Embed Size (px)
Citation preview

Commentary
Sunscreens: sense and sensibility
Rik Roelandts, MD, PhD
From the Photodermatology Unit, Department of Dermatology, University Hospital, Leuven, Belgium
CorrespondenceRik Roelandts, MD, PhD, Photodermatology Unit, Department ofDermatology, University Hospital, Kapucijnenvoer 33, 3000 Leuven,Belgium
There has been an important evolution in sun protectionover the last 20 years. The general public is now muchmore aware of the short- and long-term adverse effects ofexcessive sun exposure, and so is more motivated to usesunscreens than ever before. The sunscreens now availablegenerally have much higher sun protection factors (SPFs)than previously, and have evolved from the provision ofmerely UVB protection to giving much broader UVB–UVAprotection. People have started to use sunscreens to protecttheir skin not only against sunburn, but also againstphotodermatoses, such as polymorphous light eruption,and against the long-term adverse effects of sun exposure,such as skin aging and skin cancer. All of these effects aremainly or partly UVA induced. Thus, sun protection hasbecome a more complicated matter than it used to be.
Sun protection factor (SPF)
The usual way of obtaining an idea about the protectivevalue of a sunscreen is by looking at its SPF number;however, the real SPF of a sunscreen may be lower thananticipated, because people actually seem to applyapproximately 0.5–1 mg/cm2 of sunscreen, while 2 mg/cm2
is used to determine the SPF.1 In addition, there can be alarge variation in the SPF value of the same sunscreen fromone person to another, and the claimed SPF is only theaverage value. Differences between the actual SPF and thetheoretical SPF can be due to many other factors, such asan uneven distribution of the filters in the applied filmand their spectral stability, the rubbing technique used inapplying the product and the unevenness of its application,the thickness of the layer applied, the nature of the lightsource and its filters, the method used to determine theerythemal response, the skin type of the patient, andswimming or sweating.
Sunscreens are being marketed with ever higher SPFvalues, which are possible by the use of higher concentra-tions of filters or combinations of different filters in the
© 1998 Blackwell Science Ltd International Journal of Dermatology 1998, 37, 729–732
729
same sunscreen; this can increase the risk of irritation orcontact dermatitis. Testing a sunscreen with a high SPFvalue becomes more difficult, because of the long irradiationtime needed and the accompanying interference effects ofother wavelengths. In addition, the sun protection of asunscreen is not a linear function of its SPF: for example,a sunscreen with SPF 15 will block 93% of the UV and asunscreen with SPF 30 only 97%.2 All of these dataillustrate how deceptive the SPF value may be as a parameterfor indicating protection against erythema or sunburn.
Protection
Although we now have the technical capability to protectour skin more effectively than ever before against erythemaand many other adverse effects of sun exposure, this doesnot mean that our skin is indeed better protected. With theevolution of sunscreen technology, a new problem hasarisen that can be called sun protection euphoria: a falsefeeling of security may be given. The protective value of asunscreen has always been based on the protection itprovides against erythema, which is indicated by its SPFvalue; however, it would be wrong to conclude that nothingcan happen to one’s skin when a sunscreen with a highSPF is used. Even if a single application of a sunscreenwith a high SPF were enough to protect one’s skin fromsunburn during a day’s sun exposure, it would not beenough to protect against other UV-induced effects. Evenif erythema is prevented, metabolic changes, as well as skindamage, may still occur.3 The prevention of erythema andthe notional SPF are therefore only partial markers for sunprotection. To prevent local or to decrease systemic UVB-induced suppression of contact hypersensitivity in humanskin, a sunscreen is needed that provides more than ninetimes the protection required to prevent erythema.4
Misconception
A common misunderstanding is that the skin is protectedagainst the development of skin cancers as long as no

730 Commentary When a burn is not a burn Stewart
erythema or no sunburn reaction develops. This could givea false feeling of security, especially if one changes one’ssun exposure habits. Many people may use sunscreens witha high SPF only so that they can prolong the time theyspend in the sun. Thus, the use of sunscreens couldhave an inverse effect and even increase the exposure todangerous amounts of UVA. This is not generally realized.The appropriate use of a sunscreen involves more than justthe application of a cosmetic onto the skin in the summer.If sunscreens are meant to protect the skin against thelong-term adverse effect of sun exposure, they should beused regularly from infancy onwards, and should not belimited to vacation periods, as seems to be the case inpractice. With this in mind, sunscreens should be sold withguidelines on how to use them. The guidelines shouldexplain to the user how to apply the sunscreen on time, insufficient quantities, and with sufficient regularity, and todo this not only when sunbathing. It should clearly urgethe user not to change his or her sun exposure habitsbecause of the sunscreen, and should list the limitationsand risks that may be encountered should one do so. It
Commentary
When a burn is not a burn
Thomas P. Stewart, PhD
From the Department of Clinical Affairs, Gaymar Ind. Inc.
CorrespondenceThomas P. Stewart, PhD, 10 Centre Drive, Orchard Park, NY 14127
Do you know a burn when you see one? Don’t be so sure!Many of us are called on from time to time to act as an
expert witness or called in on a consultation. What couldbe more natural than asking a dermatologist to give experttestimony and render expert opinion on skin lesions? Thereis one group of patients in which the skin lesion presentsas a severe ‘‘burn,’’ and your knowledge of causation andpowers of deduction will be severely tested. I am referringto the surgical patient who comes through surgery withflying colors only to be found to have suffered an iatrogenic‘‘burn.’’ There are many references to ‘‘burns’’ which occurin the operating room.
If you run into a case of an iatrogenic burn occurringduring surgery, I hope that, from this day forward, the
International Journal of Dermatology 1998, 37, 729–732 © 1998 Blackwell Science Ltd
should give directions on how to use the sunscreen fordifferent indications. Even if all this information wasprovided, the SPF would still have only a relative value,because it would differ depending on the purpose for whichthe sunscreen was used. Ideally, the SPF value of a sunscreenshould be determined as a function of the indication forwhich it is used.
References
1 Stenberg C, Larko O. Sunscreen application and itsimportance for the sun protection factor. Arch Dermatol1985; 121: 1400–1402.
2 Kaminester LH. Current concepts. Photoprotection. ArchFam Med 1996; 5: 289–295.
3 Pearse AD, Marks R. Response of human skin toultraviolet radiation: dissociation of erythema andmetabolic changes following sunscreen protection.J Invest Dermatol 1982; 78: 181–189.
4 Whitmore SE, Morison WL. Prevention of UVB-inducedimmunosuppression in humans by a high sun protectionfactor sunscreen. Arch Dermatol 1995; 131: 1128–1133.
combination of the terms ‘‘burn’’ and ‘‘surgery’’ will atleast raise a suspicion in your mind that will immediatelycaution you not to jump to conclusions. If a flammableanesthetic, a spark or actual flames were present when thepatient received his/her injury, you may be justified insuspecting a burn. This is not a circumstance to which youshould be hesitant about rendering an opinion. The injuriesthat I wish to draw attention to are mysterious ‘‘burn-like’’lesions, which are not discovered until after surgery iscomplete. No witnesses are available to confirm that theburn occurred. A number of papers and, indeed, an entirebook have been written about this topic,1–5 but, nonethe-less, misunderstanding and misdiagnosis persist. Let medescribe a typical case.

Stewart When a burn is not a burn Commentary 731
Illustrated case
A patient is brought to surgery for a cardiac or cardiovas-cular procedure. The surgery in many instances requiresthe use of cardiopulmonary bypass or cross-clamping ofthe aorta. The patient may have a history of peripheralvascular disease, diabetes, or other problems with perfusion(or vascular insufficiency). The surgical procedure is long(.3 h). The ‘‘burn-like’’ injury is not found until after theconclusion of the procedure (in many instances, hours afterthe procedure). The patient presents with an injury usuallybelow the waist, which is not discovered until he/she is inthe recovery room or the intensive care unit (ICU). Inaddition to cardiopulmonary bypass, the patient waswarmed with a water-circulating hypothermia machine andblanket, and electrocautery was used extensively duringthe procedure. The patient was maintained in the lateralrecumbent position (supine) during the procedure.
The site of the injury is always at a location at whichthe body was in contact with the operating table pad.
Theories
The surgical team has completed numerous, similar caseswithout incident. The lesion is diagnosed as a ‘‘burn’’ bythe first physician called in to diagnose and treat it. Aninvestigation immediately ensues to find the source of this‘‘burn’’ and, as the patient was most recently in theoperating room, the attention quickly focuses there. Withthe diagnosis of a ‘‘burn,’’ attention is quickly brought tofocus on those items that may be a source of heat. Theelectrocautery machine and hypothermia machine are primesuspects. If convective warming was used, then this is alsoa prime suspect. During the course of the investigation,none of this equipment is found to have malfunctionedand all has tested within the manufacturer’s specifications(by the Biomedical Engineering Department). As no sourceof heat sufficient to burn is found, theories are advancedas to how the ‘‘burn’’ could have occurred in the absenceof a significant heat source. Usually, these theories arefairly creative and generally do not let factual matters standin their way. The theory cited most often is that, eventhough the hypothermia machine was operating normallyand without malfunction, it still caused a burn because thepatient’s condition was such that the skin was moresusceptible to heat, and hence burned at a temperaturethat otherwise would not cause a burn.
Another theory often cited is that the patient was burnedby or had an allergic reaction to the prep solutions, evenif the areas involved were not prepped!
Yet another theory encountered is that, even though theelectrocautery and grounding electrode were found to be
© 1998 Blackwell Science Ltd International Journal of Dermatology 1998, 37, 729–732
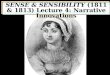
Figure 1 Although these injuries usually occur below thewaist, they can be found in any of the locations indicated,usually over a bony prominence (except posterior thigh andcalf)
operating normally, there must have been another groundpath for the electricity and this must have caused the ‘‘burn.’’
Mysterious lesions
If not ‘‘burns,’’ then what are these mysterious lesions?Most often, they are caused by a number of factors:pressure, shear, and ischemia (often exacerbated by a warmenvironment) are frequently the culprits.
The pressure is a consequence of the anesthetized patient’simmobility during surgery (.3 h). Shear is usually aconsequence of the patient’s position or positioning for the

732 Commentary When a burn is not a burn Stewart
procedure. Ischemia is a consequence of the cross-clampingof the aorta, the nonpulsatile flow during the cardiopulmon-ary bypass, and/or the patient’s underlying disease (poorperfusion or vascular insufficiency).
These lesions are usually found over, or close to, a bonyprominence; however, because of the ischemic etiology, inmany instances the buttocks, posterior thighs, and eventhe posterior aspects of the calves may be involved (Fig. 1).These wounds may initially present as blisters over theinvolved areas, that ultimately break and may evolve tolarge open ulcers. They are often very severe, with asignificant amount of tissue loss, because the ischemic timehas caused total necrosis of the muscle and subcutaneoustissue (this is why they are often mistaken for third orfourth degree burns). With necrosis of the muscle andsubcutaneous tissue, there is often the presence of a thickblack eschar (which is often described as ‘‘charred’’ skinand fits in with a burn as the diagnosis). These lesions canrange in severity from Stage I to Stage IV (pressure ulcerstaging), but the wounds are usually of a single severity,unlike some burns caused by flames that may have zonesof different severity.
One of the most important mistakes made in theseinstances is the initial diagnosis and description of thelesion as a ‘‘burn.’’ It is this single act that usually destinesthese cases for an unfortunate journey through our legalsystem. If you come across any such lesions or circumstance,be sure to refer to them as ‘‘unexplained wound’’ or‘‘unexplained lesion.’’ Once declared a ‘‘burn,’’ it is nearlyimpossible to remove this thought from the mind of thepatient, staff, attorney, and jury.
The threshold for thermal injury (burn) is 44°C for 6 h.This threshold is not dependent upon the perfusion of thetissue or underlying disease. If there is no source oftemperature above this threshold (both temperature andduration), there can be no burn. An elevated temperature
From the collection ofLawrence Charles Parish, MD,Philadelphia, Pennsylvania.
International Journal of Dermatology 1998, 37, 729–732 © 1998 Blackwell Science Ltd
can, however, exacerbate ischemia, whether it is causedby pressure, shear, cross-clamping, or cardiopulmonarybypass. Remember that ischemic tissue will become necroticat some time after its metabolic rate exceeds its oxygenand nutrient supply. The time it takes to cause death ofthis tissue is temperature dependent. If we take ischemictissue and warm it, it will die sooner than if we had notwarmed it. This is because, in general, the metabolic rateof tissue will increase by approximately 13% for everydegree Celsius rise in temperature. The mechanisms ofcell death are also decidedly different for thermal injuryvs. ischemic injury.
Finale
Pressure necrosis and ischemic necrosis should be the primesuspects in any unexplained lesions that occur duringlengthy surgical procedures.
So, I ask you again: do you know a burn when yousee one?
References
1 Gendron F. Unexplained Patient Burns: InvestigatingIatrogenic Injuries. Brea, California: Quest PublishingCo., Inc., 1988.
2 Emergency Care Research Institute. Skin injury in theOR and elsewhere. Health Devices 1980; 9:312–318.
3 Stewart TP, Magnano S. Burns or pressure ulcers in thesurgical patient? Decubitus 1988; 1: 36–40.
4 LoCicero J, Fisher E, Atlas P, et al. Remote skin injury: aprotean complication of open heart surgery. Am Surg1986; 52: 97–100.
5 Chenye FW, Posner KL, Caplan RA, Guild WM. Burnsfrom warming devices in anesthesia: a closed claimsanalysis. Anesthesiology 1994; 80: 806–810.