Embed Size (px)
Citation preview

Topical review
Stroke units: many questions, some answers
Blanca Fuentes and Exuperio Dıez-Tejedor�
Background The development of specialized stroke units has
been a landmark innovation in acute stroke care. However,
the high scientific evidence level for the recommendation for
stroke units to provide clinical attention for acute stroke
patients does not correspond to the level of stroke unit
implementation. A narrative, nonsystematic review on pub-
lished studies on stroke units was conducted, with special
emphasis on those demonstrating their efficacy and effec-
tiveness. We also attempt to provide some answers to several
open questions regarding practical issues of stroke units.
Summary of review Stroke units represent the most effica-
cious model for care provision compared with general ward
care and stroke teams. Every stroke patient can benefit from
stroke unit care. These units are efficient, cost-effective and
their benefits are consistent over time. Compared with other
specific stroke therapies such as aspirin or intravenous throm-
bolytic agents, stroke units have a higher target population
and higher benefit in terms of number of deaths and/or
dependencies avoided. New approaches in stroke unit man-
agement such as the implementation of noninvasive monitor-
ing or alternative clinical pathways could improve their
benefit even further.
Conclusion Stroke units are cost-effective and need to be
considered as a priority in health-care provision for stroke
patients.
Key words: effectiveness, efficacy, efficiency, stroke team,
stroke unit, stroke
The development of stroke units (SUs) has been a milestone in
the care provision for patients who have suffered a stroke.
From a nihilistic approach in which the clinical evolution of
the patient was allowed to proceed uninterrupted, the care for
these patients has progressed to being considered as a first-level
neurological emergency. However, despite the high grade of
scientific evidence on which the recommendations for SUs for
care provision of the patients with acute stroke are based, there
is no correspondence with the level of implementation of these
SUs worldwide (1, 2). There are few studies and surveys
analyzing the current population coverage from SU and the
differences between countries are clear. In Scandinavian coun-
tries, up to 60–70% of stroke patients are managed in SU while
in other European countries like the United Kingdom or
Germany it reaches only 30–36% and in France or Italy o10% (3). In Australia, only 19% of 261 acute public hospitals
participating in a cross-sectional survey claimed to have an SU,
and they did not treat all the stroke patients presenting to their
hospitals (4). In the United States, data from a survey
conducted in North Carolina showed that 45% of acute stroke
patients have access to SU care (5). Finally, in the Canadian
Stroke Network report in 2004, only 18% of acute stroke
patients were admitted to an SU (6). Probably, in no other
therapy with level I evidence based on randomized studies and
meta-analyses has there been such a clear need for implemen-
tation of SUs. Our objective is to review the current issues
associated with the provision of SU care from an international
perspective.
Concept and historical development
SU is usually defined as ‘a geographic location within the
hospital designated for stroke patients who are in need of
rehabilitation services and skilled professional care that such a
unit can provide’ (7). But several categories of SU have also
been defined mainly based on admission policy (acute admis-
sion units, which admitted patients at stroke onset (within
1 week); delayed admission units, which admitted patients
after a delay of at least 1 week and that are mainly focused on
rehabilitation). On the other hand, mixed or comprehensive
units are characterized by a combination of acute admission
with a period of rehabilitation (7). Acute SUs are defined as
those areas dedicated to the care (non or semi-intensive)
during the acute phase and, once stabilized, the patient is
transferred to the general neurology ward, where the diagnos-
tic–therapeutic process continues up until the discharge from
hospital, or transfer to rehabilitation or to geriatric units (8, 9).
Correspondence: Exuperio Dıez-Tejedor�, Department of Neurology,
Hospital Universitario La Paz, Autonomous University of Madrid, Paseo
de la Castellana, 261, 28046 Madrid, Spain. Tel: (134) 917 277 444; Fax:
(134) 913 581 403; e-mail: [email protected]
Stroke Unit, Department of Neurology, University Hospital La Paz,
Autonomous University of Madrid, Madrid, Spain
& 2009 The Authors.28 Journal compilation & 2009 World Stroke Organization International Journal of Stroke Vol 4, February 2009, 28–37

To date, there exist some variabilities in the medical depart-
ments in which the SU are established: geriatric medicine,
general medicine, neurology and rehabilitation medicine.
Although all of these possibilities shared the multidisciplinary
team care approach, general medicine and neurology are more
focused on acute and more disease-specific approaches and
geriatric and rehabilitation medicine on a more generic
disability approach (7).
Although in several countries stroke expertise may reside
within other hospital departments (e.g. general medicine,
geriatric medicine), mainly depending on the Health Policy
and on the different medical specialization developing and
availability, acute SUs are recommended to be situated in a
specific area within the Neurology department of the hospital
and with dedicated beds. It should be of a multidisciplinary
structure coordinated by a neurologist specializing in cere-
brovascular disease, and with specially trained support per-
sonnel (9). There need to be predefine criteria of admission,
explicit diagnostic and treatment protocols and work pro-
grams coordinated with other specialties such as cardiology,
neuroradiology, neurosurgery, vascular surgery, rehabilitation
and geriatrics. The activity of the SU needs to be continuous
over 24 h/day; the physical presence of a neurologist on duty is
a requirement (9). Further, it is recommended that the SU
facilities include multiparameter noninvasive monitoring
(EKG, oximetry, blood pressure and body temperature),
together with a laboratory for blood analytic measurements
as well as ultrasound for neurovascular assessment (transcra-
nial and extracranial Doppler sonography) (7–10).
Since the 1950s, there have been several studies conducted
with the objective of establishing an appropriate organiza-
tional model for stroke, focusing on aspects of rehabilitation
(7). It was not until the 1970s that the idea of the SU was
suggested for the first time. Initially, these were designed as
intensive care units (ICUs), with facilities for monitoring and
for the administration of intensive therapy. The patients
admitted were those with severe stroke, with greater neurolo-
gical deficit and poorer general status. Those with mild
impairment or with a transient ischemic attack (TIA) were
excluded. The results were very variable and did not show a
clear reduction in mortality, although decreases in the num-
bers of complications were noted (11–15) (Table 1)
Subsequently, in the 1980s, the concept of the SU evolved
from acute, nonICUs characterized by a systemization of care
provision for the patients and that involved trained personnel,
preestablished criteria, with special attention being paid to the
acute-phase treatment and the early functional rehabilitation
and early return to society. This implied establishing a
systematic diagnosis and precise therapy as well as an effica-
cious multidisciplinary approach. In the 1990s, interest in SUs
was renewed following the publication of several studies
comparing SUs with general medical wards that demonstrated
the benefits in terms of mortality, functional recovery and in
the rates of chronic institutionalization (16–19) (Table 1).
Also, several meta-analyses confirmed the efficacy of SUs not
only with respect to early mortality (28% reduction within the
first 4 months) but also that at 1 year (21% reduction) (20).
There was a reduction in the odds of death [odds ratio (OR)
0�86; 95% confidence interval (CI) 0�71–0�94], in the odds of
death or institutionalized care (OR 0�80; 95% CI 0�71–0�90)
and in the odds of death or dependency (0�78; 95% CI 0�68–
0�89) (21). This means that the number needed to treat to
prevent one death was 33, to prevent one patient being unable
to live at home was 20 and to prevent one patient failing to
regain independence was 20 (21).
Despite the grade I evidence of the efficacy of SUs based on
randomized studies and meta-analyses, there has not been a
generalized implementation of SUs, in contrast to that which
occurred with specialized coronary care units. We intend to
provide responses to the different questions raised regarding
the practical utility of SUs. These include: are they effective in
the management of stroke and are the benefits reproducible in
standard clinical practice? Are there alternative models? Who
benefits? Are SUs cost-effective? Is efficacy consistent within
the time of operation? Is the effectiveness comparable to other
therapeutic measures in the management of stroke patients?
How can the outcomes be improved? For this purpose, a
nonsystematic review of published studies that have specifi-
cally addressed any of those points of controversy or that have
added relevant knowledge to those questions was conducted.
Are SUs efficacious in the management of acutestroke and are the benefits reproducible in standardclinical practice?
One of the most consistent benefits demonstrated in the
randomized studies is the reduction in mortality, which is
clearest in the analysis of early mortality (5 days to 6 weeks), the
most frequent cause of death being pneumonia, recurrent
stroke and pulmonary embolism. In the first week following a
stroke, there are no significant differences with respect to the
effect of SU. This is probably due to the fundamental cause of
death in this period being directly related to the severity of the
stroke and is not modifiable by any specific therapeutic
intervention. From about 5 days onwards, however, a signifi-
cant reduction in mortality is observed in the patients receiv-
ing attention in the SU compared with those receiving
attention in the general medical ward (18, 19). Further, the
results of follow-up over 5–10 days of patients attended to in
the SU compared with the general medical ward show a higher
long-term survival in the former, and that this reduction in
mortality is maintained from the first 6 weeks. This indicates
that it is the treatment in the acute phase in the SU that
determines the better prognosis of the patients (22–24).
Another important aspect to consider is the neurological
recovery of the patients, because stroke is one of the principal
causes of adult dependency. The studies that analyzed this
aspect have shown that the functional status at discharge from
hospital improves in those patients attended to in the SU
compared with those in the general medical ward (18, 22–24).
& 2009 The Authors.Journal compilation & 2009 World Stroke Organization International Journal of Stroke Vol 4, February 2009, 28–37 29
B. Fuentes & E. Dıez-Tejedor Topical review

This, together with the reduction in mortality, is the most
important benefit obtained with the SUs i.e. increase in
survival at the cost of a greater proportion of patients being
dependent would be a poor outcome for the SU.
Once the advantages of the care provision in the SU have
been demonstrated, the factors that determine these benefits
need to be evaluated, and whether the benefits observed in the
randomized studies can be reproduced in standard clinical
practice. In the Stroke Care Outcomes: Providing Effective
Services (SCOPES) study, a prospective single-blind multi-
center study conducted in Australia, the adherence to a selected
set of clinically important processes of care, which included
aspects of care within 24 h of admission, documentation and
general management, was analyzed in three models of stroke
care (equivalent to SU, STand general medical care). The main
findings were that the adherence to those predefined processes
of care was associated with improved survival at discharge and
that adherence to those processes of care was higher in SU than
in other models (25). Similarly, in the PROSIT study per-
formed in Italia, a higher quality in terms of infra-structure
and organization in terms of diagnosis and the processes of
care was found in the SU group. However, the effects of these
components on the efficacy and effectiveness of stroke treat-
ment had not been analyzed sufficiently in this last study (26).
In 1997, the Cochrane meta-analysis, based on the observa-
tions of deaths from the illness, suggested that the benefits of
the SU are related to a reduction in the secondary complica-
tions of the stroke, especially the relationship with the hospi-
talization of the patient i.e. the majority of the deaths avoided
by the SU correspond to weeks 1–4 following the stroke (27). It
has been highlighted that an early commencement of patient
mobility and rehabilitation, together with stabilization of
Table 1 Nonsystematic selection of studies that compared models of care provision for stroke
Intensive care stroke units
Kennedy et al. (11) Prospective
Randomized
No differences in mortality; reduction in complications
Drake et al. (12) Retrospective
Nonrandomized
No differences in mortality; reduction in complications; trend toward reduction in
long-stay hospitalization
Pitner and Cornelius (13) Prospective Not effective with respect to mortality
Norris and Hachinski (14) Prospective
Nonrandomized
Not effective with respect to mortality
Intermediate care stroke units
Strand et al. (16, 17) Prospective
Randomized
Reduction in medium-stay hospitalization
Reduction in hospitalization in long-stay centers
Indredavik et al. (18, 22, 23) Prospective
Randomized
Reduction in mortality
Reduction in medium-stay hospitalization
Better functional status
Reduction in hospitalization in long-stay centers
Patient follow-up for between 5 and 10 years: persistent benefit in mortality and
functional status
Stroke teams
Wood-Dauphinee et al. (49) Randomized
General medical
No significant efficacy
Webb et al. (47) Prospective
Historical controls
Reduction in medium-stay hospitalization
Reduction in morbidity (k urinary infections)
Dey et al. (50) Prospective
Randomized
Premature termination of the study
No significant differences in mortality at 6 weeks or at 12 months
Stroke units vs. neurology ward
Krespi Y et al. (37) Before and after study Reduction in in-hospital case-facility
Shorter length of stay
Stroke units vs. stroke teams
Kalra et al.(51)
Evans et al. (32)
Randomized
Three groups:
– Stroke unit
– Stroke team
– Home care
Reduction in mortality at 3, 6 and 12 months
Better functional status at 3, 6 and 12 months
Reduction in complications
Dıez-Tejedor and Fuentes (30)
Fuentes et al. (70)
Prospective
Historical controls
Neurological setting
Better functional status at discharge
Reduction in medium-stay hospitalization
Reduction in complications
Reduction in long-stay hospitalization
Reduction in health costs
Consistent benefits with respect to function
Cadilhac and Ibrahim (25) Prospective
Single blind
Higher rates of adherence to key processes of care in SU than in other models
SU, stroke units.
& 2009 The Authors.30 Journal compilation & 2009 World Stroke Organization International Journal of Stroke Vol 4, February 2009, 28–37
Topical review B. Fuentes & E. Dıez-Tejedor

blood pressure, were the most important aspects in the health
care provision in the SU (28). In an observational study in
which the clinical evolution of the patients with acute stroke
in the SU was compared with historical controls attended to by
STs within the same department of neurology, the better
attention to the overall care of the patient with a reduction
in complications (systemic and neurological) was found to be
independent good prognostic factor not only with respect to
mortality or dependence but also chronic hospitalization (29–
31). Further, a post hoc analysis of a randomized study that
compared SU vs. ST concluded that the differences in the
management of the patients (with respect to the diagnostic
procedures and therapeutics) and the reduction of complica-
tions were the two factors that determine the greater efficacy of
the SU compared with the ST (32). The importance of SUs in
the reduction of complications, especially of infections and of
mortality associated with them, has been confirmed recently in
a systematic review (33).
Hence, it is evident that, apart from the organizational
differences, one of the fundamental aspects of the SU is the
specialized management of the patient in the acute phase,
especially with regard to overall care, with strict control of the
blood pressure, temperature, glycemia, oxygen saturation and
prevention of complications. Maintenance of homeostasis in
this phase has a direct impact on functional prognosis in the
short term (31, 34). Differences in the management of these
physiological parameters of the patients in acute phase deter-
mine, in great part, the different stroke-related mortality rates
in different countries (35). Further, the benefits of SUs are
reproducible in standard clinical practice and result in an
increase in patient transfer to home care and improvement in
functional status (29, 30, 36–38).
Are there alternative models for care provisionfollowing stroke?
� Nonneurological care: The majority of SU trials were
conducted in nonneurological wards and the benefits when
compared with general wards without specific stroke care
programs is clear. To date, there exist some controversies
regarding which medical specialist should manage acute stroke
patients (39–41). However, there are some studies suggesting
that specific neurological care could provide additional ben-
efits to stoke patients. Already in 1995 a randomized study that
compared the efficiency of the Neurology Department vs. that
of Medicine demonstrated a mean reduction in hospital stay,
improved the functional status at discharge from hospital and
an increase in the number of patients capable of returning
home in the group that was attended to in the neurology ward
(42). This was reinforced by a multicenter study of the Spanish
Stroke Study Group, which demonstrated that early care
(within the first 6 h) by the neurologist was related to a better
functional prognosis and shortening of hospital stay (43).
Other observational studies have shown better outcomes in
patients treated by neurologists as compared with other
specialists (44–46). Thus, in our opinion, although a multi-
disciplinary approach is the basis of SU care, neurologists
should have a key role in SU organization as it is recommended
by some societies (8, 9). In fact, in many countries in Europe,
SUs are predominantly set up in neurological departments (1).
� Stroke teams (STs): These are defined as multidisciplinary
teams available for the care of stroke patients in any hospital
environment. Generally, this would be composed of one or two
neurologists, a physiotherapist or occupational therapist and a
nurse specialized in care of the stroke patient. There have been
few studies conducted to assess the efficacy of STs. Initial
studies highlighted a benefit of STs in relation to the mean
reduction in hospital stay and in morbidity (decrease in
urinary infections) (47). Subsequent observational studies,
randomized trials and meta-analyses (29, 51, 48) that com-
pared STs with general medical wards (49, 50) and with SUs
(30) confirmed that the STs are not an effective alternative in
the care provision for patients with acute stroke (21, 52, 53).
Nevertheless, in those centers in which it is not feasible to set up
SUs, the ST could be considered as a valid organizational option
but always with the premise that those ST be integrated in a
Stroke care network with tight collaboration with a reference
center with an SU (Comprehensive Stroke Centre) (54).
� Care pathways: There have been, over the past few years, new
tools of clinical administration developed of note, among
which are clinical decision trees. This deals with care-provision
plans that define and regulate sequences of health-care activ-
ities or interventions for a defined group of patients with a
predictable clinical course and whose principal objective, is to
provide quality care for the patient based on the best scientific
evidence available. A further objective is to avoid the inter-
individual variation between health-care professionals. When
analyzing its efficacy in general neurology wards, set up as
an alternative to SUs, there were no benefits observed with
respect to the management of the patients whereas, conversely,
there was a trend towards a poorer clinical evolution of the
patient (55).
Which patients benefit from care in SUs?
Starting from the premise that, to achieve a benefit, all patients
with stroke, independent of severity, age or comorbidity
should be attended to in SUs, it is clear that on many occasions
the resources available in the SU, especially with respect to bed
availability, are limited. A health-care political priority would
be to select those patients who may benefit from SU attention.
Hence, in the studies published on SUs, there has been, with
disturbing frequency, a search for a patient profile that would
best benefit from the specialist attention. To date, there have
been analyses based on the severity of the stroke, age of the
patient, presence of comorbidity and stroke sub-type.
Analysis of the clinical evolution of the stroke patient
attended to in the SU compared with the general medical
ward with respect to age and grade of neurological involvement
have highlighted the presence of hemiparesis on admission to
& 2009 The Authors.Journal compilation & 2009 World Stroke Organization International Journal of Stroke Vol 4, February 2009, 28–37 31
B. Fuentes & E. Dıez-Tejedor Topical review

hospital and advanced age as factors determining mortality
and/or dependency. The effect of age depends on the moment
in which its impact is evaluated. For example, patients o75
years of age are those that benefit most from attention in the SU
in the short term because this attention accelerates the patient’s
neurological recovery; in the long term, however, the recovery
will be the same if the patient was attended to in the general
ward. Conversely, in patients 475 years of age, the differences
are modest initially but become statistically significant in favor
of the SUs in the years following the stroke (17). Another
circumstance that has been considered is the presence of
comorbidity especially in relation to the presence of concur-
rent heart disease i.e. patients with cardiac disease benefit more
at 3 months in terms of mortality and/or institutionalization
when attended to in SUs (17, 56).
The Cochrane meta-analysis of 2002 analyzed the differ-
ences between sub-groups of patients. The main conclusion
was that the benefits observed with the organized care and
specialized for stroke were not confined to a specific patient
sub-group. The analysis highlighted that clear benefits were
obtained in patients of either gender, of different age ranges
and independent of the grade of neurological involvement. The
more severe stroke patient groups have a higher mortality risk
inherent in the severity of the stroke, and are those patients who
benefit most in terms of mortality or dependency rates, the
benefit being less evident when mortality and institutionalized
care were assessed (21). Also of note is that patients with
preexisting functional dependency were not included in rando-
mized studies on SU but data from observational studies suggest
that they do not obtain a clear benefit from SU attention (57).
With respect to the stroke type, a few authors have analyzed
the possible differences in the benefits from SU care in terms of
mortality and functional recovery, despite the known differ-
ences in prognoses. In a post hoc analysis of a randomized trial
that compared SU against ST and home care, the prognostic
differences and associated costs were evaluated in patients with
nonlacunar cerebral infarction (CI) compared with patients
with lacunar strokes attended to in the SU vs. those receiving
ST attention in the general ward. In the group of patients with
large-vessel CI, attention provided by the ST was associated
with higher mortality probability at 3 months and at the end of
1 year and also mortality and institutionalization. In the group
with lacunar infarction, no significant differences were ob-
served in the prognosis at 3 months or at 1 year between the
two organizational models. However, there were higher costs
resulting from an increase in the mean hospital stay and greater
use of resources (physiotherapy, occupational therapy and
logopedia) (58). Nevertheless, the patients with lacunar strokes
benefited from SU attention as well, with a reduction in
complications and hospital stay apart from achieving a better
functional status at discharge from hospital. The significant
increase in patient independence was clearer in the multi-
variate analysis in which being treated in the SU was an
independent factor for a better prognosis with respect to the
dependency variable (59).
In relation to cerebral hemorrhage (CH), there have been
few studies that have specifically evaluated the benefits of SU in
the management of CH. The possible benefit (mortality
reduction) in the patients with CH attended to in the SU
compared with those in the general medicine ward and
compared with those receiving attention in the ST in the
neurology ward was noted for the first time in 1998 (60). The
study demonstrated a reduction in complications, mean
hospital stay and improvement in functional status associated
with the SU. Subsequently, in a controlled prospective study in
which 121 patients with stroke were randomized to an SU or to
a general medical ward, a significant decrease in mortality at
30 days and at 1 year was found in favor of the SU (61).
The majority of the studies that analyzed the efficacy of SUs
or STs did not include patients with TIA, and there are few
studies on the short-term prognosis or the diagnostic and
therapeutic implications of care provision for TIA. In observa-
tional studies, care provision for patients with TIA in the SU
was associated with a reduction in the mean hospital stay,
health-care costs and improved diagnostic efficiency com-
pared with those attended to in the same neurology ward by the
ST (29) with earlier application of specific treatments (62).
In summary, all the patients with acute stroke, independent
of age, severity, cardiac comorbidity or stroke sub-type, benefit
from care provision in SUs.
Are SUs cost-effective?
Taking into account elevated health-care costs and limitations
on resources, it is necessary to identify care-provision models
that are not only efficacious but also efficient. The costs of
acute stroke derive from hospital costs while, in the long term,
the costs are related mainly to the grade of the residual
incapacity of the patients. Direct costs are those derived from
the use of the health service resources (drugs, nursing care,
rehabilitation, y) and indirect costs are those that are implied
in the loss of productivity of the subject who has suffered a
stroke. At the time of assessing those with stroke, we need to
consider different variables: those in the acute phase, funda-
mentally attributable to hospital costs and directly related to
the mean hospital stay, and those of the long term, which are
derived from the care of the patient with functional depen-
dency requiring rehabilitation, short-stay hospitalization,
long-stay hospitalization, home care, etc (63). Clearly, the
care organization model that shows a reduction not only in the
mean hospital stay but also in the percentage of patients with
dependency at discharge from hospital can be considered as the
more cost-effective system.
The care provision in the several models of SU (acute care,
rehabilitation or mixed) is associated with a reduction in the
mean stay in hospital, despite the heterogeneity in the calcula-
tion of this variable (hospitalization in the acute phase, overall
duration of hospitalization and long-stay institutions) as
demonstrated in individual studies and in systematic reviewers
(16, 21, 29–30, 37, 47, 64–66). This reduction in hospital stay is
& 2009 The Authors.32 Journal compilation & 2009 World Stroke Organization International Journal of Stroke Vol 4, February 2009, 28–37
Topical review B. Fuentes & E. Dıez-Tejedor

associated with a reduction in hospital costs (30). Further, SU
care achieves an increased transfer to home care with less long-
term hospitalization (16–19, 27, 29, 30). Further, if we consider
that the SU improves the functional status at discharge from
hospital and that fewer patients are discharged to home-care
with physical dependencies, we observe a greater effectiveness
of SU, whose repercussion is a reduced burden on family and
on society.
With respect to the cost-effectiveness from the point of view
of the health economy, it has been highlighted over the past
few years that SU implementation has an increased cost due to
the increase in personnel and of the diagnostic/therapeutic
procedures, which reach 7% of the cost of the admission to
hospital and 15�6% if we consider the mean costs per day
of admission to general neurology wards (67). However,
although the costs related to resource use are generally higher
in SU as compared with conventional care, but similar to
mobile service, when outcomes are included in the analysis, SU
appears to be more cost-effective than either mobile stroke
teams or general medical care because of the potential health
benefits that can be achieved (68).
On the other hand, with the objective of calculating the
clinical and economic consequences of establishing SUs com-
pared with conventional care, the study conducted by Launois
et al. (69) in France is of considerable interest. Focusing
essentially on administration, the authors performed an
analysis in which the important variables included were the
grade of incapacity of the patients, the destination on discharge
from hospital and probability of stroke recurrence. These
variables were in addition to those usually considered in
economic studies on care provision such as the probability of
death or survival and the specific model of care provision. As
such, the study could be considered as the most comprehensive
cost-effectiveness study of stroke care provision conducted to
date. The study not only confirmed that the SU results in a
higher patient survival rate without sequelae in the 5 years of
follow-up but also, and more significantly from the perspective
of the administrative process, the SU cost-effectiveness ratio is
much lower than the threshold of acceptability recognized by
the scientific community. This finding justifies, as highlighted
by the authors of the study, the need for organizational changes
in the care provision for stroke patients, and that it is essential
that SUs are established in France. Certainly, these data cannot
be extrapolated to other countries but they do provide
important departure points, demonstrating, from the clinical
administration perspective, that the SUs are superior to
conventional care not only in terms of efficacy but also cost
i.e. the implementation of such units is clearly justified.
Are the benefits of SUs consistent over the time theyhave been in operation?
The majority of long-term studies performed have focused on
the follow-up at 5–10 years of patients initially attended to in
SUs. The authors of these studies demonstrated high survival
rates in the long term and an increase in the patient’s capacity
to return home (22–24). However, what remains to be
determined is whether the efficacy of the SU is maintained
over the period in which the SUs have been operating. This
question is of considerable importance because a possible bias
in the analysis of efficacy of a new organizational model is the
motivation and enthusiasm of those health-care professionals
involved in the initial implementation of such units. Further,
almost all randomized trials compared SUs with the attention
provided to stroke patients in other non-specific wards in
which the personnel did not follow the same protocols or
guidelines for the management than in the SU groups. As such,
some of the favorable results observed for SUs could be a
reflection of the greater dedication and specific care provided
by the SU personnel (7). Thus, the good outcomes not only in
the acute phase but also in the subsequent follow-up of the
patients in these studies could be due to the differences in the
clinical management related to each of the care-provision
models during the hospitalization phase, and not due to a real
benefit of the SU per se. The response to this criticism is that an
analysis has been performed of the functional status at 8 years
of the SU that demonstrated that the benefits of the SU in terms
of reductions in the mean hospital stay, mortality/dependency
and institutionalization were maintained over the period of 8
years analyzed and that, indeed, over the last few years, further
reductions in the mean hospital stays, intrahospital complica-
tions and a higher percentage of survival have been achieved
(70). As such, as with the health-care personnel and diagnostic
protocols/therapies, it is the specific attention provided in the
SU that determines the good results, and that have been
consistent over the time they have been in operation.
Is SU effectiveness comparable to othertherapeutic measures in the managementof stroke patients?
In 1999, Hankey and Warlow published an analysis of the
effectiveness of the different treatments available for acute-
phase CI, such as aspirin, fibrinolytic treatment tissue-type
plasminogen activator (rt-PA) and attention received in SUs.
The authors considered the impact of the application of these
treatments at the level of the community and on the overall
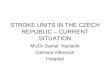
stroke load. Although thrombolysis would be the therapeutic
measure with the best numbers needed to treat (NNT; 16 for
thrombolysis vs. 18 for SU and 83 for aspirin), the analysis of
mortality and/or dependencies avoided showed 8�3% for SU
vs. 1�2% for thrombolysis and 1�8% for aspirin (Fig. 1) (71).
The cost-effectiveness analysis highlighted that the SUs are
highly cost-effective because they achieve an absolute benefit
similar to thrombolysis but can be applied to greater numbers
of patients (71). These data have been confirmed in a study
conducted by Gilligan and colleagues in which the eligibility of
the different specific treatments available (including further
hypothetical data on neuroprotection deduced from clinical
trials) was analyzed in a group of acute-stroke patients
& 2009 The Authors.Journal compilation & 2009 World Stroke Organization International Journal of Stroke Vol 4, February 2009, 28–37 33
B. Fuentes & E. Dıez-Tejedor Topical review

attended to in the hospital, and the results were extrapolated
to the general population. Of the patients, 83% would
be candidates for management in a specialized SU, 40% to
treatment with aspirin in the first 48 h and only 10% to
intravenous thrombolysis with rt-PA in the first 3 h (Fig. 1).
The authors concluded that greater benefit to the community
is achieved with SUs and that although all these therapeutic
measures should be accessible to the acute-stroke patients,
access to the SU needs to be considered a priority (72).
How can we improve the results of the SUs?
� Monitored SUs: Over a considerable period of time, the early
rehabilitation has been considered as the most important
component and determinant of efficacy. However, the study
by Indredavik et al. (28) highlighted the possible influence of
general care, particularly in relation to the control of blood
pressure and the early treatment of hypothermia; the impor-
tance of maintaining homeostasis of the patients is becoming
progressively more evident in terms of short-term prognosis
(34) and the reduction in the complications (30, 32, 33, 73).
These beneficial effects have been demonstrated in the SU in
which vital signs are noninvasively measured four times daily.
Over the past few years, several studies have been published
highlighting the importance of continuous monitoring of
these parameters and the implication in the patient’s prognosis
and have demonstrated lower mortality rates at 3 months (74)
and at 1 year (75). This benefit is probably due to a better
detection of complications (cardiac events, fever, hyperten-
sion, hypotension and hypoxia) in the monitored patients and,
hence, a more rapid deployment of appropriate therapy.
Because a lack of a properly designed study of conventional
SU with physiological variable measurement (blood pressure,
cardiac frequency, body temperature and oxygen saturation)
four times a day compared with SUs with continuous mon-
itoring of these same variables, there continues to be consider-
able controversy on the convenience and/or the desirability of
SUs with continuous monitoring (76–78). Currently, the cost
on continuous monitoring in SUs is advisable, but it is not vital
to implement a new SU in such a manner that the cost of
acquiring noninvasive monitors does not convert to being
inconvenient, being sufficient to monitor these vital signs
clinically because only this model of SU (nonmonitored) has
demonstrated cost-effectiveness in randomized trials.
� Care pathways: There have been several studies on the
implementation of care pathways of administration in the
care provision of stroke patients. These have focused on aspects
of rehabilitation and without analyzing the impact of these
clinical routes on acute-phase stroke. The emphasis has been
on increasing the diagnostic tests and reducing the risk of
urinary infections, and of re-hospitalization. However, there is
insufficient scientific evidence regarding their benefits in the
prognosis of vital function and status. As highlighted by the
Cochrane reviews (79–81), this is due to methodological
limitations such as a nonrandomized design in the majority
of trials. Only one study with historical controls had analyzed
the impact of the introduction of a new stroke care pathway in
an acute SU. The study showed a greater quality in the process
of diagnosis and a reduction in the urinary infection as an
intrahospital complication (82). Further, the care pathways
specifying the day-to-day diagnostic and therapeutic measures
that need to be applied to the stroke patients assure a continued
quality of care provision. The process should also include
greater monitoring and follow-up on weekends and holidays.
Admission into the SU on the weekend or in vacation periods
has been shown to be associated with a higher mortality rate
and poorer functional recovery, which can be attributed to
decreased numbers of clinical personnel, a lower multidisci-
plinary treatment intensity and a delay in the rehabilitation
process (83, 84). Hence, it is necessary to ensure continuous
care in the SU that includes not only an adequate proportion of
nursing care but also continuity in the diagnostic processes,
together with physiotherapy and rehabilitation, including on
weekends and holidays.
Final considerations, SUs: scientific and socialdemand
Since 1995, the World Health Organization (WHO) and
the European Stroke Committee have implemented the
10%Intravenous thrombolysis
NNT 16
Target population
AspirineNNT 83
80%
40%
Stroke UnitsNNT 18
Fig. 1 Effectiveness of the different treatments available for acute phase confidence interval (CI).
& 2009 The Authors.34 Journal compilation & 2009 World Stroke Organization International Journal of Stroke Vol 4, February 2009, 28–37
Topical review B. Fuentes & E. Dıez-Tejedor

Declaration of Helsingborg in which it was specified, as an
objective to be achieved by the year 2005, that all stroke
patients in the acute phase should have an early, and specia-
lized, evaluation and treatment in an SU. In the year 2006, the
revised Declaration of Helsingborg declared that by the year
2015 ‘all patients in Europe with stroke will have access to a
continuum of care from organized SU in the acute phase, to
appropriate rehabilitation, and to secondary prevention mea-
sures’ (85). Neurology scientific societies insist on the need to
establish SUs in the majority of hospitals, the option of STs
being acceptable only when it is not possible to implement
SUs (86–91).
Based on the scientific evidence, specialized neurology care
provision for stroke patients is not only a necessary and cost-
effective facility but also a social demand (92). As such, for
example in Spain, the Associations of Neurological Diseases
and the Spanish Society of Neurology [Sociedad Espanola de
Neurologıa] developed the ‘Madrid Declaration’ [Declaracion
de Madrid] in 2000, which proclaimed ‘the right of all citizens
to receive attention by an expert with specialist competence in
the different neurological pathologies, to have access to up-to-
date diagnostic and therapeutic techniques, and to be attended
to by specific interdisciplinary units in which they can obtain
all the help necessary for their health problem, with guarantees
of it being the best quality possible’ (93). More recently, the
Defensor del Pueblo in his report on overcoming cerebral
damage, recommended that the Health Authorities should
emphasize the early and specialized care for stroke patients by
creating specialized SUs to provide sufficient cover for the total
population (94). A questionnaire conducted among 1713
stroke patients receiving attention in hospitals in the United
Kingdom had a higher percentage of satisfaction with the
language and communication skills of the carers, with the basic
activities such as hygiene and alimentation, together with the
planning of care, rehabilitation and physiotherapy at discharge
from hospital as well as a greater confidence in the health-care
personnel (95).
In summary, the SU is the most efficacious care organization
model for acute stroke, even in comparison with STs. All
patients suffering from a stroke can benefit from attention
in the SU. These units are efficient and cost-effective, and
consistent over the time period of their operation. When the
community benefits of the different specific treatments for
stroke such as aspirin and intravenous thrombolytic agents are
considered, the SUs have a higher target population potential
and a higher benefit in terms of numbers of deaths or
dependencies avoided. As such, the SU is a necessary care-
provision facility that is also cost-effective.
References
1 Brainin M, Bornstein N, Boysen G, Demarin V: Acute neurological
stroke care in Europe: results of the European stroke care inventory. Eur
J Neurol 2000; 7:5–10.
2 Leys D, Ringelstein EB, Kaste M, Hacke W: Executive Committee of the
European stroke initiative: facilities available in European hospitals
treating stroke patients. Stroke 2007; 38:2985–91.
3 Rudd AG, Matchar DB: Health policy and outcome research in stroke.
Stroke 2004; 35:397–400.
4 Cadilhac DA, Lalor EE, Pearce DC, Levi CR, Donnan GA: Access to
stroke care units in Australian public hospitals: facts and temporal
progress. Int Med J 2006; 36:700–4.
5 Goldstein LB, Hey LA, Laney R: North Carolina stroke prevention and
treatment facilities survey. Statewide availability of programs and
services. Stroke 2000; 31:66–70.
6 Kapral MK, Laupacis A, Phillips SJ et al, for the Investigators of the
Registry of the Canadian Stroke Network : Stroke care delivery in
institutions participating in the Registry of the Canadian Stroke
Network. Stroke 2004; 35:1756–62.
7 Langhorne P, Dennis M: Stroke Unit. An Evidence-Based Approach.
London: BMJ Books, 1998.
8 The European Ad Hoc Consensus Group: European Strategies for early
intervention in stroke. A report of a Hoc Consensus Group Meeting.
Cerebrovasc Dis 1996; 6:315–24.
9 European Federation of Neurological Societies Task Force: Neurolo-
gical acute stroke care: the role of European Neurology. Eur J Neurol
1997; 4:435–41.
10 Leys D, Ringelstein EB, Kaste M, Hacke W, for the European Stroke
Initiative executive committee: The main components of stroke unit
care: results of a European expert survey. Cerebrovasc Dis 2007; 23:
344–52.
11 Kennedy FB, Pozen TJ, Gabelman EH, Tuthill JE, Zaentz SD: Stroke
intensive care – an appraisal. Am Heart J 1970; 80:188–96.
12 Drake WE Jr, Hamilton MJ, Carlsson M, Blumenkrantz J: Acute stroke
management and patient outcome: the value of Neurovascular Care
Units (NCU). Stroke 1973; 4:933–45.
13 Pitner SE, Cornelius JM: An evaluation of stroke intensive care: results
in a municipal hospital. Stroke 1973; 4:737–41.
14 Norris JW, Hachinski VC: Intensive care management of stroke
patients. Stroke 1976; 7:573–7.
15 Millikan CH: Stroke intensive care units: objectives and results. Stroke
1979; 10:235–7.
16 Strand T, Asplund K, Eriksson S, Hagg E, Lithner F, Wester PO: A non-
intensive stroke unit reduces functional disability and the need for
long-term hospitalization. Stroke 1985; 16:29–34.
17 Strand T, Asplund K, Eriksson S, Hagg E, Lithner F, Wester PO: Stroke
unit care – who benefits? Comparisons with general medical care in
relation to prognostic indicators on admission. Stroke 1986; 17:377–81.
18 Indredavik B, Bakke F, Solberg R, Rokseth R, Haaheim LL, Holme I:
Benefit of a stroke unit: a randomized controlled trial. Stroke 1991;
22:1026–31.
19 Jorgensen HS, Nakayama H, Raaschou HO, Larsen K, Hubbe P, Olsen
TS: The effect of a stroke unit: reductions in mortality, discharge rate to
nursing home, length of hospital stay, and cost. A community-based
study. Stroke 1995; 26:1178–82.
20 Langhorne P, Williams BO, Gilchrist W, Howie K: Do stroke units save
lives? Lancet 1993; 342:395–8.
21 Stroke Unit Trialists’ Collaboration: Organised inpatient (stroke unit)
care for stroke. Cochrane Database Syst Rev 2002: CD000197.
22 Indredavik B, Slordahl SA, Bakke F, Rokseth R, Haheim LL: Stroke unit
treatment. Long-term effects. Stroke 1997; 28:1861–6.
23 Indredavik B, Bakke F, Slordahl SA, Rokseth R, Haheim LL: Stroke unit
treatment. 10-year follow-up. Stroke 1999; 30:1524–7.
24 Jorgensen HS, Kammersgaard LP, Nakayama H et al. Treatment and
rehabilitation on a stroke unit improves 5-year survival. A com-
munity-based study. Stroke 1999; 30:930–3.
25 Cadilhac DA, Ibrahim J, for the SCOES Study Group: Multicenter
comparison of processes of care between stroke units and conventional
care wards in Australia. Stroke 2004; 35:1035–40.
& 2009 The Authors.Journal compilation & 2009 World Stroke Organization International Journal of Stroke Vol 4, February 2009, 28–37 35
B. Fuentes & E. Dıez-Tejedor Topical review

26 Bersano A, Candelise L, Sterzi R et al. Stroke Unit care in Italy.
Results from PROSIT (Project on Stroke Services in Italy). A
nationwide study. Neurol Sci 2006; 27:332–9.
27 Stroke Unit Trialists’ Collaboration: How do stroke units improve
patient outcomes? A collaborative systematic review of the randomized
trials. Stroke 1997; 28:2139–44.
28 Indredavik B, Bakke F, Slordahl SA, Rokseth R, Haheim LL: Treatment
in a combined acute and rehabilitation stroke unit: which aspects are
most important? Stroke 1999; 30:917–23.
29 Fuentes B, Diez Tejedor E, Frank Garcia A, Lara Lara M, Barreiro Tella
P: The organization of health care for stroke. The stroke units make the
difference. Rev Neurol 2001; 32:101–6.
30 Diez-Tejedor E, Fuentes B: Acute care in stroke: do stroke units make
the difference? Cerebrovasc Dis 2001; 11(Suppl. 1):31–9.
31 Diez-Tejedor E, Fuentes B: Acute care in stroke: the importance of early
intervention to achieve better brain protection. Cerebrovasc Dis 2004;
17(Suppl. 1):130–7.
32 Evans A, Perez I, Harraf F et al. Can differences in management
processes explain different outcomes between stroke unit and
stroke-team care? Lancet 2001; 358:1586–92.
33 Govan L, Langhorne P, Weir CJ: Stroke unit Trialists collaboration:
does the prevention of complications explain the survival benefit of
organized inpatient (stroke unit) care? Further analysis of a systematic
review. Stroke 2007; 38:2536–40.
34 Langhorne P, Tong BL, Stott DJ: Association between physiolo-
gical homeostasis and early recovery after stroke. Stroke 2000;
31:2518–9.
35 Bhalla A, Tilling K, Kolominsky-Rabas P et al. Variation in the
management of acute physiological parameters after ischemic
stroke: a European perspective. Eur J Neurol 2003; 10:25–33.
36 Stegmayr B, Asplund K, Hulter-Asberg K et al. Stroke units in their
natural habitat: can results of randomized trials be reproduced in
routine clinical practice? Risk-Stroke Collaboration. Stroke 1999;
30:709–14.
37 Krespi Y, Gurol ME, Coban O, Tuncay R, Bahar S: Stroke unit versus
neurology ward – a before and after study. J Neurol 2003; 250:
1363–9.
38 Seenan P, Long M, Langhorne P: Stroke units in their natural
habitat: systematic review of observational studies. Stroke 2007;
38:1886–92.
39 Caplan L: Stroke is best managed by neurologists. Stroke 2003; 34:2763.
40 Lees KR: Stroke is best managed by a neurologist: battle of the titans.
Stroke 2003; 34:2764–5.
41 Donnan GA, Davis SM: Neurologist, internist or strokologist? Stroke
2003; 34:2765.
42 Kaste M, Palomaki H, Sarna S: Where and how should elderly stroke
patients be treated? A randomized trial. Stroke 1995; 26:249–53.
43 Davalos A, Castillo J, Martinez-Vila E: Delay in neurological attention
and stroke outcome. Cerebrovascular Diseases Study Group of the
Spanish Society of Neurology. Stroke 1995; 26:2233–7.
44 Mitchel JB, Ballard DJ, Whisnant JP, Ammering CJ, Samsa GP, Matchar
DB: What role do neurologists play in determining the costs and
outcomes of stroke patients? Stroke 1996; 27:1937–43.
45 Goldstein LB, Matchar DB, Hoff-Lindquist J, Samsa GP, Horner RD:
VA Stroke Study. Neurologist care is associated with increased testing
but improved outcomes. Neurology 2003; 61:792–6.
46 Smith MA, Liou JI, Frytak JR, Finch MD: 30-day survival and
rehospitalization for stroke patients according to physician specialty.
Cerebrovasc Dis 2006; 22:21–6.
47 Webb DJ, Fayad PB, Wilbur C, Thomas A, Brass LM: Effects of a
specialized team on stroke care. The first two years of the Yale Stroke
Program. Stroke 1995; 26:1353–7.
48 Ovary C, Szegedi N, May Z, Gubucz I, Nagy Z: Comparison of stroke
ward care versus mobile stroke teams in the Hungarian stroke database
project. Eur J Neurol 2007; 14:757–61.
49 Wood-Dauphinee S, Shapiro S, Bass E et al. A randomized trial of
team care following stroke. Stroke 1984; 15:864–72.
50 Dey P, Woodman M, Gibbs A et al. Early assessment by a mobile
stroke team: a randomized controlled trial. Age Ageing 2005;
34:331–8.
51 Kalra L, Evans A, Perez I, Knapp M, Donaldson N, Swift CG:
Alternative strategies for stroke care: a prospective randomized con-
trolled trial. Lancet 2000; 356:894–9.
52 Langhorne P, Dey P, Woodman M et al. Is stroke unit care portable?
A systematic review of the clinical trials. Age Ageing 2005; 34:
324–30.
53 Stroke Unit Trialists’ Collaboration: Organised inpatient (stroke unit)
care for stroke. Cochrane Database Syst Rev 2007: CD000197.
54 Alvarez Sabin J, Alonso de Lecinana M, Gallego J et al. Plan for stroke
healthcare delivery. Neurologia 2006; 21:717–26.
55 Taylor WJ, Wong A, Siegert RJ, McNaughton HK: Effectiveness of a
clinical pathway for acute stroke care in a district general hospital: an
audit. BMC Health Serv Res 2006; 6:16.
56 Fagerberg B, Claesson L, Gosman-Hedstrom G, Blomstrand C:
Effect of acute stroke unit care integrated with care continuum
versus conventional treatment: a randomized 1-year study of
elderly patients: the Goteborg 701 Stroke study. Stroke 2000;
31:2578–84.
57 Glader EL, Stegmayr B, Johansson L, Hulter-Asberg K, Wester PO:
Differences in long-term outcome between patients treated in stroke
units and in general wards: a 2-year follow-up of stroke patients in
Sweden. Stroke 2001; 32:2124–30.
58 Evans A, Harraf F, Donaldson N, Kalra L: Randomized controlled study
of stroke unit care versus stroke team care in different stroke subtypes.
Stroke 2002; 33:449–55.
59 Fuentes B, Tejedor ED: Randomized controlled study of stroke unit
versus stroke team care in different stroke subtypes. Stroke 2002;
33:1740–1.
60 Ronning OM, Guldvog B: Stroke units versus general medical wards, I:
twelve- and eighteen-month survival: a randomized, controlled trial.
Stroke 1998; 29:58–62.
61 Ronning OM, Guldvog B, Stavem K: The benefit of an acute stroke unit
in patients with intracranial haemorrhage: a controlled trial. J Neurol
Neurosurg Psychiatry 2001; 70:631–4.
62 Calvet D, Lamy C, Touze E, Oppenheim C, Meder JF, Mas JL:
Management and outcome of patients with transient ischemic attack
admitted to a stroke unit. Cerebrovasc Dis 2007; 24:80–5.
63 Evers SM, Ament AJ, Blaauw G: Economic evaluation in stroke
research: a systematic review. Stroke 2000; 31:1046–53.
64 Ronning OM, Guldvog B: Stroke unit versus general medical wards, II:
neurological deficits and activities of daily living: a quasi-randomized
controlled trial. Stroke 1998; 29:586–90.
65 Wentworth DA, Atkinson RP: Implementation of an acute stroke
program decreases hospitalization costs and length of stay. Stroke 1996;
27:1040–3.
66 Odderson IR, McKenna BS: A model for management of patients with
stroke during the acute phase. Outcome and economic implications.
Stroke 1993; 24:1823–7.
67 Epifanov Y, Dodel R, Haacke C et al. Costs of acute stroke care on
regular neurological wards: a comparison with stroke unit setting.
Health Policy 2007; 81:339–49.
68 Moodie M, Cadilhac D, Pearce D et al. for the SCOPESStudyGroup:
Economic evaluation of Australian stroke services: a prospective,
multicenter study comparing dedicated stroke units with other care
modalities. Stroke 2006; 37:2790–5.
69 Launois R, Giroud M, Megnigbeto AC et al. Estimating the cost-
effectiveness of stroke units in France comparedwith conventional
care. Stroke 2004; 35:770–5.
70 Fuentes B, Diez-Tejedor E, Ortega-Casarrubios MA, Martinez P, Lara
M, Frank A: Consistency of the benefits of stroke units over years of
& 2009 The Authors.36 Journal compilation & 2009 World Stroke Organization International Journal of Stroke Vol 4, February 2009, 28–37
Topical review B. Fuentes & E. Dıez-Tejedor

operation: an 8-year effectiveness analysis. Cerebrovasc Dis 2006;
2:173–9.
71 Hankey GJ, Warlow CP: Treatment and secondary prevention of stroke:
evidence, costs, and effects on individuals and populations. Lancet
1999; 354:1457–63.
72 Gilligan AK, Thrift AG, Sturm JW, Dewey HM, Macdonell RA, Donnan
GA: Stroke units, tissue plasminogen activator, aspirin and neuropro-
tection: which stroke intervention could provide the greatest commu-
nity benefit? Cerebrovasc Dis 2005; 20:239–44.
73 Diez-Tejedor E, Fuentes B: Homeostasis as basis of acute stroke
treatment: stroke units are the key. Cerebrovasc Dis 2005; 20(Suppl
2): 129–34.
74 Sulter G, Elting JW, Langedijk M, Maurits NM, De Keyser J: Admitting
acute ischemic stroke patients to a stroke care monitoring unit versus a
conventional stroke unit: a randomized pilot study. Stroke 2003;
34:101–4.
75 Cavallini A, Micieli G, Marcheselli S, Quaglini S: Role of monitoring in
management of acute ischemic stroke patients. Stroke 2003; 34:2599–
603.
76 Steiner T: Stroke unit design: intensive monitoring should be a routine
procedure. Stroke 2004; 35:1018–9.
77 Indredavik B: Intensive monitoring should not be the routine. Stroke
2004; 35:1019–20.
78 Davis SM, Donnan GA: Stroke unit design: high tech versus low tech.
Stroke 2004; 35:1021.
79 Kwan J, Sandercock P: In-hospital care pathways for stroke: a Cochrane
systematic review. Stroke 2003; 34:587–8.
80 Kwan J, Sandercock P: In-hospital care pathways for stroke. Cochrane
Database Syst Rev 2004: CD002924.
81 Kwan J: Care pathways for acute stroke care and stroke rehabilitation:
from theory to evidence. J Clin Neurosci 2007; 14:189–200.
82 Kwan J, Hand P, Dennis M, Sandercock P: Effects of introducing an
integrated care pathway in an acute stroke unit. Age Ageing 2004; 33:362–7.
83 Hasegawa Y, Yoneda Y, Okuda S et al. The effect of weekends and
holidays on stroke outcome in acute stroke units. Cerebrovasc Dis
2005; 20:325–31.
84 Saposnik G, Baibergenova A, Bayer N, Hachinski V: Weekends: a
dangerous time for having a stroke? Stroke 2007; 38:1211–5.
85 Kjellstrom T, Norrving B, Shatchkute A: Helsingborg Declaration 2006
on European stroke strategies. Cerebrovasc Dis 2007; 23:231–41.
86 Egido JA, Alonso de Lecinana M, Martinez-Vila E, Dıez-Tejedor E:
Guidelines for the treatment of acute cerebral infarct; in Dıez-Tejedor E
(eds): Guidelines for the Treatment and Prevention of Stroke 2002.
Neurologıa 2002; 17 (Suppl. 3):43–60.
87 Alonso de Lecinana M, Egido JA: Management of cerebral infarction in
the acute phase. Ad hoc editorial committee of the task force on
cerebrovascular diseases of Spanish Society of Neurology. Neurologia
1998; 13(Suppl. 3):13–23.
88 European Stroke Initiative recommendations for stroke management:
European Stroke Council, European Neurological Society and Eur-
opean Federation of Neurological Societies. Cerebrovasc Dis 2000;
10:335–51.
89 Adams Jr HP, Adams RJ, Brott T et al. Guidelines for the early
management of patientswith ischemic stroke: a scientific statement
from the stroke council of the American Stroke association. Stroke
2003; 34:1056–83.
90 Hacke W, Kaste M, Skyhoj Olsen T, Bogousslavsky J, Orgogozo JM:
Acute treatment of ischemic stroke. European Stroke Initiative (EUSI).
Cerebrovasc Dis 2000; 10(Suppl. 3):22–33.
91 Hacke W, Kaste M, Bogousslavsky J et al. European Stroke Initiative
Recommendations for Stroke Management – update 2003. Cere-
brovasc Dis 2003; 16:311–37.
92 Fuentes B, Diez Tejedor E: Stroke unit: a cost-effective care need.
Neurologia 2007; 22:456–66.
93 Declaracion de Madrid. Available at: http://www.sen.es/pdf/declara-
cion_madrid.pdf
94 Defensor del Pueblo: Dano cerebral sobrevenido en Espana. Un
acercamiento epidemiologico y sociosanitario. Available at: http://
www.defensordelpueblo.es/documentacion/informesmonograficos/
INFORMEDANIO.zip, 2005
95 Mayor S: Stroke patients prefer care in specialist units. BMJ 2005;
331:130.
& 2009 The Authors.Journal compilation & 2009 World Stroke Organization International Journal of Stroke Vol 4, February 2009, 28–37 37
B. Fuentes & E. Dıez-Tejedor Topical review