Embed Size (px)
Citation preview

PROPERTIES OF SOFT TISSUE-
Response To Immobilization And Stretch

TYPES OF TISSUES• Contractile
Muscle, tendon, musculotendinous junction, tenoperiosteal junction
• Non contractile / Inert Capsule, ligament, blood vessels, articular cartilage, bursa, Dura, etc

The ability of the body to move freely,i.e. without restrictions and with control during functional activities, is dependent on
• passive mobility of soft tissues• active neuromuscular control. The soft tissue that become restricted
and impair mobility are muscles with their contractile and non contractile elements and various types of connective tissue ( tendons, ligaments, joint capsules, fascia, skin).

• It’s the decreased extensibility of connective tissue not the contractile elements of muscle tissue which is the primary cause of restriction ROM.
• Changes when soft tissues are stretched
elastic , viscoelastic, plastic

• ELASTICITY: it is ability of soft tissue to return to
its prestretch resting length directly after a short duration stretch force has been removed.eg. Contractile & non contractile
• VISCOELASTICITY: it is time dependent property of soft
tissue that initially resist deformation of tissue when stretch force is first applied.if force is sustained, viscoelaasticity allows a change in length of tissue and enables the

tissue to return gradully to prestretch state after the stretch force is removed.
eg. Connective tissues• PLASTICITY : it is the tendency of soft
tissue to assume a new and a greater length after the stretch force is removed. Eg. Contractile and non contractile tissues

Mechnical Properties of Contractile Tissue
• Muscle - contractile elements contractility and irritability - non contractile connective tissue resist deforming force connective tissue- innermost endomysium separates myofibrils perimysium encase fibre bundle


• Epimysium envelope fascial sheath around entire muscle.
-adhesions
contractile elemnts of muscleMuscle muscle fibres
myofibrils sarcomeres myofilaments of
actin and myosin


Response to stretch:• During passive stretch both longitudinal
and lateral force transduction occurs.• Initial lengthening-sharp rise in tension • After a point, there is mechanical
disruption of cross-bridges as filaments slide apart, leading to abrupt lengthening of sarcomere (sarcomere give)
• After release of force gain normal length.


Response to immobilization and remobilization
morphological changes:• Decay of contractile protein• decrease in muscle fibre dia. • dec in no. of myofibrils• Dec in cross sectional size of m fibres
over time• Significant deterioration in motor unit
recruitment reflected in emg • dec in intramuscular capillary density

– atropy and weakness – inc fibrous and fatty tissue in muscle.
tonic(slow twitch)postural > phasic(fast twitch)

IMMOBILIZATION IN SHORTENED POSITION
• Reasons???• Reduction in length of muscle and its
fibre• In no. of sarcomere in series within
myofibrils as a result of sarcomere absorption – muscle atrophy and weakness
• Shift to left in length-tension curve • Frank-Sterling’s law???


IMMOBILIZATION IN LENGTHENDED POSITION
Application of serial casts,use of dynamic splints to stretch a long standing contracture or inc ROM
• Muscle adapts by inc in no. of sarcomere in series(myofibrillogenesis)
may lead to permanent form of m lengthening if newly gained length is used in regular basis in ADL.
• prestate if not use in 3 to 5 weeks.

Neurophysiological Properties of Contractile tissue
• Two sensory organs, Muscle spindle & golgi tendon organ – convey information to the CNS about muscle tendon unit & affect a muscle response to stretch.


• Muscle spindle:-functn to rcv and convey
information abt change in length of m and velocity of length change
-intrafusal, types??, motor neuron at ends?? , Ia n IIa sensory fibre,
-primary respond to quick n sustain stretch-bag
-sec only to sustain- chain

• Golgi tendon-musculotendinius junctn-monitor change in tension of m t
unit being stretch
• Neurophysiological response of m to stretch..
-reciprocal inhibition-autogenic inhibition

Mechanical Properties of Non Contractile Soft Tissue
• Composition of connective tissue - collagen -elastin and reticulin -nonfibrous ground tissue

• Collagen fibers:-strength and stiffness of tissue-resist tensile deformation-joint stability
Tropocollagen-building block of collegen microfibrils



• Elastin fibers:- ↑ Elastin – Greater flexibility-Smaller in diameter than collagen
fibers, branch & join together to form a network within a tissue
-Consists of protein elastin surrounded by glycoprotein - fibrillin
-grt elongation with small load,break at higher load

• Reticulin fibers: -provide tissue with bulk• Ground Substance:-made up of proteoglycans(PGs) and
glycoprotein.-Component of connective tissues
between the cells & fibers-Supports cells & binds them together,
stores water, & provides a medium through which substances are exchanged between the blood & cells

1.Reduces friction 2.transport nutrients 3.Prevent excessive cross linking
between fibers.• PG – stabilize collagen network,
hydrate matrix, resist compresive force
• Glycoproteins – Linkage between matrix components & between the cells & matrix components.

Mechanical Behaviour of Noncontractile Tissue
It depends on collagen, PGs• ↑ in collagen , ↓ in PGs ---- resist high tensile load • ↑ in conc. of PGs - withstand
greater compressive load

• Collagen…. - Tension generation -10% collagen elongate for 150%
elastin elongate -collagen 5 times strong thn elastin -alignment reflects tensile force tendon, skin, ligaments, jt
capsules

Interpreting Mechanical Behaviour of Connective
Tissue:Stress-Strain Curve • Stress – force per unit area
resistance to external load• Kinds -tension -compression -shear• strain –amount of deformation tht occurs
when load or stretch force is applied


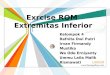
STRESS - STRAIN CURVE 33
STRESS
STRAIN
TOE REGION
ELASTIC RANGE
ELASTIC LIMIT
PLASTIC RANGE
NECKING
FAILURE
STRESS – STRAIN CURVE

Regions of the stress - strain curve
• Toe region• Elastic range/linear phase• Elastic limit• Plastic range• Ultimate strength• Failure• Structural stiffness

Connective tissue responses to loads
• Creep – Related to viscosity & time dependent• Stress - relaxation• Cyclic loading & connective tissue loading

Changes in Collagen affecting Stress-Strain Response
• Effects of immobilization• Age• Inactivity(Dec in normal activity)• Corticosteroid• Injury

Determinants of Stretching interventions
• Alignment• Stabilization• Intensity of stretch• Duration of stretch shorter the duration –
greater the no of repetitions & vice versa)• Speed of stretch• Frequency of stretch• Mode of stretch

broad categories of stretching exercise
-Static stretching-cyclic stretching-ballistic stretching-stretching tech based on principles
of pnf other types- manual or mechanical -active or passive -self

Alignment • Positioning a limb or the body such
that the stretch force is directed to the appropriate muscle grp.
-for comfort n stability during ex.-influence the amount of tension in soft
tissue and affect ROM available in jts.Eg : rectus femoris stretchAlternate position in case of discomfort,
inadequate nmsclr control, cardiopulmonary capacity.

Stabilization• Fixation of one site of attachment of
muscle as the stretch force is applied to the other bony attachment.
-either proximal or distal site-Manual stretching–proximal-Self stretching- distal-Multiple seg stabilizatin 4 effective stretchEg iliopsoas stretch

• Sources of stabilization-manual contact, body weight or firm surface such as table, wall or floor

O the Intensity of stretch• Magnitude of the stretch force
applied-it is determined by load placed on soft
tissue to elongate it.Low intensity stretch better than high
intensity-maneuver more comfortable-minimize vol or invol muscle guarding
so pt remain relaxed or assist with stretching maneuver.

-good for inc ROM without exposing the weakened tissue to excessive loads n potential injury.
-effective for dense connective tissue elongation with less soft tisssue damage and post ex soreness thn high int stretch

Duration of stretch• The period of time a stretch force is
applied and shortened tissue is held in a lengthened position
-safe, effective ,practical and efficient for each situation.
-Inverse relation betn I and D I and F30 sec twice = 10 sec 6 timesBut 15 sec thrice significant thn 5 sec
9 times

Long duration stretch- static, sustained, maintained and prolonged
Short duration stretch- cyclic, ballistic, or intermittent
no specific time period assign

• Static stretching- Here softt tissues are elongated just
past point of tissue resistance and then held in lengthened position with a sustain stretch force over a period of time.
- Effective to inc flexibiity, safer- Tension half - Contractile n non-contractile tissues less tissue trauma and less m
soreness

• Static progressive stretching-capitalize on stress relaxation
properties of soft tissue Eg dynamic orthosis

• Cyclic (intermittent) stretching- A relatively short duration stretch
force tht is repeatedly but gradually applied, released and thn reapplied is described as cyclic stretch.
- Applied for multiple repetitions during single treatment session.
- Slow vel controlled manner n low int.

Speed of stretch• slowly applied stretch - ensure optimal m relaxation - prevent injury -less likely to inc tensile stress on
conn tissue, inc tnsn in contractile tissue, activate stretch reflex

• Ballistic stretching -A rapid, forceful intermittant
stretch-tht is, a high speed and high intensity stretch- is called ballistic stretching.
-greater trauma and m soreness -not recommended for elderly or
sedentary individuals or pts with mskltl pathology or chronic contracture… reason??
- athlete , young active pt

• Frequency of stretch-no. of bouts per day or per week -depend on underlying cause of impaired mobility quality and level of tissue healing chronicity and severity of contracture pts age use of cortcosteroids- sessions??

• If there is progressive loss oof ROM over time rather thn gain in range, continued low grade inflammation from repetitive stress can cause excessive collagen formation and hypertrophic scarring.

• Mode of stretching• Form or manner in which the - stretch force is applied (static,
ballistic, cyclic) ; - degree of pts
participation(passive, assisted, active);
- or the sourse of the stretch force(manual, mechanical, self)

• It is imperative tht shortened m remains relaxed n tht connective tissue yield as easily as possible to stretch.
for this stretch procedure shud b preceded by either low intensity active ex or heat to warm up tissue

Manual stretching