Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Surgical approaches to jugular foramen schwannomas: An anatomic study
Noritaka Komune, MD, PhD,1,2 Ken Matsushima, MD,1 Toshio Matsushima, MD, PhD,3 Shizuo Komune, MD, PhD,2 Albert L. Rhoton Jr, MD1*
1Department of Neurosurgery, University of Florida, College of Medicine, Gainesville, Florida, 2Department of Otorhinolaryngology Head and Neck Surgery,Kyushu University, Fukuoka, Japan, 3Department of Neurosurgery, Saga University, Saga, Japan.
Accepted 31 May 2015
Published online 4 September 2015 in Wiley Online Library (wileyonlinelibrary.com). DOI 10.1002/hed.24156
ABSTRACT: Background. The variety of surgical approaches to jugularschwannomas makes selection of an approach difficult. The purpose ofthis study was to define the anatomic elements of these approaches.Methods. Ten adult cadaveric heads were examined.Results. There are lateral, posterior, and anterior routes that access vari-ous parts of the jugular foramen. Removal of the jugular process of theoccipital bone provides access to the posterior aspect of the foramen,the infralabyrinthine mastoidectomy provides access to the lateral edgeand dome of the jugular bulb, and the preauricular approaches provideaccess to the anterior margin of the bulb and foramen. Additions to these
approaches may include cervical and vertebral artery exposure, facialnerve transposition, foramen magnum exposure, and external canal andcondylar resection.Conclusion. An understanding of the anatomy of the jugular foramen iscrucial in achieving total tumor removal while minimizing risk. VC 2015Wiley Periodicals, Inc. Head Neck 38: E1041–E1053, 2016
KEY WORDS: jugular foramen, jugular process, schwannoma, tem-poral bone, skull base
INTRODUCTIONTwenty-five percent of schwannomas are found in the headand neck.1 Intracranial schwannomas can arise from cranialnerves (CNs), however, except for the vestibular schwan-noma, they are uncommon.2–4 Jugular foramen schwan-nomas arise mainly from the ganglion of CNs IX and X.Song et al5 proposed that the growth pattern of these tumorsin the jugular foramen depends on the ganglion of origin.However, the variable location and nerve and vesselinvolvements make the precise site of origin of sometumors difficult to define.5–9 Advances in imaging haveaided in differentiating jugular foramen schwannomas fromglomus jugulare, meningioma, and other tumors, and indefining the precise location, extension, and vascular rela-tionships of the tumor.9 Selection of an appropriateapproach should be based on the preoperative neurologicalfindings, and on tumor size, location, and extensionrevealed by MRI, CT, and angiographic studies. Severalclassifications of jugular foramen schwannomas have beenbased on tumor location, size, and extension.3,7,10,11 Theclassification by Kaye et al7 is popular and Pellet et al10
added an hourglass-type tumor. Type A tumors are primar-ily intracranial with some extension into the foramen; typeB tumors are primarily in the foramen with or without intra-cranial extension; type C tumors are primarily extracranialwith a minor extension into the foramen or into the poste-rior fossa; and type D tumors are dumbbell-shaped with
intracranial and extracranial extension linked via the fora-men. Placing the tumor in one of these categories facilitatesoperative planning and selection of an appropriate surgicalapproach.
The jugular foramen is commonly accessed by posteriorand lateral approaches and less commonly by anteriorapproaches. This abundance of approaches to the foramen hasgiven rise to confusion in selecting the appropriate approach.In this study, the literature on the approaches to the jugularforamen was combined with dissections defining the mainanatomic features of each approach (Table 1).3,6,7,12–33
MATERIALS AND METHODSTen hemicrania from formalin-perfused adult cadaveric
heads in which the arteries and veins were injected with redor blue silicone rubber (Dow Corning, Midland, MI), Thinner200 (Dow Corning), and RTV catalyst (Dow Corning), weredissected using 33 to 340 magnifications of the surgicalmicroscope and a 08, 18-cm Hopkins endoscope (Karl StorzGmbH, KG, Tottlingen, Germany) connected to a xenon lightsource and a high-definition camera. The lateral suboccipital,far lateral,20,32,34 postauricular transtemporal,14,35 preauricularsubtemporal infratemporal fossa,28 and endoscopic transnasal/transmaxillary transpterygoid approaches16,36,37 were per-formed to open the jugular foramen from a variety of angles.
RESULTS
Microsurgical anatomy of the jugular foramenand its surrounding area
The petrous part of the temporal bone forms the antero-superior part of the foramen and dome of the jugular
*Corresponding author: A. L. Rhoton, Jr, Department of Neurosurgery,University of Florida, College of Medicine, P.O. Box 100265, Gainesville, FL32610-0265. E-mail: [email protected]
HEAD & NECK—DOI 10.1002/HED APRIL 2016 E1041

TABLE1.
Review
ofliteratureon
approaches
tothejugularforam
en.
Tumor
type
Elem
entsofapproach
Optionalexposureifneeded
Approach
byroute
Author
Year
ABCAnt.
Mast.
Neck
JPDu
raCond.
FMC1
VAFN
EAC
Anterior
Endoscopictransnasal/transmaxillarytranspterygoid
Dallan1
62010
Lateral
Gardner’s
approach
Gardner17
1977
IL1
12
22
22
1Ifnecessary
Type
Ainfratemporalfossa
Fisch1
21979
IL1
2Possible
22
22
11
Infralabyrinthine
Kaye
71984
IL1
22
22
22
11
Infralabyrinthine
Lambert2
21985
IL1
22
22
22
11
Preauricularsubtem
poralinfratemporalfossa
Sekhar28
1987
21
22
22
22
22
Postauriculartranstemporal
Tedeschi14
1994
IL1
1PreorRS
orSi
22
22
11
Cervicaltransmastoid
Samii3
1995
IL1
1Pre
Posterior
22
22
2Juxtacondylar
George
181995
Limited
11
Possible(Si)
1/3posterior
21
Possible
22
Fallopian
bridge
technique
Pensak
271997
IL2
22
22
22
22
Transjugularcraniotomywith
fallopian
bridge
technique
Oghalai26
2004
IL1
N.D.
Si2
22
22
2Transcondylarsuprajugular
Kadri6
2004
IL1
Posterior
Pre
1/2-2/3posterior
12
22
2Presigmoidalsuprabulbarinfralabyrinthine
Cinibulak1
52013
IL2
2Pre
22
22
22
Posterior
Retrosigm
oidlateralsuboccipital
Krause
331903
22
2RS
22
22
22
Farlateral
Heros2
01986
22
2RS
21
22
22
Extremelateral
Sen2
91990
IL1
1RS
Posteriorh
alf
12
22
2Suboccipitalapproachwith
openingJF
Sasaki31
1991
22
1RS
Posterior
12
22
2Paracondylar
Wen
321997
LimitedN.D.
1RS
21
PossiblePossible
22
Posteriortransjugularand
transcervical
Nakamizo2
52013
Limited
11
Si1/3posterior
11
22
2Combined
Suboccipitalcraniectomywith
retrolabyrinthineremoval/
retromastoidealcraniectomycombinedwith
amastoidectomy
Hakuba
191979
IL1
1RS
orSi
22
12
22
Transsigmoid
Mann2
41991
IL1
1Si
Ifnecessary
22
22
2Transcondylar
Seyfried3
01994
Limited
11
SiPosterolateral
11
12
2PetrooccipitalTranssigm
oid
Mazzoni13
1995
IL1
1Si
Ifnecessary
22
21
2Hearingpreservationtechnique
Kim21
2001
IL1
1Si
22
22
12
ThecombinedtransmastoidretrolabyrinthineandInfralabyrinthine
transjugulartranscondylartranstubercularhigh
cervical
Liu2
32006
IL1
1Si
1/3posterior
12
1Ifnecessary
2
Abbreviations:A
nt.,anterior;Mast.,
mastoidectomy;Neck,neckdissection;JP,jugular
process;Du
ra,duraopening;Cond.,removalofoccipitalcondyle;FM,opening
offoramen
magnum;C
1,removalofC1
transverseprocess;VA,vertebralarterytranslocation;FN,
translocationofthefacialnerve;EAC,
resectionoftheexternalearcanal;IL,infralabyrinthine;Pre,presigmoid;RS
,retrosigm
oid;Si,resectionofthesigm
oidsinus;N.D.,notdescribed;JF,jugularforam
en.
Yellowincludes
infralabyrinthineapproach;lightgreenincludes
resectionofjugularp
rocess;darkorange
representstheapplicabletumortype;and
lightorange
isused
forselectedcases.
KOMUNE ET AL.
E1042 HEAD & NECK—DOI 10.1002/HED APRIL 2016

bulb. The jugular process of the occipital bone forms theposterior margin of the foramen. The jugular foramen ispositioned between the occipitomastoid suture laterallyand petro-occipital fissure medially (see Figure 1). The
dome of the jugular bulb is located just below the vestib-ular labyrinth.
The jugular foramen is divided into 3 parts: a petrosalpart through which the petrosal sinus passes, a sigmoid
APPROACHES TO JUGULAR SCHWANNOMAS
HEAD & NECK—DOI 10.1002/HED APRIL 2016 E1043

part through which the sigmoid sinus passes, and an intra-jugular part through which the nerves pass. The intrajugu-lar part is positioned between the sigmoid and petrosalparts, and is the site of bony prominences called the intra-jugular processes on the opposing surfaces of the tempo-ral and occipital bones (Figure 1A). An intrajugular ridgeextends forward from the intrajugular process of the tem-poral bone along the medial edge of the jugular bulb tomeet the ridge along the posterior edge of the entranceinto the carotid canal called the carotid ridge. The intraju-gular ridge of the temporal bone is directed slightlymedial and is the site of a shallow glossopharyngealgroove on its medial surface along which the glossopha-ryngeal nerve courses. The carotid ridge separates thejugular foramen and carotid canal and meets the styloidprocess near its lateral edge (Figures 1B and 1C). CNsIX, X, and XI pass through the intrajugular part of thejugular foramen. The dura covering the jugular foramenis divided by a dural fold into the glossopharyngeal andvagal meati. CN IX enters the glossopharyngeal meatusabove and lateral to where CNs X and XI enter the vagalmeatus. CN XII, after passing through the hypoglossalcanal, joins CNs X and XI to descend with them in thecarotid sheath (Figures 1D–1F).
The occipital condyle is situated along the lateral mar-gin of the anterior half of the foramen magnum in thearea below and medial to the jugular foramen (Figures1B and 1C). The occipital condyle is located anterior andinferior to a shallow depression, the condylar fossa, inwhich the posterior condylar emissary vein enters the pos-terior condylar canal to reach and empty into the sigmoidsinus. The jugular process of the occipital bone extendslaterally from the area just above the posterior half of theoccipital condyle and forms the posterior margin of theforamen. Removing the jugular process provides access tothe posterior edge of the jugular bulb and internal jugularvein when combined with the lateral suboccipitalapproach, infralabyrinthine mastoidectomy, or cervicalexposure. The occipitomastoid suture passes between thelateral edge of the jugular process and the medial edge ofthe digastric groove and styloid process to end at the jug-ular foramen (Figures 1B and 1C). The stylomastoid fora-men, through which the facial nerve passes, is locatedjust anterolateral to the jugular process.
The jugular bulb and adjacent part of the internal jugu-lar vein receive drainage from both intracranial andextracranial veins, including the sigmoid and inferiorpetrosal sinuses, the vertebral venous plexus, the venousplexus of the hypoglossal canal, the posterior condylaremissary vein, and the vein coursing along the inferioraspect of the petro-occipital fissure. The inferior petrosalsinus communicates with the cavernous sinus and basilarvenous plexus at its upper end and with the jugular bulbor the internal jugular vein at its lower end (Figure 1F).38
Multi-approach exposure of the jugular foramen
No single previously reported operative approach pro-vides access to the full margin of the jugular foramen,however, selection from among the reported approachesprovides access to selective segments of all edges of theforamen depending on the approach selected. In evaluat-ing this, the approaches exposing the anterior, lateral, andposterior surface of the foramen were performed on singlespecimens. It began with the postauricular transtemporalapproach with a high cervical exposure to gain control ofthe internal carotid artery, internal jugular vein, and lowerCNs below the jugular foramen. The initial step involveddetaching the muscles attached to the mastoid process,including the sternocleidomastoid, semispinalis, longissi-mus, and digastric, to expose the occipital artery, rectuscapitis lateralis, transverse process of C1, and suboccipitaltriangle. After this first step, the transverse process of C1,mastoid tip, parotid gland covering the facial nerve, andrectus capitis lateralis remain as obstacles to exposing theforamen (Figure 2A). Next, the infralabyrinthine mastoi-dectomy was performed to expose the superior and lateralaspects of the jugular bulb (Figure 2B). Removing themastoid tip and extending the drilling downward alongthe occipitomastoid suture and exposing the sigmoid sinusaccessed the attachment of the rectus capitis lateralis tothe inferior surface of the jugular process. The sigmoidsinus crosses the occipitomastoid suture just before emp-tying into the jugular bulb. This surgical field is limited ifthe facial nerve is not transposed anteriorly and the jugu-lar process is not removed (Figure 2C). Detaching therectus capitis lateralis and removing the jugular processof the occipital bone opened the posteroinferior aspect ofthe jugular foramen and provided wide access for tumor
FIGURE 1. (A) Posterior superior view of the right jugular foramen. The foramen is divided into 3 parts: petrosal, sigmoid, and intrajugular. Theintrajugular part, through which cranial nerves (CNs) IX, X, and XI pass, is the site of the intrajugular process and ridge, which separates the sig-moid and petrosal parts. The sigmoid sinus drains through the sigmoid part and the inferior petrosal sinus passes through the petrosal part. (B andC) Inferior view of the jugular foramen and jugular process. The occipital condyle is located anterior to the condylar fossa (interrupted line). Thejugular process (green) is located posterior to the jugular foramen and extends laterally from the posterior half of the occipital condyle. The jugularfossa and foramen are positioned superior and lateral to the anterior half of the occipital condyle. (D) Posterior view, right cerebellopontine angle.The jugular foramen is located between the internal acoustic meatus and the jugular tubercle. The rectus capitis lateralis attaches to the inferiorsurface of the jugular process, which is located posterior to the jugular foramen. (E) Endoscopic view of the right jugular foramen. CNs IX, X, andXI pass through the intrajugular part of the foramen. The dural roof of the foramen is the site of the glossopharyngeal and vagal meati. A dural sep-tum separates the 2 meati. (F) Lateral view of the intrajugular part of the left jugular foramen. The jugular bulb has been translocated posteriorlyafter removing all of the temporal bone except the petrous apex. The inferior petrosal sinus passes between the glossopharyngeal and vagusnerves to empty into the jugular bulb. The accessory nerve passes posterior to the vagus nerve. A., artery; Ac., acoustic; Atlanto-occip., atlanto-occipital; Cap., capitis; Car., carotid; Cond., condylar, condyle; Fiss., fissure; Flocc., flocculus; For., foramen; Glossopharyng., glossopharyngeal;Hypogloss., hypoglossal; Inf., inferior; Int., internal; Intrajug., intrajugular; Jug., jugular; Lat., lateralis; Lt., left; M., muscle; Mag., magnum; Mast.,mastoid; Meat., meatus; N., nerve; Occip., occipital; Occipitomast., occipitomastoid; Pet., petrosal; Petro-occip., petro-occipital; P.I.C.A., posteriorinferior cerebellar artery; Proc., process; Pyramid., pyramidal; Rec., rectus; Rt., right; Sig., sigmoid; Styl., styloid; Stylomast., stylomastoid; Sup.,superior; Temp., temporal; Tuberc., tubercle; Vag., vaginal; Vert., vertebral.
KOMUNE ET AL.
E1044 HEAD & NECK—DOI 10.1002/HED APRIL 2016

removal without transposition of the facial nerve (Figure2D). Extending the drilling medially above the jugularbulb exposes the cochlear aqueduct, which opens into thepyramidal fossa located medial to the glossopharyngealgroove of the temporal bone (Figures 1C and 2E). Next,
several steps were added to widen the surgical field. Thefallopian bridge technique in which the facial canal isskeletonized without transposition is completed to exposethe junction of the inferior petrosal sinus, the jugularbulb, the area anterolateral to the jugular bulb, and the
APPROACHES TO JUGULAR SCHWANNOMAS
HEAD & NECK—DOI 10.1002/HED APRIL 2016 E1045

middle ear cavity (Figure 2E).27,39 An intracranial exten-sion of the tumor can be accessed by opening the presig-moid or retrosigmoid dura. In the presigmoid approach,the otic capsule will rarely be an obstacle if the sigmoidsinus and the posterior fossa dura behind the cochlearcanaliculus are exposed to provide access to the areabetween the jugular foramen and the nerves entering theinternal acoustic meatus (Figure 2F). For the retrosigmoidapproach, the superior oblique muscle is detached fromthe superior nuchal line and a lateral suboccipital craniec-tomy is completed to access the lower CNs intradurally(Figure 2G).
The far lateral approach, a modification of the lateralsuboccipital approach used to access the lower cerebello-pontine angle and foramen magnum, was completed bydrilling the edge of the foramen magnum up to the poste-rior edge of the occipital condyle (see Figure 3). Thebasic far lateral approach without drilling of the occipitalcondyle provides increased access to the entry of CNs IX,X, and XI into the dural roof and intrajugular part of thejugular foramen (Figures 3C and 3D).32 Detaching themuscles attached to the superior and inferior nuchal linesexposed the condylar fossa, vertebral artery, and sur-rounding venous plexus, which is continuous with theposterior condylar emissary vein passing through the con-dylar canal located superior to the occipital condyle (Fig-ures 3A and 3B). From the posterior view, the insertionof the rectus capitis lateralis is identified medial to theoccipital artery and digastric muscle. Opening the poste-rior edge of the jugular foramen extradurally required theremoval of the jugular process, which extends laterallybehind the jugular foramen (Figures 3C and 3E). The jug-ular process is removed after detaching the rectus capitislateralis from its inferior surface to expose the posteroin-ferior surface of the jugular foramen, as described byWen et al32 (Figure 3E). Drilling the occipital condyleand area above the condyle to expose the hypoglossalcanal and its junction with the medial surface of the inter-nal jugular vein adds minimally to the exposure of theforamen, is infrequently needed, and may result in cervi-cocranial instability requiring occipitocervical fusion (Fig-ure 3E). The accessory nerve occasionally passes betweenthe C1 transverse process and the internal jugular vein.40
The Fisch and Pillsbury12 and Fisch et al41 type Ainfratemporal fossa approach or Sekhar et al28 and Senand Sekhar42 preauricular subtemporal infratemporal fossaapproach, both lateral approaches, were utilized to accessthe anterolateral aspect of the jugular foramen. The pre-auricular subtemporal infratemporal fossa approach, asdescribed by Sekhar et al,28 provides access to the middleand infratemporal fossae and the anterolateral aspect ofthe jugular bulb and makes it possible to translocate thepetrous carotid anteriorly and access the petrous apex(Figures 4A and 4B). Removing the floor of the middlefossa around the foramen ovale, petrous carotid, inferiorpetrosal sinus, and the medial half of the inferior part ofthe vaginal process of the temporal bone exposed theanterior edge of the jugular bulb, carotid ridge, and exitsite of the glossopharyngeal nerve (Figure 4B). Removingthe styloid process allowed exposure of the anterolateraledge of the opening of the jugular bulb, however, carehad to be taken to avoid injury of the facial nerve at thissite.
Recently, the jugular foramen has been exposed endo-scopically.16,36,37,43 In this technique, dissection extendedposteriorly along the eustachian tube via the transnasal/transmaxillary and transpterygoid routes (Figure 4C). Theeustachian tube is an important landmark for reaching thejugular foramen. After transecting the lateral pterygoidmuscle, the medial pterygoid and tensor veli palatinimuscles are reflected laterally to expose the eustachiantube, tubal attachment of the levator veli palatini muscle,and the stylopharyngeal fascia (aponeurosis), which cov-ers the internal carotid artery, internal jugular vein, andlower CNs, and is opened to expose the area just belowthe jugular foramen. The internal carotid artery ascendsjust anteromedial to the internal jugular vein. CN IXdescends laterally between the internal jugular vein andinternal carotid artery after it exits the jugular foramen(Figure 4D). The vaginal process enclosing the base ofthe styloid process covers the anterolateral to lateralaspects of the junction of the internal jugular vein andjugular bulb (Figure 4D).
Finally, after completing the far lateral approach, infra-labyrinthine mastoidectomy, resection of the jugular pro-cess while preserving its inferior surface, and the
FIGURE 2. (A) High cervical exposure. The insert (upper left) shows the left postauricular C-shaped incision. The high cervical dissection hasexposed the mastoid tip, rectus capitis lateralis, and suboccipital triangle (dotted line) between the superior and inferior oblique and rectus capitisposterior major muscles. (B) The infralabyrinthine mastoidectomy. Each semicircular canal has been exposed; superior (S), lateral (L), and posterior(P). The infralabyrinthine and retrofacial air cells have been removed to expose the jugular bulb. A posterior tympanotomy has been performed tofacilitate exposure of the facial canal. (C) Removing the mastoid tip exposes the attachment of the rectus capitis lateralis to the inferior surface ofthe jugular process. To avoid injuring the facial nerve, the cuff of fibrous tissue encasing the nerve and the stylomastoid artery at the stylomastoidforamen have been preserved. (D) Removing the jugular process and rectus capitis lateralis exposes the posterior surface of the jugular bulb. Theposterior condylar emissary vein connects the jugular bulb and the vertebral venous plexus. (E) Fallopian bridge technique, which leaves a thinshell of bone around the facial nerve. The drilling has been extended below the facial recess, and the bone between the facial canal (fallopiancanal) and the posterior wall of the external auditory canal have been removed to provide a view into the middle ear and the anterolateral aspectof the jugular foramen. (F) Presigmoid exposure. The cochlear aqueduct has been exposed before opening the presigmoid dura. The dura in frontof the sigmoid sinus has been opened to expose cranial nerves (CNs) VII to XI. (G) Retrosigmoid exposure. The dura behind the sigmoid sinus hasbeen opened to expose CNs VII to XI. A., artery; A.I.C.A, anterior inferior cerebellar artery; Acc., accessory; Ant., anterior; Aque., aqueduct; Aud.,auditory; Auric., auricular; Br., branch; Cap., capitis; Car., carotid; Chor., chorda, choroid; Cochl., cochlear; Cond., condylar; Dig., digastric; Emiss.,emissary; Endolymph., endolymphatic; Ext., external; Flocc., flocculus; For., foramen; Gl., gland; Gr., greater; Inf., inferior; Int., internal; Jug., jugu-lar; Lat., lateral, lateralis; Lev., lavator; M., muscle; Mast., mastoid; Meat., meatus; N., nerve; Obl., oblique; Occip., occipital; Occipitomast., occipi-tomastoid; Pet., petrosal; Plex., plexus; Post., posterior; Rec., rectus; Scap., scapulae; Sig., sigmoid; Stylomast., stylomastoid; Suboccip.,suboccipital; Sup., superior; Surf., surface; Temp., temporal; Tymp., tympani, tympanic; V., vein.
KOMUNE ET AL.
E1046 HEAD & NECK—DOI 10.1002/HED APRIL 2016
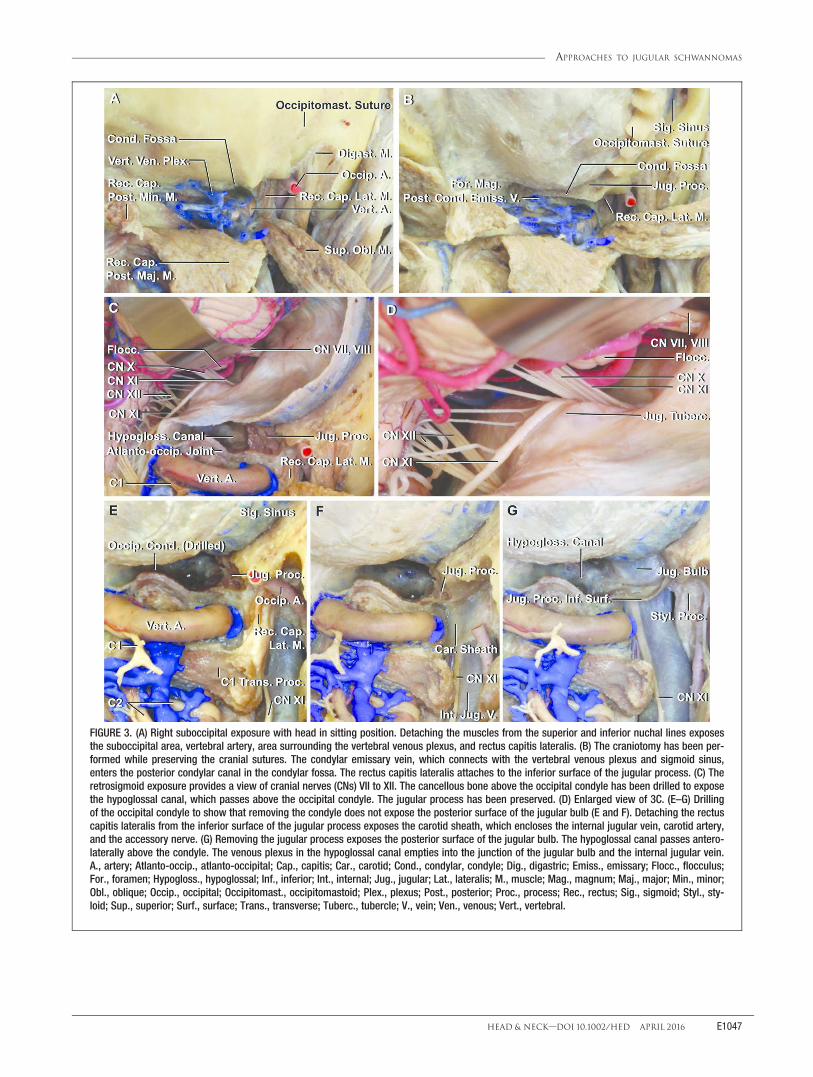
FIGURE 3. (A) Right suboccipital exposure with head in sitting position. Detaching the muscles from the superior and inferior nuchal lines exposesthe suboccipital area, vertebral artery, area surrounding the vertebral venous plexus, and rectus capitis lateralis. (B) The craniotomy has been per-formed while preserving the cranial sutures. The condylar emissary vein, which connects with the vertebral venous plexus and sigmoid sinus,enters the posterior condylar canal in the condylar fossa. The rectus capitis lateralis attaches to the inferior surface of the jugular process. (C) Theretrosigmoid exposure provides a view of cranial nerves (CNs) VII to XII. The cancellous bone above the occipital condyle has been drilled to exposethe hypoglossal canal, which passes above the occipital condyle. The jugular process has been preserved. (D) Enlarged view of 3C. (E–G) Drillingof the occipital condyle to show that removing the condyle does not expose the posterior surface of the jugular bulb (E and F). Detaching the rectuscapitis lateralis from the inferior surface of the jugular process exposes the carotid sheath, which encloses the internal jugular vein, carotid artery,and the accessory nerve. (G) Removing the jugular process exposes the posterior surface of the jugular bulb. The hypoglossal canal passes antero-laterally above the condyle. The venous plexus in the hypoglossal canal empties into the junction of the jugular bulb and the internal jugular vein.A., artery; Atlanto-occip., atlanto-occipital; Cap., capitis; Car., carotid; Cond., condylar, condyle; Dig., digastric; Emiss., emissary; Flocc., flocculus;For., foramen; Hypogloss., hypoglossal; Inf., inferior; Int., internal; Jug., jugular; Lat., lateralis; M., muscle; Mag., magnum; Maj., major; Min., minor;Obl., oblique; Occip., occipital; Occipitomast., occipitomastoid; Plex., plexus; Post., posterior; Proc., process; Rec., rectus; Sig., sigmoid; Styl., sty-loid; Sup., superior; Surf., surface; Trans., transverse; Tuberc., tubercle; V., vein; Ven., venous; Vert., vertebral.
APPROACHES TO JUGULAR SCHWANNOMAS
HEAD & NECK—DOI 10.1002/HED APRIL 2016 E1047
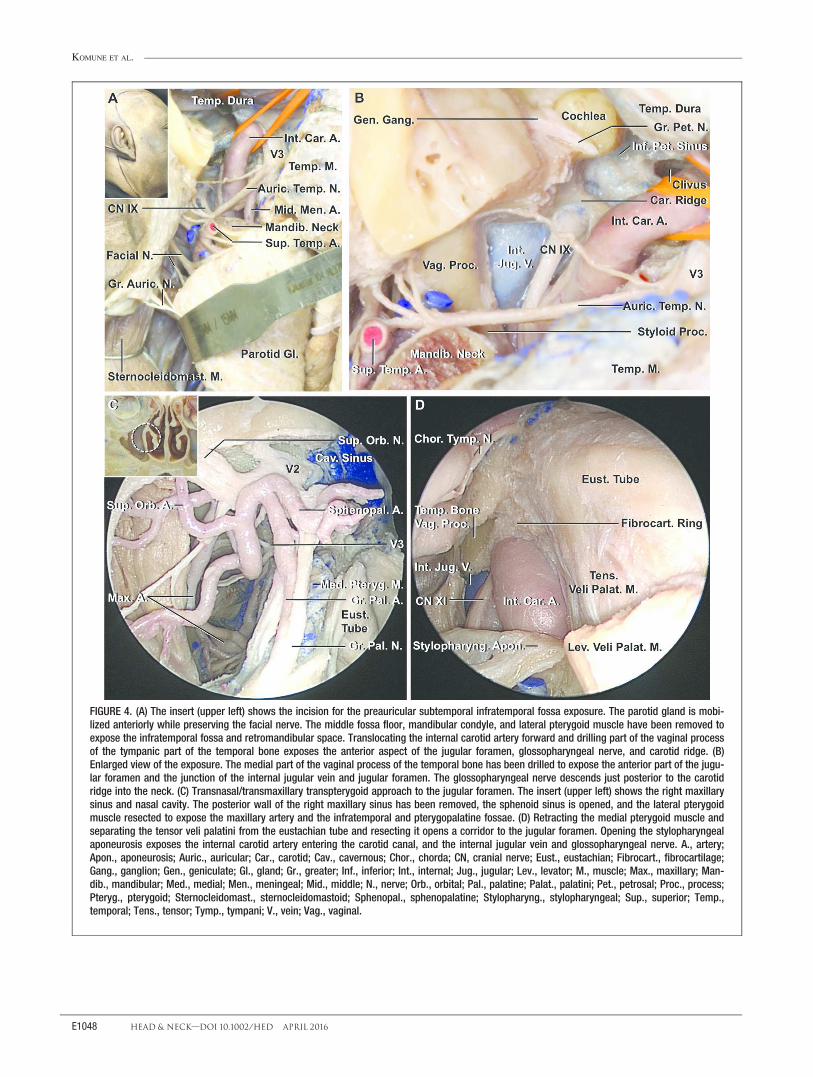
FIGURE 4. (A) The insert (upper left) shows the incision for the preauricular subtemporal infratemporal fossa exposure. The parotid gland is mobi-lized anteriorly while preserving the facial nerve. The middle fossa floor, mandibular condyle, and lateral pterygoid muscle have been removed toexpose the infratemporal fossa and retromandibular space. Translocating the internal carotid artery forward and drilling part of the vaginal processof the tympanic part of the temporal bone exposes the anterior aspect of the jugular foramen, glossopharyngeal nerve, and carotid ridge. (B)Enlarged view of the exposure. The medial part of the vaginal process of the temporal bone has been drilled to expose the anterior part of the jugu-lar foramen and the junction of the internal jugular vein and jugular foramen. The glossopharyngeal nerve descends just posterior to the carotidridge into the neck. (C) Transnasal/transmaxillary transpterygoid approach to the jugular foramen. The insert (upper left) shows the right maxillarysinus and nasal cavity. The posterior wall of the right maxillary sinus has been removed, the sphenoid sinus is opened, and the lateral pterygoidmuscle resected to expose the maxillary artery and the infratemporal and pterygopalatine fossae. (D) Retracting the medial pterygoid muscle andseparating the tensor veli palatini from the eustachian tube and resecting it opens a corridor to the jugular foramen. Opening the stylopharyngealaponeurosis exposes the internal carotid artery entering the carotid canal, and the internal jugular vein and glossopharyngeal nerve. A., artery;Apon., aponeurosis; Auric., auricular; Car., carotid; Cav., cavernous; Chor., chorda; CN, cranial nerve; Eust., eustachian; Fibrocart., fibrocartilage;Gang., ganglion; Gen., geniculate; Gl., gland; Gr., greater; Inf., inferior; Int., internal; Jug., jugular; Lev., levator; M., muscle; Max., maxillary; Man-dib., mandibular; Med., medial; Men., meningeal; Mid., middle; N., nerve; Orb., orbital; Pal., palatine; Palat., palatini; Pet., petrosal; Proc., process;Pteryg., pterygoid; Sternocleidomast., sternocleidomastoid; Sphenopal., sphenopalatine; Stylopharyng., stylopharyngeal; Sup., superior; Temp.,temporal; Tens., tensor; Tymp., tympani; V., vein; Vag., vaginal.
KOMUNE ET AL.
E1048 HEAD & NECK—DOI 10.1002/HED APRIL 2016

preauricular subtemporal infratemporal fossa approach, thespecimen was examined to determine the extent to whicheach approach added to the exposure of the jugular fora-men (see Figure 5). This dissection shows that the externalear canal, facial canal, mastoid process, and root of the sty-loid process are obstacles to opening the jugular foramencompletely and that resecting the jugular process provideswide access for the removal of tumor within the foramen
(Figures 5B–5D). In the preauricular subtemporal infratem-poral fossa approach, drilling the medial part of the vaginalprocess exposed the anterolateral part of the jugular bulb(Figures 5E and 5F), and resection of the styloid processwidened this exposure. The lateral suboccipital approachcombined with resection of the jugular process providedaccess to the jugular foramen both extracranially and intra-cranially, and widened the exposure of the posteroinferior
APPROACHES TO JUGULAR SCHWANNOMAS
HEAD & NECK—DOI 10.1002/HED APRIL 2016 E1049

aspect of the jugular bulb. Resection of the occipital con-dyle provided access to the hypoglossal canal, but did notincrease the exposure of the jugular foramen (Figures 5Gand 5H).
DISCUSSIONMost jugular foramen schwannomas are approached by
a lateral or posterior route. Some of these lateral and pos-terior approaches are similar but named differently, andsome are a combination of previous approaches givennew names (Table 1). This adds difficulty in selecting asurgical approach. The purpose of this study was todefine the anatomic steps in the approaches to the jugularforamen. Among the operative steps involved in theapproaches to the jugular foramen, resection of the jugu-lar process is one of the most important. Wen et al,32
Nakamizo et al,25 Nakamizo et al,31 and Sanna et al44
described the importance of resection of the jugular pro-cess for exposing the posteroinferior surface of the jugu-lar bulb (Figure 6A). It is reasonable to consider addingthe removal of the jugular process if the tumor within theforamen extends posteriorly or occludes thebulb.3,6,8,14,17,19,21,23–26,29,30,45 Care should be taken toavoid injury to the facial nerve during drilling of the jug-ular process, because the stylomastoid foramen is locatedjust lateral to the jugular process. Another important stepis the infralabyrinthine mastoidectomy, which is com-monly included in lateral or combined approaches but canalso be included in a posterior approach (Table 1).
The type A infratemporal fossa approach12,41 and pre-auricular subtemporal infratemporal fossa approaches,28,42
both lateral routes, provide access to the anterolateral andanterior edges of the jugular foramen. The jugular fora-men is formed by the petrous part of the temporal boneanterosuperiorly and by the jugular process of the occipi-tal bone posteroinferiorly. The vaginal process enclosingthe base of the styloid process blocks access to theanterolateral to lateral aspects of the junction of the inter-nal jugular vein and jugular bulb. The exposure of theanterolateral aspect of the jugular foramen is challenging
because the lower opening of the foramen is positionedjust posterolateral to the carotid canal. Accessing theanterolateral aspect of the foramen may require transloca-tion of the facial nerve, management of the petrouscarotid artery, sacrifice of the external ear canal and mid-dle ear, and drilling of the vaginal process. The approachdescribed by Fisch and Pillsbury12 in 1979 provides supe-rior, lateral, and anterior exposure of the jugular foramenand includes anterior translocation of the facial nerve andsacrifice of the external auditory canal and tympanic cav-ity as needed. Since then, others have modified andextended Fisch’s approach. Mazzoni and Sanna13 pro-posed the petro-occipital trans-sigmoid approach for pos-terolateral exposure of the jugular foramen, and Tedeschiand Rhoton14 introduced a postauricular transtemporalapproach. Sanna et al44 reported the infratemporal fossaapproach type A with transcondylar and transtubercularextension to obtain posteroinferior and medial access tothe jugular bulb. In addition, a variety of other surgicalapproaches to the jugular foramen have beendescribed.3,6–8,13,15–32,44–47 The endoscopic transnasal/transmaxillary transpterygoid approach is an infrequentlyutilized anterior route.
In our dissections, the external ear canal, facial canal,and root of the styloid process prevented the completeopening of the lateral aspect of the jugular foramen. Theonly area that cannot be opened without the transpositionof the facial nerve is just medial to the root of the styloidprocess (Figures 5 and 6A). Complete resection of jugularforamen schwannomas is generally possible without ante-rior transposition of the facial nerve, which may causefacial nerve deficit.27,48 The transmastoid approach withsacrifice of the labyrinth and cochlea to enlarge the surgi-cal field is rarely selected for jugular foramen schwan-noma because preservation and improvement in hearing iscommon after tumor removal.49–51
Translocation of the vertebral artery, which ascends inthe transverse foramen and runs horizontally behind theatlantal or occipital condyles, is not necessary. However,removal of the transverse process of the atlas is helpful
FIGURE 5. Multi-approach exposure of the jugular foramen. (A–H) The far lateral, preauricular transtemporal infratemporal, and transmastoid infra-labyrinthine exposures have been completed on the right side to show the extent of exposure of the jugular bulb that can be achieved withoutresection of the external ear canal and translocation of the facial nerve. The parotid has been removed to make it easier to see the facial nerveand the area around the jugular foramen. The angle of view of each figure is shown in the insert using 3D coordinate axes. (A) Lateral view. Themastoid tip, styloid process, and external ear canal are obstacles to exposing the jugular foramen. (B) Posterolateral exposure viewed parallel tothe external ear canal. The superior and lateral surfaces of the jugular bulb can be identified from this angle. In this view, the mastoid tip does notblock access to the lateral aspect of the jugular bulb. However, the facial canal blocks access to the jugular bulb. (C) A 45o posterolateral view.The jugular process has been removed while preserving its inferior surface. Removing the jugular process exposes the posterior wall of the jugularbulb. (D) Rotating the view posteriorly provides a view of cranial nerves (CNs) IX, X, and XI entering the dural roof of the jugular foramen. (E) Lateralview of the preauricular subtemporal infratemporal fossa approach. The floor of the middle fossa has been removed and the medial half of the vag-inal process of the tympanic part of the temporal bone drilled to expose the sigmoid sinus at the anterior edge of the jugular foramen. The parotidgland has been removed to facilitate the view of the anterior edge of the jugular foramen. (F) Superolateral view. The floor of the middle fossa lat-eral to the cochlea has been removed. The inferior petrosal sinus empties into the internal jugular vein just below the jugular bulb. The glossopha-ryngeal nerve descends through the dural glossopharyngeal meatus and turns downward lateral to the inferior petrosal sinus. (G) Lateralsuboccipital (retrosigmoid) approach. This approach accesses the dural roof of the jugular foramen. Removing the jugular process of the temporalbone exposes the posterior and inferior surfaces of the jugular bulb. In this view, the vertebral artery partially blocks the view of the course of theaccessory nerve. (H) View lateral to that shown in panel G. The intracranial, posterior/inferior surfaces of the jugular foramen, and hypoglossalcanal have been exposed. The course of the accessory nerve is visible without translocation of the vertebral artery. A., artery; Atlanto-occip.,atlanto-occipital; Aud., auditory; Car., carotid; Dig., digastric; Ext., external; Gr., greater; Hypogloss., hypoglossal; Inf., inferior; Int., internal; Jug.,jugular; M., muscle; Mast., mastoid; Max., maxillary; N., nerve; Pet., petrosal; P.I.C.A., posterior inferior cerebellar artery; Post., posterior; Proc.,process; Sig., sigmoid; Styl., styloid; Sup., superior; Surf., surface; Temp., temporal; Trans., transverse; V., vein; Vert., vertebral.
KOMUNE ET AL.
E1050 HEAD & NECK—DOI 10.1002/HED APRIL 2016

because it widens the surgical field posterior to the sig-moid sinus and internal jugular vein and the lower CNswithout translocation of the vertebral artery.25,45
Removing the occipital condyle without resection ofthe jugular process does not aid in opening the jugularfossa and is unnecessary.32 Resection of the posterolateraledge of the condyle may prove helpful in exposing theposteromedial edge of the internal jugular vein, butremoving more than the posterior one third of the condylemay cause craniocervical instability.
Sacrifice of the sinus with ligation of both the sigmoidsinus and internal jugular vein and opening the jugularbulb, developed for glomus jugulare tumors in the region,may infrequently be considered for achieving completeremoval of the jugular foramen schwannoma occludingthe sinus.6
Approaches based on tumor type
The key steps to expose the contents of the foramenand jugular bulb are the infralabyrinthine mastoidectomyand/or resection of the jugular process, which may becombined with the lateral suboccipital approach or a post-auricular transtemporal approach and/or cervical expo-sure. The selection of which procedures should beselected is based on the pattern of growth of an intrafora-minal tumor. Infralabyrinthine mastoidectomy would beadded if the foraminal part of the tumor extends into theinfralabyrinthine area and pushes the jugular bulb inferi-orly. Resection of the jugular process would be added ifthe tumor extends posteroinferiorly. The combined infra-labyrinthine and jugular process resection can add a muchwider field for resection of foraminal tumors.
The lateral suboccipital approach has a variety of modi-fications. The far lateral extension will aid in removingtumors extending anterior to the lower brainstem.20 Forforaminal tumors with intracranial growth, the lateral sub-occipital approach may be combined with infralabyrin-thine mastoidectomy and/or removal of the jugularprocess. The petro-occipital trans-sigmoid approach uti-lizes a combination of a retrolabyrinthine and infralabyr-inthine mastoidectomy and the lateral suboccipitalapproach with sacrifice of the sigmoid sinus.13 Thisapproach can access the intracranial, foraminal, and cervi-cal pathology while preserving facial nerve function, andthe external auditory canal, tympanic cavity, and laby-rinth.52 If a type A (intracranial) tumor has some exten-sion into only the upper part of the foramen, thesuprajugular extension, in which only the medial part ofthe roof of the jugular foramen is removed, may allowcomplete tumor removal.26,53 Recently, an endoscopic ret-rosigmoid approach that includes drilling only the roof ofthe foramen in the area below the internal acoustic mea-tus has been developed that may allow complete removalof a tumor with small extension into the foramen.54
The infralabyrinthine mastoidectomy provides accessalong the dome and lateral side of the jugular bulb.15,55
When a tumor within the jugular fossa extends upwardabove the bulb or displaces the jugular bulb inferiorlywithout extension intracranially, the infralabyrinthinemastoidectomy is a good option but provides only limitedspace for accessing the tumor and should often be com-bined with another approach to widen the exposure. For atype B (foraminal) tumor with some intracranial exten-sion, an infralabyrinthine mastoidectomy combined with
FIGURE 6. (A) Inferior view of jugular foramen. The site of the jugular bulb (dark blue), internal carotid artery (red), and sigmoid sinus (light blue)are shown on an image of the lower surface of the right jugular foramen. The margin of the foramen exposed by removal of the jugular process isshown (green). The area exposed by the preauricular infratemporal approach is along the anterolateral edge of the foramen (solid black line) andremoval of the vaginal process of the tympanic part (black interrupted line) allows anterior transposition of the carotid artery and drilling of theanterior margin of the foramen. (B) Anterior view of the posterior face of a coronal section through the skull posterior to the right external acousticmeatus at the level of the white line shown in the insert in the upper corner of panel B. The infralabyrinthine mastoidectomy opens a wide areafrom the top of the dome to the lateral side of the jugular bulb (solid purple line in panel B). The cervical exposure provides access to the internaljugular vein below the foramen (interrupted purple line in panel B). The lateral suboccipital approach (retrosigmoid exposure) can access the jugu-lar foramen intracranially (orange circle area in panel B). A., artery; Ac., acoustic; CN, cranial nerve; Car., carotid; Cond., condyle; Int., internal; JF,jugular foramen; Jug., jugular; Mand., mandibular; Mast., mastoid; Meat., meatus; N., nerve; Occip., occipital; Pet., petrosal; Proc., process; Sig.,sigmoid; Stylomast., stylomastoid; V., vein.
APPROACHES TO JUGULAR SCHWANNOMAS
HEAD & NECK—DOI 10.1002/HED APRIL 2016 E1051

the presigmoid exposure, which allows minimum retrac-tion of the cerebellum, is a good option for removingtumors extending anteromedially or superiorly in the areabetween the acoustic meatus and jugular foramen.6,15,47
High cervical exposure will provide access to the areajust below the jugular foramen, but is often combinedwith the infralabyrinthine mastoidectomy and/or resectionof the jugular process for a tumor within the foramen thatextends downward into the high cervical area, or a pri-marily extracranial tumor that extends upward into theforamen. This combination, which includes the Kayeet al,7 Lambert et al,22 and Gardner et al17 approachesand was originally called the infralabyrinthine approach,can provide a wide exposure from the top of the jugularbulb to the neck (Figure 6B).
Jugular foramen schwannomas often involve severalregions; A1B, B1C, and D tumors. The reportedapproaches for type D tumors are combined approaches,which include the lateral suboccipital approach and cervi-cal exposure combined with infralabyrinthine mastoidec-tomy and/or jugular process resection.14,18,21,23,45 Almostall reported approaches added resection of the jugularprocess. However, previous studies have reported that thetranscondylar suprajugular approach with preservation ofthe wall of the jugular bulb usually results in preservationof its patency after tumor removal even if the preopera-tive studies revealed an absence of its flow into the jugu-lar bulb.6,56,57
Generally, an approach with modifications to widen thesurgical field is advantageous. Cervical exposure com-bined with an infralabyrinthine mastoidectomy and resec-tion of the jugular process can provide a wide surgicalfield that can be enlarged further through a variety ofmodifications, including the fallopian bridge techniquewithout translocation of the facial nerve, which providesmore surgical space and improves the visualization forthe tumor extending to the hypotympanum or anterolat-eral part of the jugular bulb. If the tumor extends intracra-nially, the retrosigmoid or presigmoid approach can beadded. If the tumor extends in the direction of the petrousapex and encases the petrous carotid, it may be necessaryto translocate the facial nerve after resecting the externalear canal as in Fisch’s type A infratemporal fossaapproach.11,12,41 If facial nerve translocation is needed,preserving the stylomastoid artery and a fascial cuffaround the facial nerve will aid in avoiding facial paraly-sis. However, the most effective way to preserve thefunction of the facial nerve is to avoid opening the facialcanal. If the schwannoma cannot be separated from thejugular bulb or internal jugular vein, sacrifice of the bulbafter ligation of both the sigmoid sinus and internal jugu-lar vein can be added to enlarge the surgical field if pre-operative studies show compromised flow through theforamen.
If a foraminal schwannoma extends anteriorly, a type Ainfratemporal fossa approach or preauricular subtemporalinfratemporal fossa approach can be used to expose theanterolateral aspects of the foramen. An endoscopic trans-nasal/transmaxillary transpterygoid approach may be con-sidered for tumors that extend to the infratemporal fossaand along the petrous portion of the internal carotid arterythrough the eustachian tube, or to the cancellous portion
of the petrous apex. However, the application of thisapproach is limited and should be considered only if thetumor occupies the infratemporal fossa and creates a sur-gical corridor by displacing the carotid artery and internaljugular vein posteriorly, and only minimum dissection ofthe pterygoid muscles is required.16,36,37 Foraminal andintracranial tumors with anterior extension are difficult toapproach. Sanna et al44 proposed that the type A infra-temporal fossa approach be combined with the transjugu-lar, transcondylar, and transtubercular extensions to treatFisch’s type C2 to C4 tympanojugular paraganglioma,with some technical refinements, which includes the ante-rior rerouting of the facial nerve creating a new bonycanal using fibrin glue, and the extraluminal compressionof the sigmoid sinus with Surgicel (Johnson & Johnson,Piscataway, NJ) as compared to the type A infratemporalfossa approach. This extension allows posteroinferior andmedial access in addition to the superior and anterolateralexposure of the foramen. Schwannomas rarely extendanteriorly with infiltration of the wall of the petrouscarotid artery. However, if the schwannoma expandsaggressively from the intracranial and foraminal areas tothe petrous apex along with the petrous carotid artery,this approach should be considered.
CONCLUSIONSelecting the best approach from among the numerous
reported approaches should be based on the preoperativeexaminations showing the size and location of thesetumors. Care should be taken to avoid injury to the CNs,because jugular foramen schwannomas are mostly benignand slow-growing and usually cause minimal CN deficits.A precise understanding of each approach and the com-plex anatomy involved of the jugular foramen is impor-tant in achieving complete removal of tumors whileminimizing risk.
AcknowledgmentsThe authors appreciate Ms. Robin Barry for assistancewith the preparation of the illustrations and Ms. JessicaStriley for editorial assistance.
REFERENCES1. Katz AD, Passy V, Kaplan L. Neurogenous neoplasms of major nerves of
face and neck. Arch Surg 1971;103:51–56.2. Ho KL. Schwannoma of the trochlear nerve. Case report. J Neurosurg
1981;55:132–135.3. Samii M, Babu RP, Tatagiba M, Sepehrnia A. Surgical treatment of jugular
foramen schwannomas. J Neurosurg 1995;82:924–932.4. Tan LC, Bordi L, Symon L, Cheesman AD. Jugular foramen neuromas: a
review of 14 cases. Surg Neurol 1990;34:205–211.5. Song MH, Lee HY, Jeon JS, Lee JD, Lee HK, Lee WS. Jugular foramen
schwannoma: analysis on its origin and location. Otol Neurotol 2008;29:387–391.
6. Kadri PA, Al-Mefty O. Surgical treatment of dumbbell-shaped jugularforamen schwannomas. Neurosurg Focus 2004;17:E9.
7. Kaye AH, Hahn JF, Kinney SE, Hardy RW Jr, Bay JW. Jugular foramenschwannomas. J Neurosurg 1984;60:1045–1053.
8. Mazzoni A, Sanna M, Saleh E, Achilli V. Lower cranial nerve schwan-nomas involving the jugular foramen. Ann Otol Rhinol Laryngol 1997;106:370–379.
9. Wilson MA, Hillman TA, Wiggins RH, Shelton C. Jugular foramenschwannomas: diagnosis, management, and outcomes. Laryngoscope 2005;115:1486–1492.
10. Pellet W, Cannoni M, Pech A. The widened transcochlear approach to jug-ular foramen tumors. J Neurosurg 1988;69:887–894.
11. Franklin DJ, Moore GF, Fisch U. Jugular foramen peripheral nerve sheathtumors. Laryngoscope 1989;99(10 Pt 1):1081–1087.
KOMUNE ET AL.
E1052 HEAD & NECK—DOI 10.1002/HED APRIL 2016

12. Fisch U, Pillsbury HC. Infratemporal fossa approach to lesions in the tem-poral bone and base of the skull. Arch Otolaryngol 1979;105:99–107.
13. Mazzoni A, Sanna M. A posterolateral approach to the skull base: thepetro-occipital transsigmoid approach. Skull Base Surg 1995;5:157–167.
14. Tedeschi H, Rhoton AL Jr. Lateral approaches to the petroclival region.Surg Neurol 1994;41:180–216.
15. Cinibulak Z, Krauss JK, Nakamura M. Navigated minimally invasive pre-sigmoidal suprabulbar infralabyrinthine approach to the jugular foramenwithout rerouting of the facial nerve. Neurosurgery 2013;73(1 Suppl Oper-ative):ons3–ons15.
16. Dallan I, Bignami M, Battaglia P, Castelnuovo P, Tschabitscher M. Fullyendoscopic transnasal approach to the jugular foramen: anatomic study andclinical considerations. Neurosurgery 2010;67(3 Suppl Operative):ons1–ons7; discussion ons7–ons8.
17. Gardner G, Cocke EW Jr, Robertson JT, Trumbull ML, Palmer RE. Com-bined approach surgery for removal of glomus jugulare tumors. Laryngo-scope 1977;87(5 Pt 1):665–688.
18. George B, Lot G, Tran Ba Huy P. The juxtacondylar approach to the jugu-lar foramen (without petrous bone drilling). Surg Neurol 1995;44:279–284.
19. Hakuba A, Hashi K, Fujitani K, Ikuno H, Nakamura T, Inoue Y. Jugularforamen neurinomas. Surg Neurol 1979;11:83–94.
20. Heros RC. Lateral suboccipital approach for vertebral and vertebrobasilarartery lesions. J Neurosurg 1986;64:559–562.
21. Kim CJ, Yoo SJ, Nam SY, Kim SY. A hearing preservation technique forthe resection of extensive jugular foramen tumors. Laryngoscope 2001;111(11 Pt 1):2071–2076.
22. Lambert PR, Johns ME, Winn RH. Infralabyrinthine approach to skull-baselesions. Otolaryngol Head Neck Surg 1985;93:250–258.
23. Liu JK, Sameshima T, Gottfried ON, Couldwell WT, Fukushima T. Thecombined transmastoid retro- and infralabyrinthine transjugular transcon-dylar transtubercular high cervical approach for resection of glomus jugu-lare tumors. Neurosurgery 2006;59(1 Suppl 1):ONS115–ONS125;discussion ONS115–ONS125.
24. Mann WJ, Amedee RG, Gilsbach J, Perneczky A, Wolfensberger M. Trans-sigmoid approach for tumors of the jugular foramen. Skull Base Surg 1991;1:137–141.
25. Nakamizo A, Akagi Y, Watanabe T, Kawahara N, Sasaki T. Posteriortransjugular and transcervical approach for glomus tumours within the headand neck. Br J Neurosurg 2013;27:212–217.
26. Oghalai JS, Leung MK, Jackler RK, McDermott MW. Transjugular crani-otomy for the management of jugular foramen tumors with intracranialextension. Otol Neurotol 2004;25:570–579; discussion 579.
27. Pensak ML, Jackler RK. Removal of jugular foramen tumors: the fallopianbridge technique. Otolaryngol Head Neck Surg 1997;117:586–591.
28. Sekhar LN, Schramm VL Jr, Jones NF. Subtemporal-preauricular infratem-poral fossa approach to large lateral and posterior cranial base neoplasms.J Neurosurg 1987;67:488–499.
29. Sen CN, Sekhar LN. An extreme lateral approach to intradural lesions ofthe cervical spine and foramen magnum. Neurosurgery 1990;27:197–204.
30. Seyfried DM, Rock JP. The transcondylar approach to the jugular foramen:a comparative anatomic study. Surg Neurol 1994;42:265–271.
31. Sasaki T, Takakura K. Twelve cases of jugular foramen neurinoma. SkullBase Surg 1991;1:152–160.
32. Wen HT, Rhoton AL Jr, Katsuta T, de Oliveira E. Microsurgical anatomyof the transcondylar, supracondylar, and paracondylar extensions of the far-lateral approach. J Neurosurg 1997;87:555–585.
33. Krause F. To expose the posterior temporal bone area and cerebellum [inGerman]. Bruns Beitr Klin Chir 1903;37:728–764.
34. Lanzino G, Paolini S, Spetzler RF. Far-lateral approach to the craniocervicaljunction. Neurosurgery 2005;57(4 Suppl):367–371; discussion 367–371.
35. Katsuta T, Rhoton AL Jr, Matsushima T. The jugular foramen: microsurgi-cal anatomy and operative approaches. Neurosurgery 1997;41:149–201;discussion 201–202.
36. Hofstetter CP, Singh A, Anand VK, Kacker A, Schwartz TH. The endo-scopic, endonasal, transmaxillary transpterygoid approach to the pterygopa-latine fossa, infratemporal fossa, petrous apex, and the Meckel cave.J Neurosurg 2010;113:967–974.
37. Lee DL, McCoul ED, Anand VK, Schwartz TH. Endoscopic endonasalaccess to the jugular foramen: defining the surgical approach. J NeurolSurg B Skull Base 2012;73:342–351.
38. Zhang W, Ye Y, Chen J, et al. Study on inferior petrosal sinus and its con-fluence pattern with relevant veins by MSCT. Surg Radiol Anat 2010;32:563–572.
39. Pensak ML, Friedman RA. Fallopian bridge technique in surgery forchronic ear disease. Laryngoscope 1997;107(11 Pt 1):1451–1456.
40. Hinsley ML, Hartig GK. Anatomic relationship between the spinal acces-sory nerve and internal jugular vein in the upper neck. Otolaryngol HeadNeck Surg 2010;143:239–241.
41. Fisch U, Fagan P, Valavanis A. The infratemporal fossa approach for thelateral skull base. Otolaryngol Clin North Am 1984;17:513–552.
42. Sen CN, Sekhar LN. The subtemporal and preauricular infratemporalapproach to intradural structures ventral to the brain stem. J Neurosurg1990;73:345–354.
43. Komune N, Komune S, Matsushima K, Rhoton AL Jr. Comparison of lat-eral microsurgical preauricular and anterior endoscopic approaches to thejugular foramen. J Laryngol Otol 2015;129 Suppl 2:S12–S20.
44. Sanna M, Shin SH, Piazza P, et al. Infratemporal fossa approach type awith transcondylar-transtubercular extension for Fisch type C2 to C4 tym-panojugular paragangliomas. Head Neck 2014;36:1581–1588.
45. Bruneau M, George B. The juxtacondylar approach to the jugular foramen.Neurosurgery 2008;62(3 Suppl 1):75–78; discussion 80–81.
46. Sanna M, Bacciu A, Falcioni M, Taibah A, Piazza P. Surgical managementof jugular foramen meningiomas: a series of 13 cases and review of the lit-erature. Laryngoscope 2007;117:1710–1719.
47. Hakuba A. Surgical anatomy of the skull base. Tokyo: Miwa Shoten; 1996.48. Borba LA, Ale-Bark S, London C. Surgical treatment of glomus jugulare
tumors without rerouting of the facial nerve: an infralabyrinthine approach.Neurosurg Focus 2004;17(2):E8.
49. Clemis JD, Noffsinger D, Derlacki EL. A jugular foramen schwannomasimulating an acoustic tumor with recovery of retrolabyrinthine cochleo-vestibular function. Trans Sect Otolaryngol Am Acad Ophthalmol Otolar-yngol 1977;84(4 Pt 1):ORL-687–ORL-696.
50. Neely JG. Reversible compression neuropathy of the eighth cranial nervefrom a large jugular foramen schwannoma. Arch Otolaryngol 1979;105:555–560.
51. Yamakami I, Nakamura T, Ono J, Yamaura A. Recovery of hearing afterremoval of a large jugular foramen schwannoma: report of two cases. SurgNeurol 1999;51:60–65.
52. Mazzoni A. The petro-occipital trans-sigmoid approach for lesions of thejugular foramen. Skull Base 2009;19:48–56.
53. Matsushima K, Kohno M, Komune N, Miki K, Matsushima T, Rhoton ALJr. Suprajugular extension of the retrosigmoid approach: microsurgicalanatomy. J Neurosurg 2014;121:397–407.
54. Takemura Y, Inoue T, Morishita T, Rhoton AL Jr. Comparison of micro-scopic and endoscopic approaches to the cerebellopontine angle. WorldNeurosurg 2014;82:427–441.
55. Matsushima T, Fukui M. Jugular foramen tumors (2) – suboccipital craniot-omy combined with infralabyrinthine approach trough mastoidectomy tothe jugular schwannomas. Hakuba A, Yamamura A, editors. In: Surgery ofCranial Base Standard and Modified Techniques [in Japanese]. Tokyo,Japan: IGAKU-SHOIN, Ltd; 1994. pp 331–336.
56. Bowles AP, Kinjo T, Al-Mefty O. Skull base approaches for posterior cir-culation aneurysms. Skull Base Surg 1995;5:251–260.
57. Arnautovic KI, Al-Mefty O. Primary meningiomas of the jugular fossa.J Neurosurg 2002;97:12–20.
APPROACHES TO JUGULAR SCHWANNOMAS
HEAD & NECK—DOI 10.1002/HED APRIL 2016 E1053





























