Embed Size (px)
Citation preview

Stress and Disease Dr. Donald B. Giddon
Harvard University, Fall 2013
Pain
1

Pain
• As response to stress affecting particular organ system (QIII)
• Illness response to disease (Question IV)
2

Dimensions of pain experience• Sensory-discriminative
– Rapidly conducting spinal systems
• Motivational-affective- – Unpleasant experiences that motivate person to avoid those
situations
– Influenced by reticular and limbic structures
• Cognitive- evaluative- – Related to pain input
– Compare to past experiences
• Mediated by neocortex and higher CNS processes• Behavioral responses to pain
− Behaviors to reduce the source of pain as quickly as possible
3

Cognitive Processes
Sensory Awareness Emotional and Motivational Reactions
Experience of “Pain”
Spinal “gate” mechanisms
affect and are affected by all of the components
above
Sensory nerve impulses from receptors (e.g. free nerve endings) 4

Pain/Causal Factors
Biological –
*Stimulation of pain receptors in body
*Release of substance P, endorphins, other neurotransmitters affecting brain regions involved in pain perception
*Opening and closing of spinal “gates”
Cognitive -
*Perceived meaning: of pain stimuli
*Placebo effects
- Attitudes and beliefs
*Use of cognitive – behavioral pain control strategies
*Perceived self-efficacy
Intrapsychic –
*Unresolved conflicts in somatoform pain disorders
*Pain as a means of controlling others
- Secondary gain
*Personality conflicts
*Meaning or significance of pain (Beecher) 5

Pain/Causal Factors
External
Environmental -
*Cultural factors influencing perceived meaning of pain stimuli
*Previous learning
6

7

Three Thresholds in Response to Physical Stimulation
Biological: “I feel something”
Biological: “I feel pain”
Psychosocial: “I can’t tolerate any more, e.g., suffering
ForceHeatCold
8

9

10
ACUTE PAIN
•Normal physiological response to adverse chemical, thermal or mechanical stimulus or injury.
•Short duration (minutes, hours, days)
•Psychological component: Anxiety in proportion to perceived significance of injury.

11
CHRONIC PAIN
•Except for intractable medical conditions, e.g. cancer, source of pain not easily identified
•Long duration (weeks, months, years)
•Psychological comorbidity−Depression −Occasional agitation

12
CLINICAL PAIN
•With or without external provocation, individual reports feeling pain
•Psychological component: − Anxiety or depression

13
IATROGENIC PAIN
•Induced in a patient by a physician's activity, manner, or therapy
•Associated with anticipation of current treatment and its consequences
−Fear of pain
•Psychological component: −Anxiety−Reduced by patient control

14
PATHOGENIC PAIN
•Associated with disease, dysfunction, or a trauma prior to beginning of treatment.
•Psychological component: −Anxiety or depression, Depending upon location or significance of body part.

15
LABORATORY PAIN
•Operationally defined by responses to manipulated noxious stimulus
•Psychological component: −Anxiety−Can distinguish among sensation, pain, and suffering thresholds

16
PSYCHOGENIC PAIN•Regardless of source and objective measures,
−Pain is real to the patient.
•Defined as physical pain that is caused, increased, or prolonged by mental, emotional, or behavioral factors
• There are no discernible pathological conditions consistent with patient’s pain report.
− 50/50 low back pain example
•Difficult to distinguish from hypochondriasis − Defined as undue preoccupation with the body and its processes
•Psychological component: −Anxiety or depression depending on duration

Why is measurement of pain important?Why is measurement of pain important?
• Clinical vs. Laboratory Pain• To determine pain intensity, quality, duration• To aid in diagnosis• To help decide on choice of therapy• To relate to biological, physical and psychosocial
variables• To evaluate relative effectiveness of different therapies• Limitations: pain rarely has one-to-one relationship to
stimulus– Psychological factors and influences by fear, anxiety– Cultural backgrounds, and meaning of situation to person
17

Pain AssessmentPain Assessment
SubjectiveSubjective1. Visual analog scale (VAS)2. Verbal rating scale- mild, moderate, severe3. Numerical rating scales- 1-1004. McGill pain questionnaire (MPQ)5. Descriptor differential scale
• Self-report
ObjectiveObjective• Behavioral approaches
– Clinical (passive)• Reporting
– Experimental (active)• Psychophysiological• Eliciting
• Neurophysiological– fMRI
18

McGill Pain Questionnaire• Most widely tested and used pain instrument• Developed by Melzack and Torgerson in 1971 to
specify qualities of pain• 102 adjectives are classified into three categories:
sensory qualities, affective qualities, evaluative qualities• Five words are used to express pain intensity: 1=mild,
2=discomforting, 3=distressing, 4=horrible, 5=excruciating
• Descriptor-lists read to patient with instructions to choose only those words which describe how they are feeling right now
19

20

21

Orofacial Pain
- Disproportionate- same needle elsewhere evokes less response- identify other sensation as pain- homunculus (see next slide)- significance for survival
- face/milk, needle/rape- emotional support and contact - sucking- teeth as weapon
- teething one of first pain experiences c.f. circumcision- has lasting effect
22

23

24
REFERRED PAIN

Cultural Differences
• Tursky
25

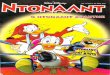
Six-month pain prevalence based on the anatomical site and race. For comparison, results from Six-month pain prevalence based on the anatomical site and race. For comparison, results from Von Korff et al.’s (1988) study of a smaller Caucasian group are also presented.Von Korff et al.’s (1988) study of a smaller Caucasian group are also presented.
26

7 0 7 0 doctor rates paindoctor rates pain 6 06 0 higher than patient higher than patient 5 0000 5 0000 4 00000000 4 00000000 3 000000000000000 3 000000000000000 2 000000000000000000000 2 000000000000000000000 1 00000000000000000000000 1 00000000000000000000000 0 00000000000000000000000 0 00000000000000000000000 same ratingsame rating - 1 0000000000000000000000 - 1 0000000000000000000000 - 2 0000000000 - 2 0000000000 - 3 000000 - 3 000000 - 4 000 - 4 000 - 5 0- 5 0 doctor rates pain doctor rates pain - 6 00 - 6 00 lower than patient lower than patient
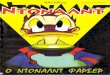
RESULTSRESULTSDoctor’s pain rating minus patient’s pain rating, post-encounterDoctor’s pain rating minus patient’s pain rating, post-encounter
30% of ratings differed by 3+ points. 30% of ratings differed by 3+ points. 27
Doctor vs. Patient Pain Rating

The “pain-prone” personality:
“By virtue of providing for others and not being able to fully depend on their own parents as children they had postponed gratification of such needs until a minor injury provided a rational and socially acceptable means of depending on others for emotional and economic support.”
-- Gentry (1974)
Catastrophizing is associated with negative cognitive and affective and related psychopathological responses to pain which include feelings of helplessness, pessimism, magnification, and rumination (Edwards, Calahan et al. 2011).
28

Other “pain-prone” models:
Alexithymia and somatization-- Stephanos (1979)
Pain-prone characteristics• Somatic complaints• “Solid citizen” presentation• Depression• History of abuse or models of invalidation
- Blurner and Heilbronn (1932)
29

Conscious and unconscious origins:
Disorder Symptom Production Motivation
Malingering con conSomatoform ucs ucsHypochondriacal ucs ucsMὕnchausen’s syndrome con (ucs) con (ucs)Mὕnchausen’s by proxy con (ucs) con (ucs)
- from Eisendrath, S.J. Psychiatric aspects of chronic pain
Neurology 45:26-34, 1995.30

31

32