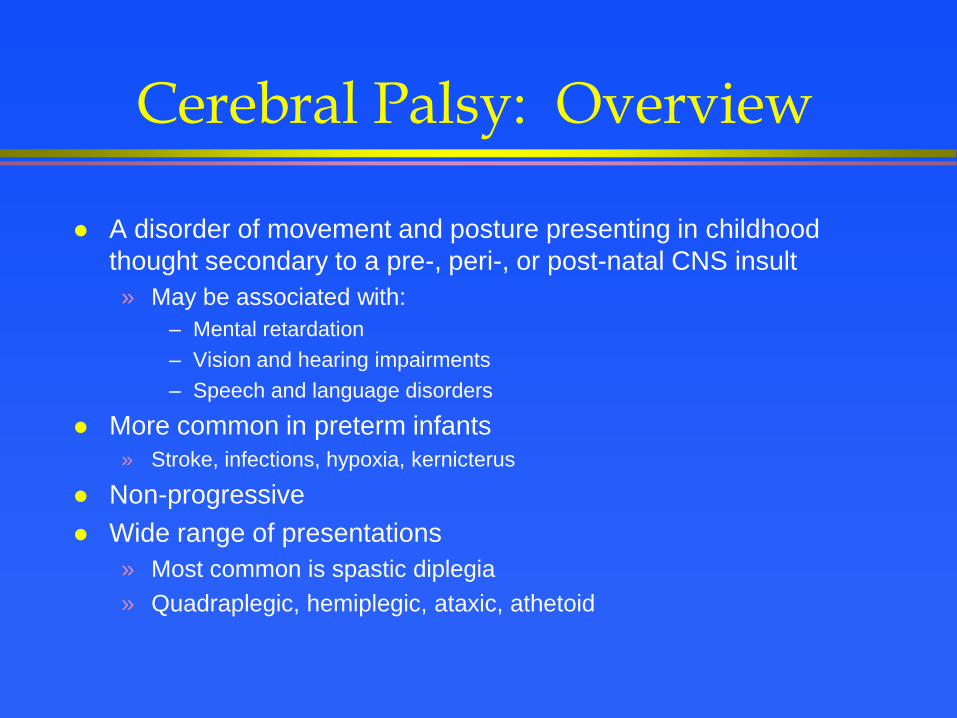
Cerebral Palsy: Overview
A disorder of movement and posture presenting in childhood
thought secondary to a pre-, peri-, or post-natal CNS insult
» May be associated with:
– Mental retardation
– Vision and hearing impairments
– Speech and language disorders
More common in preterm infants
» Stroke, infections, hypoxia, kernicterus
Non-progressive
Wide range of presentations
» Most common is spastic diplegia
» Quadraplegic, hemiplegic, ataxic, athetoid
END