Embed Size (px)
Citation preview

SURGICAL APPROACHES TO CEREBELLOPONTINE ANGLE: A 17-year experience of our skull base team
Isabel Correia, MD1; Vítor Sousa, MD1,2; Luis Marques-Pinto, MD1,2; Victor Gonçalves, MD, PhD2,3; Ezequiel Barros, MD1
1Department of Otorhinolaryngology, Head and Neck Surgery; 2Skull Base Team; 3Department of Neurosurgery Centro Hospitalar de Lisboa Central, Lisbon, Portugal
INTRODUCTION DISCUSSION RESULTS
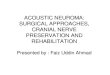
Table 1. Facial function results of patients with vestibular schwannoma who underwent extended RSM surgery. HB, House-Brackmann classification of facial function.
ABSTRACT
METHODS
CONCLUSIONS
REFERENCES
CONTACT
Objectives: We give an overview of the current state of cerebellopontine angle (CPA) surgery, based on the recent evidence, and describe our center experience in surgical approaches to these lesions. Methods: Retrospective review of cases who underwent surgery for CPA lesions at our hospital during the last 17 years (1996-2013), with focus on the description of the currently most used technique - extended retrosigmoid. Brief review of the literature on CPA surgery, comparing the different approaches, their indications and complications. Results: During this period, 203 patients underwent surgery of CPA. The most frequent indication was vestibular schwannoma (84.7%). Other indications were meningiomas (8.4%), epidermoids (1%), vestibular neurectomies (1.5%), arteriovenous malformations (1%), PICA/AICA aneurisms (1%), trigeminal microscopic decompression (0.5%), and other rarer tumors (2%). The most used approach was extended retrosigmoid (71.9%), followed by the translabirinthine (26.1%) and middle fossa approach (2%). Until 2004, the most used approach was the translabyrinthine; after 2004, the most used was the extended retrosigmoid. Conclusions: Currently, the preferred surgical approach used by our team is extended retrosigmoid, because it allows a complete exposition of sigmoid sinus from the transverse sinus to the jugular bulb, enhances CPA vision, avoids cerebellar retraction and is a simple way to get a wide route to the CPA. It also allows good functional outcomes (hearing and facial nerve preservation) in most cases. However, indications for approaches depend on the size of the lesion, its location and the quality of preoperative hearing, being necessary familiarity with all approaches.
Between 1996 and 2013, 203 patients underwent surgery of CPA. The most frequent indication was vestibular schwannoma (84.7%). Other less common indications are displayed in Chart 1. The most used approach was extended RSM in 71.9% of cases, followed by the TL and MF approaches (Chart 2). Until 2004, the most used approach was the TL; after 2004, the most used was the extended RSM. The main results of our patients with vestibular schwannoma who underwent extended RSM surgery were: o Preservation (House-Brackmann grade I-II) of their
long-term facial function (>1 year postoperative) in all cases except in the larger (Koos grade 4) tumors (Table 1).
o Hearing preservation in 47.5% of cases. o Complications:
• CSF leak (6.3%) • Persistent dizziness (5.1%) and headache (3.8%) • IX, X or XI nerve palsy (3.8%) • Meningitis (1.3%) • Cerebellar edema (1.3%) • Cerebellar hemorrhage with death (1.3%)
The resection of lesions in the CPA can be challenging due to surrounding neurovascular structures that have low tolerance for retraction.4 Approaches to this anatomical compartment include the standard RSM, TL and MF.1-6 Each of these techniques has its own set of indications, advantages and disadvantages.1,5,6 The extended RSM is a modification of the standard RSM, that results from a partial mastoidectomy that provides a complete exposition of sigmoid sinus from the transverse sinus to the jugular bulb, maximizing the surgeon´s working angle and avoiding cerebellar retraction. This allows for a maximal resection with minimal morbidity.2-4 This approach has been used in some centers of skull base surgery2-4, where good results and low complication rates have been described. The primary risk is of venous injury/congestion.4 It has been the most used approach in our center during the last decade (previously it was TL). The main reasons for this change are the possibility of hearing preservation, being faster, decreasing CSF fistula incidence and avoiding cerebellar retraction. This could also be the keypoint to the lower rates of postoperative headaches observed in our patients, comparing to those described for traditional RSM.1,5,6
Retrospective review of cases who underwent surgery for CPA lesions at our hospital during the last 17 years (1996-2013). These surgeries were performed by ENTs and neurosurgeons. Our currently most used technique is the extended RSM, described briefly below (Figures 1-3).
Currently, the preferred surgical approach used by our team is extended RSM, because: • It allows a complete exposition of sigmoid sinus
from the transverse sinus to the jugular bulb • Enhances CPA vision • Avoids cerebellar retraction • It is a simple way to get a wide route to the
CPA • It also allows good functional outcomes
(hearing and facial nerve preservation) in most cases
However, indications for approaches depend on the size of the lesion, its location and the quality of preoperative hearing, being necessary familiarity with all approaches.
About 10% of all intracranial tumors involve the cerebellopontine angle (CPA) and the vast majority of these are vestibular schwannomas, accounting for 70-90%.1 The most common surgical approaches to the CPA lesions are retrosigmoid (RSM), translabyrinthine (TL) and middle fossa (MF).1-6 The extended retrosigmoid is a simple and safe modification of the traditional RSM approach, that increases the exposure of the CPA and avoids cerebellar retraction.2-4 Such modification results from a limited mastoidectomy and skeletonization of the sigmoid sinus.
1. Springborg J, Thomsen J. Management of nonacoustic cerebellopontine angle tumors. In: Gleeson M. Scott Brown´s otorhinolaryngology, head and neck surgery, 7th ed. Edward Arnold; 2008: 4007-17.
2. Abolfotoh M, Dunn IF, Al-Mefty O. Transmastoid retrosigmoid approach to the cerebellopontine angle: surgical technique. Neurosurgery. 2013 Sep;73(1 Suppl Operative):ons16-23.
3. Quiñones-Hinojosa A, Chang EF, Lawton MT. The extended retrosigmoid approach: an alternative to radical cranial base approaches for posterior fossa lesions. Neurosurgery. 2006 Apr;58(4 Suppl 2):ONS-208-14.
4. Raza SM, Quiñones-Hinojosa A. The extended retrosigmoid approach for neoplastic lesions in the posterior fossa: technique modification. Neurosurg Rev. 2011 Jan;34(1):123-9.
5. Ansari SF, Terry C, Cohen-Gadol AA. Surgery for vestibular schwannomas: a systematic review of complications by approach. Neurosurg Focus. 2012 Sep;33(3):E14.
6. Chamoun R, McDonald J, Shelton C, Couldwell WT. Surgical approaches for resection of vestibular schwannomas: translabyrinthine, retrosigmoid, and middle fossa approaches. Neurosurg Focus. 2012 Sep;33(3):E9.
Isabel Araújo Marques Correia Centro Hospitalar Lisboa Central Email: [email protected] Phone: 00351-937148763
Figure 1. Intraoperative pictures of extended RSM surgical approach. A, supine or park bench position and head fixation with Mayfield. Skin incision 3 cm behind the pinna. B,C, exposure of bone and craniotomy with 3 burr holes united with a skull saw. D, ENT surgeon proceeds to mastoid dissection (with drill) and skeletonization of sigmoid sinus, until E, complete exposition of sigmoid sinus.
Figure 3. Dural flap suspension. A, the dura of the cisterna magna is opened, and CSF release allow a relaxation of the cerebellum and its displacement down by gravity. The dural flap suspended also includes the sigmoid sinus for B, an enhanced visualization of the CPA.
A B C
D E
Figure 2. Comparison between the area above the sigmoid sinus A, before and B, after its skeletonization with the bone drill, allowing complete exposition of sigmoid sinus. This is the difference between the traditional RSM and extended RSM.
A B
A B
Chart 2. Surgical approaches used in our hospital in the last 17 years.
Chart 1. Indications for cerebellopontine angle surgery. PICA, posterior inferior cerebellar artery; AICA, anterior inferior cerebellar artery.
MIDDLE FOSSA TRANSLABYRINTHINE RETROSIGMOID (standard)
Advantages
• Hearing preservation • Good access to internal
auditory canal
• Any size of tumor • Good facial nerve
preservation
• Hearing preservation • Any size of tumor • Good facial nerve
preservation
Disadvantages
• Limited access to CPA • Temporal lobe retraction • Limited to small lesions • Risk to facial nerve
• Invariably destroys residual hearing
• High incidence of CSF fistula
• Cerebellar retraction • Postoperative headache • High incidence of CSF
fistula
Tumor size (Koos classification)
Long-term functional results
HB I-II HB III-IV HB V-VI
Koos grade 1 100% 0% 0%
Koos grade 2 100% 0% 0%
Koos grade 3 100% 0% 0%
Koos grade 4 74.3% 18.0% 7.7%
Table 2. Comparison of the different approaches to the CPA.