Embed Size (px)
Citation preview
IBD PEEKC
Anterior CervicalSpacer System
Surgical Technique
IBD PEEKC Cervical Spacer
2
Table of Contents
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Step 1: Exposure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Step 2: Discectomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Step 3: Endplate Preparation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Step 4: Trialing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Step 5: Implant Preparation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Step 6: Implant Insertion and Positioning . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Step 7: Closure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Implants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Instruments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Product Information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13

IBD PEEKC Cervical Spacer
3
This surgical technique guide describes usage of the IBD PEEKC Spacer as an interbody fusion device (IBD) ofthe cervical spine (C2-T1) . The IBD PEEKC Spacers are intended to be used with autogenous or allogenic bone graft .
Introduction
Pre-Operative Planning
It is important to view pre-operative films so that the placement of the incision is accurate . Surgical approach (left or right sided) is determined according to surgeon preference, patient anatomy and patient pathology .
Approach
The instruments can be used in either a left or right sided approach to the cervical spine . Blunt dissection is used to expose the anterior cervical spine and a self-retaining retractor is used to elevate the longus colli muscles and provide optimal visualization and exposure .
Incision
An incision is made at the desired disc level . If possible, a transverse skin incision parallel to the skin creases of the neck is recommended for cosmetic purposes . Otherwise, a vertical midline incision may be used (Figure 1) .
A K-Wire may be used to confirm that the correct level and midline of the disc have been exposed .
Step 1: Exposure
Figure 1 - The patient should be positioned in the supine position with the head stabilized in extension and rotated slightly away from the site of the approach. If possible, a transverse incision, parallel to the skin creases in the neck, is recommended.

IBD PEEKC Cervical Spacer
4
Pre-Operative Planning
An anterior annulotomy is performed and should be wide enough to allow insertion of the implant (Figure 2) . The IBD PEEKC Spacer is offered in 14mm and 16mm medial-lateral widths . It is recommended that the appropriate width be selected based on pre-operative measurements .
Using short rongeurs, pituitaries, curettes and/or kerrisons, a discectomy is subsequently performed until an appropriate amount of the disc material has been removed, the posterior longitudinal ligament is exposed and decompression is achieved .
Distraction may be performed using the Parallel Pin Distractor and Distraction Pins, which are designed to facilitate both a left and right sided approach thanks to a 360° rotation arm . Curettes are used to elevate additional disc material from the endplates, taking care not to damage the lateral annulus .
Step 2: Discectomy
Figure 2
Reliance C Parallel Pin Distractor 48365020
Solis Distraction Pins 874002 & 874009

IBD PEEKC Cervical Spacer
5
Straight and angled curettes or rasps should be translated parallel to the endplates until sufficient decortication is achieved (Figure 3) . The curettes can be used to “feel” the endplates ensuring that no soft tissue remains .
Step 3: Endplate Preparation
Figure 3
Reliance C Rasps483652(04-12)

IBD PEEKC Cervical Spacer
6
To assist in determining the appropriate cage, several different Trials are available in the set . These trials are designed to approximate the overall height, angulation and endplate dimensions of the disc space . Each trial option has a matching cage (Figure 4) .
Step 4: Trialing
Note: The trials measure line to line (e.g., a 6mm trial measures 6mm), but cage sizes are oversized because they do not include the implant teeth that are .5mm on each side (e.g., a 6mm cage measures 7mm including the teeth) (Figure 4).
Height 4, 5, 6, 7, 8, 9, 10, 11, 12mm
Angulation 0°, 4°
Footprint 12 x 14mm, 14 x 16mm
Insert the appropriate trial into the Quick Release Handle and carefully insert into the disc space . The trial should pass into the distracted disc space without excessive force . A mallet can be used to aid insertion or removal of the trial .
Properly sized trials should fit flush within the confines of the anterior cortex, posterior cortex and unconvertebral joints, producing a tight interface with both the superior and inferior endplates . Care should be taken not to use a trial that is too large for the disc space, for this may result in overdistraction .
Note: The IBD PEEKC implant height with teeth is 1mm greater than the trial height.
Figure 4 Trials (4-12mm)See page 11 for reference numbers
ACP 1 Quick Release Handle48805080

IBD PEEKC Cervical Spacer
7
The IBD PEEKC Spacers areprovided sterile in Ascential’s proprietary Advanced Inventory Management (AIM) packaging (Figure 5) .
Once the appropriate spacer size has been identified, select the corresponding IBD PEEKC implant package, remove the spacer from the double blister packs, and place the spacer in the surgical field . The spacer can be assembled to the AVS AS Inserter by positioning the collet tip in the insertion hole with the lever lifted . Subsequent depression of the lever will cause the collet tip to expand, thereby providing a rigid and stable attachment to the spacer .
Note: It is important to regularly lubricate the proximal and distal areas of the AVS AS Inserter with instrument milk (commonly found in hospitals) to prevent the lever and collet tip from binding.
Autogenous or allogenic bone graft material may be packed into the graft chamber of the IBD PEEKC Spacer using an appropriate graft support and graft compactor .
Step 5: Implant Preparation
AVS AS Inserter 48329000
Figure 5 - AIM Packaging

IBD PEEKC Cervical Spacer
8
The IBD PEEKC Spacer is introduced into the disc space, centered at the midline, and tapped into place (Figure 6) . Axial compression to the IBD PEEKC Spacer should then be applied .
There are three vertical tantalum markers embedded in the implant to help visually confirm its position under fluoroscopy (Figure 7) .
Note: The anterior markers are 2.5mm long and are located 2mm from the anterior edge.
The posterior marker is 1mm long and is located 1mm from the posterior edge.
Step 6: Implant Insertion and Positioning
Figure 6
Figure 7
Anterior marker is 2.5mm
Posterior marker is 1mm
Anterior marker is 2.5mm

IBD PEEKC Cervical Spacer
9
The application of supplemental fixation, such as Ascential’s ACP 1 cervical plate system, is recommended (Figure 8) . If ACP 1 is selected for supplemental fixation, please reference the ACP 1 Surgical Technique for full detail of the recommended fixation procedure .
Check the surgical site for any bone fragments or extraneous soft tissue . Once satisfactory decompression is confirmed, the wound should be closed in a routine manner .
Implant Removal
To remove the implant, position the collet tip of the AVS AS Inserter in the insertion hole with the lever lifted . Subsequent depression of the lever will cause the collet tip to expand, thereby providing a rigid and stable attachment to the spacer . With the AVS AS Inserter connected to the implant, gently remove the implant from the disc space .
Note: It is recommended that the Reliance C Parallel Pin Distractor and Solis Distraction Pins be used to distract the disc space before removing the cage.
Step 7: Closure
Figure 8 - Supplemental fixation shown above is from the recommended ACP 1 Anterior Cervical Plating System.
IBD PEEKC Cervical Spacer
10
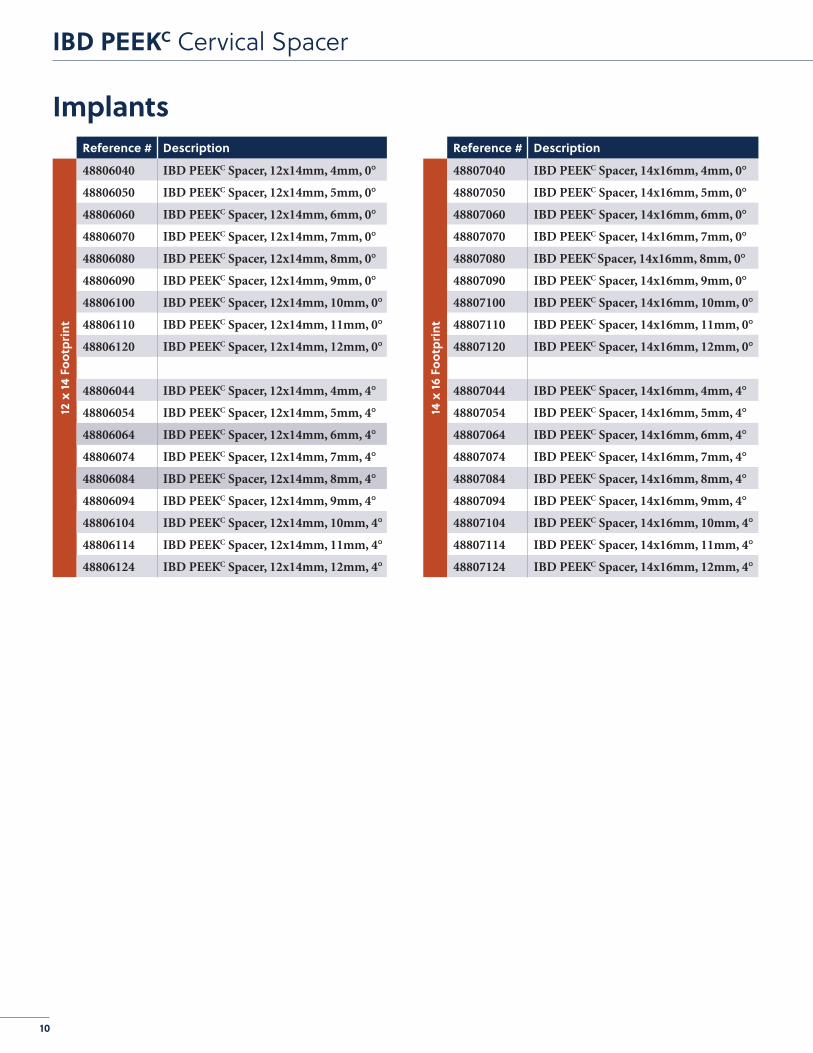
ImplantsReference # Description
12 x
14 F
ootp
rint
48806040 IBD PEEKC Spacer, 12x14mm, 4mm, 0°
48806050 IBD PEEKC Spacer, 12x14mm, 5mm, 0°
48806060 IBD PEEKC Spacer, 12x14mm, 6mm, 0°
48806070 IBD PEEKC Spacer, 12x14mm, 7mm, 0°
48806080 IBD PEEKC Spacer, 12x14mm, 8mm, 0°
48806090 IBD PEEKC Spacer, 12x14mm, 9mm, 0°
48806100 IBD PEEKC Spacer, 12x14mm, 10mm, 0°
48806110 IBD PEEKC Spacer, 12x14mm, 11mm, 0°
48806120 IBD PEEKC Spacer, 12x14mm, 12mm, 0°
48806044 IBD PEEKC Spacer, 12x14mm, 4mm, 4°
48806054 IBD PEEKC Spacer, 12x14mm, 5mm, 4°
48806064 IBD PEEKC Spacer, 12x14mm, 6mm, 4°
48806074 IBD PEEKC Spacer, 12x14mm, 7mm, 4°
48806084 IBD PEEKC Spacer, 12x14mm, 8mm, 4°
48806094 IBD PEEKC Spacer, 12x14mm, 9mm, 4°
48806104 IBD PEEKC Spacer, 12x14mm, 10mm, 4°
48806114 IBD PEEKC Spacer, 12x14mm, 11mm, 4°
48806124 IBD PEEKC Spacer, 12x14mm, 12mm, 4°
Reference # Description
14 x
16 F
ootp
rint
48807040 IBD PEEKC Spacer, 14x16mm, 4mm, 0°
48807050 IBD PEEKC Spacer, 14x16mm, 5mm, 0°
48807060 IBD PEEKC Spacer, 14x16mm, 6mm, 0°
48807070 IBD PEEKC Spacer, 14x16mm, 7mm, 0°
48807080 IBD PEEKC Spacer, 14x16mm, 8mm, 0°
48807090 IBD PEEKC Spacer, 14x16mm, 9mm, 0°
48807100 IBD PEEKC Spacer, 14x16mm, 10mm, 0°
48807110 IBD PEEKC Spacer, 14x16mm, 11mm, 0°
48807120 IBD PEEKC Spacer, 14x16mm, 12mm, 0°
48807044 IBD PEEKC Spacer, 14x16mm, 4mm, 4°
48807054 IBD PEEKC Spacer, 14x16mm, 5mm, 4°
48807064 IBD PEEKC Spacer, 14x16mm, 6mm, 4°
48807074 IBD PEEKC Spacer, 14x16mm, 7mm, 4°
48807084 IBD PEEKC Spacer, 14x16mm, 8mm, 4°
48807094 IBD PEEKC Spacer, 14x16mm, 9mm, 4°
48807104 IBD PEEKC Spacer, 14x16mm, 10mm, 4°
48807114 IBD PEEKC Spacer, 14x16mm, 11mm, 4°
48807124 IBD PEEKC Spacer, 14x16mm, 12mm, 4°
IBD PEEKC Cervical Spacer
11
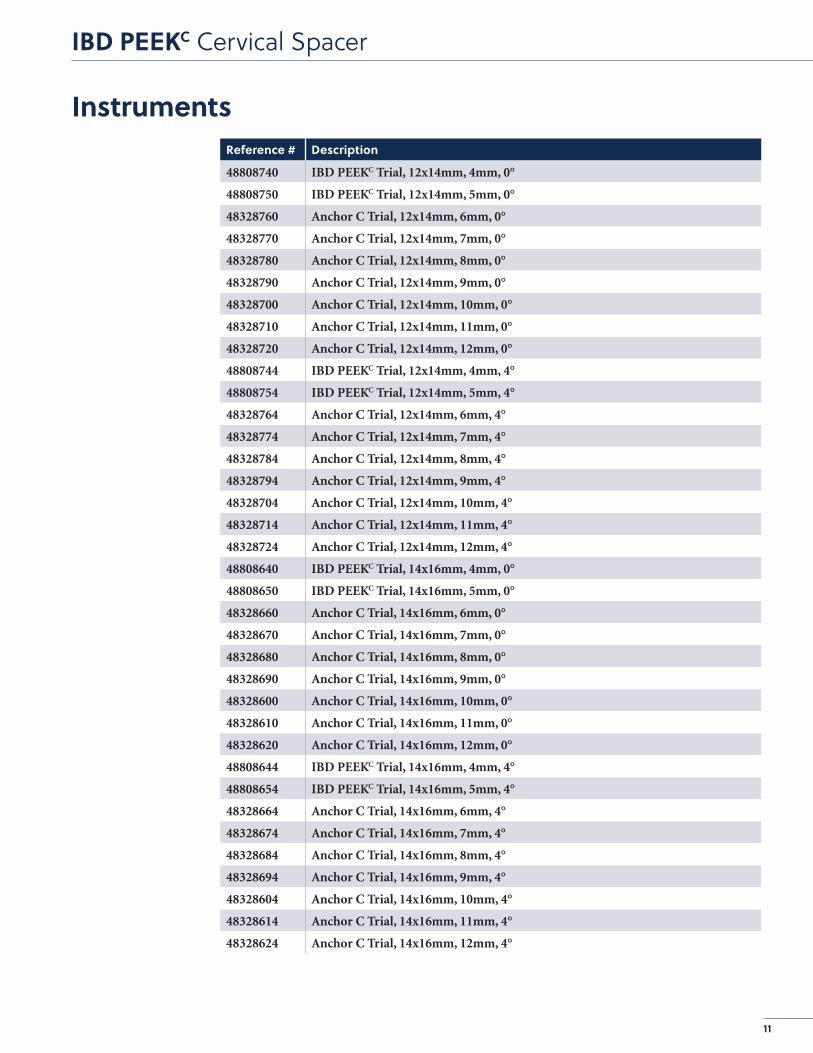
InstrumentsReference # Description
48808740 IBD PEEKC Trial, 12x14mm, 4mm, 0°
48808750 IBD PEEKC Trial, 12x14mm, 5mm, 0°
48328760 Anchor C Trial, 12x14mm, 6mm, 0°
48328770 Anchor C Trial, 12x14mm, 7mm, 0°
48328780 Anchor C Trial, 12x14mm, 8mm, 0°
48328790 Anchor C Trial, 12x14mm, 9mm, 0°
48328700 Anchor C Trial, 12x14mm, 10mm, 0°
48328710 Anchor C Trial, 12x14mm, 11mm, 0°
48328720 Anchor C Trial, 12x14mm, 12mm, 0°
48808744 IBD PEEKC Trial, 12x14mm, 4mm, 4°
48808754 IBD PEEKC Trial, 12x14mm, 5mm, 4°
48328764 Anchor C Trial, 12x14mm, 6mm, 4°
48328774 Anchor C Trial, 12x14mm, 7mm, 4°
48328784 Anchor C Trial, 12x14mm, 8mm, 4°
48328794 Anchor C Trial, 12x14mm, 9mm, 4°
48328704 Anchor C Trial, 12x14mm, 10mm, 4°
48328714 Anchor C Trial, 12x14mm, 11mm, 4°
48328724 Anchor C Trial, 12x14mm, 12mm, 4°
48808640 IBD PEEKC Trial, 14x16mm, 4mm, 0°
48808650 IBD PEEKC Trial, 14x16mm, 5mm, 0°
48328660 Anchor C Trial, 14x16mm, 6mm, 0°
48328670 Anchor C Trial, 14x16mm, 7mm, 0°
48328680 Anchor C Trial, 14x16mm, 8mm, 0°
48328690 Anchor C Trial, 14x16mm, 9mm, 0°
48328600 Anchor C Trial, 14x16mm, 10mm, 0°
48328610 Anchor C Trial, 14x16mm, 11mm, 0°
48328620 Anchor C Trial, 14x16mm, 12mm, 0°
48808644 IBD PEEKC Trial, 14x16mm, 4mm, 4°
48808654 IBD PEEKC Trial, 14x16mm, 5mm, 4°
48328664 Anchor C Trial, 14x16mm, 6mm, 4°
48328674 Anchor C Trial, 14x16mm, 7mm, 4°
48328684 Anchor C Trial, 14x16mm, 8mm, 4°
48328694 Anchor C Trial, 14x16mm, 9mm, 4°
48328604 Anchor C Trial, 14x16mm, 10mm, 4°
48328614 Anchor C Trial, 14x16mm, 11mm, 4°
48328624 Anchor C Trial, 14x16mm, 12mm, 4°

IBD PEEKC Cervical Spacer
12
Reference # Description
48805080 ACP 1 Quick Release Handle
48329000 AVS AS Inserter
48365020 Reliance C Parallel Pin Distractor
48365110 Reliance C Cobb Spinal Elevator
48365204 Reliance C Double Sided Rasp, 4mm
48365205 Reliance C Double Sided Rasp, 5mm
48365206 Reliance C Double Sided Rasp, 6mm
48365207 Reliance C Double Sided Rasp, 7mm
48365208 Reliance C Double Sided Rasp, 8mm
48365209 Reliance C Double Sided Rasp, 9mm
48365210 Reliance C Double Sided Rasp, 10mm
48365211 Reliance C Double Sided Rasp, 11mm
48365212 Reliance C Double Sided Rasp, 12mm
48365320 Reliance C Flat Tamp
48365321 Reliance C Curved Tamp
874002 Solis Distraction Pin, 10mm
874009 Solis Distraction Pin, 15mm
874005 Reliance C Pin Driver
874007 Reliance C Pin Guide
48808200 IBD PEEKC Container Lid
48808200A IBD PEEKC Container Base
48808200B IBD PEEKC Container Instrument Insert
48808200C IBD PEEKC Container Instrument Insert
48808200D IBD PEEKC Container Instrument Insert
48808200E IBD PEEKC Container Instrument Insert
48808200F IBD PEEKC Container Instrument Insert
Instruments

IBD PEEKC Cervical Spacer
13
Product Information for IBD PEEKC SpacerSterile Product
DESCRIPTIONThe Ascential IBD PEEKC Spacer is a hollow, ring-shaped PEEK Optima® LT1 cage with three Tantalum marker pins . The cages are offered in a variety of lengths, heights, and lordotic angles to adapt to varying patient anatomies . The hollow, ring-shaped implants have serrations on the top and bottom surfaces of the cage . The hollow space of the implant is intended to hold bone graft material . The IBD PEEKC Spacer is to be used as an interbody fusion device (IBD) for the cervical spine (from C2-C3 to C7-T1) .
INDICATIONSThe Ascential IBD PEEKC Spacers are indicated for use in cervical interbody fusion procedures in skeletally mature patients with degenerative disc disease (DDD) at one level from the C2-C3 disc to the C7-T1 disc . DDD is defined as back pain of discogenic origin with degeneration of the disc confirmed by history and radiographic studies . The IBD PEEKC Spacers are to be used with autogenous bone graft and/or allogenic bone graft comprised of cancellous and/or corticocancellous bone graft, and implanted via an open, anterior approach .
The Ascential IBD PEEKC Spacer is intended to be used with supplemental fixation systems that have been cleared for use in the cervical spine . This cervical device is to be used in patients who have had six weeks of non-operative treatment .
MATERIALAll components of the system are manufactured out of the following materials:• Polyetheretherketone (PEEK) (ASTM
F2026)• Tantalum (ASTM F560)
GENERAL CONDITIONS OF USEBefore clinical use, the surgeon should thoroughly understand all aspects of the surgical procedure and limitation of the spinal device . Knowledge of surgical techniques, proper reduction, selection and placement of implants, and pre- and post-operative patient management are other considerations essential to a successful surgical outcome . Consult the medical literature for information regarding proper surgical techniques, precautions, and potential adverse effects associated with spinal fixation surgery .
The implantation of the device must be performed only by experienced spinal surgeons having undergone the necessary specific training in the use of such systems
because this is a technically demanding procedure presenting a risk of serious injury to the patient .
CAUTION• Based on the fatigue testing results, the
physician/surgeon should consider the levels of implantation, patient weight, patient activity level, other patient conditions, etc . which may impact on the performance of the system .
• The implantation of the device must be performed only by experienced spinal surgeons with specific training in the use of this device because this is a technically demanding procedure presenting a risk of serious injury to the patient .
• Potential risks identified with the use of this device, which may require additional surgery, include: device component fracture, loss of fixation, pseudoarthrosis (i .e . non-union), fracture of the vertebrae, neurological injury, and vascular or visceral injury .
• Patients with previous spinal surgery at the level(s) to be treated may have different clinical outcomes as compared to those without a previous surgery .
• The device is designed to be used with a supplemental fixation system .
• The IBD PEEKC Spacers have not been evaluated for safety and compatibility in the MR environment . The IBD PEEKC Spacers have not been tested for heating or migration in the MR environment .
• Specialized instruments are provided by STRYKER Spine and must be used to assure accurate implantation of the device . While rare, intraoperative fracture or breakage of instruments can occur, instruments, which have experienced extensive use or extensive force, are more susceptible to fracture depending on the operative precaution, number of procedures, and disposal attention . Instruments must be examined for wear or damage prior to surgery . Instruments for implantation of the IBD PEEKC Spacers are provided non-sterile and cleaned and must be sterilized prior to use .
CONTRA-INDICATIONSContraindications can be relative or absolute . The choice of a particular device must be carefully weighed against the patient’s overall evaluation . Circumstances listed below may reduce the chances of a successful outcome:• The IBD PEEKC Spacer should not be
implanted in patients with an active infection at the operative site .
• The IBD PEEKC Spacers are not intended for use except as indicated .
• Marked local inflammation .
• Any abnormality present which affects the normal process of bone remodeling including, but not limited to, severe osteoporosis involving the spine, bone absorption, osteopenia, primary or metastatic tumors involving the spine, active infection at the site or certain metabolic disorders affecting osteogenesis .
• Any mental or neuromuscular disorder which would create an unacceptable risk of fixation failure or complications in postoperative care .
• Open wounds .• Pregnancy .• Inadequate tissue coverage over the
operative site .• Any neuromuscular deficit which places an
unsafe load level on the device during the healing period .
• Obesity . An overweight or obese patient can produce loads on the spinal system which can lead to failure of the fixation of the device or to failure of the device itself . Obesity is defined according to the W .H .O . standards .
• A condition of senility, mental illness, or substance abuse . These conditions, among others, may cause the patient to ignore certain necessary limitations and precautions in the use of the implant, leading to failure or other complications .
• Foreign body sensitivity . Where material sensitivity is suspected, appropriate tests must be made prior to material selection or implantation .
• Other medical or surgical conditions that could preclude the potential benefit of surgery, such as congenital abnormalities, immunosuppressive disease, elevation of sedimentation rate unexplained by other diseases, elevation of white blood count (WBC), or marked left shift in the WBC differential count, must be carefully analyzed before surgery .
• Prior fusion at the levels to be treated .• Bone stock compromised by disease,
infection or prior implantation which cannot provide adequate support and/or fixation to the devices .
• Rapid joint disease, bone absorption, osteopenia, osteomalacia, and/or osteoporosis . Osteoporosis or osteopenia are relative contraindications, since this condition may limit the degree of obtainable correction and/or the amount of mechanical fixation .
• Anytime implant utilization would interfere with anatomical structures or physiological performance .
These contra-indications can be relative or absolute and must be taken into account by the physician when making his decision . The above list is not exhaustive .

IBD PEEKC Cervical Spacer
14
PRE-OPERATIVE PRECAUTIONSThe surgical indication and the choice of implants must take into account certain important criteria such as:• Patients involved in an occupation or
activity that applies excessive loading upon the implant (e .g ., substantial walking, running, lifting, or muscle strain) may be at increased risk for failure of the fusion and/or the device .
• Surgeons must instruct patients in detail about limitations of the implant, including, but not limited to, the impact of excessive loading through patient weight or activity, and be taught to govern their activities accordingly . The procedure will not restore function to the level expected with a normal, healthy spine, and the patient should not have unrealistic functional expectations .
• A condition of senility, mental illness, chemical dependence or alcoholism . These conditions among others may cause the patients to ignore certain necessary limitations and precautions in the use of the implant, leading to failure and other complications .
• Foreign body sensitivity . Where material sensitivity is suspected appropriate tests should be made prior to material implantation .
• Surgeons must advise such patients who smoke have been shown to have an increased incidence of non-unions . Such patients must be advised of this fact and warned of the potential consequences .
• Care must be taken to protect the components from being marred, nicked, or notched as a result of contact with metal or abrasive objects .
• Patients with previous spinal surgery at the level(s) to be treated may have different clinical outcomes compared to those without a previous surgery .
THE CHOICE OF IMPLANTSThe choice of proper shape, size and design of the implant for each patient is crucial to the success of the surgery . The surgeon is responsible for this choice, which depends on each patient .
Patients who are overweight may be responsible for additional stresses and strains on the device which can speed upimplant fatigue and/or lead to deformation or failure of the implants .
The size and shape of the bone structures determine the size, shape and type of the implants . Once implanted, the implants are subjected to stresses and strains . These repeated stresses on the implants must be taken into consideration by the surgeon at the time of the choice of the implant, during implantation as well as in the postoperativefollow-up period . Indeed, the stresses and
strains on the implants may cause fatigue, fracture or deformation of the implants, before the bone graft has become completely consolidated . This may result in further side effects or necessitate the early removal of the osteosynthesis device .
INTRA-OPERATIVE PRECAUTIONS• The insertion of the implants must be
carried out using instruments designed and provided for this purpose and in accordance with the specific implantation instructions for each implant . Those detailed instructions are provided in the surgical technique brochure supplied by Ascential .
• Discard all damaged or mishandled implants .
• Never reuse an implant, even though it may appear undamaged .
PATIENT CARE FOLLOWING TREATMENTPrior to adequate maturation of the fusion mass, implanted spinal instrumentation may need additional help to accommodate full load bearing . External support may be recommended by the physician from two to four months postoperatively or until x-rays or other procedures confirm adequate maturation of the fusion mass; externalimmobilization by bracing or casting be employed . Surgeons must instruct patients regarding appropriate and restricted activities during consolidation and maturation for the fusion mass in order to prevent placing excessive stress on the implants which may lead to fixation or implant failure and accompanying clinical problems . Surgeons must instruct patients to report any unusual changes of the operative site to his/her physician . The physician must closely monitor the patient if a change at the site has been detected .
ADVERSE EFFECTSThe surgeon should warn the patient of all the potential side effects . They include but are not limited to:• Late bone fusion or no visible fusion mass
and pseudarthrosis;• While the expected life of spinal implant
components is difficult to estimate, it is finite . These components are made of foreign materials which are placed within the body for the potential fusion of the spine and reduction of pain . However, due to the many biological, mechanical and physicochemical factors which affect these devices but cannot be evaluated in vivo, the components cannot be expected to indefinitely withstand the activity level and loads of normal healthy bone;
• Peripheral neuropathies, nerve damage, heterotopic bone formation and neurovascular compromise, including paralysis, loss of bowel or bladder function, or foot-drop may occur .
• Superficial or deep-set infection and inflammatory phenomena;
• Allergic reactions to the implanted materials, although uncommon, can occur;
• Decrease in bone density due to stress shielding;
• Neurological and spinal dura mater lesions from surgical trauma;
• Dural leak requiring surgical repair;• Cessation of growth of the fused portion of
the spine;• Loss of proper spinal curvature, correction,
height and/or reduction;• Delayed Union or Nonunion: Internal
fixation appliances are load sharing devices which are used to obtain alignment until normal healing occurs . In the event that healing is delayed, does not occur, or failure to immobilize the delayed/nonunion results, the implant will be subject to excessive and repeated stresses which can eventually cause loosening, bending or fatigue fracture . The degree or success of union, loads produced by weight bearing, and activity levels will, among other conditions, dictate the longevity of the implant . If a nonunion develops or if the implants loosen, bend or break, the device(s) must be revised or removed immediately before serious injury occurs;
• Pain, discomfort, or abnormal sensations due to the presence of the device;
• Early loosening may result from inadequate initial fixation, latent infection, premature loading of the device or trauma . Late loosening may result from trauma, infection, biological complications or mechanical problems, with the subsequent possibility of bone erosion, or pain;
• Serious complications may occur with any spinal surgery . These complications include, but are not limited to, genitourinary disorders; gastrointestinal disorders; vascular disorders, including thrombus; bronchopulmonary disorders, including emboli; bursitis, hemorrhage, myocardial infarction, infection, paralysis or death .
• Inappropriate or improper surgical placement of this device may cause distraction or stress shielding of the graft or fusion mass . This may contribute to failure of an adequate fusion mass to form .
• Intraoperative fissure, fracture, or perforation of the spine can occur due to implantation of the components . Postoperative fracture of bone graft or the intervertebral body above or below the level of surgery can occur due to trauma, the presence of defects, or poor bone stock .
Adverse effects may necessitate reoperation . The surgeon must warn the patient of these adverse effects as deemednecessary .

IBD PEEKC Cervical Spacer
15
REMOVALIf fusion / bone graft growth occurs, the device will be deeply integrated into the bony tissues . As a result, the IBD PEEKC Spacer is not intended to be removed unless the management of a complication or adverse event requires the removal . Any decision by a physician to remove the device should take into consideration such factors as:• The risk of the patient of the additional
surgical procedure as well as the difficulty of removal .
• Migration of the implant, with subsequent pain and/or neurological, articular or soft tissue lesions
• Pain or abnormal sensations due to the presence of the implants
• Infection or inflammatory reactions• Reduction in bone density due to the
different distribution of mechanical and physiological stresses and strains .
The Spacer Inserter will be used to hold and disengage the device from the vertebrae .

A surgeon must always rely on his or her own professional clinical judgment when deciding whether to use a particular product when treating a particular patient . Stryker does not dispense medical advice and recommends that surgeons be trained in the use of any particular product before using it in surgery .
The information presented is intended to demonstrate the breadth of Stryker product offerings . A surgeon must always refer to the package insert, product label and/or instructions for use before using any Stryker product . Products may not be available in all markets because product availability is subject to the regulatory and/or medical practices in individual markets . Please contact your Stryker representative if you have questions about the availability of Stryker products in your area .
Stryker Corporation or its divisions or other corporate affiliated entities own, use or have applied for the following trademarks or service marks: Ascential, AVS, Reliance, Solis, Stryker . All other trademarks are trademarks of their respective owners or holders .
Not intended for promotional or marketing use outside the United States . IBPKC-ST-1_11163SC/GS 09/16
Copyright © 2016 StrykerPrinted in USA
Stryker Spine2 Pearl Court Allendale, NJ 07401-1677 USAt: 201 749 8000www.stryker.com





























