Embed Size (px)
Citation preview

STUDY PROTOCOL Open Access
Sequential learning of psychomotor andvisuospatial skills for laparoscopic suturingand knot tying – study protocol for arandomized controlled trial “The shoeboxstudy”Jonathan D. Hendrie1, Felix Nickel1, Thomas Bruckner2, Karl-Friedrich Kowalewski1, Carly R. Garrow1,Maisha Mantel3, Philipp Romero3 and Beat P. Müller-Stich1*
Abstract
Background: Laparoscopy training has become an integral part of surgical education. Suturing and knot tying is abasic, yet inherent part of many laparoscopic operations, and should be mastered prior to operating on patients.One common and standardized suturing technique is the C-loop technique. In the standard training setting, on abox trainer, the trainee learns the psychomotor movements of the task and the laparoscopic visuospatial orientationsimultaneously. Learning the psychomotor and visuospatial skills separately and sequentially may offer a moretime-efficient alternative to the current standard of training.
Methods: This is a monocentric, two-arm randomized controlled trial. The participants are medical students in theirclinical years (third to sixth year) at Heidelberg University who have not previously partaken in a laparoscopic trainingcourse lasting more than 2 hours. A total of 54 students are randomized into one of two arms in a 1:1 ratio tosequential learning (group 1) or control (group 2). Both groups receive a standardized introduction to the trainingcenter, laparoscopic instruments, and C-loop technique. Group 1 learn the C-loop using a transparent shoebox, thusonly learning the psychomotor skills. Once they reach proficiency, they then perform the same knot tying procedureon a box trainer with standard laparoscopic view, where they combine their psychomotor skills with the visuospatialorientation inherent to laparoscopy. Group 2 learn the C-loop using solely a box trainer with standard laparoscopicview until they reach proficiency. Trainees work in pairs and time is recorded for each attempt. The primaryoutcome is mean total training time for each group. Secondary endpoints include procedural and knotquality subscore differences. Tertiary endpoints include studying the influence of gender and video gameexperience on performance.
Discussion: This study addresses whether the learning of the psychomotor and visuospatial aspects of laparoscopicsuturing and knot tying is optimal sequentially or simultaneously, by assessing total training time, procedural, and knotquality differences between the two groups. It will improve the efficiency of future laparoscopic suturing courses andmay serve as an indicator for laparoscopic training in a broader context, i.e., not only for suturing and knot tying.
Trial registration: This trial was registered on 12 August 2015 with the trial registration number DRKS00008668.
Keywords: Laparoscopy, Training, Education, Minimally invasive surgery, Suturing, Knot tying
* Correspondence: [email protected] of General, Visceral, and Transplantation Surgery, University ofHeidelberg, Im Neuenheimer Feld 110, 69120 Heidelberg, GermanyFull list of author information is available at the end of the article
© 2016 Hendrie et al. Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Hendrie et al. Trials (2016) 17:14 DOI 10.1186/s13063-015-1145-8

BackgroundMinimally invasive surgery (MIS) involves learning aseparate skill set from that of open surgery. Althoughsome of the necessary qualities are the same, e.g.,bimanual dexterity and steadiness, many of the basicskills must be learned for the first time or anew, e.g., thefulcrum effect, tissue grasping, needle manipulation,knot tying, etc. These basic psychomotor skills give sur-geons the tools necessary to complete full operations;therefore, the learning of them has become one of thecornerstones of laparoscopic training curricula [1–3]. Asmany surgical operations defer to the laparoscopicapproach, it has become imperative for surgical traineesto demonstrate proficiency in basic and procedural skillsprior to operating on patients. Training modalities, e.g.,virtual reality (VR) simulators, inanimate box trainers,and cadaveric organ trainers can be used as a safe, ethical,and effective means to do this [4–8].Box trainers provide a realistic platform for the learning
of laparoscopic skills with real instruments [9]. Intracorpor-eal suturing and knot tying [10] is an invaluable skill neededfor minimally invasive operations [11, 12]. Suturing skillslearned via a box trainer suture model have been shown totransfer to the operating room (OR) [13]. Training withinthe box trainer familiarizes trainees with the two majorfacets of laparoscopy: psychomotor control and visuospatialorientation [14–18].Surgeons need to be familiar with depth perception and
2D–3D visuospatial understanding, since laparoscopy
utilizes an indirect view. However, it remains to be deter-mined if the learning of psychomotor and visuospatialskills simultaneously is optimal, as in a box trainer. Learn-ing these two skills separately and sequentially may offer amore effective training alternative that reduces the learn-ing or teaching time for trainees and mentors respectively.This would lower the workload of tutors and the learningcurve of trainees, and save limited time and resources in atraining center. Therefore, we aim to explore whethersequential learning with a transparent shoebox, where onelearns the psychomotor movements, followed by trainingon a box trainer with the indirect laparoscopic view,expedites the learning of the surgical C-loop technique incomparison to training solely on a box trainer with theindirect laparoscopic view, where one learns the psycho-motor and visuospatial skills simultaneously.
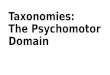
MethodsObjectiveThe primary goal of this study is to identify if studentsin group 1, who learn the surgical C-loop techniqueusing a transparent shoebox before using a box trainerwith laparoscopic view, have a shorter learning curvethan students in group 2, who learn the technique usingsolely a box trainer with laparoscopic view (Fig. 1). Sec-ondary endpoints include number of attempts taken togain proficiency, and examining procedural and knotquality subscore differences. In subgroup analyses wewill separately explore possible gender differences and
Laparoscopy-naive medical students N=54
Introduction video for suturing and knot tying
Randomization 1:1
Group 2 Simultaneous learning (Control)
N=27
Training of suturing and knot tying on a box trainer until proficiency
Group 1 Sequential learning (Intervention)
N=27
Training of suturing and knot tying on shoebox until proficiency
Training of suturing and knot tying on a box trainer until proficiency
Fig. 1 Study flowchart
Hendrie et al. Trials (2016) 17:14 Page 2 of 7

influence of previous video game experience on trainingtime, number of attempts needed to reach proficiencyand knot quality respectively.
Study designThis is a registered prospective, single-center, two-arm,parallel group randomized controlled trial.
Setting and participantsThis study is conducted in the MIS training center ofHeidelberg University Hospital’s Department of General,Visceral, and Transplantation Surgery. It offers a voluntarylaparoscopic training course to medical students. Trainingtutors are specially trained medical students (n = 4) atHeidelberg University, non-blinded to the training groups,who receive a standardized rater training prior to thebeginning of data collection.
Inclusion and exclusion criteriaThe inclusion criterion mandates that participants aremedical students in their clinical years (third to sixthyear) at Heidelberg University. Exclusion criteria includestudents who have previously participated in a laparoscopictraining course of more than 2 hours duration or who hadtraining in laparoscopic surgery in the OR.
Video introduction to laparoscopic suturing and knottyingAll students receive a standardized video-based intro-duction to the suturing and knot tying technique at thestart of the study. Students may refer to this videothroughout the course of their participation.
Introduction to the training modalities in the trainingcenterTrained student tutors provide a standardized introduc-tion for the box trainer, shoebox, and laparoscopic in-struments, as well as instructions for their use. Studentscan, therefore, familiarize themselves with the trainingmodalities, workspace, and terminology prior to theinduction of their training.
RandomizationParticipants are randomly allocated to either the sequen-tial learning group (group 1) or control group (group 2) ina 1:1 ratio. The randomization of subjects is performed byan employee otherwise not involved in the study usingsealed envelopes labeled by block. Trainees are allocatedto groups without stratification by gender or gamingexperience. Although this study would benefit from a 1:1ratio of men to women, this cannot be mandated since thedata is collected through participation in a universityelective course which is offered on a first-come-first-servebasis. Consequentially, we cannot explore outcome
differences in heterogeneous or homogeneous groups,e.g., male-female, male-male, female-female, in a standard-ized manner; there may be an influencing factor thatstems from the communication dynamic, previous experi-ence of a partner, etc. We aim to explore these differencesby comparing outcomes between pair group subgroupanalysis following data acquisition. An employee of theDepartment of Medical Biometry at Heidelberg University,who is otherwise not involved with the training, tests, ordata collection from the present study, assigned blockrandomization.
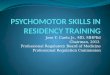
Training curriculumThe sequential learning group (group 1) learn the psy-chomotor aspects of laparoscopic suturing and knottying first on the transparent shoebox without having toadjust to the visuospatial orientation inherent to the lap-aroscopic view of a box trainer. Once they reach the pre-defined proficiency criteria explained below (Tables 1, 2and 3), these students then train on the box trainer withlaparoscopic view until proficient (Fig. 2). The controlgroup (group 2) learn the psychomotor skills and visuo-spatial aspects of laparoscopy simultaneously, as is trad-itionally done. They train using the box trainer withlaparoscopic view until proficient in the predefined cri-teria. Specially trained peer tutors assist trainees duringthe course of the study and are available on demand inthe training room for both groups; this has proven to bebeneficial to trainee learning [19].Following randomization, participants are put into
training pairs, which is a common practice within surgicaltraining [20, 21]. This allows the trainees to give eachother real-time competency assessment and feedback,which is motivational [22, 23], in addition to saving timefor the trainers, and space in the training center. We re-cently explored the difference between laparoscopic train-ing alone and in pairs and found there to be no distinctionin outcome between the two groups (protocol, own data,unpublished). It has been shown that students – whetheralone or in a collaborative pair – can learn as much by ob-serving their peers learn a task as they can by performingthe task themselves [24, 25]. This is known as vicariouslearning, which typically does not provide for communica-tion between the student being tutored and the studentwatching. It should be made clear that students in ourtraining environment can communicate directly with oneanother, which may prove even more useful. Based onthese grounds, we believe that the pragmatic aspect of sav-ing time and resources in a busy training center outweighsthe potentially confounding effect of partner training.The student who is watching records the time taken
for each attempt of the operating partner, starting fromwhen the needle is grasped and ending once the finalknot is tied. All attempts must be completed and the
Hendrie et al. Trials (2016) 17:14 Page 3 of 7

time per attempt must be recorded for each trainee. Inthe event of technical or instrument failure, e.g., thesuture thread getting stuck in the grooves of the instru-ment, time is stopped and recorded, and “N/A” and abrief description of what happened are written next tothe attempt. Rather than mass practice, we implementthe more effective interval training [26–28]; trainees arerequired to switch positions at least every five completedknot attempts. Students train using two laparoscopicneedle holders (KARL STORZ GmbH & Co. KG, Tuttlin-gen, Germany) and a standardized silicone suture padwith diagonal incisions and predefined suture entry and
exit points (Fig. 3) (Big Bite Medical GmbH, Heidelberg).The suture material is a Polysorb 3-0 braided absorbablesuture with a CV-23 taper ½ 17-mm needle (CovidienTM,Minneapolis, MN, USA).Training pairs are required to rate each other through-
out the training process until they reach the predefinedcompetency levels for knot quality, suture position, andtime. Procedural competency is assessed using a previ-ously validated modified 23-point implementationchecklist [14] (Table 1), originally published by Munz etal. [29].Knot quality is scored using a 5-point scale designed
by Muresan et al. [10], which assesses a knot’s throws,tightness, edge opposition, and ability to hold underTable 2 Knot quality checklist
Knot quality assessment Availablepoints
No visible gaps between stacked throws 1
Knot tight at base 1
Only edges are opposed (no extra tissue in knot, e.g.,back wall)
1
Knot holds under tension 2
Maximum 5
Table 3 Competency checklist
Competency assessment Goal Yes/No
Time (min:sec) ≤01:15
Procedure ≥18
Knot quality ≥4
Accuracy (mm) ≤2
Competency (if all “Yes” above)
Table 1 Procedural proficiency checklist
Procedure assessment Yes/No
Needle position 1 1 Held at one half to two thirds distance from the tip
2 Angle 90° ± 20°
3 Uses tissue or other instrument for stability
4 Attempts at positioning (≤3)
Needle driving 1 (entry to incision) 5 Entry at 60° to 90° to the tissue plane
6 Driving with one movement
7 Single point of entry through the tissue
8 Removes the needle along its curve
Needle position 2 9 Held at one half to two thirds distance from the tip
10 Angle 90° ± 20°
11 Uses tissue or other instrument for stability
12 Attempts at positioning (≤3)
Needle driving 2 (incision to exit) 13 Driving with one movement
14 Removes the needle along its curve
Pulling the suture 15 Needle on needle holder in view at all times
16 Uses the pulley concept
Technique of knots 17 Correct C-loop (no S- or O-loops)
18 Smoothly executed throw, no fumbles
19 Correct inverse C-loop (no S- or O-loops)
20 Smoothly executed throw, no fumbles
21 Knot squared (capsized/reef/surgical)
22 Correct third C-loop (no S- or O-loops)
23 Smoothly executed throw, no fumbles
Total points
Hendrie et al. Trials (2016) 17:14 Page 4 of 7

tension (Table 2). Furthermore, accuracy is recorded bymeasuring the distance (mm) of the stitch from the edgeof the entry and exit points of the standardized suturepad. Operative time is also recorded.A trainee demonstrates competency for the C-loop
upon finishing it in ≤01:15 (min:sec), attaining ≥18points on the procedural implementation checklist, scor-ing ≥4 on the knot quality scale, and maintaining stitching≤2 mm from the edge of the suture pad’s entry and exitpoints (Table 3). According to the available medical litera-ture, experienced surgeons (expert level) reach these goalsfor the surgical C-loop [14]. Once a student has reachedcompetency according to his or her training partner, aspecially trained peer tutor is asked to provide expertassessment. If the participant then performs a C-loop,attaining the aforementioned competency criteria under
supervision of the tutor, he or she is considered proficientin the technique; thus proficiency is achieved once atrainee completes the C-loop suturing technique on twoconsecutive occasions with the predefined competencycriteria – once for the partner and once for the peer tutorassessment.
Primary endpointThe primary endpoint is total training time needed toreach proficiency in a predefined standardized suturingand knot tying technique.
Secondary endpointsSecondary endpoints include the number of attempts,procedure subscore differences, and knot quality sub-score differences.
Tertiary endpointsTertiary endpoints involve subanalyses of gender differ-ences and the influence of video game experience. Sur-gery has traditionally been a male-dominated field andresearch has demonstrated that male medical studentsare faster at acquiring surgical skills and demonstratesuperior visuospatial skills in comparison to their femalepeers [30–33]. We will explore this further by comparingmale and female performance in both groups for totaltime taken and number of attempts. Furthermore, wewill explore the influence of video game experience, inyears, on total time taken and number of attempts, forboth groups.
Statistical analysisThe empirical distributions of all parameters of interestare described using mean and standard deviation in caseof continuous data, with absolute and relative frequenciesin case of categorical parameters. Possible difference inthe primary outcome, time to reach proficiency, will betested using a two-sided t test. All secondary parametersincluding subgroup analyses will be descriptively analyzedaccording to their underlying distribution, two-sidedMann-Whitney U tests in case of continuous parameters,and Chi-square test in case of categorical data. Graphicalstatistical methods will illustrate the findings, wheneverappropriate.
Sample size determinationSample size calculation was done with respect to the pri-mary endpoint. A previously evaluated pilot study showedthe following data for total training time needed to reachproficiency: mean difference between group 1 and group 2was 15 seconds; standard deviation in group 1 was15.6 seconds, whereas it was 22.2 seconds in group 2. Thisdifference can be detected with a two-sided significance
Fig. 3 Standardized silicone suture pad
Fig. 2 Transparent shoebox used by intervention group (left). Boxtrainer with laparoscopic view used by both groups (right)
Hendrie et al. Trials (2016) 17:14 Page 5 of 7

level α = 0.05 and a power of 1 − β = 0.8, with a group sizeof 27 participants randomized to each group.
Ethical and legal aspectsAll data for the study is recorded anonymously, treatedconfidentially, and is evaluated by authorized staff forscientific purposes only. Participants’ names are keptseparate from all study data and are not used for thestudy. Each participant is assigned a designated codethat is used for the entire study documentation and datacollection. This study is offered in addition to compul-sory university courses. Participation in this study is vol-untary and may be ended at any time. There are noforeseeable negative consequences related to participa-tion. The participating staff of the Heidelberg MIS train-ing center is experienced in the handling of trainingdevices and in tutoring MIS. The benefits of training forstudents are numerous: stamina, concentration, andmanual adroitness are enhanced and practiced, surgicalinterest may be sparked or strengthened, and studentsreceive practical laparoscopy experience, which may beused during later work. In the event that a participant’sphysical or mental health becomes jeopardized due toparticipation in the present study, the participant will bewithdrawn immediately and excluded from the study.Written informed consent is obtained from each trainee.Ethical approval was obtained from the Ethics Commit-tee of the Medical Faculty at Heidelberg University priorto the beginning of the study (Code S-334/2011). TheConsolidated Standards of Reporting Trials (CONSORT)guidelines for randomized controlled trials and StandardProtocol Items: Recommendations for InterventionalTrials (SPIRIT) guidelines for implementation of studyprotocols were followed [34, 35]. This trial was regis-tered with the German Clinical Trials Register (DRKS)in Freiburg, Germany on 12 August 2015 with the trialregistration number DRKS00008668.
DiscussionThis study aims to assess the differences in the learningof the psychomotor and visuospatial aspects of laparo-scopic suturing and knot tying between those who learnthem sequentially and those who learn them simultan-eously. Trainees typically learn these aspects simultan-eously, but no support was found necessitating thismethodology. We expect that trainees who start on theshoebox will learn the C-loop much quicker than thosewho begin with the box trainer. However, it remains tobe determined whether these skills quickly transfer tothe box trainer with laparoscopic view. Nonetheless, it isimportant to ascertain which training method will be themost efficient for training centers. The potential forshorter learning curves and more effective use of re-sources, e.g., training center space, time, and trainers is
rationale in itself to explore alternatives to current stan-dards. The results of this study have the potential to shiftthe current paradigm for the training of laparoscopic su-turing and knot tying or strengthen the present standard.
Trial statusRecruitment started in April 2015 and is expected to finishby December 2015.
ConsentWritten informed consent was received from the partici-pants for publication of this manuscript and accompany-ing images. A copy of the written consent is available forreview by the editor-in-chief of this journal.
AbbreviationsICC: intraclass correlation coefficient; LC: laparoscopic cholecystectomy;MIS: minimally invasive surgery; OR: operating room; VR: virtual reality.
Competing interestsThe authors hereby declare that they have no competing interests.
Authors’ contributionsStudy conception and design: BPMS, FN, JDH, MM, K-FK, CRG and PR. Statisticalplanning: TB. Drafting of manuscript: JDH, FN, K-FK, MM and CRG. Criticalrevision: BPMS, PR and FN. All authors read and approved the final version ofthis manuscript.
AcknowledgementsWe would like to thank Marion Link for her help with organizing this study.
FundingThis project was supported by the Heidelberg Foundation for Surgery.
Author details1Department of General, Visceral, and Transplantation Surgery, University ofHeidelberg, Im Neuenheimer Feld 110, 69120 Heidelberg, Germany. 2Institutefor Medical Biometry and Informatics, University of Heidelberg, ImNeuenheimer Feld 305, 69120 Heidelberg, Germany. 3Department ofPediatric Surgery, University of Heidelberg, Im Neuenheimer Feld 110, 69120Heidelberg, Germany.
Received: 15 September 2015 Accepted: 23 December 2015
References1. Watanabe Y, McKendy KM, Bilgic E, Enani G, Madani A, Munshi A, et al. New
models for advanced laparoscopic suturing: taking it to the next level. SurgEndosc, 2015. [Epub ahead of print]
2. Nickel F, Brzoska JA, Gondan M, Rangnick HM, Chu J, Kenngott HG, et al.Virtual reality training versus blended learning of laparoscopiccholecystectomy: a randomized controlled trial with laparoscopic novices.Medicine (Baltimore). 2015;94(20), e764.
3. Nebiker CA, Mechera R, Rosenthal R, Thommen S, Marti WR, von Holzen U,et al. Residents’ performance in open versus laparoscopic bench-modelcholecystectomy in a hands-on surgical course. Int J Surg. 2015;19:15–21.
4. Aggarwal R, Balasundaram I, Darzi A. Training opportunities and the role ofvirtual reality simulation in acquisition. J Surg Res. 2008;145(1):80–6.
5. Undre S, Darzi A. Laparoscopy simulators. J Endourol. 2007;21(3):274–9.6. Korndorffer Jr JR, Stefanidis D, Scott DJ. Laparoscopic skills laboratories:
current assessment and a call for resident. Am J Surg. 2006;191(1):17–22.7. Aggarwal R, Darzi A. Training in laparoscopy – which model to use? Indian J
Gastroenterol. 2005;24(3):95–6.8. Aggarwal R, Moorthy K, Darzi A. Laparoscopic skills training and assessment.
Br J Surg. 2004;91(12):1549–58.9. Felix N, Felix J, Andreas M, Matthias G, Hendrie JD, Tobias G, et al. One or
two trainees per workplace in a structured multimodality training
Hendrie et al. Trials (2016) 17:14 Page 6 of 7

curriculum for laparoscopic surgery? Study protocol for a randomizedcontrolled trial – DRKS00004675. Trials. 2014;15:137.
10. Muresan 3rd C, Lee TH, Seagull J, Park AE. Transfer of training in thedevelopment of intracorporeal suturing skill in medical student novices: aprospective randomized trial. Am J Surg. 2010;200(4):537–41.
11. Nguyen NT, Mayer KL, Bold RJ, Larson M, Foster S, Ho HS, et al. Laparoscopicsuturing evaluation among surgical residents. J Surg Res. 2000;93(1):133–6.
12. Pennings JL, Kenyon T, Swanstrom L. The knit stitch. An improved methodof laparoscopic knot tying. Surg Endosc. 1995;9(5):537–40.
13. Korndorffer Jr JR, Dunne JB, Sierra R, Stefanidis D, Touchard CL, Scott DJ.Simulator training for laparoscopic suturing using performance goalstranslates to the operating room. J Am Coll Surg. 2005;201(1):23–9.
14. Romero P, Brands O, Nickel F, Müller B, Günther P, Holland-Cunz S. Intracorporalsuturing – driving license necessary? J Pediatr Surg. 2014;49(7):1138–41.
15. Korndorffer Jr JR, Clayton JL, Tesfay ST, Brunner WC, Sierra R, Dunne JB, et al.Multicenter construct validity for southwestern laparoscopic videotrainerstations. J Surg Res. 2005;128(1):114–9.
16. Chung SD, Tai HC, Lai MK, Huang CY, Wang SM, Tsai YC, et al. Novelinanimate training model for urethrovesical anastomosis in laparoscopicradical prostatectomy. Asian J Surg. 2010;33(4):188–92.
17. Yoshida K, Kinoshita H, Kuroda Y, Oshiro O, Matsuda T. Analysis oflaparoscopic dissection skill by instrument tip force measurement. SurgEndosc. 2013;27(6):2193–200.
18. Siska VB, Ann L, de Gunter W, Bart N, Willy L, Marlies S, et al. Surgical skill:trick or trait? J Surg Educ. 2015;72(6):1247–53.
19. Van Bruwaene S, De Win G, Miserez M. How much do we need expertsduring laparoscopic suturing training? Surg Endosc. 2009;23(12):2755–61.
20. Fearn SJ, Burke K, Hartley DE, Semmens JB, Lawrence-Brown MM. Alaparoscopic access technique for endovascular procedures: surgeontraining in an animal model. J Endovasc Ther. 2006;13(3):350–6.
21. Hoffman MS, Ondrovic LE, Wenham RM, Apte SM, Shames ML, Zervos EE, et al.Evaluation of the porcine model to teach various ancillary procedures togynecologic oncology fellows. Am J Obstet Gynecol. 2009;201(1):116. e1-3.
22. Botden SM, de Hingh IH, Jakimowicz JJ. Suturing training in Augmented Reality:gaining proficiency in suturing skills faster. Surg Endosc. 2009;23(9):2131–7.
23. Gonzalez R, Bowers SP, Smith CD, Ramshaw BJ. Does setting specific goalsand providing feedback during training result in better acquisition oflaparoscopic skills? Am Surg. 2004;70(1):35–9.
24. Chi MT, Roy M, Hausmann RG. Observing tutorial dialogues collaboratively:insights about human tutoring effectiveness from vicarious learning. CognSci. 2008;32(2):301–41.
25. Stegmann K, Pilz F, Siebeck M, Fischer F. Vicarious learning during simulations:is it more effective than hands-on training? Med Educ. 2012;46(10):1001–8.
26. Buckley CE, Kavanagh DO, Nugent E, Ryan D, Traynor OJ, Neary PC. Theimpact of aptitude on the learning curve for laparoscopic suturing. Am JSurg. 2014;207(2):263–70.
27. Gallagher AG, Ritter EM, Champion H, Higgins G, Fried MP, Moses G, et al.Virtual reality simulation for the operating room: proficiency-based trainingas a paradigm shift in surgical skills training. Ann Surg. 2005;241(2):364–72.
28. Metalis SA. Effects of massed versus distributed practice on acquisition ofvideo game skill. Percept Mot Skills. 1985;61(2):457–8.
29. Munz Y, Almoudaris AM, Moorthy K, Dosis A, Liddle AD, Darzi AW.Curriculum-based solo virtual reality training for laparoscopic intracorporealknot tying: objective assessment of the transfer of skill from virtual reality toreality. Am J Surg. 2007;193(6):774–83.
30. Donnon T, DesCôteaux J-G, Violato C. Impact of cognitive imaging and sexdifferences on the development of laparoscopic suturing skills. Can J Surg.2005;48(5):387–93.
31. Thorson CM, Kelly JP, Forse RA, Turaga KK. Can we continue to ignoregender differences in performance on simulation trainers? J LaparoendoscAdv Surg Tech A. 2011;21(4):329–33.
32. Schlickum M, Felländer-Tsai L, Hedman L, Henningsohn L. Endourologicalsimulator performance in female but not male medical students predictswritten examination results in basic surgery. Scand J Urol. 2013;47(1):38–42.
33. Ali A, Subhi Y, Ringsted C, Konge L. Gender differences in the acquisition ofsurgical skills: a systematic review. Surg Endosc. 2015;29(11):3065–73.
34. Chan AW, Tetzlaff JM, Gøtzsche PC, Altman DG, Mann H, Berlin JA, et al.SPIRIT 2013 explanation and elaboration: guidance for protocols of clinicaltrials. BMJ. 2013;346, e7586.
35. Schulz KF, Altman DG, Moher D. CONSORT 2010 Statement: updatedguidelines for reporting parallel group randomised trials. Trials. 2010;11:32.
• We accept pre-submission inquiries
• Our selector tool helps you to find the most relevant journal
• We provide round the clock customer support
• Convenient online submission
• Thorough peer review
• Inclusion in PubMed and all major indexing services
• Maximum visibility for your research
Submit your manuscript atwww.biomedcentral.com/submit
Submit your next manuscript to BioMed Central and we will help you at every step:
Hendrie et al. Trials (2016) 17:14 Page 7 of 7