Embed Size (px)
Citation preview

'43
SURGICAL TREATMENT OF CHRONIC GASTRICAND DUODENAL ULCER
By RODNEY MAINGOT, F.R.C.S.Surgeon, Royal Free Ho;pital; Senior Surgeo?a Svuthend General Hospital
Much of the confusion of thought and teachingwhich now exists regarding the surgical manage-ment of patients suffering from chronic gastric andchronic duodenal ulcer arises from the fact that inrecent years it has become customary to class thesetwo conditions together as one disease-pepticulcer.
It is true that chronic gastric and chronicduodenal ulcer have certain features in common;the early signs and symptoms presented by thetwo conditions are in many respects similar, theacid gastric chyme plays an all-important role inthe perpetuation of the lesions, and the medicalmeasures advocated for their treatment are almostidentical.
Nevertheless, the risk of malignant transforma-tion, the degree of morbidity and the potentialitiesof disaster with the accompanying economic dis-turbances are factors which differ widely accordingto whether they are associated with chronicduodenal ulcer or with chronic ulcer of thestomach.
Cancerous. degeneration of a duodenal ulcer issuch a rare event as to constitute a pathologicalcuriosity, but the malignant transformation of agastric ulcer is a potent factor to be reckoned within treatment, and is indeed an ever-present menacewhich cannot be ignored.
The surgical treatment of these two diseases alsovaries in many important details, and it is for thesereasons in particular that I propose to discuss themseparately.
(A) Chronic Gastric Ulcer(1) Indications for OperationThe main indications for operative interference
may be detailed as follows(a) Acute perforation.(b) Intermittent or continuous haemorrhage
arising from the base of a chronic gastric ulcerwhich efficient medical qxeasures are incapable ofarresting.
(c) Anatomical organic deformity of the stomachdue to stenosing ulceration and associated with
progressive loss of weight; (i) hour-glassstomach; and (ii) pyloric obstruction.
(d) Failure of healing of the ulcer despite pro-longed (four-eight weeks) and well-supervised in-patient medical treatment.
(e) Recurrence of ulceration following (i) one ormore courses of in-patient medical treatment; (ii)simple suture of an acute perforation; (iii) -wedge-or V-excision of the ulcer or other type of un-suitable operation; or (iv) transgastric transfixionand obliteration by sutures of the ulcer crater toicontrol severe haemorrhage.
(f) Multiple chronic gastric ulcers or combinedgastric and duodenal ulcer.
(g) The suspicon of malignancy which cannot beexcluded by combined clinical, biochemical,radiological and gastroscopic examination.
(h) The patient is 6o years of age or over,having an ulcerating lesion in the stomach, andgiving' a short history of dyspepsia.
(i) Ulcers situated on or about the greater curva-ture of the stomach or in the pyloric region.
(j) A large gastric ulcer which has penetrateddeeply into the substance of the pancreas or liver.
(k) Expedient circumstances and economicreasons in certain-instances, e.g., indigent patients,mental cases with callous lesions, etc.
(2) Some Factors Influencing the Choiceof TreatmentEvery patient is subjected to the same routine
clinical methods of investigation, and if thepresence of an ulcer in the stomach has beendemonstrated by means of X-rays, and in certaincases by gastroscopy, the physician and surgeonshould meet in consultation and decide themethod of treatment to be undertaken. Thefollowing factors will influence the choice oftreatment
(a) Hour-Glass Deformity. This lesion, whichis due to a stenosing ulcer of the stomach, is ex-tremely rare in men (about 2 per cent.) andseldom responds to medical therapy. In the-absence of other contra-indications gastric re-section is the best form of treatment.
by copyright. on January 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.24.269.143 on 1 March 1948. D
ownloaded from

POST GRADUATE MEDICAL JOURNAL March 1948
In women it is conceivable that medical treat-Iment, or rather stringent dietetic measures, maymaintain a state of nutrition compatible withtolerable health if on healing the ulcer has left asmall but adequate channel for the passage of food.But the majority of such patients are elderly orhave suffered from dyspepsia for many years andhave become chronic invalids; sooner or laterpartial gastrectomy (for choice) or gastro-gas-trostomy (when gastric resection is not feasible)must be performed to overcome the effects ofobstruction.
I would regard hour-glass deformity associatedwith progressive loss of weight and strength as adefinite indication for operative interference at anyage, and I have successfully performed partialgastrectomy (under local anaesthesia) upon patientswho were aged 71, 75, 78 and 8i respectively, withgood immediate and late results.
(b) The Age of the Patient. With RoscoeGraham (1937) and other surgeons,-I have so farfailed to find a simple chronic gastric ulcer whichhas not been accompanied by clinical Evidence ofits presence in a patient under 6o years of age. Inother words, I believe that all gastric ulcers whichmake their appearance after 6o years of age areulcerating carcinomata, and the patient should beadvised to have a partial or subtotal gastrectomyperformed as soon as adequate pre-operativepreparation permits.
Patients under the age of 40 who give a relativelyshort history of ulcer and who on barium mealX-ray examination are found to have a 'smallniche on the vertical portion of the lesser curvatureare best treated medically. Patients who show asatisfactory response to medical therapy should beexamined at intervals over a period of some yearsto ensure that the healed area in the stomach isstaunch.Aged and infirm patients respond poorly to
medical measures, but the risks of operative in-terference may be considerable. Each case has tobe judged on its own merits, but the bias would,on the whole, be in favour of medical treatment.
(c) Sex. The proportion of men to womensuffering from gastric ulcer is about three to one,but gastric resection is called for in approxi-mately four times as many men as women. Thereis, however, considerable variation in these pro-portions in different parts of Great Britain andeven in different quarters of any large city. Myexperience has been that malignant degenerationof a gastric ulcer is commoner in women than inmen.
(d) The Position of the Ulcer. It is frequentlystated that ulcers situated on or near the greatercurvature of the stomach or in the pyloric (egionare commonly malignant in character, and that
they require surgical attention as soon as they arediagnosed. Matthews (I935), who described twopersonal cases and analysed 139, voices the opinionheld by most surgeons. He writes:
' Ulcers of the greater curvature produce nocharacteristic symptoms distinguishing them fromother peptic ulcers. There is no certain method ofdetermining whether a lesion found on thegreater curvature ig benign or malignant, exceptby histological examination. A review of thecases described illustrates how difficult it may beto differentiate this type of peptic ulcer fromcarcinoma.'
Simple ulcers of the greater curvature are rare,and less than 200 cases have been reported to date.As these 'lesions are easily visualized on gas-troscopy and on barium meal X-ray examination,their response to the therapeutic test can be closelyobserved.
In a personal series of six cases of chronic ulcerof the greater curvature, four were subjected togastric resection, and the microscopic examinationof the lesions proved that two were innocent andtwo were malignant. In the other two cases, asthe clinical, radiological and (in one case) gastro-scopic evidence supported the diagnosis of simpleulceration, medical treatment was given a trialwhich proved to be successful, as the ulcer ap-peared to be healed soundly in each case withinsix weeks. Subsequent examinations of thesecases has shown the healing to be satisfactory.
Ulcers of the greater curvature should be treatedon their merits. If the presence of malignancycannot be ruled out after expert investigation, or ifthe crater stubbornly refuses to shrink following acourse of intensive medical treatment, then it iswiser and safer to operate than to wait and see.In my opinion, the majority of ulcerating lesionsof the greater curvature can. be diagnosedaccurately by modern methods, and I considerthat the incidence of malignancy in circum-scribed lesions in this 'particular part of thestomach has been exaggerated. I do, however,believe with Holmes and Hampton (I932) andFinsterer (1934) that gastro-duodenal' resection isthe best form of treatment for chronic ulcers of thepyloric region, as they are frequently cancerous innature, leisurely or obstinate in their response tomedical therapy, 'and a cause-though by nomeans the commonest-of pyloric obstruction.When this area is the seat of a small destructive
lesion visualization through a gastroscope is oftenimpossible or fleeting at best; serial X-raypictures of the belladonna- and barium-filledwrithing spastic gastric. outlet usually fail todemonstrate the niche, the meniscus, or the tell-tale filling defect; and the clinical picture, is thatof a low-grade or established obstruction with its
by copyright. on January 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.24.269.143 on 1 March 1948. D
ownloaded from

March i948 MAINGOT: Surgical Treatment of Chronic Gastric and Duodenal Ulcer
accompanying cramp-like epigastric pain,vomiting, dehydration and decline in weight.
(e) The Presence of Multiple Chronic Ulcers inthe Stomach as well as the Combination of GastricUlcer plus Duodenal Ulcer. It is generally agreedthat, where found, such combinations are sufficientto warrant surgical meas,ures.
I once performed subtotal gastrectomy upon apatient who had two chronic ulcers in the stomach,one being situated on the lesser curvature aboutthe incisura, and the other directly opposite on thegreater curvature. The lesser-curve ulcer wasbenign, but on the greater curvature was anulcerating carcinoma.
Multiple chronic gastric ulcers are seen in about3 per cent. of resected stomachs, whilst chronicgastric ulcer is associated with a chronic duodenalulcer in some I2 per cent. of the cases subjectedto operation.
(f) The Size of the Ulcer. It was hoped at onetime that the size of the 'ulcer as revealed onbarium meal X-ray examination and/or on gastro-scopy might be a good index of its character. It istrue that the majority of ulcers over one inch indiameter are carcinomata while most of the smallerulcers prove to be innocent. There are, however,so many exceptions to this general rule that it isalmost valueless as a guide to treatment in theindividual case.The large gastric ulcer which has breached all
the coats of the stomach and the base of whichlies deeply in the substance of the pancreas orliver may, of course, be the seat of malignanttransformation. Such ulcers, nevertheless, some-times show remarkable powers of recuperation andretrogression on gastric intubation, which pro-vides rest to the inflamed organ whilst the nourish-ment and strength of the patient are maintained(Freeman, I944).
Relapses or rather recurrence of ulcerationfollowing a course of ' home treatment' are therule. The large penetrating gastr?c ulcer is not asurgical emergency. Many of the deaths followinggastric resection for such ulcers are due to a lackof genera.lship on the part of the surgeon;. tohasty pre-operative management; to insufficientrehabilitation of the patient; and to the per-formance of a major surgical undertaking on aviscus which is friable and sodden withinflammatory products.
These cases demand prolonged hospitalization;continuous feeding through an indwelling Ryletube employing the milk-drip method; thesystematic administration of alkaline draughts;sedative drugs; the essential vitamins in fulldosage; transfusion of blood before, during andafter operation; periodic screening of the ul-cerated zone to determine the response to the
treatment which has been given; and the selectionof the optimum time for operation, namely, whenthe lesion appears to be healing satisfactorily andthe patient's general condition shows an all-roundimprovement.On occasion the irremovable duodenal ulcer is
encounted on coeliotomy, but intubation and feed-ing through a Ryle tube, sustained for some weeks,have rendered all-or nearly all-gastric ulcersresectable.
(g) Response to Medical Treatment. Everypatient with an active gastric ulcer should, ideally,be investigated and treated as an in-patient in awell-equipped hospital or clinic. But in thiscountry there are not at present sufficient hospitalbeds available to treat all patients on theselines.The medical treatment of ulcer of the stomach
is a social, psychological, economic, and dieteticproblem. Many patients cannot afford the timeand expense incurred by prolonged hospitalization,and the majority, owing to nervous tension,anxiety 'about the future, and worry concerningfamily affairs, are unable or unwilling to give theirfull, whole-hearted co-operation. To be success-ful, medical treatment must be thorough, pro-longed, well-supervised, and conducted by oneWho has made a special study of this subject.Some ulcers will not heal even under the besttherapy; they are indolent or malignant and callfor surgical enquiry. Others, on the other hand,heal soundly, as can be proved by periodicalgastroscopic and radiological examination. Activetreatment must be continued until healing is com-plete and final ; the risk of recurrence is a veryreal one, and it may be emphasized here that themajority of so-called recurrences are not, in fact,recurrences at all, but lesions which have nevercompletely healed.
It is now generally accepted that complete dis-appearance of symptoms with a gain in weightwhen the patient is subjected to medical treatmentis no evidence that the ulcer is benign, since acancerous gastric lesion will, on occasion, respondin this manner when it presents irrefutable X-rayevidence of its malignancy. 'the disappearance ofthe crater as shown on X-ray films, although afavourable sign, does not necessarily imply that theulcer has healed. The crater may at times be-come obliterated by exuberant cancer cells whichhave tipped over into the niche from the malignantmargin, or it may be temporarily filled withpoorly-nourished, oedematous granulation tissuewhich has made a brave but ephemeral attempt atbridging the gap. It is also by no means excep-tional to find on gastroscopy that the ulcer hashealed well, but that months later a sinister moundof actively-growing carcinoma cells has arisen from
by copyright. on January 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.24.269.143 on 1 March 1948. D
ownloaded from

146 POST GRADUATE MEDICAL JOURNAL March 1948
the ill-fated scarred area in the stomach to threatenthe life of the patient.
Surgery will therefore be called for in the greatmajority of patients suffering from chronic gastriculcer. The case which appears to respond satis-factorily to medical management should be care-fully followed up over a long period, as the chancesof recurrence of ulceration are great. When re-currence does take place it is almost impossiblepre-operatively to exclude, by the means at ourdisposal, the possibility of cancerous change inthe margin of the ulcer.
(3) Choice of Operation(a) Acute Perforation of a Gastric Uker. The
object of operation in acute perforation is to savethe patient's life by a simple expeditious procedure.The operation which fulfils this requirement issimple suture by the method advocated by RoscoeGraham (I937). Three sutures are passed, onethrough the margins of the hole in the stomach,one above and one below. Then, after drawing agenerous amount of great omentum over theperforation, the sutures are securely tied, thuseffectively sealing off the puncture. Operationssuch as excision of the ulcer, gastro-jejunostomy,or partial gastrectomy, should not, in my opinion,be performed in the presence of this catastrophe.If later, however, in the quiescent period ofmedical treatment the ulcer proves refractory, asit does in a fairly large proportion of such cases,then the claims of gastric resection will have tobe considered.
(b) Haemorrhage. The prognosis is best inpatients under the age of 40 and in women.Medical treatment is instituted in all cases inwhich massive bleeding from a chronic gastriculcer occurs. If there 1s evidence of continued orrecurrent haemorrhage after medical therapy hasbeen carried out for 48 hours, it is my view that asurgical attack should be made upon the ulcerwithout further delay. The patient is given anopportunity to respond to conservative treatment,but if this response is not satisfactory in 48 hours Iwould advise immediate laparotomy.The outlook is grave after the age of 50 and in
those with large penetrating lesions. When opera-tion is indicated the surgeon has a choice of twoprocedures: (i) detaching the ulcer from itssclerotic base and closing the hole in the stomach;or (ii) performing partial gastrectomy. Theformer operation is reserved for the desperatecase and the latter for the expert.
(c) Hour-Glass Stomach. Gastro-gastrostomy,i.e., anastomosis of the proximal and the distalpouches of the stomach, is a simple, effectiveoperation which should be carried out in frailelderly subjects when the isthmus is situated high
up in the stomach and the patient is obviously notfit enough to withstand the ordeal of gastric re-section. In most cases, however, partial gastrec-tomy, performed under local or cyclopropaneanaesthesia, is a safe and satisfactory procedureassociated with a low death-rate.
(d) Chronic Gastric Ulcer or Ulcer-Cancer.During the last 50 years a large number of opera-tions have been recommended for the unresponsivegastric ulcer and I have practised most of them atone time or another. During the last ten years Ihave abandoned the following operations, as theimmediate or late results were unsatisfactory in ahigh proportion of the cases: (i) excision alone;(ii) gastro-jejunostomy alone (von Hacker); (iii)wedge- or V-excision of the ulcer followed bygastro-jejunostomy; (iv) cautery excision ordestruction of the ulcer followed by gastro-jejunostomy (Balfour); (v) segmental or sleeveresection (Riedel-Rodman); (vi) excision of apyloric ulcer combined with pyloroplasty (Judd);(vii) partial gastric exclusion (Devine); (viii)cholecysto-gastrostomy (Braithwaite); and (ix)jejunostomy.
I have, in a previous issue of this Journal(I942) and in my work 'Abdominal Operations'(I940), set forth at some length the reasonswhich led me to abandon all of the proceduresenumerated above.
Following the advice of Allen, Cave, WaltmanWalters, Lahey and other surgeons, vagotomyshould not be employed in the treatment of chronicgastric ulcer.
Dockerty, of the Mayo Clinic, told me that i8per cent. of the gastrectomy-specimens referred tohim and diagnosed macroscopically as simplepeptic ulcer proved on microscopic investigation(of a large number of serial sections) to be under-going malignant change in the margin of theulcer.When we operate for chronic ulcer of the
stomach we should do so as for cancer of thisorgan. I do not know what percentage of gastriculcers undergo malignant change or what pro-portion of lesions diagnosed as gastric uleer are, infact, ulcerating carcinomata. But I do know thatif operation is undertaken only on those caseswhich prove unresponsive to stringent medicaltreatment or on neglected cases with sizeablelesions, the microscope will reveal the presence ofcancer cells in some IO-20 per cent. of cases.A study of 50 of my own gastrectomy specimens
(women only) showed ' ulcer-cancer" or ' ul-cerating carcinoma' in i i of the cases diagnosedpre-operatively as chronic peptic ulcer of thestomach.The operation of choice for suspected ulcer-
cancer, indolent ulcer or recurrent ulcer is sub-
by copyright. on January 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.24.269.143 on 1 March 1948. D
ownloaded from

March i948 MAINGOT: Surgical Treatment of Chronic Gastric and Duodenal Ulcer
total gastrectomy by one of the following methods:(i) anterior Polya-Hofmeister; (ii) posterior Polya-Hofmeister ; -(iii) Billroth I types-Finochietto'sfor preference.The anterior Polya-Hofmeister operation, which
has been carried out in go per cent. of my cases,is the one of choice for the following reasons: (i)the anastomosis is readily performed near theaccessible greater curvature by construction of aHofmeister valve; (ii) post-operative obstructivesymptoms and the sensation of fullness after mealsare obviated; (iii) the technique is simple and themortality under 4 per cent.; and (iv) in the rareevent of jejunal ulceration the implicated visceraare approached with ease.The posterior Polya-Hofmeister operation may be
called for when the mesentery of the jejunum isshort or where for some special reason a partialrather than a subtotal gastric resection is indicated.Obstructive symptoms are decidedly more com-mon with the posterior operation, due perhapspartly to the proximal and distal jejunal limbsbecoming tethered together in the funnel of re-tracting mesocolon.The technical beauty of Finochietto's modifica-
tion of the Billroth I method has always appealedto me, and when I am constrained to perform anaxial anastomosis between the cut ends of stomachand duodenum I choose this procedure. TheBillroth I operation is indicated in feeble senilepatients; where the infracolic compartment isshrouded in adhesions (the aftermath of a previousperitonitis); or where the supporting structures ofduodeno-jejunal flexure show some strange de-parture from the normal. The Finochietto end-to-end union is.quick, limited to the supracoliccompartment, associated with little if any shock,and has a low death-rate (3 per cent.) even indebilitated subjects. It has one drawback-a flawcommnon to all the Billroth I methods-regurgita-tion of bile into the mouth. Nausea after meals,the occasional stricture at the anastomotic junction,a sense of oppression in the epigastric region aftermeals, the taste of gall or acid in the mouth-moreespecially when the patient is recumbent-aresome of the unpleasant features which restrict theuse of this otherwise attractive operation.
(4) The Technique of the OperationA scheme of pre- and post-operative nursing for
subtotal gastrectomy cases is outlined at the endof this chapter.(a) Ante-colic or Anterior Polya-HofmeisterSubtotal Gastrectomy
Incision. There is a choice of five incisions:mid-line, left paramedian, left vertical transrectalmuscle-splitting, left oblique and transverse. Allthese incisions have their good and bad points.
In cases of gastric ulcer the choice lies betweena lengthy left subcostal incision and a vertical lefttransrectal muscle-splitting incision. The for-mer commences near the tip of the right costalcartilage and extends across the epigastrium justbelow the xiphisternum before sweeping down-wards one inch below the left costal margin to theouter border of the rectus muscle. A portion ofthe right rectus muscle is divided and the wholeof the left rectus, together with the anterior andposterior sheaths of the muscle and peritoneum, iscut across obliquely close to tne left costal margin.
This incision gives an excellent exposure of thebody of the stomach, the fundus and cardia, andgreatly simplifies the operation of radical excisionof the stomach.The wound is closed in layers, using long strands
of No. 0 medium chromic catgut for the con-tinuous sutures. A few mattress sutures areplaced in the posterior sheath to draw together thecut margins before the continuous suture is in-serted. The edges of the wound are approximatedwith vertical mattress sutures of fine biack silk.The vertical muscle-splitting incision gives a goodexposure and is easy to close securely. I havebeen employing this incision more and moreduring the last few years.
Exploration of the Abdomen. In all cases athorough exploration of all the. abdominal viscerais conducted. The upper abdominal organs areinspected by sight and touch, but the lower areexamined only with the palpating hand. Thewhole stomach-anterior and posterior wall,duodenum, pancreas, spleen, liver, gall-bladderand biliary passages, mesocolon, duodeno-jejunalflexure, proximal loop of jejunum and the meso-jejunum, must be carefully scrutinized before de-ciding upon the scope of the operation.
If the ligament of Treitz appears to beanomalous, if the first loop ofjejunum is caught upin scar tissue,' or if the infracolic compartment isenmeshed in adhesions, it is far wiser to performa Billroth I operation than to persevere with aPolya type of resection and anastomosis in the faceof these obstacles.A small gastric ulcer or an ulcer which appears
almost to have healed does not imply the need fora small operation, e.g., simple excision. The sizeof the ulcer must not influence the choice of operation,for once we are committed to operation for achronic gastric ulcer which has defied medicaltreatment the only procedure that can be coun-tenanced is gastric resection. The presence of in-fracolic adhesions or the combination of a gastriculcer with a penetrating duodenal ulcer may in-fluence the choice of anastomosis, but does notalter the fundamental principle that the best andsafest method of dealing with an ulcer of the stomach
by copyright. on January 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.24.269.143 on 1 March 1948. D
ownloaded from

I48 POST GRADUATE MEDICAL JOURNAL March 1948
consists in removing it together with at least five-sixths of the viscus.
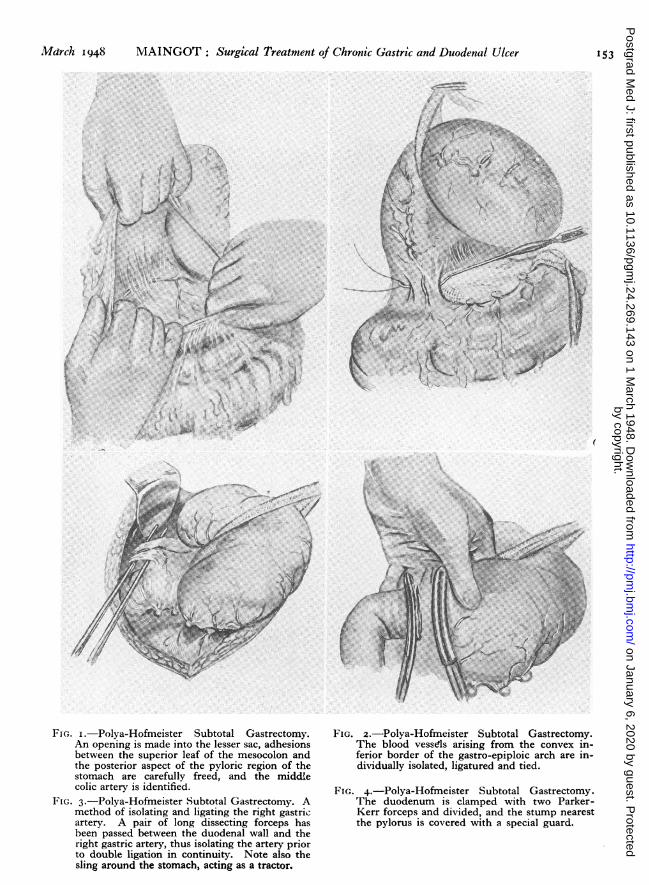
Mobilization of the Stomach and Duodenum.The great omentum and transverse colon aredrawn through the wound and covered withlarge warm moist pads. Then, after the gastro-colic ligament has been put on the stretch and anavascular area chosen well to the left of the greatercurvature, a wide opening into the lesser sac isobtained by tearing the omentum apart with thefingers (Fig. i).
After dissecting free with scissors any adhesionswhich are found in the lesser sac between theupper leaf of mesocolon and the posterior aspectof the stomach, or possibly between the ulcer andthe mesocolon, and after freeing the middle colicand possibly the arching branch of the right colicartery from its fibrinous attachments to the pyloriczone, a large warm swab is packed into the stomachbed to keep these vulnerable vessels out of harm'sway. A good view of the ulcer, or rather of itsposterior anchorage and its relations to the middlecolic artery, can thus be obtained.
In some cases, as in the operation for cancer ofthe stomach, the major part of the omentum isdetached from the colon and left hanging attachedto the greater curvature ; .but in most gastric re-sections for simple ulcer the blood vessels whichspring from the inferior border of the curvingright gastro-epiploic artery are isolated, clipped,divided, and tied off with No. 4 silk, one by one,until the lower border of the pylorus is reached(Fig. 2).The right gastro-epiploic vessels are ligatured
and divided where they come into view beneaththe antrum, the right gastric artery is under-run and tied off securely, the first part of theduodenum freely mobilized and clamped with twoParker-Kerr forceps just distal to the sphinctericring, and the gut divided with a carbolized knifebetween the two clamps (Figs. 3 and 4).The blades of the Parker-Kerr forceps which
embrace the short segment of duodenum close tothe pylorus are immediately covered by a specialmetal sheath which is well illustrated in Fig. 4.The stomach is drawn over the left side of the
chest out of the operative field for the time being,and is surrounded with warm, moist abdominalpacks. The duodenal stump is now closed in aConnell suture or sewing-machine stitch of No. 2silk reinforced with a series of interrupted mattresssutures of fine silk, or in the simple manner de-picted in Fig. 5. I often place the suturedduodenum retroperitoneally by attaching the cap-sule of the pancreas to the anterior wall of theduodenum or, as an added precaution, cover theclosed stump with a pad of fatty omentum.The stomach is picked up again and held well
over to the patieftt's right side, while an assistantfirmly retracts the left margin of the abdominalwound. This manoeuvre brings the spleen andthe left portion of the great omentum containingthe branching gastro-ppiploic vessels into view.Care must be taken at this stage to avoid tearing thecapsule of the friable spleen by vigorous retractionwith the Deaver's retractor or by pulling tooforcibly on the great omentum or on the gastro-splenic omentum itself.
All the remaining blood vessels along the greatercurvature of the stomach up to the main vascularpedicle of the spleen are isolated, clipped withhaemostats, divided and ligatured seriatim. Inperforming subtotal gastrectomy it is necessary todetach the lower half or more of the filmy gastro-splenic omentum.When the ulcer deeply pits the pancreas or liver,
after isolating the operative field w~ith Lahey'sCellophane squares, the stomach is cut adriftcautiously from its moorings with a cautery, thepearly-white sclerotic base is coagulated with adiathermy disk or button, and the hole in thestomach wall is closed with a purse-string suture ofstrong silk. The now leathery ' cooked' base ofthe crater is cleansed or mopped with penicillincream.The left gastric artery must now be displayed
close to its origin, tied off in continuity about I-2in. below the oesophagus, and divided betweenligatures of No. 4 silk. Fig. 6 shows how this maybe done by insinuating a pair of dissecting forcepsbetween the lesser curvature and the large vesselscoursing upwards in the gastrohepatic omentum.As soon as the right gastric vessels have been
ligated the raw surface which remains on thelesser curve is reperitonealized (Fig. 6).
Resection of Stomach and Gastro-JejunalAnastomosis. At this point in the operation Allisforceps are applied to the lesser and greatercurvatures to act as markers before the large,strong, thin-bladed Payr clamp is crushed homeobliquely across the stomach. The first marker isclipped to the reperitonea'Lized lesser curvatureabout 2 in. below the oesophagus, the second pairof Allis forceps is applied high up on the greatercurvature, and the Payr clamp is locked in positionprecisely above these markers.Upward traction is now made on the Payr clamp
in order to draw the posterior aspect of the stomachinto the wound whilst the redundant portion of theorgan beyond the blades of the enterotome issurrounded with abdominal pads and laid on theleft side of the patient's chest.The stomach is now prepared for anastomosis
to the proximaljejunum, and the Hofmeister valveis fashioned. A portion of the stomach at leastthree finger-breadths in length towards the
by copyright. on January 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.24.269.143 on 1 March 1948. D
ownloaded from

March 1948 MAINGOT: Surgical Treatment of Chronic Gastric and Duodenal Ulcer 149
greater curvature is reserved for the stoma, andthe part towards the lesser curvature is under-sewn, divided and inturned. A straight, short,round-bodied needle, threaded with a strand ofNo. 3 silk, is passed beneath the Payr clamp,through both walls of the stomach about J in.from the free margin of the lesser curvature. Thesuture is then tied, and that part of the gastricwall embraced by the suture is cut free, the bladeof the knife being kept close to the under-surfaceof the clamp (Fig. 7).
This procedure is repeated again and againuntil a sufficient amount of stomach towards thelesser curvature has been cut adrift ahd anadequate amount (22-3 in.) remains suspendedfrom the clamp for the gastro-jejunal stoma whichwill shortly be constructed (Fig. 8). Alternatively,the upper portion of the stomach embraced in thePayr clamp may be securely closed by a Shoulders'machine stitch, after which the small portion ofstomach between this stitch and the Payr clamp iscut through with a knife. The new lesser curva-ture from the ligature on the left gastric artery tothe Payr clamp is next completely invaginated by aseries of closely-placed mattress or cross suturesof No. i silk mounted on small half-circle needles.A circular incision is made precisely below the
Payr enterotome through the posterior and an-terior seromuscular layers of the small gastric tubedown to the submucosa in order to expose, isolateand individually under-run and ligate all the bloodvessels which are seen coursing upwards towardsthe clamp (Fig. 9). The blood vessels in -theanterior wall are more numerous and larger thanthose on the posterior wall of the stomach.The great omentum and transverse colon are
held upwards and the duodeno-jejunal flexure isidentified by sight, and a long loop of proximaljejunum is drawn into the wound. After packingthe great omentum and the transverse colon intothe empty stomach bed and beneath the over-hanging right lobe of the liver, the proximaljejunum close to the duodeno-jejunal flexure isdrawn across the transverse colon and applied tothe ligated stump of the left gastric artery and aportion ofjejunum some 6-8 in. beyond this pointis selected for anastomosis to the gastric pouch.The length of taut jejunum from the duodeno-jejunal flexure to the ligated stump of the leftgastric artery is variable (=x), as it will dependupon the amount of stomach resected, but itusually measures about 2 in. If we allow afurther 6-8 in. for slack at the duodeno-jejunalflexure and in the portion of bowel proximal tothe reconstructed lesser curvature, and also forupward retraction of the gastric pouch when theanastomosis is completed, the loop stretching fromthe flexure to a point some 2 in. below the right
border of the cardiac orifice will take a gracefulS-shaped curve for 8-io in. (=x plus 6-8 in.).The stoma itself will be a further 2-3 in. be-
yond in the descending limb of jejunum (seeFig. I3). The loop is therefore a long one, isantecolic, is made to swing from right to left inthe reverse direction to that recommended byMoynihan, Lahey and Pannett, and the opening isplaced towards the greater curvature. The afferentjejunum is buttressed against the new lessercurvature, thus reinforcing the valve, after whichthe intestine, i in. from its mesenteric attachment,is fixed with fine silk stitches to the posterioraspect of the stomach, X in. away from the sero-muscular groove.A Cushing right-angled continuous posterior
seromuscular suture of No. oo medium chromiccatgut mounted on an eyeless needle is next intro-duced, uniting the contiguous margins of thestomach and jejunum from the greater to thelesser curvature (Fig. 9).The stomach contents are aspirated through the
indwelling Ryle tube which was passed beforeoperation and which will be allowed to remain insitu for a day or two after operation. The sero-muscular coats of jejunum are then incisedlongitudinally and ; in. away from the Cushingsuture (Fig. 9), and any sizeable blood vesselswhich are seen lying on the submucosa are under-run and ligated with the finest silk. The exposedmucous merabrane of the jejunum is picked upand incised, and the intestinal contents are as-pirated with a sucker, after which the stomach islikewise opened posteriorly for the full length ofthe incision and any remaining gastric chyme re-moved by suction.
Starting at the greater curvature, the secondposterior continuous suture is passed as a lock-stitch which evenly approximates the opposingcut margins of the stomach and small bowel(Fig. io). When' this stitch reaches the lessercurvature it is continued anteriorly as a Bell-Schmieden or in-out iii-out suture (Fig. ii). AConnell or loop-on-the-mucosa stitch is also verysatisfactory and produces a neat inversion. Trac-tion on the Payr clamp is maintained while theanterior wall of the stomach is divided and almostuntil the last suture is inserted, thereby facilitatingthe introduction of the anterior continuous suturewhich is finally tied to'the end that has been keptlong (Figs. ii and I2).The operation is completed by picking up the
first posterior suture and introducing this an-teriorly as a continuous Lembert suture whichinvaginates the suture line. When this suturereaches the point where it started at the greatercurvature it is tied to the end which has beenleft long and clipped by a small haemostat. A
by copyright. on January 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.24.269.143 on 1 March 1948. D
ownloaded from

150 POST GRADUATE MEDICAL JOURNAL March 1948
few interrupted sutures of fine silk are introducedat the greater curvature and at any weak or untidypoints in the length of the anastomosis.
In order to prevent sagging I reinforce theregion of the greater curvature with omentum andalso anchor the transverse colon and the afferentcurving jejunal loop to the capsule of the pancreaswith a few well-placed sutures. Fig. 13 shows theposition of the stoma.
Comments on the OperationMuch of the success of the operation depends
upon choosing a suitable length of proximaljejunum and upon applying this to the stomach bythe method I have suggested. The valve and thestoma (which should admit about three fingers)should be constructed so that all nourishment in-troduced into the funnel-shaped stomach isdeflected into the distal limb of jejunum and sothat no food can find its way into the duodenum,which is rebellious to even a minor degree ofdistension (Fig. I3).The anastomosis may be performed by the
closed or aseptic method with the Furniss clamp(Culligan, i944), or on the lines advocated byWangensteen (I940), Pannett (I945) or Babcock(I942).
It is claimed that the closed (aseptic) method ofgastro-jejunal union reduces the incidence of post-operative peritonitis and infection of the wound,shock and the length of time expended on theoperation. As, however, the procedure is nottruly aseptic and the measures taken to preventpost-operative haemorrhage are not uniformlysatisfactory, and as the sutures cannot be intro-duced with the same precision and security as inthe open operation, I seldom resort to the closedtechnique in gastric operations.The large Petz clamp may be employed to
simplify the fashioning of the gastro-jejunalanastomosis. The Petz instrument is crushedhome along the same oblique line of the stomachin its upper fifth or sixth as the Payr clamp. Thestomach is then steadied with Allis forceps and acautery cuts through the crushed groove betweenthe two rows of clips. The upper one-third or soof the crushed rim of the stomach with its con-tained metallic clips is inverted with a series ofHalsted sutures and the portion of the stomachtowards the greater curvature is used for theanastomosis. The crushed area with its clips,which mark the extent of the new stoma, must now,of course, be cut away with scissors, after whichthe gastro-jejunal anastomosis is carried out inthe usual manner.The immediate and late results of the anterior
Polya-Hofmeister subtotal gastrectomy are mostgratifying; the average post-operative stay in
hospital is ten days; the patients on discharge areallowed full diet without restrictions; they re-quire no medical treatment; approximately 98
* per cent. are restored to full economic efficiency;the subsequent onset of jejunal ulceration is lessthan 0.5 per cent., and the majority show a definitegain in weight and strength.The operative death-rate is low. At the Mayo
Clinic in I943 partial gastrectomy was performedon 145 cases with only two deaths (I.4 per cent.)(Counseller, I944), whilst in 1945 of the I43patients subjected to gastric resection there werebut three deaths (2.I per cent.). In a personalseries (I938-I942) of 77 cases of subtotal g-is-trectomy for gastric ulcer there were threefatalities (3.6 per cent.). In a later series (I943-I945), 6i cases of chronic gastric ulcer were sub-jected to subtotal gastrectomy without fatality.
(b) The Posterior Polya-Hofmeister OperationThe mobilization of the stomach and the closure
of the duodenal stump are the same as in theanterior operation. In the posterior operation ashorter loop of jejunum is chosen for anastomosisto the stomach (about 5-6 in.), the opening is madein the mesocolon to the left of the middle colicartery, and the margins are sutured all around thegastric pouch, thus placing the stomach in theinfracolic compartment of the abdomen. Thevalve and anastomosis are constructed as described,but at the completion of the operation the greatercurvature is deliberately rotated so that it comes tolie anteriorly and the lesser curvature posteriorly,thereby permitting the proximal jejunum to pur-sue its natural course without any danger of itsbeing kinked or obstructed.
(c) Finochietto's OperationFinochietto's method of performing the Bill-
roth I operation is described in some detail andfreely illustrated in ' Post-Graduate Surgery'(I936) to which the reader is referred. Theessential steps of the operation will, however, bereadily appreciated by studying Fig. 14.
Conclusionsi. The main indications for operation in cases
of gastric ulcer are:(a) Acute perforation;(b) The failure of efficient medical treat-
ment; and(c) The impossibility of excluding malignancy
in certain cases.2. lThe operation of choice for chronic gastric
ulcer is the anterior Polya-Hofmeister subtotalgastrectomy, the details of which are given.
3. T'he operative mortality of subtotal gas-trectonmy in this disease is 2-4 per cent.
by copyright. on January 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.24.269.143 on 1 March 1948. D
ownloaded from
March I948 MAINGOT: Surgical Treatment of Chronic Gastric and Duodenal Ulcer 151
4. I'he risks of death from malignant degenera-tion in a patient with chronic gastric ulcer aregreater than those which attend surgical inter-ference.
(B) Chronic Duodenal UlcerThe following groups of patients who have
chronic duodenal ulcer should receive medicaltreatment:
i. All those who have uncomplicated ulcers,especially if they have been present for only ashort time.
2. All patients 30 years of age or under, urtlesstheir lesions are complicated.
3. All older patients whose symptoms are mildand do not impair their efficiency.
4. Any patient whose ulcer is complicated bysome medical condition which would renderoperation hazardous.
5. Psychoneurotic patients who have hyper-irritable gastro-intestinal tracts, and whose ulcersare not complicated by deep penetration to thepancreas, repeated haemorrhage or obstruction. Iagree with Morlock (I944) who writes:
' One of the essentials leading to success in themedical treatment of any duodenal ulcer is theproper evaluation of the factors which promote thechronicity of the lesion. One of the most im-portant means of determining these is a carefullydetailed history which brings to light not only achronological record of the development of symp-toms but reveals the patient's general familybackground and personal make-up.'Again:' If the symptoms of duodenal ulcer are recog-
nized and treated adequately, satisfactory controlcan be expected in the majority of cases. Un-fortunately, it is still true that go per cent. of allduodenal ulcers which lend themselves to controlby medical measures are inadequately treated.This inadequacy of treatment results in recurrentulceration and complications which can berectified only by surgical measures.'
(1) Indications for Operation(a) Acute Perforation.(b) Intermittent or continuous haemorrhage aris-
ing from the base of a chronic duodenal ulcerwhich medical therapy is incapable of controlling.
(c) Pyloric obstruction due to a long-standingcicatrizing duodenal ulcer.
(d) Failure of efficient medical treatment.(e) Recurrence of ulceration associated with severe
symptoms following: (i)- Simple suture of anacute perforation; (ii) an inadequate operationsuch as pyloroplasty; (iii) transduodenal trans-fixion and obliteration by sutures of an ulcercrater to control severe bleeding.
(f) Chronic penetrating duodenal ulcer accom-panied by a gastric ulcer.
(g) Large penetrating duodenal ulcer whichshows no encouraging response to medicaltherapy (see also (d)).
(h) Expedient circumstances and economicreasons in certain cases.
(2) Some Factors Influencing the Choiceof Treatment(a) Age. The younger the patient and the
shorter the history, the more likely are medicalmeasures to be successful. Medical treatment forelderly patients is usually much less effective thanfor those who are younger, this being no doubt inpart due to the impaired circulation and dim-inished recuperative powers in the former.Gastro-jejunostomy should not be performed inyoung patients, i.e., those below the age of 30, asthe incidence of jejunal ulceration following thisoperation in such patients is more than 35 percent. The operation of choice in young patientswith complicated lesions is gastro-duodenal re-section combined with vagotomy.
(b) Sex. Sex does not necessarily influence thechoice of treatment, although it should be notedthat the mortality following gastric operations inwomen is lower than it is in men, and the lateresults are uniformly better in women. This, atleast, has been my experience. Again, stomalulceration is much more rare in women than inmen after any type of short-circuiting procedure orgastric resection. Operation for gastric andduodenal ulcer is, of course, muGh rarer in womenthan in men.
(c) Length of Ulcer History. The shorter theduration of the disease, the better are the prospectsof permanent healing by medical measures. Thispoint at least is undisputed. Patients thereforegiving a short history of duodenal ulcer are notgood candidates for surgery, and I have no faithin a surgeon who would advise surgical inter-ference in such cases. Patients giving a longhistory, for example iO-I5 years, during whichtime they have undergone many courses of medicaltreatment for persistent recurrence of symptoms,are best operated upon if no specific contra-indications are found to exist.
(d) Pyloric Stenosis. The commonest cause ofpyloric stenosis is a cicatrizing duodenal ulcer.We have to distinguish between organic pyloricstenosis and spastic obstruction due to inflamma-tion and oedema around the ulcer. The lattercondition is amenable to good medical therapy, theformer is not. I used to be taught that pyloricstenosis due to duodenal ulcer was a clear-cut in-dication for gastro-jejunostomy. Long-standingscar stenosis in an elderly patient with low acid values
by copyright. on January 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.24.269.143 on 1 March 1948. D
ownloaded from

152 POST GRADUATE MEDICAL JOURNAL March 1948
in the gastric juice is an indication for a short-circuiting operation, but stricture of the duodenumdue to chronic uker associated with hyperaciditycalls for gastric resection.
(e) The Acid Problem. Most of the problems inulcer management hinge upon the quantity andquality of the hydrochloric acid in the stomach,and it is agreed that operations performed forchronic duodenal ulcer show a far higher per-centage of good results in patients with low aciditythan in those in whom the acidity is high.
In certain instances, frequent fractional test-meal examinations are of value in helping thesurgeon to arrive at a decision as to whether heshould perform a short-circuiting operation or awide resection. But age, the general condition ofthe patient, and other factors will also have to betaken into account. For example, a young man,say of 30, with spastic pyloric stenosis due toduodenal ulcer in which test-meal examinationsshow anacidity or hypochlorhydria may be suffer-ing from a concomitant gastro-duodenitis whichappropriate medical measures will quickly cir-cumvent, and re-examination some days later re-veal a sharply climbing acid curve. The hyper-acidity has in this case been masked by a thickcoat of mucus.
Take, for example, the case of an old man of75 with scar stenosis who is vomiting largequantities of fluid daily, losing weight and slowlystarving to death. Here, gastro-jejunostomy per-formed under local anaesthesia is unquestionablythe operation of choice.
Therefore, the acid factor dominates treatment.Gastro-jejunostomy should not be performed uponpatients with hyperacidity or upon those under theage of 6o, but should rather be reserved for thoseover this age with proved hypoacidity or anacidity,for the aged and infirm, and for those who onaccount of some debilitating disease are unable towithstand the major procedure of gastro-duodenalresection.
(3) The Choice of OperationIn cases of chronic duodenal ulcer there is a
choice of: (i) Gastro-jejunostomy (anterior orposterior) ; (ii) gastrectomy by the Polya-Hof-meister method (anterior or posterior) ; (iii)Bancroft's procedure followed by subtotal gas-trectomy; or (iv) vagotomy alone, vagotomycombined with gastro-jejunostomy, or vagotomycombined with gastric excision.
(a) Acute Perforation of a Duodenal Ulcer. Assoon as the diagnosis of acute perforated duodenalulcer is made, a Ryle tube is passed through thenostril into the stomach and all the gastric con-tents are aspirated. This prevents any furthercontamination of the peritoneal cavity. The tube
is left in situ during the operation and for the firsttwo to three post-operative days.The best operation for acute perforation of a
duodenal ulcer is simple suture, and for preferencethe three-suture method which I have previouslydescribed.
In those cases where following simple suture itis thought that there is some narrowing of the firstpart of the duodenum, the indwelling' stomachtube can be coaxed through the strictured zoneinto the capacious bowel beyond and be used bothfor aspiration and for feeding purposes. AnotherRyle tube is introduced into the stomach to ensurethat this organ remains completely deflated duringthe first two or three critical days.
In my opinion, gastro-jejunostomy or gastro-duodenal resection should not be carried outfollowing the performance of simple suture. Whenthe patient is convalescent or some months laterduring the tranquil period of medical treatment,the case can be reviewed and, if surgery is clearlyindicated, the appropriate operation can be per-formed under the most favourable conditions.The majority of perforations diagnosed at
operation as perforated pyloric ulcers are, in fact,perforated duodenal ulcers. Perforation of apyloric ulcer is an extremely rare event. If all thepresumed perforated pyloric ulcers were sub-jected to barium meal X-ray examination duringthe period of convalescence, I am convinced thatthe radiologist would report' deformity of the cap'in over go per cent. of them.The late results of simple suture of a perforated
duodenal ulcer are poor, as over 70 per cent. of thecases have crippling symptoms and fully 50 percent. of these have eventually to undergo gastricresection or gastro-jejunostomy.
I do not advise conservative (or non-operative)treatment for acute perforated duodenal ulcer, asrecently revived by Hermon Taylor, Reid, Visickand others.
(b) Bleeding Duodenal Ulcer. The operativetreatment of bleeding duodenal ulcer may entaileither partial gastro-duodenal resection or elseexposure of the ulcer through an incision in theanterior wall of the duodenum, followed bytransfixion with strong silk sutures.
There is no operation which will afford greaterprotection against recurrence of haemorrhage thanresection. When, therefore, the patient can beoperated upon within 48 hours of the onset ofbleeding, when he appears to be in a satisfactorycondition, when the duodenum can be mobilizedand the ulcer is not too large in size or too firmlyfixed to the underlying head of the pancreas,partial gastro-duodenal resection should be per-formed, the blood-drip being regulated to a steadypace.
by copyright. on January 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.24.269.143 on 1 March 1948. D
ownloaded from
Mdrch 5948 MAINGOT: Surgical Treatment of Chronic Gastric and Duodenal Ulcer 153
.........
......
FIG. i.-Polya-Hofmeister Subtotal Gastrectomy.An opening is made into the lesser sac, adhesionsbetween the superior leaf of the mesocolon andthe posterior aspect of the pyloric region of thestomach are carefully freed, and the middlecolic artery is identified.
FIG. 3.-Polya-Hofmeister Subtotal Gastrectomy. Amethod of isolating and ligating the right gastric-artery. A pair of long dissecting forceps hasbeen passed between the duodenal wall and theright gastric artery, thus isolating the artery priorto double ligation in continuity. Note also thesling around the stomach, acting as a tractor.
FIG. 2.--Polya-Hofmeister Subtotal Gastrectomy.The blood vessels arising from the convex in-ferior border of the gastro-epiploic arch are in-dividually isolated, ligatured and tied.
FIG. 4.-Polya-Hofmeister Subtotal Gastrectomy.The duodenum is clamped with two Parker-Kerr forceps and divided, and the stump nearestthe pylorus is covered with a special guard.
by copyright. on January 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.24.269.143 on 1 March 1948. D
ownloaded from

i54 POST GCRADUATE MEDICAL JOURNAL March 1948
::.-----........:.. -'..-.,:I:::,...,.:e......,.,.,.,:::..,.,.:.-...::;.,::f !.. .......::: ::... :. .",!......:..1. "' ,..,.P.........: ,:.. -..:.-,..:-. -..-'. '.. :':....:..:...?dm ,........ ....::..;., -.,.:. .::.:.:.:::......:--,.-,.-,::- ':. .: .::.:..-... .,. ..., .:.!::! ...... -. ..." %.,, e..,-..-.,.,.., ..." ..", "--.'.';.i.::I........ .........'...."...,....-....,....-....-,...,...,..,..."..,...,..,.,.,...,.",,.-...,...,,.....,-.....-'.-.....-,",.:-,-. .:.,::,.,.:.:::.-.-...-':..i...',.::.,i.::.:: "'-....l"...i."..!i...'-"...'.."...''., 'I.,, ,,------..------""-----, .'.."...-'---.'-..."...,.-..,.".... .....,......:.:.:.: 1: :!. :-.:: OP--,-...:i..ii8 --".'-.'---.----. -e,.-N-.'--.;-"--,----., ..,-......,.....:..:. ::..:.:...:: -..:.. ., ........ .1. h...A. !..::..:... .', .....:.:.....:.... %...,"" "I"''I"""I'll""'........:,j:".:.:::. :,.:".,.,-.-,:--:--:...:":".'.-.i........ :..::-..."...'..'."..,..,:.........,...,,.."...."..."....".'.'...'.......'....'.,......;.:!.:...."......'.....'.'.."'.....'...".......,'........."......'...'.......,:,-
.- .: .,. .' N" ..... I....,"'"" "'' .:: """"'," "',,""-"",,,, '".:.. ..,-" ""'""""'"" ""..."'..... -.. .....". .,..- .-.. -... ...... ... ----... -,. ..-i.-.....".....-...'....-.......... ,.A':,:...: %:.,.,:..-....-..-.- ----.------ -..--..-. ..:..-.." -:.. :... ..'. .....!:::'.....-......:....... .....:"i......"::..':..--...-.... -..... ......-..,-...-....-.,.... -:::. ...': ::..: :,...........::'-':'.'.:':' ,:..,...., -::::."-,:i:Z--:.-.i'-... .... ,'.1.1.1.11" ," ..... ----':.,.., ".,-.. .:::.:.:-.:.--.-.- ::... ::. ..".: :::.-.... ........... ...'.... -:.::...-.':::.:..:
-..... ...:: ,:.... .. ,"'F...-.....::,..:. .,..'. '..:.....,:.,:.:,.::......... ;;.. .. ,,, ,- -:-::.:::'?.--.:.::::.:.:i... .,,. .,... ,:. ........: .... ::;.:....
..... :., .:.. ....1 ............:: -..... .!:. :::.-,,..i.. ..4; :,::.. .! ..:: .: ..:!-....%......... ... .....:.-..: :.::::..-.--.:::-..:.I. ..:.:::.......:.-::: ...: -...-'....,...,..,..,.,..,.."...,.."..:.. .:.,- ....
...:::.:.::.::-:,. .::::'- :,,......... :-,--,::-:;.;. .......'..."..'. ::. --,.:.,..::..!:.:i::..
:..:..,::,...:: ....-.. ..: .:.... ..*.-.,:::.:.:!:..:.--.-.-- ..........:: ..:--..:.. ......%..:....... -,.....:...:.::....., .......-.......:.,:: ..: ....-!-,.:.i.,..,:.:: .:......,.....::: ..::..::..:.........:"., ....:... ..... ..:...........,::,:,.-.-,......,..-.: ... :, ,.. ...:
.:. ..;,.... ....-:,.' .!-"--..i :!-", "',. .:: ...-. ...Pl.... ..:...:-,.. ... ...-... .'. .....'.... .-':.-.."'.:
I........-K.::: :.. ... .. ...-.-'. ......,,-,".1.:,,.......:.4:.... ....I-..,..: .'. ...:..-..:::::::-.. :..: "- -. ::..: ::::-':.'-- ::' .;.:!. .......... !::.... .-.:-:. ...... ....--- :.'.-.: .-...'-::: -..:.J:.. ..; ....--::::........ ....:.::...,,........-...;-':.:. !,... ... .......-...--....... ....... ..:::::..:...::::"'r.:... :U ." .... "... ,,;., .... m-:.f.....:..... ..:.:........-I.. ....... ........i.-.....,.:.:.,........................I.,... :.": .:..:..:::.,.:.......... .. ..::..:,.,,--I ,-I...'.......... .......,..................::-
...,,.......- ..:r -.: .'..:. ...'.l.:;:..:: .............:-. '.. -!-........ ....;!..... :.... ......" ,, ,.'.","',,........--... :- .--:;., -,---,!.::.-.- .....'.::....f..:..:-.....-,..,.,.,.....,.,..,.,.:..-.-"...- .,...:...,....:..,...-. :-.
I....:.. ......: ,,%:...-.,... ..:.-:...:.: .:-....... :: ........... %... --.., i: -.'.--. ... .......'..... .... '...., ...-.--- .. ...., .. .. ...--:.o -....". --.. ...... ..... ..:. -:-...-.:..'.-,-'."... .---'ii ...-.-.,. :, ...'. ,---,.-.. ..,....,., ......... ...,;: ::! :..
..,... :.::%.:......::-.."-.: :-:::.-'...:.,'. ::!:.::..-,:i...:,-,...-..i..... I-,'," ,:-,-l,-.-,T: :.,..,."........-...........,.,:,- ...... -.........I...":.,..::........
.....%.... ..........
:': ...I"':...,,,.'---.::.-,. -:....: ...:..:..:,,:.::.,.. .. ......:..... ...-... ...::::-.- .":....:.:....,:..:.. "':. ,-.:..'- ..:.:.:... ..:..'..: .:..:. ...": ......::..:..:.:-:::;.:".:.:..!.......-.,....... ...:..: :::....... .:: '..:: .: ........--,.:;
.:-:-,:...-::.: :.. t...:.. ...:. ....: -.. :,::...
...:....:.......,.....:.%-......-h.
...:;..' --.---..",:",. ::. .i........ .: ::': :::.i.-. ..:..-'.----: .:-----...,..'. .:---.:,,....:,......,. ..: -:..: ::;..:i:: .,::.!.'.',...:::..-::, !!% :-:,...,!: :!:,,.,............ ,::..,- .;. .: ;. .:.-.'.: ... ..,.:. .,- .:.", .....:.., -,-.". :.::.:; -'.-'.:; :::.::...,... -.: ,:-,.,.,:--,.,!.-;- --.-.:.-..,.. ....:... .......-!.",::!:;..--,---.,.... ': ,: :.: :.'..::. .::: ."... -.4.-.'-.:.: .%-..-.- ..Z.......:.:
.:..:. ::i..-,.O-". i:::..,.::!....., ....: ':. .: .:;%.:.'.:-.L,:...-. --, --.,.. ........:.......!;..... ...-:. --.c- ...
...- .:..-...-,"...,.-.....,..,:...,.,:.e..- -::.-'-'. ,., .:.., .:...,.*..,........:-:... ..". +;. .,. .-,, ,,, 7,..,--.!.-..-. ---:.-.. :-. -.-": '.."..;. :. -.-, -.'-.": .?.....
.::%.:.::..'....%-:.:.:;.!::.........,:;... .. .. .., .... .. .- .: .: .-,:. .-..' .'.' ...., :.-.'.-. :..!. %";;.:..: .:.: ,:,;. ;:...-,.-..-..::..-....:."..:-.- ,,.,.6!. ..., ,,.- -,,.:::.,,,.... .... -,-......: ..::...:"." .:-....... ... -.1, ..,-.: -'... ..., ..'...., ....- ...-.....,..'.., .:: .!..,? .-,...:,..-. :.--' ..:;::: ..,:::..: .,. ---..:--.,., .,....-...e. :.:,, ,,,--'....,...;... .....::.:.".: ..!":,.
.... :::.! -", -'. --;- i-N."...." --;l..-,.,--'l----'!.i,% -,--5--,---,."--, .".,..,;..... --::i.--,-4--,:;:i; ..: ... "i, "'.! ,:.:!::R --...r -...-, '' ...". 'i'.-'.:::.:!..---.'.':..;..!...............-.....'..-.,.,.,.-.."...'....,'....'...,...-.'. .....r..:l.... -:... -:::..-..:-::.::.. l.,:--l'-l---,.:-:--.,-.;. ..I.!:.:'...:.;:.:.,......-:,.,:,.,::,.-, .:..:.:. .... -.:.. :::.:.::..".,ii','..5.........-.",...,-..',.,...'...,..",...,.,,.;:,i:: '....: "- :!:.. .ii-;i-.!.--.:::: --..-..- ....:...-..: ::..-,.,-,.,.,-....'$..,-,..:iL,:,::;.:..4..-............-i-1,"'..,.%:;:..
.... ..4:. ".. -............, "' .""-I-,.......... .- -.::.,..'. -..-,............ .- :. '.. .:: .....-.-..:'.:. ::. --'..:-'.:-... --:.. .:.. .e..'.. '. ..-., !." ....,"....:.:, ...... ....-,..::.:.......::.:.....;...-m :: .........:...-;-' --,-.: ":.'- '....::3.: .-".1 -::,..l::-,--..,-.---- ..-".......,-, :........ .... ..'..-':.-.'......- .;.,4 .L.... .....'. ..-..I:.i.....'. .... ::f:::..'.! :-':... .:.::::.,.-." --.-' .:. ..'. -.."-... ..': ..:;...:..::..: ..q..":..':.........:i ..... .... ;:....-..,. -.-....:. -". ".".' ,..:.. ...-...-.!-.--' .,...:;..,:: '.. -:..".--.-.....::-:.:.!...:..i.:.,.-....----.----.--.;---,.-..,""::,:,: ..--- -:..... ..:.1. ,,.": S:..:.:.-,:.--:::'..:::.,.,:...'...".....-",..,....,..!!-- -....:..... ,..".'..-. --'---,..--., .....'.-.':,. -:-.-...:....,.:.,.,.....,.,.i..,.', ::..---.-.,::,., .. .. .:..:.%.:.".-- -.:. :..::.: .::::!..: .:.. ....: !:........ ..: ..i:? k....... :...,,. ..r....M: ..'.. ....-%s!F:... ........--....:.., ..'.. .....,..-.--::: :-..;..":..,,..,..... ...:..i..:.Z.:.:;.I. ": .:'.":.-'...A........:!
...-.......: ...:.%:.% ..". 'I.: '. .....,...:..:.%..-...:.:,.-. .:. .;.
.::... ..:. ...:.:.....:: ..:.:....:..!-",..:... ..:. ....:!-... ....- -----....::.. ..;:... ... .:,... :;-. :1..:.-.--::.:-,.,:.--,:.,. -.. "..:...... ....::.: ..;..-.--';-----:.....:. !.- :. ,:;.: .-..: ..: :: %.....!. .. !...:..-..:..:...........:......-':. ... .::..: ......: :.;:
.. :, .:.....,:, ,:" ,"', ,,..,'. '!.'. -.: ......-,.....,.-,.;: -... .:.
-:.". :..--.....-!:.....----'...:.....k.............:.....:.......:::........,.,,..,. .".....- .:: .: .-S. ...'.'.. --..- ..' -...-... -... .-.... :.:-l. ,.'-.-:'.::.
..... :..F... ...-..- ....... .... ...
..:.... :., .....:. -.:'-'-. .. .::, .-'.': .: .......!-::..:. ..::; ::: :...:: ::,::..... .::.: ".. ..%...... .1..::., ..:: ,:,:..:.:......,.:..:: ...,... :,::;:::-::::i....,, :;!..:..: .. :: :: ,; -..:.:::.:!:..:.. ....:...:..:::..:: "',...:. .:.:... ...:.::....,".:" ..:,.. '. :.., ?..,"'..
..... :: ....:: .. ",.: ':. :.::.":..,. ::.- "" .. .:. ...: :......... :- -.-.---.::. .::-..I ,:.:,:.:: -.. I.. ---,,..:. .........:.
.. ,......",. ...- "N......:., -:..-.-,,,......:. .-...-..,- ,.. .-. --. -l."----:---,-::':.- -,,'' ,,.
FIG. 5.-Polya-Hofmeister Subtotal Gastrectomy. A method commonly employed for securely closing theduodenal stump.
FIG. 6,-Polya-Hofmeister Subtotal Gastrectomy. Isolation of the left gastric artery prior to ligation.INSET.-The raw surface on the lesser curvature which remains after the left gastric artery has been divided,
ligated and is reperitonized.
by copyright. on January 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.24.269.143 on 1 March 1948. D
ownloaded from

AlVarch I948 MAINGOT : Surgical T'reaitmitentt of Chrontic Gastric anid Duodenal Ulcer 54
FIG. 7.-Polya-Hofmeister Subtotal Gastrectomy.The Payr clamp has been applied to the stomach.The commencement of the fashioning of theHofmeister valve. A round-bodied needlethreaded with No. 3 silk is passed through bothwalls of the stomach near the lesser curvature andtied, and the portion of the stomach wall abovethe ligated area is divided close to the clamp.I his manoeuvre is repeated until the right marginof the portion of stomach selected for the stomais reached.
FIG. 9.-Polya-Hofmeister Subtotal Gastrectomy.The introduction of the Cushing right-angledcontinuous posterior suture.
FIG. 8.-Polya-Hofmeister Subtotal Gastrectomy. Aportion of the stomach towards the lessercurvature has been cut free and sutured. Thepart towards the greater curvature is about to beemployed for the anastomosis.
FIG. io.-Polya-Hofmeister Subtotal Gastrectomy.The second continuous posterior suture ispassed as a lockstitch.
by copyright. on January 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.24.269.143 on 1 March 1948. D
ownloaded from

156 POST GRADUATE MEDICAL JOURNAL March i948S.-
..: .......... ..:..::::....::.:.f,.:,.:....,:;.:. :..:!..:......:: :.,. :....:: :,:.:
...-. :'-.'- '..:,. ...... '.'.iii.,... :.-,.........."" ,,, ...'.:.....-.,,,",.4"""' "' ":"', ",, ""' ""' ,.i.,,,, ",,. ..........., "'....
..... .-..---. ..","' ... -'......""..'....... ........-!...... .... .-... ..-...... ..-..... -...-..",,,.:,,, ,,,,, -i-i----!---,,,,,.,,..-.,.,,.,- ----------.'------,--., :.
.....-.---. --..--.----..- ........ ...... ....-.......... .... ......... ......-,.,.........,.-,..,..- ...... ,:.,.::..'... ..............,:.i;r.-.....,....,...:..,'.:.... :.: -:- .: .:.'::...".,-.. ......... .:;: .. -............i..
..". .--- ..... ..----.. --.'. -.-....I..... -..... -.....'......--.-.-- ......"....'........,.......,....-.,.- ....-....,.... .......... ...'.,...-- -li-...!....,... .. .... ,... -ii. ----,-.,,.,-"-.,---"-.:::..:!%' ...
..!:.:.:.. ........ ,..:..::".. ......... R..i... --. ...",...N...",",..:. .: :: .::." .: ...."...'... ': ::.'.., ......:::, ,:::,:.. ::...!.., .!..... :,.:::. :...-..'...:-,. ":.,: .. ,..:.:4'..:.:..:...........I.....-"""'",.:, ,.".,:,:.,..--..,'.:.-..."...:....".....::.:!........:...-'.'.:':.'.":-.....................,2:..:-:,. ,-.: .::...,.'.. 'I-,' -,.........,-...... .::.....:.:,.,.............!'.... .... .... ...:.;:; ...."', ....... ..,. .:.:
.: ::. .... ...:.'. .:,:. :.... .-...:.......-.... ....-...".,.:...:.."-.:!..'-........--.'.-.,:....-...........,..'! ,-.-.-.-..
.-,-..::... ,, ,.... ... .,. ..-..f:.:....:....:'-.:.-..'... -. -." .7
::':'.-' -.. ....:..:..::.::: ,... .,:.I
.-':-... ..-. .'.'...%...'.-'-."" --..:-.-,!,..-i-'.------:---.' i.!----, ..- .,.'-'.. iii........:..::: :.- .-:: !.. .-.-'! .-..... ........- ...,-..:.--.----,.-....:..-._,....-..i.,...,:...-..i..-.. :!.-.-. .- .,.......-.,..2.,.......
" ,. -.. :.:. .:. ";.!...:....::.. .:. -..... ... :. ..: .::.....::.j., .,.,,-"' .:,:-,--.- ..'.-.....-...:.,.-......"............--.....-;...-..,......--.'...-......-.....-.-,I-.:... .,: ..:-, .".. ."..': .., .." .... .:. ..' --",.... ....,,---.,. ---.:. ,,-.-.-,--, ....".--...-...., ",.. .:. ---.:::-..:-,..'.-,.--,::.- -..:.,!.....--.-.... --..
:. ... :::----..-- !..--, -1 S'.--' I"i -'i:.,:...--i ..- .." --... --'i...::--:-::-- .::, ..,....,'.-..."!..........'.......'.', --..--', ----.'!!.----'. --i.,.--.--,. ::. .....;....- -'..,..--..:.- --.. ------..--'.----.--... -.:.--. "i". -'-...--'. ..."'." ...,-..". ...... .- .... ---:..---'---..-,--.::--:.:.i.... ,..-. .......... ...
1:1: .:.,,. -,---..--.- .....,....i!.-., ...-.....,!.....,.......,......g...,...,....,....,......,-,.---....... :..,:. ., ."...:,....;!.. !:;.. -:. ..,:. .-..:::::...:.,:"::,:.... .....,-::..,..:: '..-... .., -.... ...-." ...-' ..".....'."',.-.:.I--..---..-k.::..:..:..?.""', ....:..:,-, ... ...--..,!...-.....,...,..:..-....-...!- .: .t.i....-..-::-:;.---. ...'........ .,::.:.....'.....-.....-....."...,;. .......'..".......'."." .-., -"".::", ..--... ...---..-: :..--."..... ..'... ..-...'--iilY----"--,--.".".-..----".---,."-"--.,-, .'....".....;".'.....'."!...".....'.'.".'.'...'......'..".. -. -11 ....-....-...--...!",..".,.",..,,.....:..:..::!::.-,:..::,:.::::"...:- i ....'--...,.j!: ...--.:----.,..,."--".:-,-, :. .i. :.:. .:. '!!"",j.;:. C!.,..:!I..,....,...,....,...."....,!...".,.,-........"!.,....,.,."-......i..."."..."..."!.....'.."..."....,!.....,,......, .---.."----,:i..,.---,--.-`.: .i:!:----".,,;i.: !.:.,::-,.,:-".,. .:::..'.':...!".".....-'."...i..'.'..'....ii....'.l.;..,,....".;..'."i..-"."i..-..-'.."I...-,. ..:..:. .:,: ,,, ,,,,, ,,,";..,:!: ::.
,. :;..,-,..- .,., ,-. .."----,-----,---. ..;..,...,... .." ...".... ".."-!----.,.i:...".'...,:.,..::: ..-:-". ": .:: t., .... .:!.. ..-.. ... ... .. ..-- .........:.i.:. .;. .;f--:,.:i:.:: ::. -,-.., i-,--" .'."..' .."..'i"'...., -`!.'! !..-,.:.. i..:::. -:. :..%..!. `3 -'---!.----.---"... "'.---." ......, '..." .i...... i: ..-,
:...:---:--- ...;.,.............,....".....":!.... ...II::...;!:..,--:.-,.".; -, .'---.i----;'!--,---,..i.--" ---,-,.",--.".!.......,::: '..-----::.i ..:::...,.i...,.,!,..,,:!;.,....,..,! ,.,--"..: ...." ....-.."...!,,.."!i.--"i-"-...,..,-...?g",".i..,.,..,,....,.,.,.:;...":.,.,....Iie";: ,.:.:.:,.:::.;..ii.!.:;..::,.!::.."..'...:.- -:- "'".!
,,","'"" ,,,;, "'
,,,,
,,...,: :",,,, ,, ,,,
.. ..........-.. .!..-,'.---'. ...,.- :.m .; -----:.!l.;!:--. .I........
::...:.;..!.. .5:.: ". ,:...'.,,,.: -:,.,-,..:.-'.:::-:: .:- .,.:,....1!. ., ,,,, ."'..'.!..'r..'i;..;;:: '!!",;; ,,,,. ,,,,;!,-..:. ...... ....
,, ,,, "",
--,,Mi:: :.:.." ..i.'...":;...,..,...-..".'...', ......"., ":'.'..,...-:... -'?-.!::.i....-,..... -1". "I "'. ..----...-... ... ... .....'... ... ...:::i.`-.,---,.-'- ...., :..,. ..,." ...-.." ...."." ,.-. ..-'.....".,...,., .." .......... ... ...l. ....... .... ........... ..!.....'...... .,--.:: :. -,:1:,,,, ..,,"'-...i."....::..,,"..,,, ,"' "",--".:.""..,:..:..::....:::..:.".. ..-."--,: .,..,...."i....-.......,.,...,.......-', ....'....'...-.'."......,..' .."...-........-...,i,-.-,.:..."......,...f'......'-...;.......,....!!...".."...-,... .::.....::,-.:--.,i,::i:..'.' ".."...".,..." ,.,...".,......,... ...,..-......,., ....,-..,.."...".....-'.-'...,....."!!..".,!:..,....:.: .....:..... ......."" "',,... -...-.. ......' ... ...-... -:,.....- ..... -... ... .:..... .--... .,.,::- :: .-------.:,.----,!, .--.-. :-,.-::..::-" :,:....1 -.. ... -.... ... ... .....-.. .. ., .....:.......I.-...............-............,....,..- ---,---.---,--- ........', .. .. .... -,: """' '-' '.-' .""."!."-.. """" ..........x :i, .:--,c-. f,.
:-.. .... ... ..... -::..:..- .,:: ..-..- .--....'!.'. ..--..-.-'..--.--- 6-.:" --l: ..,..-..'. -...-......-.... ...-..-.. -........-.. ..,:.:.-.... ......:-.:--. ..'...z .... .'......-,-,-.-.::....z.!-.. --i: --:..---------------.:-..'.'.'-..-'..."..:.:.,.....-...-...... ..-.:,-, .-..'. ....." -- ..-I...............-......... ...'. -,,-,.. , i.. ,.-.........i......... ."... ......... :... ..'-....... .;.-.--....,..-..,ii..-.. ,...,. --:-,-:i.,'!:-.-'..---'i::.. .'. ..., ". .-.-..... ..--,--..-.:...... V...-,.:..-".,......-.. -.: ..:.. I .:... ..--. -..---., ----::..!:!i' ...,.- ..'.--.'... .-.-:::-...-.....::........ M.N.I...4".i:?:..:. ?. 11.1-1. ."
.,: .!::-..%::,.-", ",.. A7 ---,: .1 -:-M- W. -t-:.:.;,."..,::.......".,.,;:...:..;':. -:-. .:. .i...:::.i:. ..., '.' -ii -'.ii.. ".....--. "" " "".::,::"..'..-':.:::.:.::...:.._--................- ..... ....- ....- ..-..'! I: .....i. ....'.... ...", ,.....,--,....'-I .-. -,:,:-K:: -....::::.......:. -OiN.:...'. --,---.,--..ll;---,- ........., '....., ...............!""'...."......'.--.... ....'',.'3 Ii-N."....'. ....,.. .. .... ........ ,--..-":il.,, ....'. .".., '.......'....-!..'..'..',.'i::..,......-..-:.;i.........?..-s.."'::.'.:;::.;V......-... ...;."N ",.""" "', "" ,.-,;" " 'r" "....,-, ..... ..... .-.... -.:::..--,-Ii--,. !---..'... I... ..'. "..... ".. .... .. ...., .-...,,..,.....-.....'r '...'...,.....I.-!.--ii"',.1'.,......., -, i'...:.::..;::::.,..!:.:.:i.....i.-......!..;..'.'...-,4 ,--;.--,;:!. .i.....".."', ..."'...."....'... ..'.'..',...-, .,..,,.'....i.'......i...'f.'.i.'....'..'..'.....'.i'.,i!.,'..'.,.,.:: :X.i..i-,.--.:r"-9,;.s ig.;i-"..' ".i "! '! -A .,." .."""......""' .... "", lli........",I..4.............--..-...";i '-'....!'....i.'..' ..'.. ...-- .11." ..'.1--,.-,:..;..'-'-.k'*'.- -'... I..' ...'.., .1", "N..... .-- .-,I-!.i ....'...'i...'.... -`:;I:. ....,;:.:: '-'i,:.:!:::!::i.: '... j.:ii.,..'.. .: ii ...,--'-'--.'---j.! 6. ......:-..'..";-."-."r.,.;i.;,,, ,,, ... -, i" F"-:.!?::."-".::,::- .-"-.-.i .Y;: ,"I"I"',,-----E------l,--., ...., '.." .,.."!.",.......",..,."...,., ,-.-....-.---"-.......,..,,..,.., -....."'.... --
........ -,,,,!.,-...,....."!!..".....,:...::.:...: .., .!........., ... ... ....!.:-.Ji "..." -.--'--'--- " ...'..., ......'...,...,,.",., ....", ....-, ---.--,--.'--"-,--.l-,!x,,'I --,,., .. ... .. .! .l ??!?fiI -.----'---R .;-,.- ....':4'..., --.. ,Ii...,."!,...."......,.,!..,."........,.... ........l.
,.'-'.'.-. ,'. .",
..,,,,,,, ......-, "...-.."!,...,!;, ... .-...... '.."....."........ !i----l--!l--'l -.5 !!'.....":.;.'..':i!i ." .".. -."!:---.,--.'. .::---:.:.: !..f-----.--i,--!---...', ....,-......,"........ ,','-",' """"", "". ............: -:....-,-.-... --..:,.,. .... -.;:----."":..,;:".,:: :.............-...-........--...-...........-..- '...... ........;...:.. !., ...!............ ,.,:. :.. :.:,? .- -:. ....". :::.:. ..:........:::..-I.I.:,-, - *.:.-,.,..,-,, ,,,.:: ,- ,---.!' .',.....-. -'---L-----;.,-.,"'.::.,.:....::-,.... ..-:::;--,;-,-,---:----:----.V ,... ...'...... -: "-:. ;:... ...I.- ,--
"' -:.,::,-.-:--:,.,.... .'.-::-.-. ,.'I.::.-- .-.',' -,,----,--.--,------ ..-. .. .......- -:-,, ,-.:,.,:, ,... ............:%..-...,..:.:;,.,.-...'--..,.:,......-,?.,..,...'..-"..."..!..:.':.. .l.--.--.-. ...
-. .-.,-, :;-.... ...,...-.,.:,:"., .-:-:.,.. i.,.l. ,.:---.---.'.::.,::: -.-.'.'..N.:.':-::::-..s..I. .::.--:. ,.,: ::.. :-:..---.'.:.: .:.. .:,.. :.. ...... -..:;: .... :..:. ,!. :;.. ?...-, -, ,, ,. -.....:: ....;,..,, 'P.. .......... .i...:., -!. --.!:;--" `-'----.. :...'.-:.:;i:.::."-`: .:. ---'!. ""! IE.- -"I;.-L---,!----;:--, ..." .,..: .,...,.. ,.,.,-.- .... .....,,.:.:::.::::. ::.:;; .'. .... .!- .:... -.; ... ........... ,. ....: :..: i!.i.. ..,...,...!: ,,...i:'.'!.'.':::...:.i..!:..:;.."...,...,.,...!i .......'... ."'.. ",:..i-,-.--".-..:.;i:i .:: :'.-Y-.'---:,--Ii.-.".?.. il.:; -.. i...,."..;"....,."."i..,."......,......'....'i...!..".:: 1'. .!".. ..-., -. ?:G.-.!!.,---,;..--'.:::-. .:.:,. ,.:. -.:-, ....:.::.........X.-:. :;..iz... 0 .-...,.!ij::,.':'.'.-?!-..-'.. ........".. ... .. ... "', -"" "' ""' c.:,,,. ..!:!,.!.. .., ..,.-..., ..,!-.-:.::.-::,:::;..:::-!.-. ': ...i,..:; ............-.:..-..:..-4:--.i. .,.. ...:..,T .,..
::.:: :-X!v.-RK-I-- .." .... ."',....;:.. ....P.I.,.".., ..'-J...".1j:,;.." :.,:.4: ... ii.:i;- ::.. `:,",,..::--?,. .."..'...,.:..,....."."....:...,.e."..,.:;..!.i....'..',,,:... .'.-' .:. ---o---.---.----!i.-!!E' ..., .1..:. .1 ......: .:.. j:!:. :.-."..,;!..'. ". ,-I .:-- .....
-'-. .:: :.:Z.:. .:. ..!....-::...".'...,.;,.--...:.:..: -,:.:,:, ". .., .': ."'I"..", ..3 -:1-----.-- ..... .....'...,..."'.-.. -.: ...."", "i..."'..;:;.z. .,.,:.-..-'-Z'.,."2........ ....:.....-... --::...:: .. :........ --"----,mi.:., ,,, ":.:!,....-.. .!,:!: :....
::.....'!.'.. .: ..: ..'.. ::: ::..:: :.-'- ;.---.---.-,i.:, ;:.. .'. ': ...,. -';-i.' -'.--:. ... "' .......:.::--,.,.. :..:... Y.,.:. .... .,% ..... :-: .., ..i.--. ",!...,,....--......-......,:;....'....".......'-..,.-..-..."!.l--.,:,.-."..,:.:.:.... -...-..- -'. :. :. .::m.::...: .-...':.,.. ".
:1 -.,f-.-.:--., ... ....,....,:......... ::: ,.:.. 7.:.,.,-,... ..:::- -'.--.-. ,,...........",..,. :-.-...-:,--4. :.-,.:.:...1 -.. ,-,-.....:,--.-,.--..- .-.,:.::: -':?::::. ....... .- '.,,,"".1...::.:... "' ,--.........!.-.-'- .-.:..::. ......-. .,,, ."", .,.,., .II .".,.
....... ::: .!:.-. .:: -.....,:--.-.................-....;,."..,!::-'...-: --.- ...;..-. i......-i --:.."W.,::.:;. :-:i-.1-k.,:.!.-.l---'."' ","'.!.: ",. ....,:..-.-11 .1-4...i ,"--.----'.':i.... ...... .':::.;!;: .:...., ....-.. .."', ...".., ...."., ..-....-...,.., ..."--,.--. .":: :.:. .! ..- --".:....': ...,...'.,'i.- ..,., .:..-"..,:: -i:.i..:;:.;:-:..,,i.;::;..:.
!:.:.--. .'i::.,:..i,.,.,.i...'..I.-.........i...','.::....,..!i:::.. -;::.--.-:.T.-.;..-..'.,.,.."...,!....,....-,....,....,:...,.":.t'-.-.',...,-..-.......!-'.;.!i;:!.:..:::: .:I-,.--,..:--'.:-,-,:.!:.;: .:: :..::..:.:.:..ii.'.9....'.'!...,.,:i::..:;.....:.;.:....!.%:::.:..-.;::.!:::....", ,!!.:..::..:-.-` ....i....'..";.:;:...,.,ii.li:!..: -'!...;:.'.' ;.' '....:: :.:.:. :.: :!L:: -.!: -..;:-: .:. :.. :;::.;...-.::-,-,.'-. "...'.::.i'....":...,".,,.:....,., ....".....'..."!....'..'....'.'...'i'."I..,!,:..
FIG. II.-Polya-Hofmeister Subtotal Gastrectomy. The first anterior continuous suture is introduced as aSchmieden in-out in-out stitch. Note how the Payr clamp exerts upwards traction and facilitates theintroduction of the sutures.
FIG. I2.-Polya-Hofmeister Subtotal Gastrectomy. After the stomach has been cut adrift the first anteriorcontinuous suture is continued towards the greater curvature, and then tied to the end which has beenleft long.
FIG. I3.-Polya-Hofmeister Subtotal Gastrectomy. Diagram showing the graceful lax, S-shaped, afferent,jejunal limb, the position of the valve, the funnel-shaped gastric pouch, and the site of the stoma. Allnourishment is thereby deflected into the efferent limb of jejunum and none can find its way into theduodenum.
by copyright. on January 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.24.269.143 on 1 March 1948. D
ownloaded from
March I948 MAINGOT: Surgical Treatment of Chronic Gastric and Duodenal Ulcer 157
When resection is considered too hazardous, theulcer should be exposed by an ample incisionthrough the anterior duodenal wall and pyloricsphincter, the edges of the wound held apart withAllis forceps, and four cross mattress sutures ofstrong silk be inserted deeply through the edgesand base of the ulcer and tied very tightly.
This controls the bleeding, obliterates the ulcer,and is, in my opinion, the most efficient emergencymethod of dealing with the bleeding artery.The wound in the anterior wall of the duodenum
and pylorus is then closed transversely, but if,owing to the scarred condition of the bowel wall,this is not possible, then the adjacent edges ofstomach and duodenum are approximated with athree-tier suture and protected with an omentalgraft.
(c) Scar Stenosis due to Long-Standing DuodenalUker and Chronic Penetrating Ulcer. Here thechoice of operation is gastro-jejunostomy or gastricresection. About IS per cent. of all cases ofchronic duodenal ulcer referred to me areeventually subjected to operation, and some 8oper cent. of these undergo resection by the Polya-Hofmeister technique. The so-called irremovableduodenal ulcer is treated by Bancroft's methodplus subtotal gastrectomy, whilst gastro-jejunos-tomy is reserved for those who are obviouslyincapable of withstanding a major surgicalprocedure.
(4) The Technique of the Operations(a) Gastro-jejunostomy. As previously stated,
the indications for this operation are as follows:(i) Pyloric stenosis due to cicatrizing duodenalulcer associated with achlorhydria or hypo-chlorhydria in patients over the age of 6o; (ii)aged and feeble patients with obstructive symp-toms or severe pain due to a decply penetratingulcer; (iii) poor general condition of the patientdue to some concomitant disease rendering gastricresection too hazardous.The posterior operation is in almost every respect
superior to the anterior method of anastomosis.Nevertheless, if the first loop of jejunum is firmlyanchored to the under-surface of the mesocolon, orif there are numerous congenital bands or ad-hesions present in this situation, it may be unwiseto dissect them free in order to facilitate the per-formance of a posterior gastro-jejunostomy. Insuch cases I am convinced that the anZerioroperation is preferable.
Again, the posterior operation may be contra-indicated if the mesocolon is unduly laden withfat, or the middle colic artery or its archingbranches pursue an anomalous course or are im-possible to visualize, if numerous large ramifyingblood vessels occupy the mesocolon and no suitable
space remains between them through which thestomach or jejunum may be drawn, or where themesocolon is unduly stunted or adherent to thestomach bed.
In the posterior operation, if the stomach islarge or dilated as the result of obstruction to itsoutlet, it is best to make the stoma vertical, i.e.,from the lesser curva. xre near the incisura to thelowest point of the greater curvature. If, how-ever, the stomach is small and contracted, alongitudinal stoma, 3 in. long, placed near thegreater curvature but on the posterior wall of thestomach, is preferable. A satisfactory longitudinalstoma should be about a in. away from and parallelwith the greater curvature, and should be evenlybisected by an imaginary line dropped from thelesser curve of the stomach; in other words, itshould be situated at the most dependent portionnf the stomach.The stomi when completed should easily admit
three fingers. The portion of proximal jejunum forthe anastomosis should be chosen with the greatestcare. If the stomach is ptosed, a long loop (8-io in.) will be necessary; but if the organ is ofthe steerhorn type and lies high up in the epigas-trium, a short loop (5-6 ins.) will suffice.The opening in the mesocolon through which
the selected fold of stomach is drawn is made tothe left of the main branch of the middle colicartery, and the edges of the mesocolon are suturedto the stomach wall before the anastomasis iscommenced.Most surgeons follow the practice of Moynihan
and the Mayos and prefer to use large guardedclamps and two continuous sutures when carryingout the anastomosis. The writer usually per-forms gastro-jejunostomy without the aid ofclamps, as spillage does not occur 'when thegastric contents are aspirated before and duringthe operation, bleeding can with assurance becontrolled by well-placed sutures, and the pro-cedure is relatively atraumatic. The methodwhereby three continuous sutures are used is de-picted in Fig. 15. This is the one usually employedby the writer.
Lately, when performing anterior gastro-jejunostomy, I have adopted Lahey's plan (I944)of detaching the vascular gastro-epiploic arch fromthe pylorus to a point 3 in. or so from the lowerpole of the spleen, and of removing the relatedgreat omentum after it has been snipped free fromits filmy attachment to the transverse colon. Withthe omentum out of the way, the field is clear anda relatively snort loop of proximal jejunum averag-ing about 8 in. can be drawn across the baredtransverse colon for anastomosis to the posterioraspect of the stomach near the greater curvature.The stoma (which should be at least 24 in. long
by copyright. on January 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.24.269.143 on 1 March 1948. D
ownloaded from

i58 POST GRADUATE MEDICAL JOURNAL March i948.
and bisected by the imaginary line produceddownwards from the right border of the lessercurvature) should be situated i in. from the greatercurvature and parallel with it, and must in allcases be at the most dependent part of the stomach.There must be no compression of the transversecolon or kinking or traction at the duodeno-jejunal flexure or at the points where the proximaland distal limbs of the jejunum are stitched to thestomach. The operation is performed without theaid of clamps, and three continuous' sutures areemployed, as in making the posterior anastomosis(Fig. 15).
(b) Subtotal gastrectomy by the Polya-Hofmeistermethod. The anterior or ante-colic long-loopmethod is chosen in preference to the posterioroperation for the reasons previously stated, and ifthe first portion of the duodenum containing theulcer can with safety be freed and excised and itsdistal end soundly inturned without any risk ofleakage or of compromising the lower reaches ofthe common bile duct, this should be performedunhesitatingly.When, on the other hand, the duodenum is fixed
to the pancreas by a deeply penetrating ulcer andinflammatory adhesions, the crater has burrowedits way into the precincts of the bile duct, or theinvolved sclerotic bulb is so inaccegsible thatdissection and excision of the first part of theduodenum would prove too hazardous an under-taking, the distal transection should be carriedout through the antrum and the operation be com-pleted on the lines suggested by Bancroft (I932).Most of the deaths which follow partial or sub-
total gastrectomy for duodenal ulcer are due tounnecessary, highly dangerous and protracteddissections of the first portion of the duodenum, orto the surgeon being misguided into believing thatthe cartilagenous-like scarred and fused bulb is astenosing pyloric carinoma which must be am-putated at all costs.
It is, nevertheless, true that with practice andpainstaking dissection most chronic duodenalulcers can be excised, or at least the first portionof the duodenum can be cleared, divided, andclosed in a watertight fashion even if the crater isleft behind embedded in the substance of thepancreas.
It is important to close the duodenal stump verysecurely with at least two rows of unabsorbablesuture material, and if there .is any doubt aboutthe integrity of the suture line, the area should bedrained with a Penrose'or corrugated rubber tubethrough a stab incision in the flank.As most duodenal ulcers seen at operation are
posterior and superior, i.e., involve the posteriorwall and the lesser curvattre of the duodenum,and as with such lesions the right margin of the
gastro-hepatic omentum is usually contracted andof leathery consistency, the dissection and isolationof the right gastric artery should be carried outcautiously and with due respect to the common bileduct, and to the main branch of the hepatic arterywhich may be drawn downwards by denseadhesions.
In most cases I now display the common bileduct and ascertain the relations of the ulcer to theduct. Sometimes the commnon bile duct is openedand a Bakes dilator is passed into the duodenum, oragain one limb of a large T-tube may be intro-duced through the opening in the choledochus andthen on through the papilla so that the duct canbe seen and felt during the dissection of the ulcerfrom the pancreas. If the duct is opened forprobing or the passage of a sound, it is alwaysdrained by means of a T-tube. The T-tube is re-moved on the seventh post-operative day.The operation is planned. for acid reduction,
hence nothing short of subtotal resection of theorgan will suffice. Pylorectomy, hemi-gastrec-tomy and partial gastrectomy, whether for canceror for ulcer, are operations of a former decade.
I have learned that it is not necessary to pre-serve the vascular epiploic arch intact. The bloodvessels in the great omentum do not become in-farcted nor does gangrene of this structure super-vene when the arteries below the arch are ligaturedand divided.The mortality of subtotal gastrectomy for
chronic duodenal ulcer is low. At the MayoClinic. during 1943 no fewer than I9I cases weresubjected to this operation, and only one patientdied (from pulmonary embolism). In 1945, 241cases were treated by gastric resection with fourdeaths (I.7 per cent.).
In the hands of a skilled and careful surgeonworking under the best conditions, the death-ratefollowing gastric resection for duodenal ulcershould not exceed 3 per cent.
(c) Bancroft's procedure. This operation isemployed for the irremovable duodenal ulcer. Itconsists in making a circular incision through theseromuscular coats of the antrum about threefinger-breadths above the pyloric sphincter, anddissecting the pyloric mucous membrane free toa point where it is embraced by the muscularring.The separation of this cuff of mucous membrane
from its seromuscular sheath should be conducteddaintily and cautiously, and more especially as thedissection proceeds towards the sphincteric ringwhere the membrane is soft, oedematous andfriable. Any fissuring or tearing of the lining ofthe pyloric canal itself might be followed by seriousconsequences-leakage, abscess, peritonitis,duodenal fistula, etc.
by copyright. on January 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.24.269.143 on 1 March 1948. D
ownloaded from
March i948 MAINGOT: Surgical Treatment of Chronic Gastric and Duodenal Ulcer
A purse-string suture of No. oo medium chromiccatgut, which picks up only the submucosal coat,is passed around the unopened tube of mucousmembrane close to the pyloric sphincter, afterwhich the mucous membrane is cut away betweenhaemostats. The haemostat near the purse-string suture is removed and the crushed mucousrim is immediately invaginated as the purse-string suture is drawn taut. The tube of mucousmembrane should not be ligated and then cutaway, as leakage is likely to ensue (Fig. I6(3)). Oneor two other purse-string sutures placed on theexposed pyloric muscle complete the closure. Thesuperfluous seromuscular sheath is trimmed downand its margins drawn together with a sewing-machine stitch, and the stubby end of the pylorussmothered in omentum. No dead spaces shouldbe allowed to remain between the invaginatedstump of mucous membrane in the pyloric canaland the freed seromuscular sheath. The opera-tion is completed. by performing an ante-colicPolya-Hofmeister subtotal gastrectomy after themanner already described.Some years ago Finsterer advocated transection
of the antrum and distal closure followed bygastric excision for these irremovable ulcers of theduodenum. The late results of the operation arebad; jejunal ulceration is a common sequel, asOgilvie (I938) and others have shown; it leavesbehind in the pyloric mucous membrane an agentof evil-a hormone which stimulates the principalglands to pour out pepsin and hydrochloric acid,while the stump occasionally blows out when thesecretions generated in the antral mucous mem-brane cannot escape through a stricturedduodenum. This operation should, therefore, neverbe practised.On the other hand, Bancroft's procedure leads in
time to complete healing of the ulcer, which isconstantly bathed in alkaline juices and freedfrom the irritating breaking-down products ofdigestion. The ulcer heals rapidly and in time thefirst portion of the duodenum becomes free anddetached from subjacent pancreas. In a personalseries of 88 cases treated by Bancroft's methodthere were two deaths-both from peritonitis.
Drainage of the right subhepatic space is carriedout as a routine procedure after Bancroft's opera-tion, when T-tube drainage of the common bileduct has been performed, and also following allthose cases in which there is any doubt about theeffective closure of the duodenal stump.
(d) Vagotomy. Vagotomy, or gastric neurec-tomy by the transthoracic or abdominal route, isan interesting and fascinating lesson in humanphysiology. It is too early as yet to speak of lateresults or of what place this operation is destined totake in the treatment of duodel uker or ofgastro-
jejunal uker. At the present time I reserveabdominal gastric neurectomy for the followingtypes of cases: (i) Young patients with uncom-plicated lesions in whom repeated and prolongedtreatment in hospital has failed to effect a cure;(ii) patients under the age of 6o with chronicduodenal ulcer in whom gastric resection isdeemed too hazardous. Here the vagotomy iscombined with gastro-jejunostomy; and (iii)those cases of gastro-jejunal ulcers which havefollowed in the wake of a well-performed subtotalgastrectomy.
I do not advise transthoracic vagotomy for (iii)<as I believe that by the abdominal route large seg-ments of the right and left vagus nerves can be-resected after the surgeon has assured himself thatthe amount of stomach removed is adequate, thatthe stoma is well placed and that a gastro-jejuno-colic fistula can be excluded with safety. I wouldnot now perform vagotomy plus, gastro-jejunostomy for aged patients, as the atony of thestomach and jejunum which follows the resectionof the vagus nerves in such patients may last forseveral weeks or even months.Some of my patients have experienced a number
of ill-effects following vagotomy, including in-tractable diarrhoea, the frequent belching of malo-dorous gases, and prolonged retention. Duringthe last i8 months I have performed this operationon 36 patients, and my experience would lead meto suggest that we should reserve, this operationstrictly for the types of cases I have mentiornedabove.The reader is referred to the writings on this
subject by Dragstedt, who has now a series ofcases dating back to 1943, to Allen's MoynihanOration (I947), and to Walters' valuable and in-structive paper in the ' Proceedings of the StaffMeetings of the Mayo Clinic' (22, 28i, 1947).
Comments on Other Operations forDuodenal UlcerHorsley's pyloroplasty (i9I9), Judd's pylorm-
plasty (I922), Jaboulay's gastro-duodenostomy(I892), and Finney's gastro-duodenostomy (i9o2)are all inferior to a well-performed gastro-jejunostomy and are seldom practised to-day.The Billroth I operation, however, is popular in
certain clinics and has many able exponents. Whenemployed in the treatment of chronic duodenalulcer it is open to the following objections:
i. The surgeon, unless he is experienced in theperformance of this method, is often more con-cerned about an easy approximation of the cutend of the stomach to the cut end of the duodenumthan with a wide resection of the stonach.
2. As a result of long-standing ulceration, theduodenum may be shortened, distorted, and- the
by copyright. on January 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.24.269.143 on 1 March 1948. D
ownloaded from

i6o POST GRADUATE MEDICAL JOURNAL March I948
seat of a widespread duodenitis. Again, evenwhen it can be mobilized, the part which remainsafter the removal of the ulcer-bearing area, to-gether with the surrounding zone of inflammation,is always short, inaccessible and difficult toapproximate to the small gastric pouch, whileend-to-end union may be, and often is, a tediousand anxious undertaking in such circumstances.
3. When the anastomosis is completed, theparts often appear fixed, tense and strained, astate of affairs incompatible with sound healingand sound functioning.
4. The duodenum is a thin-walled friablestructure and quite devoid of peritoneum on itsposterior surface, and it is for these reasons thatextraordinary precautions are taken when fashion-ing the stoma to prevent leakage, peritonitis, theproduction of a valve, or extreme narrowing of thenew opening.
5. Thv late results are by no means so satis-factory as when the Polya-Hofmeister procedure isemployed.
ConclusionsI. The chief indications for operation in cases
of chronic duodenal ulcer are:(a) Acute perforation.(b) Uncontrollable bleeding.(c) Pyloric obstruction due to a stefosing
lesion.(d) Intractability-failure to respond to
medical treatment.2. The operation of choice is the ante-colic
Polya-Hofmeister subtotal gastrectomy. Ban-croft's procedure is reserved for the irremovableduodenal ulcer. Vagotomy, promising as it ap-pears to be, is as yet under trial.
3. Gastro-jejunostomy should be chosen inpreference to gastric resection for aged and infirmpatients, and for elderly patients with pyloricstenosis associated with low acid values in thegastric juice, and for those who, owing to somedebilitating condition, are considered to be pooroperative risks.
4. The pre-operative preparation of thesepatients has- been a great factor in loweringmortality-rate which is now under 3 per cent.
BIBLIOGRAPHYBABCOCK, W. W. (1942), Surg., Gynec. and Obst. 75 485.COUNSELLER, V. S., WAUG,H, J. M., and CLAGhTT, 0. T.
(X944), Proc. Staff Meet. Mayo Clinic., I9, 569.CULLIGAN, L. C. (1944): Surg., Gynec. and Obst., 79, 629.,FINNEY, J. M. T. (902) Bull. Johns Hopkins Hospital, 13, z$5.FINOCHIETTO, E. (936i, Post-Graduate Surgery (Ed. R. Main-
20t) I, 526.FINTIRER, H. (I934), Rev. de Chir., 72, SI1.FINSTERER, H. (1958), Zentrabl. f. Chir., 26, 434.FREEMAN, H. (194), Brit. 3. Surg., 32, 303.GRAHAM ROSCOE R. (1937) Surg. Gynec. and Obst. 64 235.HOLMES, G. W., and HAMVIHON, A. 0. (1932), .A..2. 99,
HORSLEY, J. S. (i9Ig), Y.A.M.A., 73, 575.JUDD. E. S. (1922),. Lacet., 42, 381,
LAHEY, F. (I944), Surg., Gynec. and Obst., 78, I69.MAINGOT, R. (I940), 'Abdominal Operations,' Appleton-
Century Co.MAINGOT, R. (I941), 'Technique of Gastric Operations,' Oxford
Univ. Press.MAINGOT, R. (r942), Post Graduate Medical j., I8, 93.MATTHEWS, W. B. (I935). Ann. Surg., IoI, 844.MORLOCK, C. G. (I944), Proc. Staff. Meet. Mayo Clinic, I9,
OGIkV9IE, W. H. (1938), Lancet, 2, 295.PANNETT, C. A. (1938),Surg., Gynec. and Obst., 67, 495.PANNETT, C. A. (1924), Brit. J. Surg., 12, 273.PANNETT, C. A. (s945), Brit. Y. Surg., 32, 4I8.POLYA, E. (I9Ii), Zbl. f. Chir., 38, 892.SIPPY, B. W. (19I5), 7.A.M.A., 64, I625.WANGENSTEEN, 0. H. (1940), Surg., Gynec. and Obst., 70, 58.WANGENSTEEN 0. H. (I937), J. Lancet, S7, I.WANGENSTEEN, 0. H. (I941), Surg., Gynec. and Obst., 72, 257.
Scheme of Nursing for SubtotalOastrectomy CasesMost cases are admitted to surgical wards seven
days before operation.Seven- to three days before operation: Strict
medical treatment; correct anaemia and dehydra-tion; gastric aspiration and lavage to relieve anyobstructive symptoms; attention to bowels; en-sure sound sleep at night; give vitamins A, Band C in full dosage.Two days before operation: Diet, Meulengracht
I. Paraffin i oz. b.d.; soap enema. Continuevitamin treatment; sleeping draught at night;pass a Ryle tube through nostril into the stomachand aspirate gastric contents, after which irrigatewith warm saline solution.One day before operation: Same as above.
Shave abdomen and pubic region, wash with ethersoap, and paint with euflavine-alcohol; applydry dressing.Day of operation: From I2 midnight give clear
fluids only by mouth. Pass Ryle tube, wash outstomach, leave tube in situ, fixing end of tube tocheek, and insert wooden spiggot.On return from operating room: Shock treat-
ment (if required); raise end of bed on blocks;give intravenous glucose-saline, plasma, serum orblood transfusion. Omnopon gr. i when fullyrecovered from anaesthetic, and then omnopongr. W six-hourly; 0° by B.L.B. mask for fiveminutes hourly (whilst awake) ; ' stir-up' treat-ment-make patient sit up in bed, breathe deeply,and cough hourly, change his position in bedfrequently and move arnis and legs i,ooo timesdaily. Using a 20 cc. Record syringe, aspirate theRyle tube two-hourly, and occasionally irrigatethe stomach with 20 CC. of warm saline; the Ryletube is left in situ for about 36-48 hours; thepatient is allowed to drink as much as two to threepints of clear fluids during the first 24 hours afteroperation. Keep a 24-hour intake and outputchart; keep an hourly pulse chart until pulsesettles down below 8o; examine the urine daily.Give penicillin 25o,000 units -intramuscularly six-hourly for four days.
by copyright. on January 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.24.269.143 on 1 March 1948. D
ownloaded from
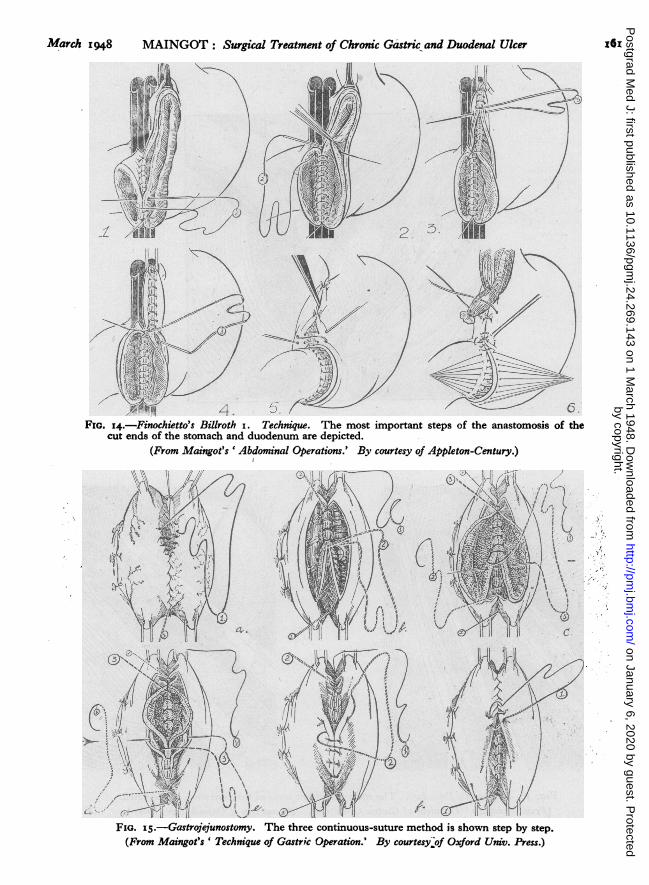
March i948 MAINGOT: Surgical Treatment of Chronic Gastric and Duodenal Ulcer
I
I
.6
* 4FIG. 14.-Finochietto's Billroth i. Technique. The most important steps of the anastomosis of the
cut ends of the stomach and duodenum are depicted.(From Maingot's 'Abdominal Operations.' By courtesy of Appleton-Century.)
f' rsJ E.s.FIG. IS.-Gastreoyjunostomy. The three continuous-suture method is shown step by step.(From Maingot's ' Technique of Gastric Operation.' By courtesy,of Oxford Univ. Press.)
by copyright. on January 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.24.269.143 on 1 March 1948. D
ownloaded from

x62 POST GRADUATE MEDICAL JOURNAL March I948
/k\ . '4 1.
4 F,,
(7
i~
1,I N1 N
FIG. I6.-Eancroft's Procedure. The more important steps of this operation are depicted.(From Maingot's ' Technique of Gastric Operations.' By courtesy of Oxford Univ. Press.)
by copyright. on January 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.24.269.143 on 1 March 1948. D
ownloaded from

March i948 MAINGOT: Surgical Treatment df Chronic Gastric and Duodenal Ulcer 163
DIET FOR GASTRIC PATIENTS
Modified Meulengracht
(I) (2) (3)
6 a.m. 3-5 oz. sweetened flavoured As No. i. As No. I.milk.
8 a.m. 3-5 oz. milk and one beaten 5 oz. milk, one egg lightly boiled or One egg lightly boiled or poached,egg. poached. Thin crustless bread or white fish baked in milk or
and butter (2 slices). steamed. Thin crustless bread (3slices) and butter. Very weakmilky tea.
10 a.m. 3-5 oz. sweetened flavoured As No. I. As No. i.milk.
12 noon. Pounded fish or 3 oz. minced Steamed or baked fish, 4 oz., and As No. i and 2, or minced lamb orand pounded sweetbreads sauce, or as No. i. Mashed mutton, 3 oz., or minced rabbit.or brains or chicken. 2j potatoes, 2 tb.sp. Sieved veget- Mashed potatoes, 3 tb.sp. Sievedmashed potatoes, 2 tb.sp. ables, 2 tb.sp. Milk pudding, vegetables, 2 tb.sp. Milk pud-Sieved vegetables, 2 tb.sp. custard or jelly. Av. serving. ding, custard or jelly. Av. serving.Milk pudding, custard orjelly. Av. serving.
2 p.m. 3-5 oz. sweetened flavoured As No. i. As No. i.milk.
4 p.m. 3-5 oz. milk and one beaten 5 oz. milk. One egg lightly boiled Very weak milky tea. Then asegg or sieved fruit. Milk or poached, or sieved fruit. Thin No. 2.jelly, custard or trifle or crustless bread and butter (2junket. slices). Milk jelly, custard, trifle
or junket.
6 p.m. 3-5 oz. sweetened flavoured As No. I. As No. I.milk. Milk pudding.
8 p.m. 3-5 oz. sweetened flavoured As No. I. As No. i.milk.
During Nights. 7 oz. milk if awake. As No. i. As No. i.
To flavour milk use Ovaltine, Bengers, Horlicks or Bourn-vita.All vegetables are cooked, rminced and sieved.Fish, sweetbreads, tripe and brains for No. i diets are minced and pounded and mixed with white sauce.Milk pudding as follows: Rice, sago, tapioca, ground rice, chocolate blancmange, vanilla blancmange (with custard
powder), semolina, using strained fruit juice to flavour when possible.Approximate caloric value:
No. I ... . . .. . .I,500No. 2 .. .. *.. .. .. .. 1,900No. 3 . .. .. .. .. .. 2,000
The above schemes of nursing and diets for gastric cases are subject to alterations and modifications in individualcases.
by copyright. on January 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.24.269.143 on 1 March 1948. D
ownloaded from

164 POST GRADUATE MEDICAL JOURNAL March i948
First day after operation: Induce patient todrink two to three pints of clear fluids and weaktea; stomach aspirations two-hourly; continuestir-up treatment. Omnopon gr. J p.r.n. for pain,if required. Ensure sound sleep at night by meansof Soneryl, Seconal, Amytal or Medinal. Recom-mence vitamin treatment and continue for tendays. Get patient out of bed for short time.
Second day after operation: Ryle tube removedabout 36-48 hours after operation; after removalof Ryle tube patient has only sips of clear fluid forfirst six hours, and after that 4 oz. hourly. Con-tinue deep breathing exercises.
Third day after operation: Give 4 oz. hourly ofwater, barley water, glucose water, Bovril, weaktea, fruit juices, etc.; sweets; paraffin I oz.. b.d.by mouth; continue vitamins and sedative drugsfor a few more days. Allow patient out of bed fora short while every day.
Fourth day after operation: Increased feeds;jellies, junkets, custards, blancmanges, eggs,paraffin i oz. b.d. Insert two glycerine sup-positories; if no result give soap or olive oil andparaffin enema.
Fifth and sixth days after operation: Meulen-gracht I diet. Skin stitches removed. Paraffini oz. b.d.; glycerine suppositories or enema ifrequired.
Seventh to tenth day after operation: Meulen-gracht II or III according to condition of patient.After the tenth day the patient is put on full dietand given a tonic mixture containing iron andarsenic.
Meulengracht DietsWeak tea, fruit juice, glucose water or barley
water may be substituted for milk drinks in theMeulengracht I Diet Scheme.
BOOK REVIEWS
CANCER OF THE BREAST
By D. C. L. FITZWILLIAMS, C.M.G., M.D., Ch.M.,F.R.C.S. William Heinemann Medical BooksLtd. I947. Pp. i99 with zo plates. Price 25s.This book appears opportunely when consider-
able interest is being revived in more conservativeoperative procedures, assofiated with radiotherapy,for the treatment of carcinoma of the breast. Theauthor has spent much of his life treating thisdisease and he illustrates his text with a greatnumber of case records which add weight to hisargument.He divides the disease into the four stages,
primary growth, lymphatic spread, floating celland metastasis. He proceeds to discuss the spreadof the tumour laying stress on the blood stream as avehicle for carcinoma cells. The chapter devoted toearly diagnosis is excellent and the case historiesappended, illustrating the mistakes made by thepractitioner and surgeon, are very instructive. Theuse of transillumination in investigating a tumour inthe breast is described as the surest and earliestmethod in the hands of those who are familiar withit.
Treatment by local removal, radical operationand radium is described in detail and illustrated byphotographs. Stress is laid on the value of radio-therapy and much valuable information is providedas to what can and cannot be expected from radiumand X-rays.
There is an additional chapter by Miss AliceRoss on the principles of X-ray therapy in bothoperable and inoperable mammary carcinomi. Theindex is deplorable and quite unworthy of the book.This is a valuable and stimulating addition to the
surgeon's library on carcinoma of the breast.S.F.T.
THE TREATMENT OF SOME CHRONIC ANDINCURABLE DISEASES
By A. T. TODD, O.B.E., M.B., Ch.B., M.R.C.P.2nd Edition. John Wright & Sons, Ltd. Pp.324. 1947. Price 25s.The reviewer finds himself in disagreement with
many of the author's views. Dr. Todd believes that'duodenitis 'produces poor respiratory m:vementsand thus inadequate return of blood to the heart;the inadequate venous return leads, we are told(p. 145), to inadequate aortic pressure-coronarydisease and myocardial degeneration. Later (p. I 56)however, he tells us that inadequate venous returnleads to hyperpiesia. His explanation of dysmenor-rhoea on the basis of faulty fat metabolism pro-ducing faulty sterols and so faulty oestrins andluteins (p. 136) is typical of the hypotheses withwhich the book abounds.
Dr. Todd's theory of diabetes is that the disease(like many others) is due to hepatic dysfunction,and that insulin is to be avoided except to rescue thepatient from the diabetic coma into which he has
by copyright. on January 6, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.24.269.143 on 1 March 1948. D
ownloaded from





























