Embed Size (px)
DESCRIPTION
Subject Seminar
Citation preview

SUBJECT SEMINAR ON APPROACH TO STRIDOR
28.6.2010

2
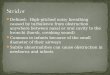
STRUCTURES OF THE UPPER AIRWAY

3
DEFINITION
Stridor, a harsh, medium-pitched, inspiratory sound associated with obstruction of the laryngeal area or the extrathoracic trachea, often accompanied by a croupy cough and hoarse voice

4
Turbulent air flow through partially obstructed / narrowed airway.
Stridor is a symptom, not a diagnosis or disease, and the underlying cause must be determined.
Stridor may be inspiratory, expiratory, or biphasic
-Inspiratory stridor = extrathoracic lesion (eg, laryngeal, nasal, pharyngeal).
-Expiratory stridor = intrathoracic lesion (eg, tracheal, bronchial).
-Biphasic stridor suggests a subglottic or glottic anomaly

5
PATHOPHYSIOLOGY During normal inspiration extrathoracic intraluminal airway
pressure is negative relative to atmospheric pressure, leading to collapse of supraglottic structures.
In contrast, stridor caused by intrathoracic obstructions tends to be more prominent on expiration. On expiration, intrathoracic pressure is positive and tends to collapse the airway.

6
DISEASES ASSOCIATED WITH ACUTE STRIDOR Acute laryngotracheitis.
Acute laryngotracheobronchitis.
Acute epiglottitis.
Bacterial tracheitis.
Foreign body.
Uncommon Peritonsillar abscess.
Retropharyngeal abscess.
Diphtheria

7
SIGNS OF WORK OF BREATHING
Tachypnoea
Chest retractions (SC / IC / SS )
Stridor / Wheeze / Grunt
Flaring of Ala nasi
Head bobbing
Abdominal breathing

8
Respiratory distress – Clinical pearlsRespiratory distress – Clinical pearls
Supra-sternal indrawingSupra-sternal indrawing(Use of accessory muscles, Upper airway (Use of accessory muscles, Upper airway
involvement)involvement)
Intercostal indrawingIntercostal indrawing(Decreased Parenchymal Compliance)(Decreased Parenchymal Compliance)
Subcostal indrawingSubcostal indrawing(Increased work of diaphragm)(Increased work of diaphragm)

9
SOUNDS DURING RESPIRATORY CYCLE
Stridor(Extra thoracic airway structures)
Wheeze(Intra thoracic airway structures)
Grunt(Parenchymal lesions)

10
RESPIRATORY NOISES
Noises Phase of Respiration Localisation
Snoring Insp. / Exp. Oro-pharynx
Stridor Inspiration Larynx
Wheeze Expiration Small AW
Grunt Expiration Alveoli

11
5 DIFFERENCES BETWEEN PEDIATRIC AND ADULT AIRWAY
Relatively larger tongue
Angled vocal cords
More anterior and cephalax larynx
Funneled shaped larynx-narrowest part of pediatric airway is cricoid cartilage
Differently shaped epiglottis

12
PHYSIOLOGY: EFFECT OF EDEMA
Poiseuille’s law Poiseuille’s law
R = 8nl/ R = 8nl/ ππrr44
If radius is halved, resistance increases 16 x If radius is halved, resistance increases 16 x Image from: http://www.hadassah.org.il/NR/rdonlyres/59B531BD-EECC-4FOE-9E81-14B9B29D139B1945/AirwayManagement.ppt

13

ANATOMIC CLASSIFICATION
BROAD SPECTRUM OF NEONATAL AIRWAY ABNORMALITIES

15

16

17
VIRAL CROUP
Common respiratory illness in young children.
Anglo-Saxon word Kropan; cry aloud.
Hoarse voice; dry barking cough; inspiratory stridor; and variable amount of respiratory distress that develops over a brief period of time.

18
CROUP SYNDROME
Group of diseases that varies in anatomic involvement and etiologic agents.
Laryngotracheitis.
Spasmodic croup.
Bacterial tracheitis.
Laryngotracheobronchitis.
Laryngotracheobronchopneumonitis.

19
CROUPACUTE LARYNGOTRACHEITIS
Disease of viral origin causing subglottic & tracheal swelling.
The narrowed airway is responsible for the hallmark of clinical picture.
The cricoid ring in the upper trachea which is subglottic, has a narrow diameter which renders children vulnerable to inflammation.

20
VIRAL CROUP( ACUTE LARYNGOTRACHEITIS)
Etiology: Respiratory viruses e.g. parainfluenza viruses
1,2,and 3, RSV, Influenza viruses A & B.
Clinical picture: Age 6mths- 3 years, M>F, Fall & winter. Gradual onset of low grade fever,URTI, barking
cough, inspiratory stridor & respiratory distress.
Hoarseness & aphonia may occur.

21
CROUP, DIAGNOSIS & TREATMENT
Clinically Lateral neck X-ray ( steeple sign). Fluid intake Cool mist/ hot steamy bathroom. Aerosolized adrenaline. Steroids( controversial) Endotracheal intubation. Helium-Oxygen Mixture. Antibiotics

22
ACUTE EPIGLOTTITIS, ETIOLOGY
Bacterial infection of the supraglottic structures (epiglottis, aryepiglottic folds & arytenoids soft tissues) causing rapid airway obstruction.
Haemophilus Influenza type B in prevaccination era.
Bacteria associated with epiglottitis in the Hib vaccine era include: HiA, Str. Pn, Staph aureus, ß-hemolytic streptococci Gps A,B,C,and F

23
ACUTE EPIGLOTTITIS, CLINICAL PICTURE
Age usually 2- 7 years.
Sudden onset.
High fever.
Apprehensive, sitting forward, drooling saliva, hyperextended neck & protruded chin.
Stridor, dysphagia.

24
ACUTE EPIGLOTTITIS, DIAGNOSIS & TREATMENT
Direct visualization. Blood cultures. Latex agglutination of serum or urine. Treatment is a medical emergency. Ventilatory support, intubation. IV antibiotics, 2nd or 3rd generation
cephalosporin's or chloramphenicol till cultures & sensitivity are known.

25ASSESSMENT- DOWNE’S
SCORE0 1 2
Stridor None Inspiratory Inspiratory + expiratory
Cough None Hoarse Barking
Retractions None Suprasternal Flaring + max.retractions
Cyanosis None In air In 40% oxygen
Breath sounds
Normal Harsh,wheeze/ rhonchi
+ delayed

26
CharacteristCharacteristicic
EpiglottitisEpiglottitis CroupCroup
AgeAge Any ageAny age 6months-6months-12yrs12yrs
OnsetOnset SuddenSudden GradualGradual
LocationLocation SupraglotticSupraglottic SubglotticSubglottic
TemperaturTemperaturee
High feverHigh fever Low-grade Low-grade feverfever
DysphagiaDysphagia SevereSevere Mild or Mild or absentabsent
DyspneaDyspnea PresentPresent PresentPresent
DroolingDrooling PresentPresent PresentPresent
CoughCough UncommonUncommon Characteristic Characteristic coughcough
PositionPosition Leaning forward, Leaning forward, mouth openmouth open
comfortablecomfortable
X-RayX-Ray Thumb signThumb sign Steeple signSteeple sign

27
ETIOLOGYLaryngotracheobronchitis (croup) Parainfluenza virus Adenovirus Echovirus Influenza viruses Respiratory Syncytial viruses Mycoplasma Epiglotitis H.influezae

28
CLINICAL FEATURES
Epiglotitis- acute onset, fever, sore throat, hoarseness, and noisy breathing. Retraction of the suprasternal & infrasternal chest.
Look for the 4 Ds Dysphagia Dysphonia (Hot potato voice) Drooling Distress

29
EPIGLOTITIS

30
EPIGLOTITIS

31
CLINICAL FEATURES
LARYNGITIS
Barking cough , fever
Tachypnea, dyspnea,subglottic obstruction, inspiratory stridor
Retraction of the suprasternal notch and supraclavicular retractions

32
CLINICAL FEATURES
Laryngotracheobronchitis
Also called viral croup or just croup
Fever is higher, restlessness & air hunger
Demonstrate substernal & intercostal retractions in addition to suprasternal notch & supraclavicular retraction.
A barky cough, bronchitic inspiratory rales & expiratory wheezes are heard

33
CROUPUSUALLY INVOLVES LARYNX TRACHEA, AND VARIABLE PART OF
BRONCHI.

34
DIAGNOSIS
Etiology should be determined
Look for hoarseness, barking cough, inspiratory stridor and retractions
Throat swabs & smears are cultured and examined
Other airway obstructions should be considered
Serological tests

35
X-RAY
A positive thumb sign on lateral X-ray of neck is diagnostic of epiglottitis.
The "steeple sign" in an anteroposterior neck X-ray is characteristic of viral croup (acute laryngotracheobronchitis).

36
X-RAYCROUP

37
Croup
This radiograph shows a long area of narrowing extending below the Normally narrowed area at the level of the vocal cords.

38
EPIGLOTTITIS

39
THERAPY
Two fold Maintenance of an adequate airway Control of infection
H. influenzae - ampicillin or chloramphenicol.
C. diphtheriae - antitoxin & erythromycin or penicillin G.

40
DRUGS IN MANAGEMENT
GLUCOCORTICOIDS
Dexamethasone - most potent, long acting & can be given orally or parenterally.
Budesonide - lower systemic bioavailability, provides greater benefit as it is deposited in upper airway
Epinephrine - short term benefit by reducing secretions & mucosal edema. effective in severe cases.

41

42

43
MIST THERAPY
Blow-by or nebulisation method
Humidified air
Benefits- soothes inflamed airway, decreases airway obstruction by reducing viscosity of secretions, improves respiratory flow pattern.

44
MANAGEMENT - MILD CROUP
Minimal interference
Continue oral feeds
Steroids-budesonide 2mg in 4ml NS
Improvement discharge
No improvement treat as moderate croup

45
MANAGEMENT - MODERATE CROUP
Oxygen if spo2<95%
Nebulised adrenaline1:1000.1st dose 1ml in 3ml NS.2nd dose 0.5ml/kg(max 4 dose)
NPO. IV Fluids.
Steroids - Dexamethasone 1mg/kg IV stat,then q 8hr for 2-3 days.
Budesonide nebulisation 2 mg in 4 ml NS single dose.

46
MANAGEMENT - SEVERE CROUP
Oxygen. Iv fluids. Nebulised adrenaline. Steroids -IV dexamethasone + budesonide neb. Artificial airway .
ET tube – one size smaller than recommended
Quickly by experienced person
preferably under halothane anesthesia.

LARYNGOMALACIALARYNGEAL CONDITIONS
Inspiratory collapse of arytenoids, aryepiglottic folds and epiglottis
Anatomic, neurologic and inflammatory factors
Symptoms:
stridor, respiratory distress
possible feeding difficulties
weak cry
vary with position and activity
Onset usually delayed several weeks

LARYNGOMALACIALARYNGEAL CONDITIONS
Treatment
Supportive
Monitor symptoms, weight and feeding
Role of antireflux medications (PPI, H2RA)
Aryepiglottiplasty division of the short aryepiglottic
folds

VOCAL CORD PARALYSIS
LARYNGEAL CONDITIONS
2nd most common neonatal laryngeal anomaly Causes about 10% of congenital airway
obstruction Etiology
increased ICP injury to vagus nerve injury to left recurrent laryngeal nerve 20% result from traumatic birth

VOCAL CORD PARALYSIS LARYNGEAL CONDITIONS
Clinical Findings
Inspiratory stridor
Cyanosis, apneas (bilateral)
Weak/hoarse cry, aphonia (unilateral)
Feeding difficulties (unilateral)
Diagnosis
direct laryngoscopy
Treatment
expectant
reduce ICP (if present)
Tracheostomy (bilateral)

LARYNGEAL WEBLARYNGEAL CONDITIONS
Etiology- failure of laryngeal recanalization complete occlusion by mucosal and submucosal tissue
partial occlusion by a thin membranous web
Incidence- 1/10,000 births Clinical findings
stridor
weak or absent cry
not positional
Treatment Perforation, excision, dilation,
Cryotherapy, CO2 laser

SUBGLOTTIC HEMANGIOMA
Relatively rare 50% are associated
with cutaneous hemangiomas
Symptomatic within first 2 months, and present before 6 months
Present with inspiratory stridor

SUBGLOTTIC STENOSISLARYNGEAL CONDITIONS
Narrowing of the subglottic airway
housed in the cricoid cartilage
narrowest area of airway
Congenital and acquired
Most common abnormality requiring trach in children <1yr

ACQUIRED SUBGLOTTIC
STENOSISFACTORS IMPLICATED IN ITS
DEVELOPMENT
ETT size relative to child’s larynx
Duration of intubation
Motion of the tube
Repeated intubations
Factors affecting wound healing
Laryngotracheal reflux
Infection (historically tuberculosis and diphtheria)

55
DO`S & DON`TS IN SEVERE CROUP
DO`S Treat on priority basis Relieve anxiety Humidified oxygen Portable x-ray neck If pus-antibiotics & send
investigation Consult ENT surgeon or
anaesthetist
DONT’S Do not panic. Don`t disturb sleep. comfort the child,Avoid crying. Don`t send to x-ray room. Don’t neglect child till x-ray. No IVF or venepuncture until
airway is secured Do not wait for culture for
antibiotics

56
IMPORTANT POINTS
Symptomatic child with increased work of breathing should be treated with glucocorticoids
Rx may be with dexamethasone or nebulised budesonide
Use L/ Epinephrine for moderate or severe croup
Glucocorticoids reduce hospitalisation
Injectable dexamethasone provides more benefit than nebulised budesonide

57
EPIGLOTTITIS
Stabilize airway under controlled situation.
Antibiotics – ampicillin and chloramphenicol or 3rd generation cephalosporins.
Bacterial tracheitis - Use appropriate antibiotics.

58
PROGNOSIS
Depends on severity of illness
Complications -obstruction of the airway, atelectasis, pneumothorax, obstructive mediastinal emphysema, and bronchopneumonia
morbidity and mortality of epiglottitis can be very high with bacteremia often resulting in meningitis, septic arthritis or osteomyelitis .

59
RECURRENT
Allergic (spasmodic) croup
Respiratory infections in a child with otherwise asymptomatic anatomic narrowing of the large airways
Laryngomalacia

60
PERSISTENT STRIDOR - CAUSES
Laryngeal obstruction
Laryngomalacia
Papillomas, other tumors
Cysts and laryngoceles
Laryngeal webs
Bilateral abductor paralysis of the cords
Foreign body

61
TRACHEOBRONCHIAL DISEASE
Tracheomalacia
Subglottic tracheal webs
Endotracheal, endobronchial tumors
Subglottic tracheal stenosis

62
EXTRINSIC MASSES
Mediastinal masses
Vascular ring
Lobar emphysema
Bronchogenic cysts
Thyroid enlargement
Esophageal foreign body
Tracheoesophageal fistulas

63
OTHER
Gastroesophageal reflux
Macroglossia, Pierre Robin syndrome
Cri-du-chat syndrome
Hysterical stridor
Hypocalcemia
Vocal cord paralysis
Chiari crisis

64
SYMPTOMS OF LARYNGOMALACIA
Onset typically days to weeks after birth
Most commonly within the first 2 weeks of life
Inspiratory stridor
Low pitch with a fluttering quality secondary to circumferential rimming of the supraglottic airway and
aryepiglottic folds
More prominent when child is
Supine
Agitated
Louder quality with more forceable inspiration
Often associated with general noisy respiration

65
DIAGNOSIS OF LARYNGOMALACIA
Clinical assessment
Suspect laryngomalacia in a neonate with auscultation of inspiratory stridor
Confirm suspicion with flexible laryngoscopy

66
FLEXIBLE LARYNGOSCOPY FINDINGS WITH
LARYNGOMALACIA Cyclical collapse of supraglottic larynx with inspiration
Short aryepiglottic folds
Draw the cuneiform and corniculate cartilages forward over the laryngeal inlet resulting in prolapse during inspiration

67
LARYNGOMALACIA SEEN BY FLEXIBLE
LARYNGOSCOPY

68
THANK YOUTHANK YOU