Embed Size (px)
Citation preview
TEMPLATE DESIGN © 2008
www.PosterPresentations.com
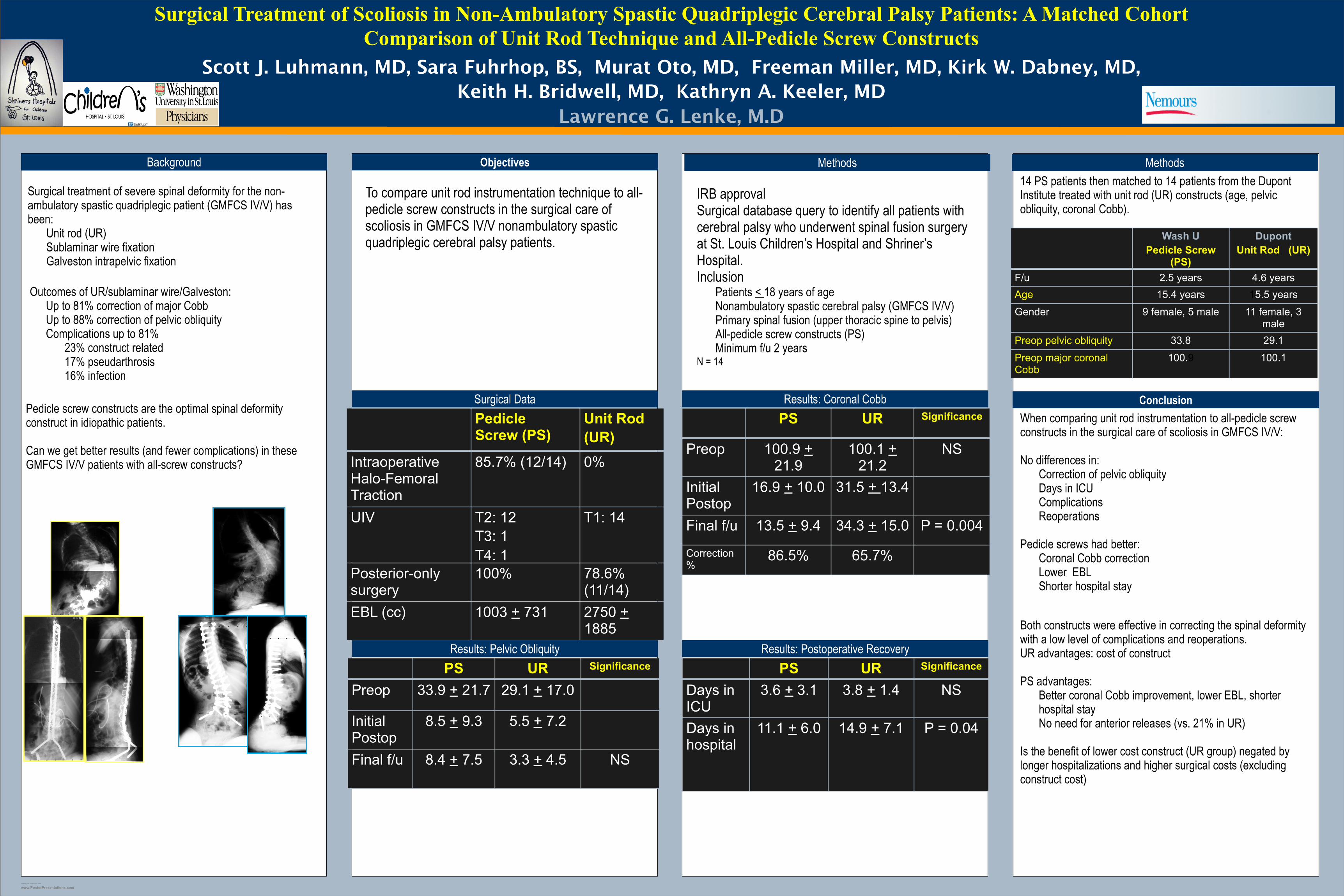
Surgical Treatment of Scoliosis in Non-Ambulatory Spastic Quadriplegic Cerebral Palsy Patients: A Matched Cohort Comparison of Unit Rod Technique and All-Pedicle Screw Constructs
Scott J. Luhmann, MD, Sara Fuhrhop, BS, Murat Oto, MD, Freeman Miller, MD, Kirk W. Dabney, MD, Keith H. Bridwell, MD, Kathryn A. Keeler, MD
Lawrence G. Lenke, M.D
Background Methods
Surgical Data
Results: Pelvic Obliquity
Conclusion
Results: Postoperative Recovery
Surgical treatment of severe spinal deformity for the non-ambulatory spastic quadriplegic patient (GMFCS IV/V) has been:
Unit rod (UR)Sublaminar wire fixationGalveston intrapelvic fixation
Objectives
To compare unit rod instrumentation technique to all-pedicle screw constructs in the surgical care of scoliosis in GMFCS IV/V nonambulatory spastic quadriplegic cerebral palsy patients.
IRB approvalSurgical database query to identify all patients with cerebral palsy who underwent spinal fusion surgery at St. Louis Children’s Hospital and Shriner’s Hospital. Inclusion
Patients < 18 years of ageNonambulatory spastic cerebral palsy (GMFCS IV/V)Primary spinal fusion (upper thoracic spine to pelvis)All-pedicle screw constructs (PS)Minimum f/u 2 years
N = 14
Outcomes of UR/sublaminar wire/Galveston:Up to 81% correction of major CobbUp to 88% correction of pelvic obliquityComplications up to 81%
23% construct related17% pseudarthrosis16% infection
Pedicle screw constructs are the optimal spinal deformity construct in idiopathic patients.
Can we get better results (and fewer complications) in these GMFCS IV/V patients with all-screw constructs?
When comparing unit rod instrumentation to all-pedicle screw constructs in the surgical care of scoliosis in GMFCS IV/V:
No differences in:Correction of pelvic obliquityDays in ICUComplicationsReoperations
Pedicle screws had better:Coronal Cobb correctionLower EBLShorter hospital stay
Both constructs were effective in correcting the spinal deformity with a low level of complications and reoperations.UR advantages: cost of construct
PS advantages:Better coronal Cobb improvement, lower EBL, shorter hospital stayNo need for anterior releases (vs. 21% in UR)
Is the benefit of lower cost construct (UR group) negated by longer hospitalizations and higher surgical costs (excluding construct cost)
14 PS patients then matched to 14 patients from the Dupont Institute treated with unit rod (UR) constructs (age, pelvic obliquity, coronal Cobb).
Wash UPedicle Screw
(PS)
DupontUnit Rod (UR)
F/u 2.5 years 4.6 yearsAge 15.4 years 15.5 years
Gender 9 female, 5 male 11 female, 3 male
Preop pelvic obliquity 33.8 29.1
Preop major coronal Cobb
100.9 100.1
Results: Coronal CobbPedicle Screw (PS)
Unit Rod (UR)
Intraoperative Halo-Femoral Traction
85.7% (12/14) 0%
UIV T2: 12T3: 1T4: 1
T1: 14
Posterior-only surgery
100% 78.6% (11/14)
EBL (cc) 1003 + 731 2750 + 1885
PS UR Significance
Preop 100.9 + 21.9
100.1 + 21.2
NS
Initial Postop
16.9 + 10.0 31.5 + 13.4
Final f/u 13.5 + 9.4 34.3 + 15.0 P = 0.004
Correction %
86.5% 65.7%
Methods
PS UR Significance
Preop 33.9 + 21.7 29.1 + 17.0
Initial Postop
8.5 + 9.3 5.5 + 7.2
Final f/u 8.4 + 7.5 3.3 + 4.5 NS
PS UR Significance
Days in ICU
3.6 + 3.1 3.8 + 1.4 NS
Days in hospital
11.1 + 6.0 14.9 + 7.1 P = 0.04












![UIV GSJnews.gifucity-tower43.jp/pdf/20160901-0930c.pdf · UIV GSJ Þ ¯ÔA¨xb o k pbyÞ Ö Ý¯t zA¨~ º 0U !Ëts ÔùU]_M byÞø x Ý ´pb åï½·¿Ä ¦ Ì §: ¨wVw\q0 Þ] w](https://img.dokumen.tips/doc/110x75/5f64bf84550a6253db7d2c05/uiv-uiv-gsj-axb-o-k-pby-t-za-0u-ts-um-by-x.jpg)


![2002 TEÓRICA 16 [Só de leitura]clinicauniversitariaradiologia.pt/aulas_teoricas/teoricas16.pdf · • no decurso de UIV • Ascendente (retrógrada) • contraste não diluído](https://img.dokumen.tips/doc/110x75/5be3f88809d3f281048c77a3/2002-teorica-16-so-de-leituraclinicauni-no-decurso-de-uiv-ascendente.jpg)













