Embed Size (px)
Citation preview

Student SYB
Chet Cunha MS IVFebruary 4, 2009

History
•75 y/o M admitted for progressive weakness, inability to get out of bed.
•C/o R sided lower leg pain

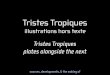
Plain films Right leg

Plain films Right leg




DDx lytic bone lesion
•Multiple myeloma
•Mets (breast, lung, kidney, thyroid)
•Eosinophilic granuloma (histiocytosis X)
•Brown tumor (hyperparathyroid)
•Benign bone lesions - endochondroma, chondroblastoma






Multiple Myeloma
•B lymphocyte defect
•Diffuse osteopenia
•Renal insufficiency
•Anemia
•Recurrent infection
•Can progress to amyloidosis

Multiple Myeloma
•Hypercalcemia
•Nongap acidosis
•Rouleaux formation
•Bence Jones proteins in urine
•Increased ESR

Multiple Myeloma•Most common primary skeletal
neoplasm
•Usually seen in vertebral column, ribs, skull, pelvis, and femora (axial skeleton)
•Typically multiple, discrete, small, lytic lesions
•Occasionally, seen as a single lytic lesion: plasmacytoma (solitary myeloma)

Multiple Myeloma
•Skeletal survey
•CT
•MRI

Further Reading
• Gourtsoyiannis, N.C., Ros, P.R. Radiologic-Pathologic Correlations from Head to Toe. Springer Publishing, Berlin 2005.
• Grossman, Z.D., Katz, D. S., et al. Cost-Effective Diagnostic Imaging. Mosby Elsevier, Philadelphia, 2006.

Thank you!