Embed Size (px)
DESCRIPTION
Surgical Oncology
Citation preview
Page 1 of 7
Atienza, Austria, Balbin (09272265029), Bandoma, Bañez, Banico
Dr. Hipolito | March 6, 2014
SURGERY 3.4 Principles of Surgical Oncology 2013-2014 2nd
OUTLINE I. Carcinogenesis VI. Postoperative Management II. Cancer Metastasis VII. Principles of Chemotherapy III. Preoperative Planning VIII. Cancer Treatment Strategies IV. Intraoperative Conduct IX. Principles of Radiation Therapy of Operation V. Types of Cancer Operations X. On-going Trials in Cancer Therapy References: Powerpoint, recording
I. CARCINOGENESIS
Single cell (clonogenic origin) undergoes complex molecular and biochemical interactions resulting in malignant transformation. This means, a normal cell acquires potential to grow and replicate due to several factors (smoking, drinking, genetics/hereditary). Environmental and hereditary factors cause underexpression or overexpression of genes. Balance between the tumor suppressor genes and thos genes which causes cancer, oncogenes.
Interaction of cancer promoting genes (oncogenes) and cancer protecting genes (suppressor genes) o Overexpression of oncogenes + the effects of
environmental factors o Deletion/underexpression of suppressor genes (ex. P53)
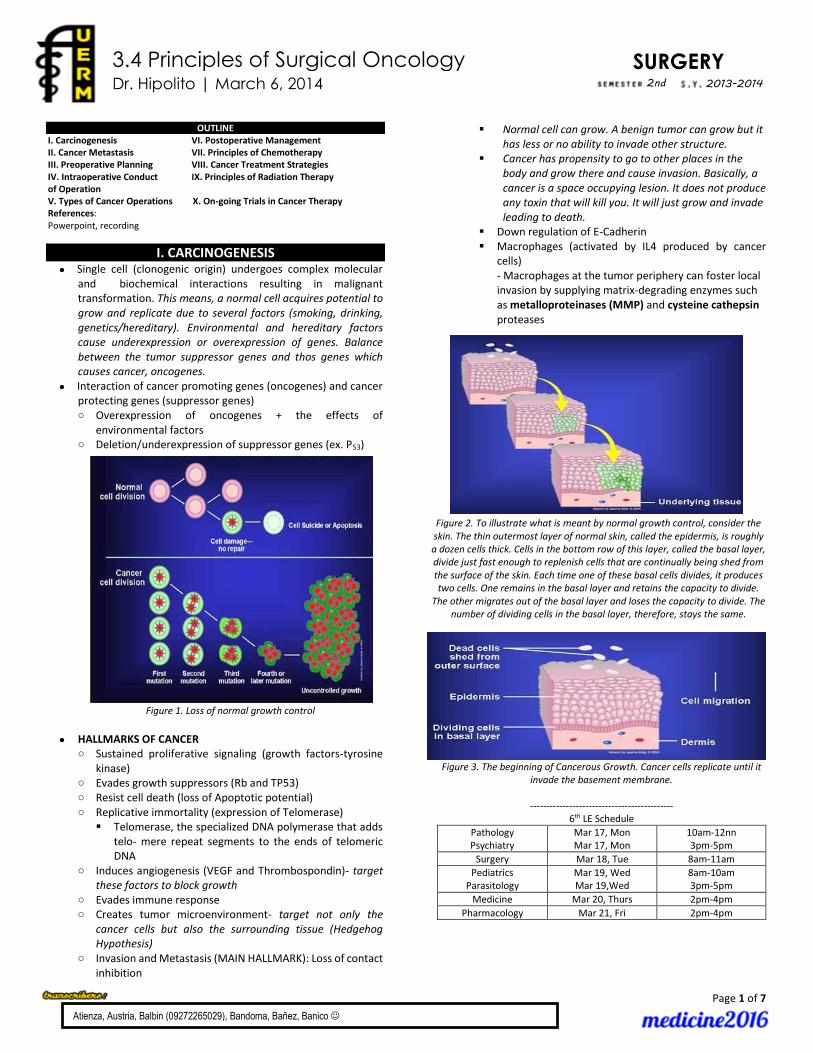
Figure 1. Loss of normal growth control
HALLMARKS OF CANCER o Sustained proliferative signaling (growth factors-tyrosine
kinase) o Evades growth suppressors (Rb and TP53) o Resist cell death (loss of Apoptotic potential) o Replicative immortality (expression of Telomerase)
Telomerase, the specialized DNA polymerase that adds telo- mere repeat segments to the ends of telomeric DNA
o Induces angiogenesis (VEGF and Thrombospondin)- target these factors to block growth
o Evades immune response o Creates tumor microenvironment- target not only the
cancer cells but also the surrounding tissue (Hedgehog Hypothesis)
o Invasion and Metastasis (MAIN HALLMARK): Loss of contact inhibition
Normal cell can grow. A benign tumor can grow but it has less or no ability to invade other structure.
Cancer has propensity to go to other places in the body and grow there and cause invasion. Basically, a cancer is a space occupying lesion. It does not produce any toxin that will kill you. It will just grow and invade leading to death.
Down regulation of E-Cadherin Macrophages (activated by IL4 produced by cancer
cells) - Macrophages at the tumor periphery can foster local invasion by supplying matrix-degrading enzymes such as metalloproteinases (MMP) and cysteine cathepsin proteases
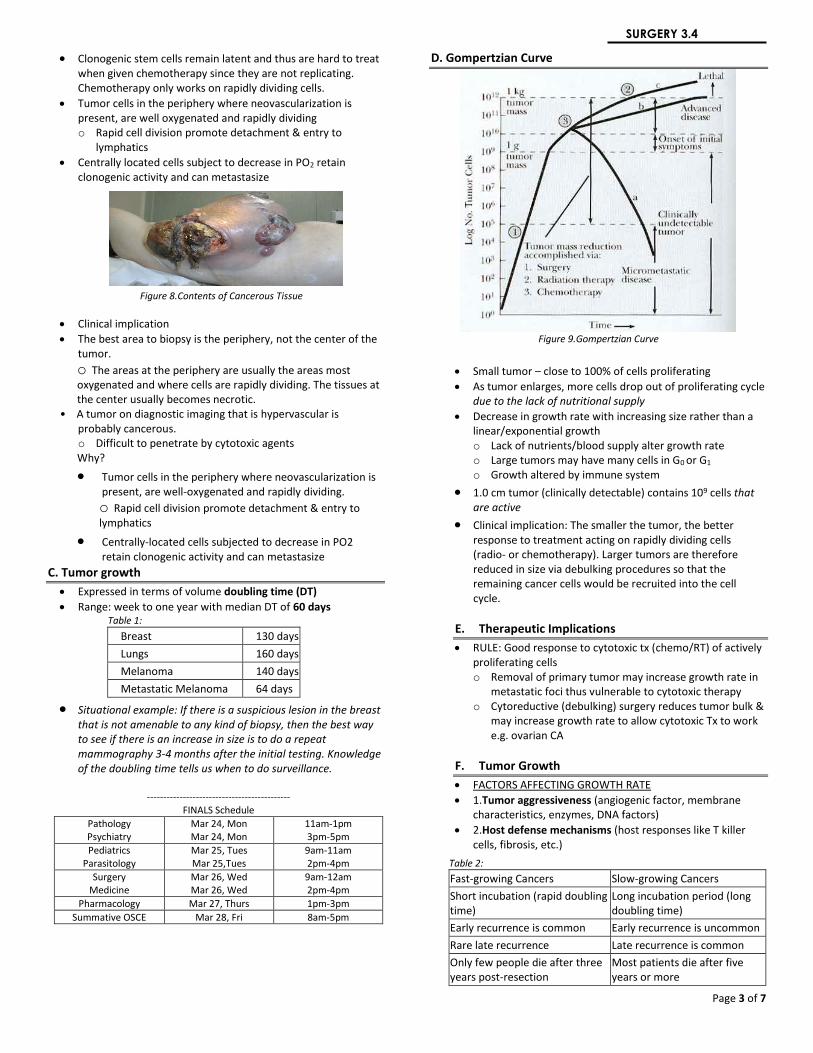
Figure 2. To illustrate what is meant by normal growth control, consider the skin. The thin outermost layer of normal skin, called the epidermis, is roughly a dozen cells thick. Cells in the bottom row of this layer, called the basal layer, divide just fast enough to replenish cells that are continually being shed from the surface of the skin. Each time one of these basal cells divides, it produces two cells. One remains in the basal layer and retains the capacity to divide.
The other migrates out of the basal layer and loses the capacity to divide. The number of dividing cells in the basal layer, therefore, stays the same.
Figure 3. The beginning of Cancerous Growth. Cancer cells replicate until it invade the basement membrane.
--------------------------------------------
6th LE Schedule
Pathology Psychiatry
Mar 17, Mon Mar 17, Mon
10am-12nn 3pm-5pm
Surgery Mar 18, Tue 8am-11am
Pediatrics Parasitology
Mar 19, Wed Mar 19,Wed
8am-10am 3pm-5pm
Medicine Mar 20, Thurs 2pm-4pm
Pharmacology Mar 21, Fri 2pm-4pm

Page 2 of 7
SURGERY 3.4
Figure 4. This gradual increase in the number of dividing cells creates a growing mass of tissue called a "tumor" or "neoplasm". If the rate of cell
division is relatively rapid, and no "suicide" signals are in place to trigger cell death, the tumor will grow quickly in size; if the cells divide more slowly, tumor growth will be slower. But regardless of the growth rate, tumors
ultimately increase in size because new cells are being produced in greater numbers than needed. As more and more of these dividing cells accumulate,
the normal organization of the tissue gradually becomes disrupted.
Figure 5.Invasion and Metastasis. When cancer cells reach the vascular supply and drainage, they are transported by the circulatory system to
distant sites
Figure 6. Distant
Metastasis
Example: o Thyroid Cancer (Papillary carcinoma of the thyroid) – most
common region of metastasis is the lymph node. Eventually, it will go to the lungs, and then bones
o Squamous Cell Carcinoma of the skin – doesn’t readily metastasize
FACTORS o Oncogenic viruses (ex. HSV/HPV & cerv CA) o Chemicals (ex. Smoking & lung CA) o Chronic irritation (ex. hyperkeratosis & oral cavity cancer) o Genetic factors (ex. BRCA1/BRCA2 & breast CA)
Note: Interplay of the factors will lead to cancer. Example, if you don’t have any gene that predisposes you to lung cancer, even if you smoke everyday, you will not have cancer. But if you have a gene for lung cancer caused by smoking, even one stick of smoke will trigger development of cancer.
CELL KINETICS – this tells the aggressiveness of the tumor, kind of treatment you want to initiate.
o G0 phase – State of cells not in the active cell cycle but capable of entering G1 upon stimulation.
o Gap 1 phase (G1) – period from mitosis to start of DNA synthesis.
o DNA Synthesis (S) o Gap 2 phase (G2) – period between DNA synthesis to next
mitotic phase. o Mitotic phase (M) – cell division seen morphologically.
A. Cell Cycle
Figure 7. The
Cell Cycle. In cancer cells, the stage of terminal differentiation is deleted. Most cancer cells
undergo G0 phase or the actively replicating phase (2014B trans). Gap 1 phase (G1) – Period from mitosis to start of DNA
synthesis
DNA synthesis (S)
Gap 2 phase (G2) – period between DNA synthesis to next mitotic phase
Mitotic phase (M) – cell division seen morphologically
Factors that prevent cells to go into G0 or latent phase (smoking, viruses, chronic irritation, etc)
Gap 1 phase (G1) – Period from mitosis to start of DNA synthesis
B. Cell kinetic
Intermitotic Time
Duration of 1 cell cycle to another cell cycle (ave. 8 – 24 hrs)
S phase (ave. 6 – 10 hrs)
Cells rapidly proliferating will have shorter intermitotic time
If a cancer has a very short intermitotic time, you are dealing with a very aggressive cancer; the doubling time decreases
C. Contents of Cancerous Tissues
Actively proliferating cells (clonogenic stem cells)
Non-actively proliferating cells but maintaining “clonogenic” capacity o Proliferation may have been inhibited by lack of nutrients
or other homeostatic factors Cells that have lost clonogenic capacity
Page 3 of 7
SURGERY 3.4
Clonogenic stem cells remain latent and thus are hard to treat when given chemotherapy since they are not replicating. Chemotherapy only works on rapidly dividing cells.
Tumor cells in the periphery where neovascularization is present, are well oxygenated and rapidly dividing o Rapid cell division promote detachment & entry to
lymphatics
Centrally located cells subject to decrease in PO2 retain clonogenic activity and can metastasize
Figure 8.Contents of Cancerous Tissue
Clinical implication
The best area to biopsy is the periphery, not the center of the tumor.
o The areas at the periphery are usually the areas most oxygenated and where cells are rapidly dividing. The tissues at the center usually becomes necrotic.
• A tumor on diagnostic imaging that is hypervascular is probably cancerous. o Difficult to penetrate by cytotoxic agents Why?
Tumor cells in the periphery where neovascularization is present, are well-oxygenated and rapidly dividing. o Rapid cell division promote detachment & entry to lymphatics
Centrally-located cells subjected to decrease in PO2 retain clonogenic activity and can metastasize
C. Tumor growth
Expressed in terms of volume doubling time (DT)
Range: week to one year with median DT of 60 days Table 1:
Breast 130 days
Lungs 160 days
Melanoma 140 days
Metastatic Melanoma 64 days
Situational example: If there is a suspicious lesion in the breast that is not amenable to any kind of biopsy, then the best way to see if there is an increase in size is to do a repeat mammography 3-4 months after the initial testing. Knowledge of the doubling time tells us when to do surveillance.
--------------------------------------------
FINALS Schedule
Pathology Psychiatry
Mar 24, Mon Mar 24, Mon
11am-1pm 3pm-5pm
Pediatrics Parasitology
Mar 25, Tues Mar 25,Tues
9am-11am 2pm-4pm
Surgery Medicine
Mar 26, Wed Mar 26, Wed
9am-12am 2pm-4pm
Pharmacology Mar 27, Thurs 1pm-3pm
Summative OSCE Mar 28, Fri 8am-5pm
D. Gompertzian Curve
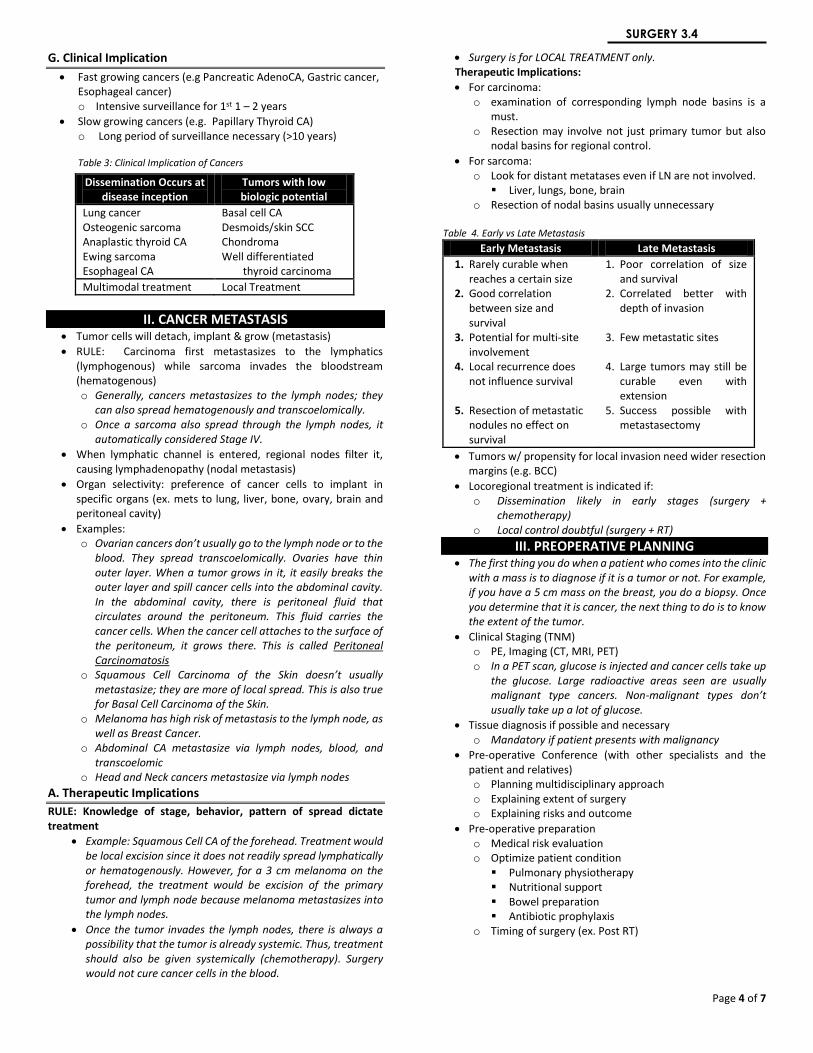
Figure 9.Gompertzian Curve
Small tumor – close to 100% of cells proliferating
As tumor enlarges, more cells drop out of proliferating cycle due to the lack of nutritional supply
Decrease in growth rate with increasing size rather than a linear/exponential growth o Lack of nutrients/blood supply alter growth rate o Large tumors may have many cells in G0 or G1 o Growth altered by immune system
1.0 cm tumor (clinically detectable) contains 109 cells that are active
Clinical implication: The smaller the tumor, the better response to treatment acting on rapidly dividing cells (radio- or chemotherapy). Larger tumors are therefore reduced in size via debulking procedures so that the remaining cancer cells would be recruited into the cell cycle.
E. Therapeutic Implications
RULE: Good response to cytotoxic tx (chemo/RT) of actively proliferating cells o Removal of primary tumor may increase growth rate in
metastatic foci thus vulnerable to cytotoxic therapy o Cytoreductive (debulking) surgery reduces tumor bulk &
may increase growth rate to allow cytotoxic Tx to work e.g. ovarian CA
F. Tumor Growth
FACTORS AFFECTING GROWTH RATE
1.Tumor aggressiveness (angiogenic factor, membrane characteristics, enzymes, DNA factors)
2.Host defense mechanisms (host responses like T killer cells, fibrosis, etc.)
Table 2:
Fast-growing Cancers Slow-growing Cancers
Short incubation (rapid doubling time)
Long incubation period (long doubling time)
Early recurrence is common Early recurrence is uncommon
Rare late recurrence Late recurrence is common
Only few people die after three years post-resection
Most patients die after five years or more
Page 4 of 7
SURGERY 3.4
G. Clinical Implication
Fast growing cancers (e.g Pancreatic AdenoCA, Gastric cancer, Esophageal cancer) o Intensive surveillance for 1st 1 – 2 years
Slow growing cancers (e.g. Papillary Thyroid CA) o Long period of surveillance necessary (>10 years)
Table 3: Clinical Implication of Cancers
II. CANCER METASTASIS
Tumor cells will detach, implant & grow (metastasis)
RULE: Carcinoma first metastasizes to the lymphatics (lymphogenous) while sarcoma invades the bloodstream (hematogenous) o Generally, cancers metastasizes to the lymph nodes; they
can also spread hematogenously and transcoelomically. o Once a sarcoma also spread through the lymph nodes, it
automatically considered Stage IV.
When lymphatic channel is entered, regional nodes filter it, causing lymphadenopathy (nodal metastasis)
Organ selectivity: preference of cancer cells to implant in specific organs (ex. mets to lung, liver, bone, ovary, brain and peritoneal cavity)
Examples: o Ovarian cancers don’t usually go to the lymph node or to the
blood. They spread transcoelomically. Ovaries have thin outer layer. When a tumor grows in it, it easily breaks the outer layer and spill cancer cells into the abdominal cavity. In the abdominal cavity, there is peritoneal fluid that circulates around the peritoneum. This fluid carries the cancer cells. When the cancer cell attaches to the surface of the peritoneum, it grows there. This is called Peritoneal Carcinomatosis
o Squamous Cell Carcinoma of the Skin doesn’t usually metastasize; they are more of local spread. This is also true for Basal Cell Carcinoma of the Skin.
o Melanoma has high risk of metastasis to the lymph node, as well as Breast Cancer.
o Abdominal CA metastasize via lymph nodes, blood, and transcoelomic
o Head and Neck cancers metastasize via lymph nodes
A. Therapeutic Implications
RULE: Knowledge of stage, behavior, pattern of spread dictate treatment
Example: Squamous Cell CA of the forehead. Treatment would be local excision since it does not readily spread lymphatically or hematogenously. However, for a 3 cm melanoma on the forehead, the treatment would be excision of the primary tumor and lymph node because melanoma metastasizes into the lymph nodes.
Once the tumor invades the lymph nodes, there is always a possibility that the tumor is already systemic. Thus, treatment should also be given systemically (chemotherapy). Surgery would not cure cancer cells in the blood.
Surgery is for LOCAL TREATMENT only. Therapeutic Implications:
For carcinoma: o examination of corresponding lymph node basins is a
must. o Resection may involve not just primary tumor but also
nodal basins for regional control.
For sarcoma: o Look for distant metatases even if LN are not involved.
Liver, lungs, bone, brain o Resection of nodal basins usually unnecessary
Table 4. Early vs Late Metastasis
Early Metastasis Late Metastasis
1. Rarely curable when reaches a certain size
2. Good correlation between size and survival
3. Potential for multi-site involvement
4. Local recurrence does not influence survival
5. Resection of metastatic nodules no effect on survival
1. Poor correlation of size and survival
2. Correlated better with depth of invasion
3. Few metastatic sites 4. Large tumors may still be
curable even with extension
5. Success possible with metastasectomy
Tumors w/ propensity for local invasion need wider resection margins (e.g. BCC)
Locoregional treatment is indicated if: o Dissemination likely in early stages (surgery +
chemotherapy) o Local control doubtful (surgery + RT)
III. PREOPERATIVE PLANNING The first thing you do when a patient who comes into the clinic
with a mass is to diagnose if it is a tumor or not. For example, if you have a 5 cm mass on the breast, you do a biopsy. Once you determine that it is cancer, the next thing to do is to know the extent of the tumor.
Clinical Staging (TNM) o PE, Imaging (CT, MRI, PET) o In a PET scan, glucose is injected and cancer cells take up
the glucose. Large radioactive areas seen are usually malignant type cancers. Non-malignant types don’t usually take up a lot of glucose.
Tissue diagnosis if possible and necessary o Mandatory if patient presents with malignancy
Pre-operative Conference (with other specialists and the patient and relatives) o Planning multidisciplinary approach o Explaining extent of surgery o Explaining risks and outcome
Pre-operative preparation o Medical risk evaluation o Optimize patient condition
Pulmonary physiotherapy Nutritional support Bowel preparation Antibiotic prophylaxis
o Timing of surgery (ex. Post RT)
Dissemination Occurs at disease inception
Tumors with low biologic potential
Lung cancer Osteogenic sarcoma Anaplastic thyroid CA Ewing sarcoma Esophageal CA
Basal cell CA Desmoids/skin SCC Chondroma Well differentiated
thyroid carcinoma
Multimodal treatment Local Treatment
Page 5 of 7
SURGERY 3.4
IV. INTRAOPERATIVE CONDUCT OF OPERATION 1. Determine stage during surgery (curability and resectability)
A tumor can be resectable but can no longer be cured
For example, a tumor in the colon has undergone multiple liver metastasis. The tumor in the colon can be resected but the patient cannot be cured.
2. Histologic confirmation if necessary 3. “En-bloc resection”
Nodal dissection not picking
Avoid tumor spillage 4. Attain tumor free margins
If you leave behind a single cancer cell in the operating field, there is always this possibility that the cancer cell will grow and replicate and recur. That is why you must do a wide excision, if possible.
Sarcoma: mandatory margins of resection is 5cm.
V. TYPES OF CANCER OPERATIONS 1. CURATIVE RESECTION (for Stages I, II, III)
o Resectable tumor & cure can be attained by surgery (e.g. radical resection)
2. CYTOREDUCTIVE SURGERY o Decrease tumor load prior to adjuvant therapy o Indicated if other effective therapies are available to control
residual disease o ex. Ovarian cancer - resection of bowel with infiltration to
prevent perforation during chemotherapy 3. DIAGNOSTIC SURGERY
o Biopsy to confirm diagnosis or histology of cancer
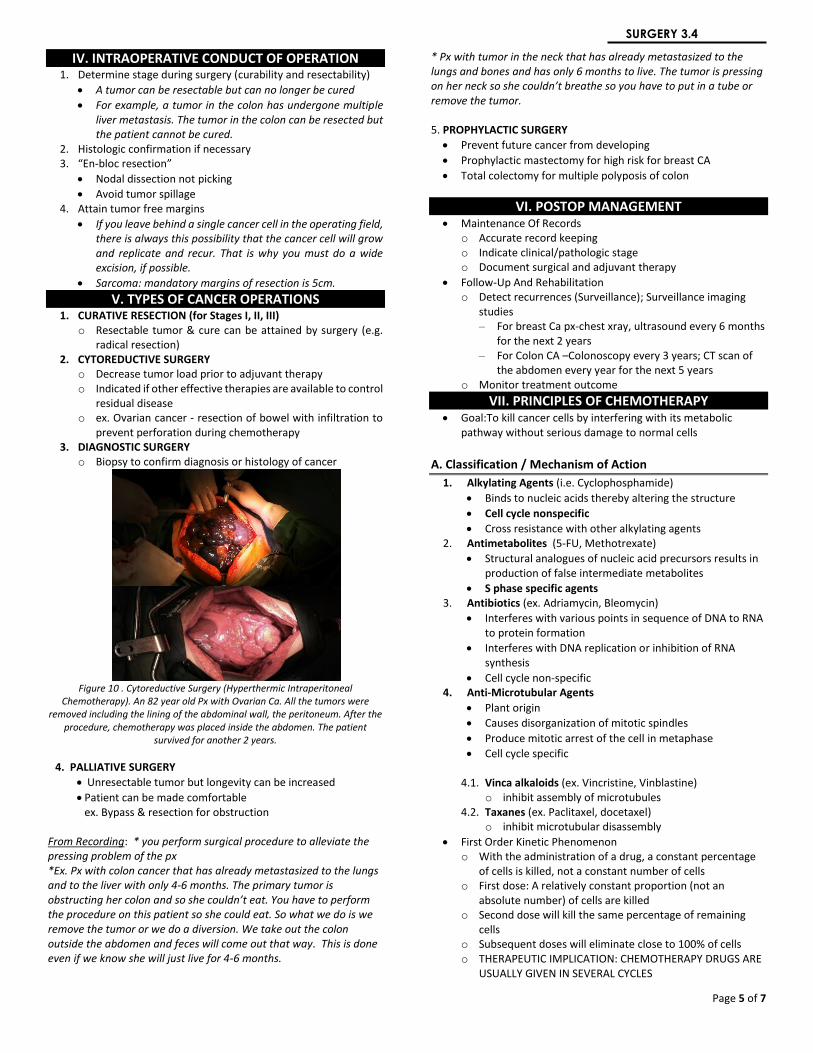
Figure 10 . Cytoreductive Surgery (Hyperthermic Intraperitoneal
Chemotherapy). An 82 year old Px with Ovarian Ca. All the tumors were removed including the lining of the abdominal wall, the peritoneum. After the
procedure, chemotherapy was placed inside the abdomen. The patient survived for another 2 years.
4. PALLIATIVE SURGERY
Unresectable tumor but longevity can be increased
Patient can be made comfortable ex. Bypass & resection for obstruction
From Recording: * you perform surgical procedure to alleviate the pressing problem of the px *Ex. Px with colon cancer that has already metastasized to the lungs and to the liver with only 4-6 months. The primary tumor is obstructing her colon and so she couldn’t eat. You have to perform the procedure on this patient so she could eat. So what we do is we remove the tumor or we do a diversion. We take out the colon outside the abdomen and feces will come out that way. This is done even if we know she will just live for 4-6 months.
* Px with tumor in the neck that has already metastasized to the lungs and bones and has only 6 months to live. The tumor is pressing on her neck so she couldn’t breathe so you have to put in a tube or remove the tumor. 5. PROPHYLACTIC SURGERY
Prevent future cancer from developing
Prophylactic mastectomy for high risk for breast CA
Total colectomy for multiple polyposis of colon
VI. POSTOP MANAGEMENT Maintenance Of Records
o Accurate record keeping o Indicate clinical/pathologic stage o Document surgical and adjuvant therapy
Follow-Up And Rehabilitation o Detect recurrences (Surveillance); Surveillance imaging
studies – For breast Ca px-chest xray, ultrasound every 6 months
for the next 2 years – For Colon CA –Colonoscopy every 3 years; CT scan of
the abdomen every year for the next 5 years o Monitor treatment outcome
VII. PRINCIPLES OF CHEMOTHERAPY Goal:To kill cancer cells by interfering with its metabolic
pathway without serious damage to normal cells
A. Classification / Mechanism of Action
1. Alkylating Agents (i.e. Cyclophosphamide)
Binds to nucleic acids thereby altering the structure
Cell cycle nonspecific
Cross resistance with other alkylating agents 2. Antimetabolites (5-FU, Methotrexate)
Structural analogues of nucleic acid precursors results in production of false intermediate metabolites
S phase specific agents 3. Antibiotics (ex. Adriamycin, Bleomycin)
Interferes with various points in sequence of DNA to RNA to protein formation
Interferes with DNA replication or inhibition of RNA synthesis
Cell cycle non-specific 4. Anti-Microtubular Agents
Plant origin
Causes disorganization of mitotic spindles
Produce mitotic arrest of the cell in metaphase
Cell cycle specific
4.1. Vinca alkaloids (ex. Vincristine, Vinblastine) o inhibit assembly of microtubules
4.2. Taxanes (ex. Paclitaxel, docetaxel) o inhibit microtubular disassembly
First Order Kinetic Phenomenon o With the administration of a drug, a constant percentage
of cells is killed, not a constant number of cells o First dose: A relatively constant proportion (not an
absolute number) of cells are killed o Second dose will kill the same percentage of remaining
cells o Subsequent doses will eliminate close to 100% of cells o THERAPEUTIC IMPLICATION: CHEMOTHERAPY DRUGS ARE
USUALLY GIVEN IN SEVERAL CYCLES

Page 6 of 7
SURGERY 3.4
o Side Effects - Vomiting - Hair loss - Depressed immunity
- Weakness/anorexia - Anemia - Organ specific (cardiac,
liver, kidney)
B. Therapeutic Implication
Intermittent Therapy (rationale) o Allow recovery of immune system (2-3 weeks) o Allows recovery of DNA damage in normal cells which is
faster than cancer cells o Destruction of cancer cells by blocking DNA synthesis in
actively proliferating cancer cells o Better effect than continous therapy
Combination of Drugs o More effective tumor kill o Less complications o Provides maximum cell kill within the range of toxicity for
each that can be tolerated by the host o Offers a broader range of coverage of resistant cell lines in
a heterogenous population o Prevents or delays the emergence of drug resistance cell
lines. o Drugs known to be active as single agents usually are
selected o Drugs with different mechanisms of actions are combined
to allow for additive or synergestic effects. Drugs with differing dose-limiting toxic effects are also combined to allow for each drug to be given at therapeutic does. Same goes with different patterns of resistance to avoid cross-resistance.
o Combining cell-cylce specific and cell-cycle-nonspecific agents are especially advantageous.
o Treatment-free interval between cycles is kept to the shortest possible time that will allow for recovery of the most sensitive normal tissue.
“Sometimes chemotherapy is given prior to surgical procedure and monitor the response. That’s the best way to see if there is any response.”
“80% of the time, if you give chemo before surgery for breast CA, then palpate it after some time, no tumor can be felt even with imaging, even if you did biopsy of breast and have it examined under the microscope, there are still some viable cancer cells, so you really need to remove the breast, then there’ll be no more viable cancer cells. That is complete pathological response” “There is no difference in prognosis/survival if even if reduced to very few cancer cells or 50% of total reduction after chemotherapy.” “Complete pathological response will have a better chance of survival compared to those who only have complete clincal response”
VIII. CANCER TREATMENT STRATEGIES
Neoadjuvant Therapy o Down stage/shrink tumor and convert the procedure from
total removal of the organ to just removal of the tumor itself
o Allow curative resection o Test response to cytotoxic therapy o Prior to surgery
Adjuvant Therapy o Given in addition to primary treatment o Eradicate microscopic CA cell not removed by primary
treatment o Prevent distant mestastasis/local recurrence o After surgery
Palliative chemotherapy (won’t be on the exam) o Incurable disease but death not imminent o Can significantly prolong life and improve quality of life o Patient must have good performance status o Treatment is given out of guilt o Patients usually just experience the drug side effects
Targeted Therapy o Newest form of cytotoxic therapy o Blocks the growth of cancer cells by interfering with
specific targeted molecules needed for carcinogenesis and tumor growth
o Targets the processes (or marker) invovled in tumor growth
o Rather than by simply interfering with rapidly dividing cells (traditional chemotherapy)
o More effective, less harmful, more expensive than chemotherapy
o Types of targeted therapy: o Small molecules
- Gefitinib: targets EGF receptor tyrosine kinase, for lung CA and some solid tumors
- Imatinib for CML, GIST - Tamoxifen: targets estrogen receptors of breast
cancer. But not all breast tumors have estrogen receptors, just only 70%
- Aromatase inhibitors: blocks formation of estrogen, includes those estrogen from fat and adrenals
o Monoclonal Antibodies - Trastuzumab: targets HER2/neu receptor of breast CA
IX. PRINCIPLES of RADIATION THERAPY A. Radiation Therapy (RT)
A local (non-systemic) effect
Affects cells by interfering with reproduction and mitosis
Affects rapidly dividing cells
Aims to effect maximal damage to cancer cells but allows recovery of normal cells
Just like surgery, only for local control of tumor
Uses ionizing radiation
Radiation deposition results in DNA damage manifested by breaks in the strand in the sugar phosphate backbone of the DNA
Manifests primarily by loss of cellular reproductive integrity. Most cell types do not show signs of radiation damge until they attempt to divide, so slowly proliferating tumors may persist for months and appear viable. Some cell types undergo apoptosis.
PRINCIPLES OF CHEMOTHERAPY
Response
1. Complete
2. Partial
3. None
4. Progression
Criterion
1. Complete disappearance
2. ≥ 50% reduction in T size
3. < 50% reduction in T size
4. > 50% increase in total
measurable disease
Criteria for objective response for
clnically measurable tumors
Page 7 of 7
SURGERY 3.4
B. Factors affecting Radiosensitivity
Oxygen Tension (work best in high oxygen tension) o Necrotic tumors – decrease O2 tension-resistant o Anemic patients – decrease O2 carrying hgb-resistant o Work best if with high oxygen tension. Radiotherapy needs
higher oxygen cause it will cause overproduction of free radicals which will cause damage to the DNA structure of the cancer cell. Repair mechanisms of cancer cells inhibited and thus death of cancer cell.
o Hypoxic cells are significantly less radiosensitive than aerated cells because presence of oxygen is thought to prolong the half life of free radicals
o Indirectly ionizing radiation is less efficacious in tumors with areas of hypoxia. In contrast, radiation damage from directly ionizing radiation is independent of cellular oxygen levels.
o The extent of DNA damage from indirectly ionizing radiation is dependent on the phase of cell cyle. The most radiation sensitive phases are G2 and M.
Fractionation o Redistribution o Re-oxygenation o work best in fractionation, little by little so that a small
amount of cancer cells die, and group will progress to dividing stage, then give another dose of radiation. It gives better results in survival and less recurrence and less adverse effects
C. Curative Role of RT
SCC of the Head & Neck (Early)
Cervix CA
Lymphoma 1. PRE-OP RT (intact blood supply)
• Reduction of tumor size (ex. Rectal cancer, neoadjuvant radiotherapy)
• Decreases recurrence 2. POST-OP RT
• For bulky or aggressive tumors – Positive margins
• Decreases recurrence
D. Combined Radiotherapy and Chemotherapy
Chemotherapy is prior to radiotherapy
Sensitize tumor cells to RT effects
For advanced head & neck and rectal cancer
E. Types of RT
1. External
X-ray
Gamma beam
Particle beam
Intensity Modulated Radiation Therapy (IMRT) 2. Interstitial radiation (brachytherapy)
Recurrences after external RT
Unresectable cancers 3. Intracavitary (Uterine Cervix Ca)
Insertion of radium packed tubes inside the cavity 4. Systemic RT
I131 – Thyroid Ca
Phosphorus 32 – bone metastasis
X. ON-GOING TRIALS IN CANCER THERAPY Genetic & Molecular Medicine
Stem Cell Therapy TYPES: 1. Remove normal cell then give high dose chemotherapy. When the body’s system is down (supper suppressed bone marrow), the stem cell it put back and reproduce normal cells. 2. Dendritic Cell Therapy. Get cancer cell and macrophage. Label (tattoo) the macrophage that would detect the tumor cell (tumor marker). Place the macrophage back to the system, that macrophage would produce antibodies that hopefully would recognize the cancer cells. Downside, not enough scientific evidence that it works with solid tumors.
IMMUNOTHERAPY 1. Dendritic cell therapy 2. Nanotechnology in Medicine-we put a device inside blood/system, give treatment and see if the treatment is working. Nanoscale devices smaller than human cells (10,000 to 20,000 nanometers in diameter) and organelles and similar in size to large biological macromolecules such as enzymes and receptors ex: Hemoglobin is approximately 5 nm in diameter, while the lipid bilayer surrounding cells is on the order of 6 nm thick. Nanoscale devices smaller than 50 nanometers can easily enter most cells, while those smaller than 20 nanometers can transit out of blood vessels.
SURGICAL ONCOLOGY – not all about techniques! • Understanding the behavior of cancer according to the
molecular biology, natural history and its response to treatment applied under the concept of multidisciplinary approach.
“THE ONLY PREPARATION FOR TOMMORROW
IS THE RIGHT USE OF TODAY”
“So be strong and courageous! Do not be afraid and do not panic before them.
For the LORD your God will personally go ahead of you. He will neither fail nor
abandon you.”- Deuteronomy 31:6





























