Embed Size (px)
Citation preview

Surgery in Ulcerative Colitis Surgery in Ulcerative Colitis –– Indication and TimingIndication and Timing
Johan D SJohan D SööderholmderholmProfessor of SurgeryProfessor of SurgeryColorectal Surgery UnitColorectal Surgery UnitLinkLinkööping University, Swedenping University, Sweden
Surgery in Ulcerative colitisSurgery in Ulcerative colitis
•• Required in 30Required in 30––40% of cases40% of cases–– First year First year –– 10 %10 %–– Within 10 years Within 10 years –– 25 %25 %–– ~50 % of these as emergency cases~50 % of these as emergency cases
•• Combined attention colorectal surgeon Combined attention colorectal surgeon and gastroenterologist essential for and gastroenterologist essential for optimal patient outcomeoptimal patient outcome
•• See surgery as additional, See surgery as additional, not as not as ””failurefailure””

Indications for surgery in UCIndications for surgery in UC
1.1. Fulminant or acute colitis not responding to Fulminant or acute colitis not responding to medical therapymedical therapy
2.2. Chronic continuous diseaseChronic continuous disease• Impaired growth and/or delayed puberty
3.3. Dysplasia and/or cancerDysplasia and/or cancer
4.4. Reconstruction after previous surgeryReconstruction after previous surgery
Timing is always essentialTiming is always essential

Timing of different indications for Timing of different indications for surgerysurgery
1.1. Acute colitis Acute colitis –– timing over hourstiming over hours--daysdays2.2. Chronic continuous disease Chronic continuous disease –– timing over timing over
weeksweeks3.3. Dysplasia and/or cancer Dysplasia and/or cancer –– timing over weekstiming over weeks--
monthsmonths4.4. Reconstructive surgery Reconstructive surgery –– timing over lifetiming over life

1. Acute Severe Colitis1. Acute Severe Colitis
• Absolute indications for surgery:– Toxic megacolon– Perforation– Severe colorectal bleeding
• Relative indications:– Deterioration during medical therapy– Severe disease with no improvement during
first 5 days

1. Acute Severe Colitis1. Acute Severe Colitis
ECCO statement 5FECCO statement 5F• The response to intravenous steroids is best assessed objectively
(by stool frequency, CRP and abdominal radiography) on or about the third day [EL2b, RGB]. Surgical options should be considered and discussed at this stage or earlier.
• Second line therapy with either ciclosporin [EL1b, RG B], orinfliximab [EL1b, RG B] or tacrolimus [EL1b, RG B] will often be appropriate.
• If there is clinical deterioration colectomy is recommended. • If there is no improvement within a further 4–7 days, colectomy
should usually be recommended [EL5, RG D]. • Third line therapy may be considered at a specialist centre
Travis, Stange, Gassull et al for ECCO working group. European evidence-based Consensus on the management of ulcerative colitis: Current managementJournal of Crohn's and Colitis (2008) 2, 24–62
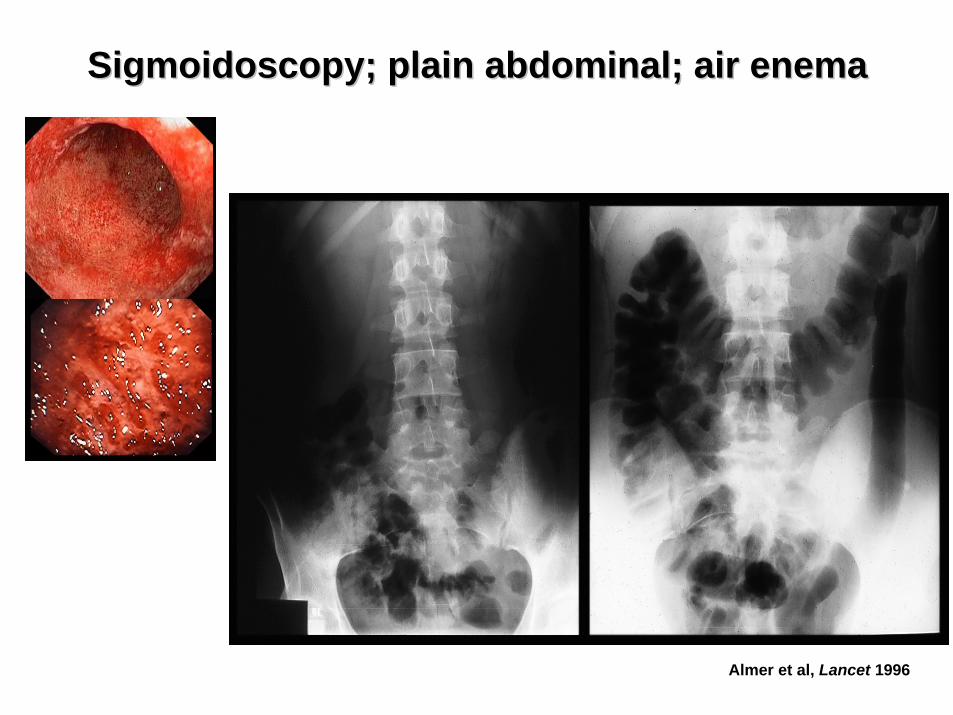
Sigmoidoscopy; plain abdominal; air enemaSigmoidoscopy; plain abdominal; air enema
Almer et al, Lancet 1996

Assessment of severityAssessment of severity
Truelove & Witts index.Truelove & Witts index.
Mild Moderate Severe
No. of haemorrhagic stools
<4 >4 if >6 and
Pulse <90 <90 >90 orTemperature <37.5oC <37.8 oC >37.8 oC orHaemoglobin >115 g/L >105 g/L <105 g/L orSR <20 mm <30 mm >30 mm oror CRP Normal <30 mg/L >30 mg/L
Sweden indexSweden index = number of daily stools + 0.14 x CRP (mg/L)• Index <8: 16% risk of colectomy • Index >8: 72% risk of colectomy within 30 days
Lindgren et al, Eur J Gastroenterol Hepatol 1998
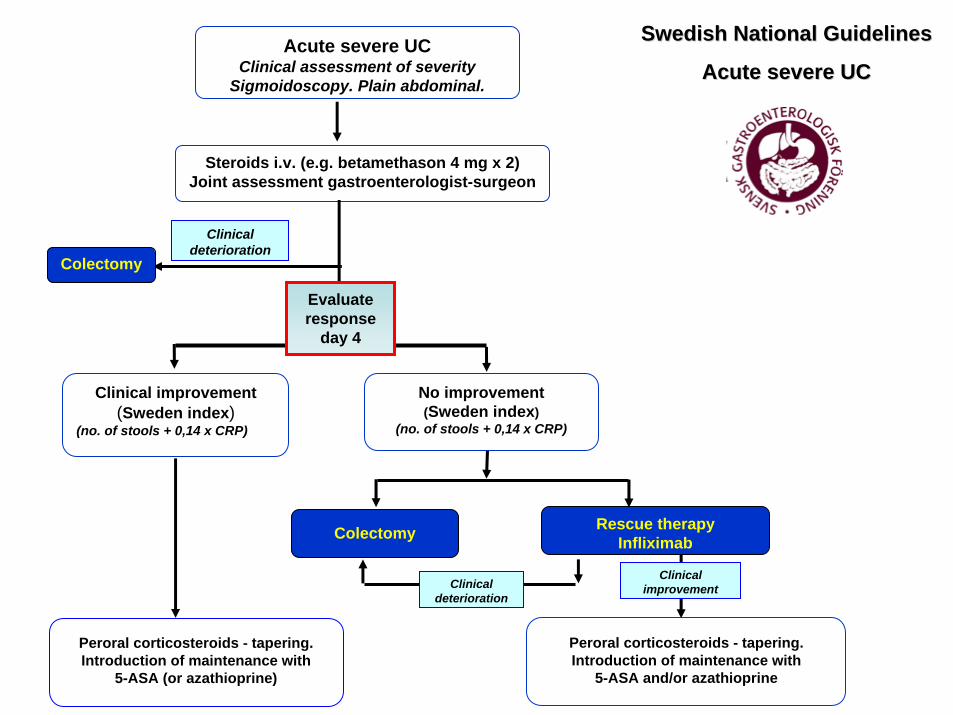
Clinical improvement (Sweden index)
(no. of stools + 0,14 x CRP)
No improvement (Sweden index)
(no. of stools + 0,14 x CRP)
Peroral corticosteroids - tapering.Introduction of maintenance with
5-ASA (or azathioprine)
Colectomy Rescue therapyInfliximab
Peroral corticosteroids - tapering.Introduction of maintenance with
5-ASA and/or azathioprine
Clinical improvement
Steroids i.v. (e.g. betamethason 4 mg x 2)Joint assessment gastroenterologist-surgeon
Clinical deterioration
Colectomy
Acute severe UCClinical assessment of severity
Sigmoidoscopy. Plain abdominal.
Clinical deterioration
Swedish National GuidelinesSwedish National Guidelines
Acute severe UCAcute severe UC
Evaluate response
day 4

Timing of surgery is crucialTiming of surgery is crucial• Medical therapy with i.v. corticosteroids and ciclosporin
for a total of 7–10 days not associated with increase in postoperative morbidity [Hyde et al, Dis Colon Rectum 2001]
• Possible to predict the need for urgent surgery after 3-4 days of medical therapy [Travis et al, Gut 1996; Lindgren et al, Eur J Gastroenterol Hepatol 1998]
• Early introduction of rescue therapy (ciclosporin or infliximab) encouraged: rapid response in >80% i.e. clear decision about surgery made within 7–10 days [Hancock et al, Colorectal Dis 2006]
1. Acute Severe Colitis1. Acute Severe Colitis

1. Acute Severe Colitis1. Acute Severe Colitis• Preferred operation in acute colitis:
Colectomy and ileostomy, with rectum left in situ.– Quick, safe and leaving all options for reconstruction– Suture rectum subcutaneously or ensure drainage of stump
©Copyright Science Press Internet Services
ECCO statement 7AECCO statement 7A (Travis et al, J Crohn’s Colitis 2008)• A staged procedure (colectomy first) is recommended in the acute
case when patients do not respond to medical therapy [EL 4, RG C]

Clinical improvement (Sweden index)
(no. of stools + 0,14 x CRP)
No improvement (Sweden index)
(no. of stools + 0,14 x CRP)
Peroral corticosteroids - tapering.Introduction of maintenance with
5-ASA (or azathioprine)
Colectomy Rescue therapyInfliximab
Peroral corticosteroids - tapering.Introduction of maintenance with
5-ASA and/or azathioprine
Clinical improvement
Steroids i.v. (e.g. betamethason 4mgx2)Joint assessment gastroenterologist-surgeon
Clinical deterioration
Colectomy
Acute severe UCClinical assessment of severity
Sigmoidoscopy. Plain abdominal.
Clinical deterioration
Swedish National GuidelinesSwedish National Guidelines
Acute severe UCAcute severe UC
Tysk Tysk et alet al 20092009
Evaluate response
day 4

©Copyright Science Press Internet Services
2. Chronic Continuous Colitis2. Chronic Continuous Colitis• Active disease despite optimized maintenance therapy• Often “steroid dependency”• High risk of septic complications; poor conditions for healing
(Lake et al, J Gastrointest Surg 2004; Aberra et al, Gastroenterology 2003)
• Optimize patient from nutritional and fluid balance point of view• Keep steroid dose at a minimum
•• ECCO statement 7AECCO statement 7A– A staged procedure (colectomy first) is recommended in the acute case when
patients do not respond to medical therapy [EL 4, RG C], or if a patient has been taking 20 mg or more of prednisolone for more than 6 weeks [EL 4, RG C]
• Subtotal colectomy + ileostomy• (important to consider rectal stump)
– Cures patient from burden of colitis– Regain of general health, normalise nutrition – Tapering of steroids– Time to consider options for reconstruction
(pouch, ileostomy, ileorectal)

3. Dysplasia/Cancer3. Dysplasia/Cancer
•• Indications for surgery must be clearly Indications for surgery must be clearly defined and verified in cases with defined and verified in cases with dysplasiadysplasia–– Often very little symptoms from their colitisOften very little symptoms from their colitis–– Surgery (proctocolectomy + IPAA) not without Surgery (proctocolectomy + IPAA) not without
complications and effects on QoLcomplications and effects on QoL–– LifeLife--long surveillance still neededlong surveillance still needed

3. Dysplasia/Cancer3. Dysplasia/Cancer•• Indications for surgery:Indications for surgery:
–– Cancer of the colon or rectumCancer of the colon or rectum–– HighHigh--grade dysplasia in flat mucosa grade dysplasia in flat mucosa –– LowLow--grade dysplasia grade dysplasia
associated with DALMassociated with DALM(Thomas, APT 2007; Odze, Mod Pathol 2002)
•• Diagnosed by 2 independent Diagnosed by 2 independent experienced GI pathologistsexperienced GI pathologists
•• Sporadic adenoma (with biopsySporadic adenoma (with biopsy--verified verified normal surrounding mucosa): polypectomynormal surrounding mucosa): polypectomy
•• LowLow--grade dysplasia in flat mucosa: grade dysplasia in flat mucosa: new colonoscopy after 3new colonoscopy after 3--6 months 6 months (Befrits R, DCR 2002; Lim, Gut 2003)
ECCO Statement 9JECCO Statement 9JHigh grade dysplasia in flat mucosa and adenocarcinoma are indications for proctocolectomy [EL2, RG B]. A patient with low-grade dysplasia in flat mucosa should be offered proctocolectomy or repeat surveillance biopsies within 3–6 months [EL2b, RG B]

3. Dysplasia/Cancer3. Dysplasia/Cancer•• Surgical techniqueSurgical technique
–– Proctocolectomy with total mesorectal excision Proctocolectomy with total mesorectal excision •• risk for nerve damagerisk for nerve damage
–– Mucosectomy with a handMucosectomy with a hand--sewn anastomosis? sewn anastomosis? –– DoubleDouble--stapled technique, leaving a rectal cuff?stapled technique, leaving a rectal cuff?
•• Functional outcome IPAAFunctional outcome IPAAhandhand--sewn vs. doublesewn vs. double--stapled stapled with inflammation in anal with inflammation in anal transitional zone transitional zone (Silvestri et al, (Silvestri et al, SurgerySurgery 2008)2008)(Lovegrove et al, Ann Surg 2006)(Lovegrove et al, Ann Surg 2006)

3. Dysplasia/Cancer3. Dysplasia/Cancer
•• Prospective followProspective follow--up stapled IPAA 10 years+, up stapled IPAA 10 years+, Cleveland Clinic: Cleveland Clinic: Cancer 0 %; Dysplasia 4.5 % Cancer 0 %; Dysplasia 4.5 % (Remzi et al, (Remzi et al, Dis Colon RectumDis Colon Rectum 2003)2003)
•• Systematic review: dysplasia in IPAA 1Systematic review: dysplasia in IPAA 1--2 % after 22 % after 2--16 years16 yearsSame frequency in pouch and cuffSame frequency in pouch and cuffSurveillance of pouch advocated after surgery for Surveillance of pouch advocated after surgery for cancercancer(Scarpa et al, Br J Surg 2007)(Scarpa et al, Br J Surg 2007)
•• Stapled or handStapled or hand--sewn?sewn?

4. Reconstructive Surgery4. Reconstructive Surgery

IPAA not perfect solutionIPAA not perfect solution•• Full continence day 65Full continence day 65--75%, night 3575%, night 35--45%45%•• Pouchitis: sporadic 50%, chronic 10% Pouchitis: sporadic 50%, chronic 10%
(St(Stååhlberg, hlberg, DCRDCR 1996)1996)
•• Failure (excision) 2Failure (excision) 2--13%13%
Ording Olsen et alGastroenterology 2002
4. Reconstructive Surgery 4. Reconstructive Surgery –– IPAAIPAA
It has been convincingly It has been convincingly demonstrated in three cohort demonstrated in three cohort studies that female fecundity or studies that female fecundity or fertility is reduced after IPAAfertility is reduced after IPAA
Time to pregnancy (months)60483624120
1.0
.8
.6
.4
.2
0.0
Before diagnosisBefore surgeryReference
Cumulative incidence of pregnancy
After surgery
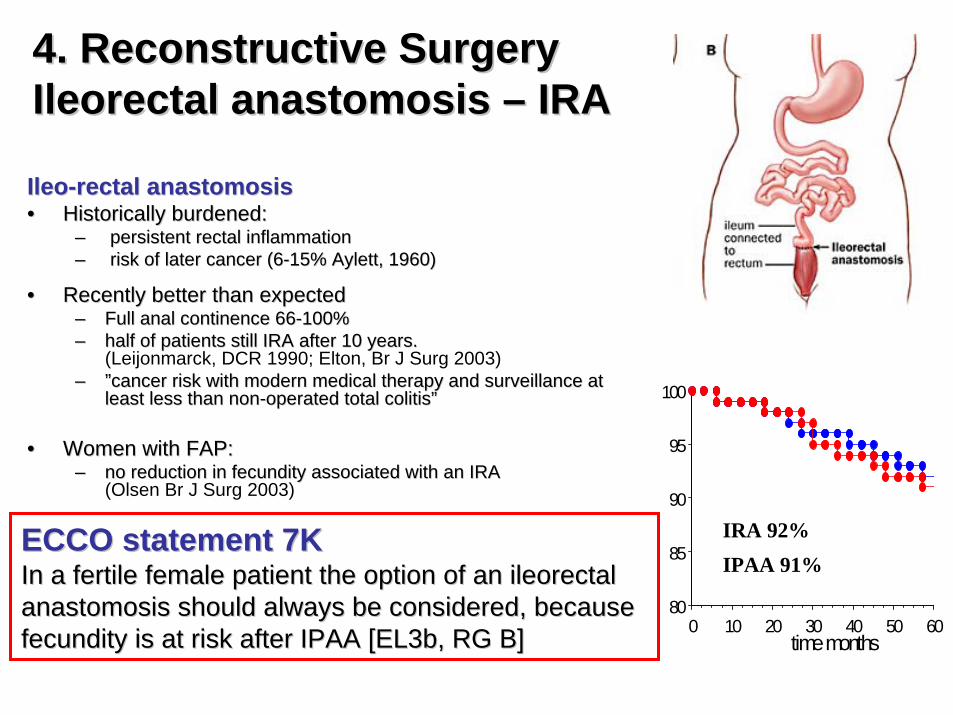
4. Reconstructive Surgery 4. Reconstructive Surgery Ileorectal anastomosis Ileorectal anastomosis –– IRAIRA
IleoIleo--rectal anastomosisrectal anastomosis•• Historically burdened:Historically burdened:
–– persistent rectal inflammationpersistent rectal inflammation–– risk of later cancer (6risk of later cancer (6--15% Aylett, 1960) 15% Aylett, 1960)
•• Recently better than expectedRecently better than expected–– Full anal continence 6Full anal continence 666--100%100%–– half of patients still IRA after 10 years. half of patients still IRA after 10 years.
(Leijonmarck, DCR 1990; Elton, Br J Surg 2003)–– ””cancer risk with modern medical therapy and surveillance at cancer risk with modern medical therapy and surveillance at
least less than nonleast less than non--operated total colitisoperated total colitis””
•• Women with FAP: Women with FAP: –– no reduction in fecundity associated with an IRA no reduction in fecundity associated with an IRA
(Olsen Br J Surg 2003)
•• Modification in practice, offering fertile female (and male?) Modification in practice, offering fertile female (and male?) patients an IRA, provided the rectum is not grossly inflamed, patients an IRA, provided the rectum is not grossly inflamed, with a view to later pouch surgery when the family is with a view to later pouch surgery when the family is complete.complete. 80
85
90
95
100
0 10 20 30 40 50 60time months
IRA 92%IPAA 91%
ECCO statement 7KECCO statement 7KIn a fertile female patient the option of an ileorectal In a fertile female patient the option of an ileorectal anastomosis should always be considered, because anastomosis should always be considered, because fecundity is at risk after IPAA [EL3b, RG B]fecundity is at risk after IPAA [EL3b, RG B]

Summary reconstructive surgerySummary reconstructive surgeryTechnique Pros Cons
IPAA Transanal defecationNo follow-up needed
PouchitisRisk for incontinenceFertility/dyspareunia
Impotence/retrogr. ejac.
Ileorectal anastomosis
Less effect sexual/fertilityGood anorectal function
Dysplasia/cancer riskFollow-up neededMedication needed
Ileostomy “Cured”Rectal stump issues
Ostomy problemsBody image
Sexual initiative
Kock pouch Less ostomy problemsNo follow-up neededImproved body image
Multiple revision surgeryRisk for pouchitis
4. Reconstructive Surgery 4. Reconstructive Surgery -- SummarySummary

4. Reconstructive Surgery4. Reconstructive Surgery•• Timing and relation to medicationTiming and relation to medication•• Cleveland Clinic experience 1991Cleveland Clinic experience 1991--2000 IPAA after acute colectomy2000 IPAA after acute colectomy
–– <3 months: higher incidence of intra<3 months: higher incidence of intra--operative complicationsoperative complications–– <6 months: more postoperative fistulas vs. >7 months<6 months: more postoperative fistulas vs. >7 months
(Dinnewitzer et al, (Dinnewitzer et al, Colorectal DisColorectal Dis 2006)2006)
•• Increased complication risk in IPAA performed after infliximab Increased complication risk in IPAA performed after infliximab treatment treatment (Holubar et al, (Holubar et al, F1000 Medicine ReportsF1000 Medicine Reports 2009)2009)
•• ECCO statement 7UECCO statement 7U• Pre-operative azathioprine does not increase the risk of postoperative
complications [EL3b, RG C]. Colectomy for ulcerative colitis immediately following or in the medium term after the use of ciclosporin appears to have no higher rate of postoperative complications [EL2b, RG D], while there are no sufficient data yet available for infliximab

In conclusionIn conclusion……
•• Surgery for ulcerative colitis with correct timing:Surgery for ulcerative colitis with correct timing:–– complimentary to medical treatment complimentary to medical treatment –– prevents complicationsprevents complications–– improves the patientsimproves the patients’’ quality of lifequality of life–– sometimes sometimes ““curativecurative””–– occasionally life savingoccasionally life saving
•• Close interaction betweenClose interaction betweengastroenterologist and surgeon gastroenterologist and surgeon key to optimized patient outcome key to optimized patient outcome over a lifeover a life--long perspectivelong perspective


4. Reconstructive Surgery 4. Reconstructive Surgery –– IPAAIPAA
• Diverting ileostomyCleveland Clinic experience:– Clinical leak: one-stage 14% vs. diverted 4% (Tjandra, Dis Colon
Rectum 1993)
– Overall complication rate for 1504 ileostomy closures: 11.4% (6% bowel obstr.) (Wong, Dis Colon Rectum 2005)
• Cannot prevent anastomotic complications, but mitigates potentially life-threatening complications (Williamsson et al, Dis Colon Rectum 1997)
•• ECCO statement 7FECCO statement 7FWhen performing a restorative proctocolectomy for ulcerative colitis a covering loop ileostomy is generally recommended, but it can be avoided in selected cases [EL 3b, RG C]

Laparoscopic technique for IPAA• Small non-randomized studies:
– Earlier return to bowel function; Shorter hospital stay; Improved cosmesis (Marcello, Dis Rectum Colon 2000; Dunker, Dis Colon Rectum 2001)
• Small randomized trial:– Similar complications rates; Functional outcomes no different from open
(Martense et al, Ann Surg 2004)
• The laparoscopic IPAA is a feasible and safe procedure. Short-term advantages of the laparoscopic approach seem to be limited and their clinical significance is arguable. (Ahmed Ali et al, Cochrane Reviews 2009)
4. Reconstructive Surgery 4. Reconstructive Surgery –– IPAAIPAA
• ECCO statement 7RLaparoscopic restorative proctocolectomy with an IPAA is a feasible operation; it gives shorter scars but there is no evidence for additional benefit to the patient [EL 2a, RG B]