-
Surgical Treatment of Burns
Author: Gail E Besner, MD; Chief Editor: Harsh Grewal, MD, FACS,
FAAP more...
Updated: Apr 2, 2012
Background
Traumatic injuries cause more deaths in childhood than all other
causes combined. Although motor vehicle injuries arethe foremost
cause of death, each year approximately 440,000 children receive
treatment for burns in the UnitedStates. More than 75,000 of these
children require hospitalization, 10,000 experience severe
permanent disability, and2,500 die from thermal injury. Burn
injuries represent the third leading cause of mortality in patients
younger than 5years. The overall morbidity from thermal injury has
improved markedly over the years as a result of an
aggressivemultidisciplinary approach to care for the pediatric
patient with thermal injury.
Etiology
Approximately 90% of burns are caused by household accidents or
child abuse. In children younger than 3 years,
scalds are responsible for most burns.[1] Scald burns may occur
when a child pulls scalding liquid onto himself or mayresult from
bathtub submersion injuries, which can often be quite severe. In
older children, flame burns are morecommon. Space heaters, matches,
and house fires are the most common etiologic factors for these
burns, which areoften full thickness and constitute most fatal
burns.
Pathophysiology
Appreciating the major differences between burn management in
children and adults is important. Children have nearly3 times the
body surface area (BSA)-to-body mass ratio of adults. Fluid losses
are proportionately higher in childrenthan in adults. Consequently,
children have relatively greater fluid resuscitation requirements
and more evaporativewater loss than adults. The large BSA-to-body
mass ratio of the child also predisposes the child to hypothermia,
whichmust be aggressively avoided.
Children younger than 2 years have thinner layers of skin and
insulating subcutaneous tissue than older children andadults. As a
result, they lose more heat and water than adults do, and they lose
these more rapidly than adults. In veryyoung children, temperature
regulation is partially based on nonshivering thermogenesis, which
further increasesmetabolic rate, oxygen consumption, and lactate
production. In addition, because of disproportionately thin skin, a
burnthat may initially appear to be partial thickness in a child
may instead be full thickness in depth. Thus, the child's thinskin
may make initial burn depth assessment difficult.
Presentation
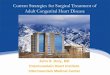
The depth of burn is classified as follows (see the image
below):
Medscape ReferenceReference
News
Reference
Education
MEDLINE
Surgical Treatment of Burns
http://emedicine.medscape.com/article/934173-overview
1 of 5 8/8/2012 3:18 PM
Generated by Foxit PDF Creator Foxit
Softwarehttp://www.foxitsoftware.com For evaluation only.
-
Skin histology diagram.
Superficial partial thickness
These burns are superficial with injury to the epidermis and
superficial dermis. These are second-degree burns andare
characterized by ruptured weeping blisters. They are also
erythematous and painful. Superficial partial-thicknessburns
spontaneously heal within 1-3 weeks, usually without scarring (see
the image below).
Superficial partial-thickness burn.
Deep partial thickness
These are deep burns with injury to the epidermis and deeper
dermis, but some viable dermis remains. These arealso considered
second-degree burns but are whiter and less erythematous as the
depth into the dermis increases.Distinguishing between deep
partial-thickness burns and full-thickness burns may initially be
difficult. Deep partial-thickness burns heal spontaneously but
often after 3-4 weeks. The degree of scarring is related to the
length of timeneeded for reepithelialization. See the image
below.
Deep partial-thickness burn.
Full thickness
Injury to the epidermis and entire dermis occurs. These are the
third-degree burns that typically are white, brown, orblack. The
eschar is leathery and insensate. These burns do not heal
spontaneously (except for very small woundsthat heal by
contraction). See the image below.
Full-thickness burn.
Electrical burns
Low-voltage injuries result from sources of less than 1000 volts
and include oral injuries from biting electrical cords,outlet
injuries from placing objects into wall sockets, and injuries from
contacting live wires or indoor appliances.High-voltage injuries
are caused by sources of more than 1000 volts and result from
contact with a live wire outdoorsor from being struck by
lightning.
Surgical Treatment of Burns
http://emedicine.medscape.com/article/934173-overview
2 of 5 8/8/2012 3:18 PM
Generated by Foxit PDF Creator Foxit
Softwarehttp://www.foxitsoftware.com For evaluation only.
-
Children who have sustained high-voltage electrical injury
require admission to the hospital with cardiac monitoring,serial
electrocardiography, urinalysis, and determination of creatine
kinase and urine myoglobin levels. Myoglobinuriaand hemoglobinuria
should be aggressively treated with hydration, osmotic diuretics,
and alkalinization of the urine toavoid renal failure. Extremities
must be carefully monitored for the development of compartment
syndrome,necessitating escharotomy or fasciotomy. Appropriate
radiographic examinations should be performed to excludeconcomitant
long bone injury.
Many children who have sustained low-voltage electrical injury
can be treated as outpatients as long as (1) the patienthas no
cardiac dysfunction, loss of consciousness, or history of tetany or
wet skin during the accident; (2) the patientremains asymptomatic
after 4 hours of observation in the emergency department; (3) the
wounds are manageable inan outpatient setting; and (4) the patient
can return for a wound check the following day. Parents of children
with oralcommissure burns must be instructed in the application of
pressure to the lip in the event that the burn erodes into
thelabial artery, a complication that usually does not develop
until several days after the injury.
Frostbite
Frostbite results from prolonged exposure to severe cold and
usually affects the ears, nose, hands, and feet. Icecrystal
formation in the tissues results in cellular dehydration, venous
dilation and vasoconstriction causing peripheralblood pooling, and
finally, tissue necrosis.
Signs and symptoms of frostbite include red, blue, or pale skin;
a prickling sensation with superficial frostbite; painlessrigid
skin with deep frostbite; and functional impairment.
Treatment involves placing the patient in a warm environment,
removing clothing from the affected region, andrewarming the
affected region by immersion in water at 100-105F for up to 30-45
minutes. Do not rewarm the frozenpart with massage or dry heat.
Chemical burns
Saturated clothing should be removed, powdered chemicals should
be brushed off the skin, and the contaminatedarea irrigated with
copious amounts of water for at least 20 minutes, and until the
patient experiences a decrease in
pain in the wound.[2]
Chemical injuries to the eye are treated by forcing the eyelid
open and flushing the eye with water or saline.
With gasoline injuries, the petroleum products may cause severe
full-thickness cutaneous tissue damage, andabsorption of the
hydrocarbon may cause pulmonary, hepatic, or renal failure.
Indications
Burn excision and grafting are recommended for all
full-thickness burns and for deep partial-thickness burns that
wouldappear to take more than 2-3 weeks to heal.
Relevant Anatomy
See Clinical for a discussion of relevant anatomy in patients
with burn injuries.
Contraindications
Any condition that would ordinarily preclude the patient with
burn injuries from having general anesthesia, otherwise
nocontraindications to surgery are noted.
Contributor Information and DisclosuresAuthorGail E Besner, MD
John E Fisher Endowed Chair in Neonatal Reseach, Director,
Pediatric Surgical Research,Department of Surgery, Nationwide
Children's Hospital; Professor of Surgery and Pediatrics,
Department ofSurgery, Ohio State University College of Medicine
Gail E Besner, MD is a member of the following medical
societies: Alpha Omega Alpha, American Academy ofPediatrics,
American Burn Association, American College of Surgeons, American
Gastroenterological Association,American Medical Association,
American Medical Women's Association, American Pediatric Surgical
Association,Association for Academic Surgery, Federation of
American Societies for Experimental Biology, Society of
CriticalCare Medicine, Society of Surgical Oncology, and Society of
University Surgeons
Disclosure: Nothing to disclose.
Surgical Treatment of Burns
http://emedicine.medscape.com/article/934173-overview
3 of 5 8/8/2012 3:18 PM
Generated by Foxit PDF Creator Foxit
Softwarehttp://www.foxitsoftware.com For evaluation only.
-
Coauthor(s)Iyore Amy Otabor, MD Clinical Instructor House Staff,
Department of General Surgery, The Ohio State UniversityCollege of
Medicine
Iyore Amy Otabor, MD is a member of the following medical
societies: American College of Surgeons, AmericanMedical Student
Association/Foundation, and Student National Medical
Association
Disclosure: Nothing to disclose.
Specialty Editor BoardDenis Bensard, MD Director of Pediatric
Surgery and Trauma, Attending Adult and Pediatric Acute Care
Surgery,Attending Adult and Pediatric Surgical Critical Care,
Denver Health Medical Center; Professor of Surgery, Universityof
Colorado School of Medicine
Denis Bensard, MD is a member of the following medical
societies: Alpha Omega Alpha, American Academy ofPediatrics,
American College of Surgeons, American Pediatric Surgical
Association, Association for AcademicSurgery, International Society
for Minimally Invasive Cardiac Surgery, Society of American
Gastrointestinal andEndoscopic Surgeons, Society of
Laparoendoscopic Surgeons, Society of University Surgeons, and
SouthwesternSurgical Congress
Disclosure: Nothing to disclose.
Mary L Windle, PharmD Adjunct Associate Professor, University of
Nebraska Medical Center College ofPharmacy; Editor-in-Chief,
Medscape Drug Reference
Disclosure: Nothing to disclose.
Michael G Caty, MD Professor of Surgery and Pediatrics, State
University of New York at Buffalo; ConsultingStaff, Department of
Pediatric Surgery, Children's Hospital of Buffalo
Michael G Caty, MD is a member of the following medical
societies: American Academy of Pediatrics, AmericanCollege of
Physician Executives, American College of Surgeons, American
Medical Association, AmericanPediatric Surgical Association,
Association for Academic Surgery, and Association for Surgical
Education
Disclosure: Nothing to disclose.
H Biemann Othersen Jr, MD Professor of Surgery and Pediatrics,
Emeritus Head, Division of Pediatric Surgery,Medical University of
South Carolina
H Biemann Othersen Jr, MD is a member of the following medical
societies: Alpha Omega Alpha, AmericanAcademy of Pediatrics,
American Association for the Surgery of Trauma, American Burn
Association, AmericanCancer Society, American College of Surgeons,
American Medical Association, American Pediatric
SurgicalAssociation, American Society for Parenteral and Enteral
Nutrition, American Surgical Association, AmericanThoracic Society,
British Association of Paediatric Surgeons, Society for Surgery of
the Alimentary Tract, Society ofCritical Care Medicine, South
Carolina Medical Association, Southeastern Surgical Congress,
Southern MedicalAssociation, Southern Society for Pediatric
Research, and Southern Thoracic Surgical Association
Disclosure: Nothing to disclose.
Chief EditorHarsh Grewal, MD, FACS, FAAP Clinical Professor of
Surgery, Temple University School of Medicine; Chief,Division of
Pediatric Surgery, Cooper University Hospital
Harsh Grewal, MD, FACS, FAAP is a member of the following
medical societies: American Academy of Pediatrics,American College
of Surgeons, American Pediatric Surgical Association, Association
for Surgical Education,Children's Oncology Group, Eastern
Association for the Surgery of Trauma, International Pediatric
EndosurgeryGroup, Society of American Gastrointestinal and
Endoscopic Surgeons, Society of Laparoendoscopic Surgeons,and
Southwestern Surgical Congress
Disclosure: Nothing to disclose.
References
Lowell G, Quinlan K, Gottlieb LJ. Preventing unintentional scald
burns: moving beyond tap water. Pediatrics.
Oct 2008;122(4):799-804. [Medline].
1.
O'Neill TB, Rawlins J, Rea S, Wood F. Complex chemical burns
following a mass casualty chemical plant2.
Surgical Treatment of Burns
http://emedicine.medscape.com/article/934173-overview
4 of 5 8/8/2012 3:18 PM
Generated by Foxit PDF Creator Foxit
Softwarehttp://www.foxitsoftware.com For evaluation only.
-
Medscape Reference 2011 WebMD, LLC
incident: How optimal planning and organisation can make a
difference. Burns. Feb 20 2012;[Medline].
Gupta SS, Singh O, Bhagel PS, Moses S, Shukla S, Mathur RK.
Honey dressing versus silver sulfadiazenedressing for wound healing
in burn patients: a retrospective study. J Cutan Aesthet Surg.
Sep
2011;4(3):183-7. [Medline]. [Full Text].
3.
Jeschke MG, Finnerty CC, Kulp GA, Przkora R, Micak RP, Herndon
DN. Combination of recombinant humangrowth hormone and propanol
decreases hypermetabolism and inflammation in severely burned
children.Pediatr Crit Care Med. Mar 2008;9:209-216. [Medline].
4.
Coruh A, Yontar Y. Application of Split-Thickness Dermal Grafts
in Deep Partial- and Full-Thickness Burns: ANew Source of Auto-Skin
Grafting. J Burn Care Res. Nov 10 2011;[Medline].
5.
Chan MM, Chan GM. Nutritional therapy for burns in children and
adults. Nutrition. Mar 2009;25(3):261-9.
[Medline].
6.
Besner GE. Burns. In: Glick PL, Pearl RH, Irish MS, et al, eds.
Pediatric Surgery Secrets. ed. Philadelphia,
PA: Hanley & Belfus; 2000:246-52.
7.
Heimbach D. What's new in general surgery: burns and metabolism.
J Am Coll Surg. Feb
2002;194(2):156-64. [Medline].
8.
Herndon DN, Hart DW, Wolf SE, et al. Reversal of catabolism by
beta-blockade after severe burns. N Engl J
Med. Oct 25 2001;345(17):1223-9. [Medline].
9.
Hildreth M, Gottschlich M. Nutritional support of the burned
patient. In: Herndon D, ed. Total Burn Care.
Philadelphia, PA: WB Saunders Co; 1996:237-45.
10.
Paddock HN, Fabia R, Giles S, Hayes J, Lowell W, Besner G. A
Silver Impregnated Antimicrobial DressingReduces Hospital Length of
Stay for Pediatric Burn Patients. J Burn Care Research. May-Jun
2007;28:409-411. [Medline].
11.
Peters DA, Verchere C. Healing at Home: Comparing Cohorts of
Children with Medium-Sized Burns Treatedas Outpatients With
In-Hospital Applied Acticoat (TM) to those Children Treated as
Inpatients with SilverSulfadiazine. J Burn Care Research. Mar-Apr
2006;27:198-201. [Medline].
12.
Sheridan RL, Weber JM, Schnitzer JJ, et al. Young age is not a
predictor of mortality in burns. Pediatr Crit
Care Med. Jul 2001;2(3):223-224. [Medline].
13.
Kraft R, Herndon DN, Al-Mousawi AM, Williams FN, Finnerty CC,
Jeschke MG. Burn size and survivalprobability in paediatric
patients in modern burn care: a prospective observational cohort
study. Lancet. Mar
17 2012;379(9820):1013-21. [Medline].
14.
Surgical Treatment of Burns
http://emedicine.medscape.com/article/934173-overview
5 of 5 8/8/2012 3:18 PM
Generated by Foxit PDF Creator Foxit
Softwarehttp://www.foxitsoftware.com For evaluation only.
-
Generated by Foxit PDF Creator Foxit
Softwarehttp://www.foxitsoftware.com For evaluation only.
-
Generated by Foxit PDF Creator Foxit
Softwarehttp://www.foxitsoftware.com For evaluation only.
-
Surgical Treatment of Burns Treatment & Management
Author: Gail E Besner, MD; Chief Editor: Harsh Grewal, MD, FACS,
FAAP more...
Updated: Apr 2, 2012
Medical Therapy
Rapid assessment and treatment of immediate life-threatening
conditions is mandatory in patients with burns.Endotracheal
intubation is indicated in children with respiratory distress or
airway compromise caused by airwayedema. Because of the small
diameter of the pediatric airway, a low threshold for intubation
should be maintained.Children with burns affecting more than 10% of
the body surface area (BSA) should receive intravenous
fluidresuscitation. Burn wounds should initially be covered with
dry sterile sheets, and a thorough history and physicalexamination
should be obtained. Wet sheets or cooling packs should not be used
because this contributes tohypothermia. Patients should be kept
warm by infusing warm intravenous fluids, elevating room
temperatures, andminimizing patient exposure. Tetanus immunization
should be administered as indicated.
Admission criteria
Hospital admission criteria for patients with thermal injury
include the following:
Partial-thickness burns greater than 10% total BSA
(TBSA)Full-thickness burns greater than 2% TBSABurns involving the
face, hands, genitalia, perineum, or major jointsCircumferential
extremity burnsAll high-voltage electrical burns, including
lightning injuryAdmission of low-voltage electrical burns is
selectiveChemical burnsInhalation injuryBurn injuries in patients
with preexisting medical disorders that could complicate
management, prolongrecovery, or affect mortality (eg, diabetes,
immunosuppression)Suspected child abuseCases in which it is
determined that it is in the best interest to admit the child (ie,
parental inability to care for theburn)
Inhalation injury
Clues to inhalation injury include increased respiratory rate,
hoarseness, being burned in an enclosed space, alteredmental
status, head and neck burns, singed nasal hairs, inflamed oral
mucosa, and carbonaceous sputum. Indicationsfor intubation include
compromised upper airway patency, the need for ventilatory support
as manifested by poor gasexchange or increased work of breathing,
or compromised mental status. Correlation of the history and
clinical findingscomprise the most practical approach to
determining the need for intubation.
Important considerations regarding the pediatric airway include
the fact that the larynx is more cephalad in children, thatchildren
deteriorate faster than adults in terms of upper airway edema and
alveolar-capillary block, and that repeatedintubation attempts may
cause edema and obstruction. For these important reasons,
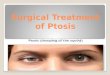
experience in pediatric intubationis needed. Once an airway is
established, securing the airway well is important, especially in
patients with facial burns,to avoid accidental extubation (see the
image below).
Medscape ReferenceReference
News
Reference
Education
MEDLINE
Surgical Treatment of Burns Treatment & Management
http://emedicine.medscape.com/article/934173-treatment
1 of 7 8/8/2012 3:43 PM
Generated by Foxit PDF Creator Foxit
Softwarehttp://www.foxitsoftware.com For evaluation only.
-
Endotracheal tube immobilization in children. The figure
demonstrates a method using umbilical tape to secure a pediatric
endotrachealtube in patients with facial burns.
Carbon monoxide (CO) toxicity is the leading cause of death in
patients with inhalation injury. CO is a byproduct ofcombustion
that displaces O2 from the hemoglobin (Hgb) molecule. It has 250X
the affinity of O2 for Hgb, therefore
shifting the Hgb-O2 disassociation curve to the left. This
impairs O2 unloading at the tissue level and causes a switch to
anaerobic metabolism with severe metabolic acidosis. CO toxicity
should be suspected with persistent metabolicacidosis despite
adequate volume resuscitation. Remember that the PaO2 in an
arterial blood gas will be normal since
the amount of O2 dissolved in arterial plasma is normal. In
addition, the O2 sat (measured O2 saturation of Hgb) will be
normal on a standard pulse oximeter in the presence of CO
toxicity since the oximeter cannot differentiate betweenHgb
saturated with O2 and Hgb saturated with CO.
To treat CO toxicity, all patients with inhalation injury should
be treated with 100% O2. This lowers the T of CO to
30-90 minutes whereas it would be 4-5 hours in room air.
Therefore, all major burns should be treated with 100% O2until CO
toxicity is ruled out or the CO level returns to normal. Hyperbaric
oxygen (HBO) therapy (3 atm) leads to evenmore rapid displacement
of CO within 20 minutes. Its use should be considered for CO
greater than 50%, severeneurologic compromise, and
nonresponsiveness to 100% O2.
Cyanide toxicity results from the burning of natural (wool,
silk, cotton, paper) or synthetic (polyurethane, plastic,
nylon,acrylic) products, which leads to the production of toxic
hydrocyanide gas. Cyanide binds to the cytochrome oxidasesystem,
inhibiting cellular metabolism and ATP production. It causes a
shift to anaerobic metabolism with profoundmetabolic acidosis and
obtundation. The treatment of cyanide toxicity involves
administration of the cyanide antidotesodium thiosulfate (8 g
intravenously if < 12 y; 12.5 g intravenously if 12 y). The
antidote converts cyanide tonontoxic, excretable thiocyanate.
Smoke inhalation can also cause a chemically induced
inflammatory reaction in the airways, leading to
microbialcolonization and pneumonia. Affected patients may need
ventilatory support. In severe cases, oscillating ventilatorsand
extracorporeal membrane oxygenation (ECMO) have been successfully
used in these patients.
Fluid resuscitation
Intravenous access may be obtained percutaneously or by cutdown,
either peripherally or centrally. Peripheral accessin an unburned
area is preferred. Intraosseous (IO) infusion may be lifesaving in
the severely burned patient ifnecessary.
Several burn resuscitation formulas can be used in pediatric
burn care; the modified Parkland formula is mostcommonly used.
Ringer lactate solution is initially used in pediatric patients of
all ages at 3-4 mL/kg for each percent ofBSA burned for the first
24 hours. One half of the calculated fluid needs are administered
in the first 8 hours after theburn occurs, and the remaining half
are administered over the following 16 hours. Maintenance fluids
should beadministered concomitantly (this represents the
modification to the Parkland formula for pediatric patients).
Representative fluid resuscitation guidelines for pediatric burn
patients with burns more than 15% TBSA are asfollows:
Modified Parkland formula (Parkland formula plus maintenance
fluids, used in patients who weigh less than 20kg)Resuscitation
fluids - 3-4 mL Ringer lactate X weight (kg) X %TBSA burned
(second-degree and third degree);half administered over the first 8
hours (from time of injury), remaining half administered over the
next 16 hoursMaintenance fluids - Ringer lactate solution with 5%
dextrose at 4 mL/kg/h for 0-10 kg, plus 2 mL/kg/h for 10-20kg, plus
1 mL/kg/h for each kg more than 20 kg
Prehospital fluids must also be considered. If prehospital fluid
resuscitation is inadequate, the fluid deficit must beadded to the
fluid rate calculated for the first 8 hours of resuscitation.
For patients with burns of 15% TBSA or less, the following are
indicated:
Patients with burns 5-10% TBSA who are taking oral fluids well -
Oral fluids onlyPatients with burns 5-10% TBSA who are not taking
oral fluids well - Maintenance fluidsPatients with burns 10-15%
TBSA - 150% maintenance fluids
The above recommendations are guidelines only. Patients with
burns of more than 15% TBSA should have a urinary
Surgical Treatment of Burns Treatment & Management
http://emedicine.medscape.com/article/934173-treatment
2 of 7 8/8/2012 3:43 PM
Generated by Foxit PDF Creator Foxit
Softwarehttp://www.foxitsoftware.com For evaluation only.
-
catheter placed. Desired urine output is 1 mL/kg/h for patients
who weigh less than 30 kg and 30-50 mL/h for patientswho weigh more
than 30 kg. For major burns, fluid resuscitation needs to be
reassessed hourly based on the patient'surine output.
Rates of fluid administration should be altered based on the
patient's response. If a patient presents after someperiod of delay
and has not been resuscitated properly during that time,
adjustments should be made in the calculatedfluid requirements to
take these factors into account. Infants are at risk of developing
hypoglycemia because of limitedglycogen stores; therefore, glucose
levels should be monitored, and Ringer lactate solution with 5%
dextrose shouldbe used for maintenance fluids. Assess response to
fluid administration by measuring urine output via an
indwellingurinary catheter. Monitoring sensorium, peripheral
circulation, and blood pH is also helpful to assess the adequacy
ofresuscitation.
Temperature regulation
As previously mentioned, children younger than 2 years lose heat
and water more rapidly than older children and adultsbecause of
their thinner layers of skin and insulating subcutaneous tissue;
temperature regulation in these very youngchildren is partially
based on nonshivering thermogenesis, which further increases
metabolic rate, oxygenconsumption, and lactate production.
Therefore, hypothermia in the pediatric burn patients should be
avoided bypaying careful attention to increasing the room
temperature, minimizing exposure time, and using radiant warmers,
fluidwarmers, and other tools.
Systemic antibiotics
Prophylactic systemic antibiotics are not used in the treatment
of burn patients because this increases the risk ofinfection with
resistant organisms. Instead, the use of systemic antibiotics is
reserved for the treatment of specificinfections, with antibiotics
administered at the first sign of clinical infection. Antibiotic
regimens are then modified asculture results and antimicrobial
sensitivity results become available.
Burn wound cellulitis refers to infection spreading in dermal
lymphatics in the nonburned skin surrounding a burn,usually
occurring in the first few days after burn injury. Burn cellulitis
is commonly caused by Streptococcus pyogenes.
Invasive burn wound sepsis leads to systemic toxicity with high
fever, bacteremia, and a hyperdynamic circulatory statewith
hypotension and cardiovascular collapse. Diagnosis can be made by
either clinical examination, or by quantitativeburn wound cultures
or burn wound histology.
Surgical Therapy
Devitalized skin and ruptured blisters should be debrided.
Topical antibiotic therapy should be used to delay
bacterialcolonization. Silver sulfadiazine cream (Silvadene) is a
commonly used broad-spectrum topical antimicrobial cream. Itis
applied as a thin layer with gauze dressings twice daily. It does
cause transient neutropenia, which resolves even
with continued use of the agent.[3] Facial burns are usually
treated with a combination antimicrobial product
containingpolymyxin B, neomycin, and bacitracin (eg, Neosporin
ointment) or an immunomodulating cream such as beta-Glucan(a cream
that contains complex carbohydrate isolated from the cell wall of
oats). The use of silver sulfadiazine creamis avoided on the
central face because it may cause severe ocular irritation. Ear
burns should be treated with mafenidecream (Sulfamylon) because the
thin subcutaneous tissue in the ears predisposes to the development
of chondritis.
Hydrotherapy provides wound and body cleansing with gentle
removal of loose eschar and topical ointments. If used,hydrotherapy
sessions are limited to 10-15 minutes once a day to decrease
promotion of infection. Topical enzymepreparations such as Santyl
(a collagenase-containing debriding ointment) can be applied to the
burn surface tochemically debride devitalized tissue without
injuring viable tissue. This allows earlier assessment of the wound
bed,with fewer days to a clean wound bed and
reepithelialization.
To avoid the need for painful dressing changes, artificial skin
substitutes, such as Aquacel Ag and Acticoat, may beused for the
treatment of partial-thickness burns. Aquacel Ag is a hydrofiber
dressing in which antibacterial silver (Ag+)ions are incorporated
into the dressing and released in a continuous sustained-release
fashion for continuous topicalantimicrobial effects. The fibers in
the dressing hydrate upon contact with the burn surface creating a
viscous gel thatprevents fluid loss and traps bacteria. Once
adherent to the burn surface, usually within 24-48 hours, the
dressing canbe left in place for as long as 2 weeks, during which
time reepithelialization is usually complete. If
reepithelialization isnot complete by that time, the Aquacel Ag can
be reapplied (see the image below).
Surgical Treatment of Burns Treatment & Management
http://emedicine.medscape.com/article/934173-treatment
3 of 7 8/8/2012 3:43 PM
Generated by Foxit PDF Creator Foxit
Softwarehttp://www.foxitsoftware.com For evaluation only.
-
Aquacel Ag adherent to burn wounds.
Preoperative Details
Successful burn wound management in children demands conversion
of open wounds to closed wounds as soon aspossible. The concept of
early removal of burn eschar and immediate wound closure has gained
widespreadacceptance. Evidence suggests that early eschar removal
is effective in decreasing morbidity and improving themortality
rate. Full-thickness burns (with the exception of very small
injuries that are allowed to heal by contraction)should be grafted.
The goal is to excise the wound within the first week of the
injury. Additionally, deep partial-thicknessburns that take longer
than 3 weeks to heal usually benefit from grafting, with less
hypertrophic scarring and bettercosmetic results.
Intraoperative Details
Preoperatively, patients must be hemodynamically sound and have
optimal acid-base, fluid, and electrolyte balance.Adequate blood
must be available before considering excision and grafting.
Preoperative antibiotics are not requiredunless patients have other
compromising systemic diseases or invasive burn sepsis; however, a
prophylactic dose ofa first-generation cephalosporin antibiotic may
be used.
Attention to maintenance of body temperature at all times is
extremely important. Burn excision involves tangentialremoval of
thin slices of eschar until profuse pinpoint bleeding from a moist,
viable, deep dermal surface orsubcutaneous fat is observed.
Meticulous hemostasis is then obtained using epinephrine-soaked
(1:100,000)sponges, topical spray thrombin, and electrocautery,
followed by immediate grafting with thin sheets of autograft.
Skingrafting involves harvesting partial-thickness pieces of skin
from donor sites on unburned areas using a dermatome.The thickness
of the harvested skin commonly is 8-12 thousandths of an inch,
depending on the age and skinthickness of the patient. The grafts
are then applied to the wound bed and secured.
Autograft skin is obviously preferred whenever possible.
Unfortunately, patients with large burns may not have
enoughautologous skin available for complete coverage. In such
patients, burns can be excised and temporarily covered withnumerous
biologic dressings (eg, cadaveric skin, pigskin) or skin
substitutes. As more donor sites become available,the temporary
wound covers are removed and the wounds are grafted. Studies have
shown that growth hormone(0.15-0.2 mg/kg/d intramuscularly) can
speed donor site healing, allowing more rapid reharvesting of
healed donor
sites.[4, 5]
Meshed autografts are harvested from donor sites and passed
through a meshing machine that cuts a series ofparallel offset
slits in the grafts at various expansion ratios (eg, 1.5:1, 2:1).
This technique allows expansion of the graftto cover a larger
surface area. In addition, the interstices in the graft allow for
drainage of fluids under the graft so thatthe grafts do not lift
off their beds. Unfortunately, the meshed patterns of the grafts
persist after healing and often leadto suboptimal cosmetic
results.
Nonmeshed or sheet grafts are harvested the same way but are not
passed through the meshing machine. The use ofsheet grafts leads to
a better cosmetic result. Because the grafts do not expand,
covering major areas with sheetgrafts alone is difficult.
Nonetheless, sheet grafts should be used whenever possible,
especially in highly visible andfunctional areas, such as the face,
neck, hands, and joints. Sheet grafts should be inspected after
approximately 48hours so that any underlying fluid can be aspirated
to avoid loss of the graft. Dressings can be left in place for as
longas 5 days if desired on meshed grafts, as long as no suspicion
of infection is noted.
Follow-up
Avoidance of scarring and contracture is the best treatment.
Scar prevention
For burns that take longer than 3 weeks to heal, or for wounds
that have been grafted, hypertrophic scarring can beminimized with
the use of compression therapy with custom-made garments that apply
25-30 mm Hg pressure to allwounds. Gel pads can be added underneath
or sewn into the garments to apply extra compression.
Compressiontherapy is continued throughout the wound healing
process (approximately 12-18 months). Lotion application
withmassage therapy is used to keep the healed or grafted areas
soft and supple.
Contracture prevention
Contractures refer to hypertrophic scar formation over joints
that result in decreased range of motion. Aggressiveattention to
occupational and physical therapy, with appropriate consultation,
is necessary to ensure optimal results.
Surgical Treatment of Burns Treatment & Management
http://emedicine.medscape.com/article/934173-treatment
4 of 7 8/8/2012 3:43 PM
Generated by Foxit PDF Creator Foxit
Softwarehttp://www.foxitsoftware.com For evaluation only.
-
Active and passive range of motion exercises are instituted and
splints are worn at night and between exerciseperiods. Patients
with burns are at risk for contractures are followed for years to
monitor for the development of thesecomplications.
Psychological sequelae
Burn scarring can lead to significant psychological sequelae and
the assistance of a trained psychologist orpsychiatrist can be an
important addition to the overall care of these patients.
Patient education
For excellent patient education resources, visit eMedicine's
Burns Center. Also, see eMedicine's patient educationarticle
Thermal (Heat or Fire) Burns.
Complications
Complications to surgery in patients with burns include
bleeding, infection, or graft loss. If infection is
suspected,dressings can be changed to include broad spectrum
aqueous Sulfamylon solution.
Outcome and Prognosis
With the exception of infants, the prognosis for survival in
children and adolescents is quite good. In the past decade,the size
of a survivable injury has increased from 70% BSA burned to more
than 95% BSA burned in children youngerthan 15 years.
A large, single-center study of pediatric burn patients analyzed
the relationship between burn size and probability ofsurvival. A
cohort of 952 severely burned patients of comparable age and sex
distribution were studied. Resultssuggest that a burn size of
roughly 60% BSA is a crucial threshold for postburn morbidity and
mortality. Child burnvictims with greater than 60% BSA burns should
be immediately transferred to a specialized burn center to combat
the
increased risk of poor outcome associated with this burn
size.[14]
Future and Controversies
Numerous areas in both the clinical and basic sciences are
undergoing active research. One such area of interest isthe
hypermetabolic response to severe burns and the association with
increased energy expenditure and muscle-protein catabolism. Studies
have investigated different mechanisms to attenuate the
muscle-protein catabolism that
occurs frequently, despite appropriate nutritional support, in
children with large burns.[6] These studies are promisingbecause
attenuation of muscle-protein losses may improve strength and
ability to recuperate.
A prospective randomized controlled trial of recombinant human
growth hormone in combination with the beta-blockerpropanolol
demonstrated attenuated hypermetabolism and inflammatory and acute
phase responses after severe burn
injury.[4] Human growth hormone improves posttraumatic
hypermetabolism, but its use alone is associated withhyperglycemia
and increased free fatty acids and triglycerides. Concomitant
administration of propanolol improved fatmetabolism and insulin
sensitivity and avoided the adverse effects of recombinant growth
hormone alone.
Another active area of research is in the development of
cultured skin to treat very large burns. At present,
culturedepidermal autografts (CEAs), which are grown from the
patient's own uninjured epidermis, are commonly used.However, these
grafts are very thin and fragile. In the future, cultured bilayered
skin (epidermis and dermis) shouldlead to better functional and
cosmetic results.
Contributor Information and DisclosuresAuthorGail E Besner, MD
John E Fisher Endowed Chair in Neonatal Reseach, Director,
Pediatric Surgical Research,Department of Surgery, Nationwide
Children's Hospital; Professor of Surgery and Pediatrics,
Department ofSurgery, Ohio State University College of Medicine
Gail E Besner, MD is a member of the following medical
societies: Alpha Omega Alpha, American Academy ofPediatrics,
American Burn Association, American College of Surgeons, American
Gastroenterological Association,American Medical Association,
American Medical Women's Association, American Pediatric Surgical
Association,Association for Academic Surgery, Federation of
American Societies for Experimental Biology, Society of
CriticalCare Medicine, Society of Surgical Oncology, and Society of
University Surgeons
Disclosure: Nothing to disclose.
Surgical Treatment of Burns Treatment & Management
http://emedicine.medscape.com/article/934173-treatment
5 of 7 8/8/2012 3:43 PM
Generated by Foxit PDF Creator Foxit
Softwarehttp://www.foxitsoftware.com For evaluation only.
-
Coauthor(s)Iyore Amy Otabor, MD Clinical Instructor House Staff,
Department of General Surgery, The Ohio State UniversityCollege of
Medicine
Iyore Amy Otabor, MD is a member of the following medical
societies: American College of Surgeons, AmericanMedical Student
Association/Foundation, and Student National Medical
Association
Disclosure: Nothing to disclose.
Specialty Editor BoardDenis Bensard, MD Director of Pediatric
Surgery and Trauma, Attending Adult and Pediatric Acute Care
Surgery,Attending Adult and Pediatric Surgical Critical Care,
Denver Health Medical Center; Professor of Surgery, Universityof
Colorado School of Medicine
Denis Bensard, MD is a member of the following medical
societies: Alpha Omega Alpha, American Academy ofPediatrics,
American College of Surgeons, American Pediatric Surgical
Association, Association for AcademicSurgery, International Society
for Minimally Invasive Cardiac Surgery, Society of American
Gastrointestinal andEndoscopic Surgeons, Society of
Laparoendoscopic Surgeons, Society of University Surgeons, and
SouthwesternSurgical Congress
Disclosure: Nothing to disclose.
Mary L Windle, PharmD Adjunct Associate Professor, University of
Nebraska Medical Center College ofPharmacy; Editor-in-Chief,
Medscape Drug Reference
Disclosure: Nothing to disclose.
Michael G Caty, MD Professor of Surgery and Pediatrics, State
University of New York at Buffalo; ConsultingStaff, Department of
Pediatric Surgery, Children's Hospital of Buffalo
Michael G Caty, MD is a member of the following medical
societies: American Academy of Pediatrics, AmericanCollege of
Physician Executives, American College of Surgeons, American
Medical Association, AmericanPediatric Surgical Association,
Association for Academic Surgery, and Association for Surgical
Education
Disclosure: Nothing to disclose.
H Biemann Othersen Jr, MD Professor of Surgery and Pediatrics,
Emeritus Head, Division of Pediatric Surgery,Medical University of
South Carolina
H Biemann Othersen Jr, MD is a member of the following medical
societies: Alpha Omega Alpha, AmericanAcademy of Pediatrics,
American Association for the Surgery of Trauma, American Burn
Association, AmericanCancer Society, American College of Surgeons,
American Medical Association, American Pediatric
SurgicalAssociation, American Society for Parenteral and Enteral
Nutrition, American Surgical Association, AmericanThoracic Society,
British Association of Paediatric Surgeons, Society for Surgery of
the Alimentary Tract, Society ofCritical Care Medicine, South
Carolina Medical Association, Southeastern Surgical Congress,
Southern MedicalAssociation, Southern Society for Pediatric
Research, and Southern Thoracic Surgical Association
Disclosure: Nothing to disclose.
Chief EditorHarsh Grewal, MD, FACS, FAAP Clinical Professor of
Surgery, Temple University School of Medicine; Chief,Division of
Pediatric Surgery, Cooper University Hospital
Harsh Grewal, MD, FACS, FAAP is a member of the following
medical societies: American Academy of Pediatrics,American College
of Surgeons, American Pediatric Surgical Association, Association
for Surgical Education,Children's Oncology Group, Eastern
Association for the Surgery of Trauma, International Pediatric
EndosurgeryGroup, Society of American Gastrointestinal and
Endoscopic Surgeons, Society of Laparoendoscopic Surgeons,and
Southwestern Surgical Congress
Disclosure: Nothing to disclose.
References
Lowell G, Quinlan K, Gottlieb LJ. Preventing unintentional scald
burns: moving beyond tap water. Pediatrics.
Oct 2008;122(4):799-804. [Medline].
1.
O'Neill TB, Rawlins J, Rea S, Wood F. Complex chemical burns
following a mass casualty chemical plant2.
Surgical Treatment of Burns Treatment & Management
http://emedicine.medscape.com/article/934173-treatment
6 of 7 8/8/2012 3:43 PM
Generated by Foxit PDF Creator Foxit
Softwarehttp://www.foxitsoftware.com For evaluation only.
-
Medscape Reference 2011 WebMD, LLC
incident: How optimal planning and organisation can make a
difference. Burns. Feb 20 2012;[Medline].
Gupta SS, Singh O, Bhagel PS, Moses S, Shukla S, Mathur RK.
Honey dressing versus silver sulfadiazenedressing for wound healing
in burn patients: a retrospective study. J Cutan Aesthet Surg.
Sep
2011;4(3):183-7. [Medline]. [Full Text].
3.
Jeschke MG, Finnerty CC, Kulp GA, Przkora R, Micak RP, Herndon
DN. Combination of recombinant humangrowth hormone and propanol
decreases hypermetabolism and inflammation in severely burned
children.Pediatr Crit Care Med. Mar 2008;9:209-216. [Medline].
4.
Coruh A, Yontar Y. Application of Split-Thickness Dermal Grafts
in Deep Partial- and Full-Thickness Burns: ANew Source of Auto-Skin
Grafting. J Burn Care Res. Nov 10 2011;[Medline].
5.
Chan MM, Chan GM. Nutritional therapy for burns in children and
adults. Nutrition. Mar 2009;25(3):261-9.
[Medline].
6.
Besner GE. Burns. In: Glick PL, Pearl RH, Irish MS, et al, eds.
Pediatric Surgery Secrets. ed. Philadelphia,
PA: Hanley & Belfus; 2000:246-52.
7.
Heimbach D. What's new in general surgery: burns and metabolism.
J Am Coll Surg. Feb
2002;194(2):156-64. [Medline].
8.
Herndon DN, Hart DW, Wolf SE, et al. Reversal of catabolism by
beta-blockade after severe burns. N Engl J
Med. Oct 25 2001;345(17):1223-9. [Medline].
9.
Hildreth M, Gottschlich M. Nutritional support of the burned
patient. In: Herndon D, ed. Total Burn Care.
Philadelphia, PA: WB Saunders Co; 1996:237-45.
10.
Paddock HN, Fabia R, Giles S, Hayes J, Lowell W, Besner G. A
Silver Impregnated Antimicrobial DressingReduces Hospital Length of
Stay for Pediatric Burn Patients. J Burn Care Research. May-Jun
2007;28:409-411. [Medline].
11.
Peters DA, Verchere C. Healing at Home: Comparing Cohorts of
Children with Medium-Sized Burns Treatedas Outpatients With
In-Hospital Applied Acticoat (TM) to those Children Treated as
Inpatients with SilverSulfadiazine. J Burn Care Research. Mar-Apr
2006;27:198-201. [Medline].
12.
Sheridan RL, Weber JM, Schnitzer JJ, et al. Young age is not a
predictor of mortality in burns. Pediatr Crit
Care Med. Jul 2001;2(3):223-224. [Medline].
13.
Kraft R, Herndon DN, Al-Mousawi AM, Williams FN, Finnerty CC,
Jeschke MG. Burn size and survivalprobability in paediatric
patients in modern burn care: a prospective observational cohort
study. Lancet. Mar
17 2012;379(9820):1013-21. [Medline].
14.
Surgical Treatment of Burns Treatment & Management
http://emedicine.medscape.com/article/934173-treatment
7 of 7 8/8/2012 3:43 PM
Generated by Foxit PDF Creator Foxit
Softwarehttp://www.foxitsoftware.com For evaluation only.
-
Emergency Escharotomy
Author: Neelu Pal, MD; Chief Editor: Erik D Schraga, MD
more...
Updated: Dec 13, 2011
Overview
Full-thickness circumferential and near-circumferential skin
burns result in the formation of a tough, inelastic mass ofburnt
tissue (eschar). The eschar, by virtue of this inelasticity,
results in the burn-induced compartment syndrome. Thisis caused by
the accumulation of extracellular and extravascular fluid within
confined anatomic spaces of theextremities or digits. The excessive
fluid causes the intracompartmental pressures to increase,
resulting in collapse ofthe contained vascular and lymphatic
structures and, hence, loss of tissue viability. The capillary
closure pressure of30 mm Hg, also measured as the compartment
pressure, is accepted as that which requires intervention to
preventtissue death.
The circumferential eschar over the torso can lead to
significant compromise of chest wall excursions and can
hinderventilation. Abdominal compartment syndrome with visceral
hypoperfusion is associated with severe burns of theabdomen and
torso. Similarly, airway patency and venous return may be
compromised by circumferential burnsinvolving the neck.
Escharotomy is the surgical division of the nonviable eschar,
which allows the cutaneous envelope to become morecompliant. Hence,
the underlying tissues have an increased available volume to expand
into, preventing further tissueinjury or functional compromise (see
image below). For more information on burn treatment, see eMedicine
articleBurns, Rehabilitation and Reconstruction.
Escharotomy to release the chest wall and allow for ventilation
of the patient.
Escharotomy is considered an emergent procedure in burn
treatment protocols. However, it rarely needs to beperformed in the
emergency department at the time of initial presentation of the
severely burned patient. Advancedventilation methods allow the
patient to be stabilized to allow for expeditious transfer to the
intensive care unit or the
surgical suite, where the procedure can be performed under more
controlled circumstances.[1, 2] For more information,see eMedicine
article Burns, Resuscitation and Early Management.
Indications
Indications for emergency escharotomy are the presence of a
circumferential eschar with one of the following:
Medscape ReferenceReference
News
Reference
Education
MEDLINE
Emergency Escharotomy
http://emedicine.medscape.com/article/80583-overview
1 of 5 8/8/2012 3:16 PM
Generated by Foxit PDF Creator Foxit
Softwarehttp://www.foxitsoftware.com For evaluation only.
-
Impending or established vascular compromise of the extremities
or digits1.
Impending or established respiratory compromise due to
circumferential torso burns[3]2.
Severely burned extremities should be elevated and range of
motion exercises performed every 15-30 minutes astolerated by the
patient. This can help to minimize tissue edema and elevated tissue
pressures.
Neurovascular integrity should similarly be monitored frequently
and in a scheduled manner. Capillary refilling time,
Doppler signals, pulse oximetry, and sensation distal to the
burned area should be checked every hour.[4] Limb deepcompartment
pressures should be checked initially to establish a baseline.
Subsequently, any increase in capillary refilltime, decrease in
Doppler signal, or change in sensation should lead to rechecking
the compartment pressures.Compartment pressures greater than 30 mm
Hg should be treated by immediate decompression via escharotomy
and
fasciotomy, if needed.[5, 6] A decision-making algorithm is
shown in the image below.
Decision-making algorithm for escharotomy in severely burned
extremities.
Contraindications
Patients who have established irreversible gangrene of the
extremity or digit in association with a circumferential
ornear-circumferential eschar would not likely benefit from an
escharotomy. This scenario is likely to be encountered inpatients
who have been managed nonoperatively for a prolonged period of
time, during which the neurovascular statusof the extremity
involved was not monitored adequately. In this group of patients,
the risks and potential complicationsof performing an escharotomy
are to be weighed carefully against the benefits.
Anesthesia
In the severely burned patient who is obtunded and intubated, no
anesthesia is required because the eschar is
nonviable tissue with complete destruction of nerve
endings.[7]
Patients who are awake or conscious require sedation and,
occasionally, general anesthesia, to allow theprocedure to be
completed adequately. For more information, see Procedural
Sedation.
Equipment
Sterile drapesPovidone-iodine solutionElectrocautery:
Escharotomy can result in substantial blood loss; hence, it should
be performed usingelectrocautery and in a controlled environment
such as the operating room or the intensive care unit.Dressing
materials
Positioning
Position the patient supine.Maintain the ability to move the
patient into lateral positions to allow circumferential access to
the extremity ortorso, as needed.
Technique
Clean the proposed surgical site with povidone-iodine solution
and drape with sterile drapes.Use electrocautery to create
incisions in the eschar up to the level of the subcutaneous
fat.Severely burned limbs may require performance of fasciotomy
concomitantly with the escharotomy.
This may be determined preoperatively by measurement of
compartment pressures greater than 30
Emergency Escharotomy
http://emedicine.medscape.com/article/80583-overview
2 of 5 8/8/2012 3:16 PM
Generated by Foxit PDF Creator Foxit
Softwarehttp://www.foxitsoftware.com For evaluation only.
-
mm Hg.Compartment pressures can be obtained intraoperatively
after completion of the escharotomy. Ifelevation of pressure above
30 mm Hg is persistent, a fasciotomy should be performed.
Carry the incision of the eschar down through to the level of
the subcutaneous fat. An immediate release intissue pressure is
experienced as a discernible popping sensation.Carry the incisions
approximately 1 cm proximal and distal to the extent of the
burn.Areas overlying joints have densely adherent skin, and the
incisions should extend across joints to allow fordecompression of
neurovascular structures. Take care to avoid damage to the
neurovascular bundles that run
superficially and near joints.[5]
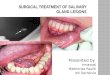
Make escharotomy incisions for the chest, neck, and limbs as
shown in the diagram below.
Diagrammatic representation of escharotomy incisions over the
chest, neck, and limbs.
Make escharotomy incisions for the digits as shown in the
diagram below.
Diagrammatic representation of escharotomy incisions over the
digits.
Bleeding from escharotomy incisions should be controlled by use
of the electrocautery.The resulting wounds are a potential source
of infection and should be treated, as the burn wound,
withapplication of topical antimicrobial and dressings.Adequacy of
the escharotomy can be tested after completion by checking
capillary filling pressures, using a
handheld Doppler, and by checking compartment pressures.[8]
Improvement in flow and decrease in compartment pressures
indicate that the procedure is adequate.Persistent low Doppler
signals or elevated compartment pressures indicate inadequate
release oftissue pressure and a need for additional escharotomy
incisions and, possibly, the addition offasciotomy.
Pearls
Escharotomy incisions for the limbs should be carried to the
level of the thenar and hypothenar eminences forthe upper extremity
and to the level of the great toe medially and the little toe
laterally for the lower extremity.Limb escharotomy incisions run in
close proximity to superficial veins, and these veins should be
identified andpreserved, if possible. If the escharotomy incision
transects these veins, adequate hemostasis should beensured using
electrocautery or ligation.Digital escharotomy should be performed
by a practitioner with experience in hand surgery for burns
wheneverpossible. The locations of the incisions for decompression
are near the digital neurovascular bundles, andinjury to these can
lead to profound and permanent loss of function.
Complications
Complications of inadequate decompression[9] or of not
performing an escharotomy when indicated are severe.[10]
Emergency Escharotomy
http://emedicine.medscape.com/article/80583-overview
3 of 5 8/8/2012 3:16 PM
Generated by Foxit PDF Creator Foxit
Softwarehttp://www.foxitsoftware.com For evaluation only.
-
They include the following:
Muscle necrosisNerve injuryGangrene resulting in amputation of
the limb or digitsRespiratory compromise due to inadequate
ventilation as a result of compressive effect of chest and
uppertorso burnsAbdominal compartment syndrome with visceral
hypoperfusion as a result of abdominal wall and upper torso
burns[11]
Systemic complications of inadequate decompression including
myoglobinuria, renal failure, hyperkalemia, andmetabolic
acidosis
Complications of an escharotomy are as follows:
Excessive blood lossInadvertent fasciotomy: This results in
exposure of the underlying viable tissue, which can become
desiccated.Incision/injury to the underlying healthy tissue
including neurovascular structures, especially in the
extremitiesand digitsBacteremia: Underlying tissue may be infected,
and the manipulation can result in bacteremia and septic shock.If
underlying infection is suspected, the escharotomy should be
performed under antibiotic coverage.Infection of the open
escharotomy wounds: These wounds are treated with the same degree
of care (withdressings and application of antimicrobial agents) as
the burns wounds. These wounds also contribute to theongoing
insensate fluid losses in a manner similar to the burns wounds.
Contributor Information and DisclosuresAuthorNeelu Pal, MD
General Surgeon
Neelu Pal, MD is a member of the following medical societies:
American College of Surgeons, American MedicalAssociation, and
Society of American Gastrointestinal and Endoscopic Surgeons
Disclosure: Nothing to disclose.
Specialty Editor BoardMary L Windle, PharmD Adjunct Associate
Professor, University of Nebraska Medical Center College
ofPharmacy; Editor-in-Chief, Medscape Drug Reference
Disclosure: Nothing to disclose.
Chief EditorErik D Schraga, MD Staff Physician, Department of
Emergency Medicine, Mills-Peninsula Emergency MedicalAssociates
Disclosure: Nothing to disclose.
Additional ContributorsThe authors and editors of eMedicine
gratefully acknowledge the assistance of Lars Grimm with the
literature reviewand referencing for this article.
References
Kupas DF, Miller DD. Out-of-hospital chest escharotomy: a case
series and procedure review. Prehosp
Emerg Care. Jul-Sep 2010;14(3):349-54. [Medline].
1.
Emergency Escharotomy
http://emedicine.medscape.com/article/80583-overview
4 of 5 8/8/2012 3:16 PM
Generated by Foxit PDF Creator Foxit
Softwarehttp://www.foxitsoftware.com For evaluation only.
-
Medscape Reference 2011 WebMD, LLC
Rumbach AF, Ward EC, Cornwell PL, Bassett LV, Khan A, Muller MJ.
Incidence and Predictive Factors forDysphagia After Thermal Burn
Injury: A Prospective Cohort Study. J Burn Care Res. Nov
2011;32(6):608-616. [Medline].
2.
Yildiz TS, Agir H, Koyuncu D, Solak M, Toker K. Survival of an
eight-year-old child with a very severehigh-tension electrical burn
injury: a case report. Ulus Travma Acil Cerrahi Derg. Oct
2006;12(4):326-30.
[Medline].
3.
Piccolo NS, Piccolo MS, Piccolo PD, Piccolo-Daher R, Piccolo ND,
Piccolo MT. Escharotomies,fasciotomies and carpal tunnel release in
burn patients--review of the literature and presentation of
analgorithm for surgical decision making. Handchir Mikrochir Plast
Chir. Jun 2007;39(3):161-7. [Medline].
4.
Roberts JR, Hedges JR, et al. Burn care procedures. In: Roberts
JR, ed. Clinical Procedures in Emergency
Medicine. Vol 1. 4th ed. USA: Saunders; 2004:39.
5.
Burd A, Noronha FV, Ahmed K, Chan JY, Ayyappan T, Ying SY, et
al. Decompression not escharotomy inacute burns. Burns. May
2006;32(3):284-92. [Medline].
6.
Feldmann ME, Evans J, O SJ. Early management of the burned
pediatric hand. J Craniofac Surg. Jul
2008;19(4):942-50. [Medline].
7.
Saffle JR, Zeluff GR, Warden GD. Intramuscular pressure in the
burned arm: measurement and response toescharotomy. Am J Surg. Dec
1980;140(6):825-31. [Medline].
8.
Brown RL, Greenhalgh DG, Kagan RJ, Warden GD. The adequacy of
limb escharotomies-fasciotomies afterreferral to a major burn
center. J Trauma. Dec 1994;37(6):916-20. [Medline].
9.
Gravante G, Delogu D, Sconocchia G. "Systemic apoptotic
response" after thermal burns. Apoptosis. Feb
2007;12(2):259-70. [Medline].
10.
Oda J, Ueyama M, Yamashita K, et al. Effects of escharotomy as
abdominal decompression oncardiopulmonary function and visceral
perfusion in abdominal compartment syndrome with burn patients.
J
Trauma. Aug 2005;59(2):369-74. [Medline].
11.
Deitch EA. The management of burns. N Engl J Med. Nov 1
1990;323(18):1249-53. [Medline].12.
Emergency Escharotomy
http://emedicine.medscape.com/article/80583-overview
5 of 5 8/8/2012 3:16 PM
Generated by Foxit PDF Creator Foxit
Softwarehttp://www.foxitsoftware.com For evaluation only.
-
Generated by Foxit PDF Creator Foxit
Softwarehttp://www.foxitsoftware.com For evaluation only.