Embed Size (px)
Citation preview

Strengthening the health system response to NCDs
in Europe Melitta Jakab (WHO-DSP) Jill Farrington (WHO-DNP)
Enrique Loyola (WHO-DNP) Juan Tello (WHO-DSP)
Copenhagen, Denmark
November 5, 2015

Outline
Overview of the work progamme
Regional trends in NCD outcomes and core interventions
Findings in 12 country assessments

OVERVIEW OF THE WORK PROGRAMME


Overview
• Goal is to support MSs to accelerate gains in NCD outcomes
• Country assessments: analytical work as entry point with medium-term policy follow-up
• Systematic approach to identifying health system challenges and opportunities
• Multidisciplinary national & international teams work toward consensus

• Background paper • Assessment guide • 12 country assessments
• ARM, BLR, CRO, EST, HUN, KAZ, KGZ, MDA, MKD, POR, TAJ, TUR • Good practice briefs • Policy dialogues and policy development • Continuous sharing of experiences across the region
Building a region-wide momentum

Sharing good practices

Purpose Why have countries embarked on this journey?
An entry point to evidence-informed policy development and dialogue
Seek to integrate fragmented risk factor and disease specific programs
Create a closer link between health system strengthening and health gain
Build a political momentum to address NCDs

Policy impact
3
4
4
6
6
7
10
0 2 4 6 8 10
Tobacco legislation
Info technology
Major SD reform
Incentives
Guidelines & training
Further analysis
Gvnance and NCD plans
Number of countries reporting follow-up action (out of 10)
Included NCDs into development plan
New tobacco control law in line w/ FCTC
Complete re-orientation of PHC
Strengthening e-health system for NCDs

Policy impact • One component of intensifying pressure to
respond to NCDs more effectively
• Forging in-country partnerships for greater impact (UNDP, World Bank, OECD)

Mutually reinforcing with Health 2020
11

Experience sharing
• Annual Flagship course on health system strengthening
• Since 2011 with a focus on NCDs
• Each country assessment is integrated
• 50+ participants
• Russian/English

Three pillars of the assessments
Health system
strengthening
through addressing
health system
challenges and
responding to
opportunities for
scaling up coverage
of core services
Core
services
Population
interventions
Expected
health gain
Achieve 25%
mortality
reduction for
NCDs by
2025 Individual
services

THE REGIONAL PERSPECTIVE ON NCD OUTCOMES AND CORE INTERVENTIONS & SERVICES

y = -11.401x + 551.99 or 40,4% between 2010 and 2025
y = -6.9757x + 325.42 or 42.2% between 2010 and 2025
y = -11.242x + 604.17 or 35.3% between 2010 and 2025
y = -19.125x + 943.98 or 39.8% between 2010 and 2025
0
100
200
300
400
500
600
700
800
900
1000
2000 2002 2004 2006 2008 2010 2012 2014 2016 2018 2020 2022 2024
SDR
, age
s 3
0-6
9 y
rs, m
ajo
r N
CD
, pe
r 1
00
.00
0
Year
Age-standardized NCD death rates 30-69 and projections to 2025
European Region EU members before May 2004 EU members since May 2004 CIS
Source: WHO. European Health for All database, 2015
Regional trends in premature NCD mortality are promising
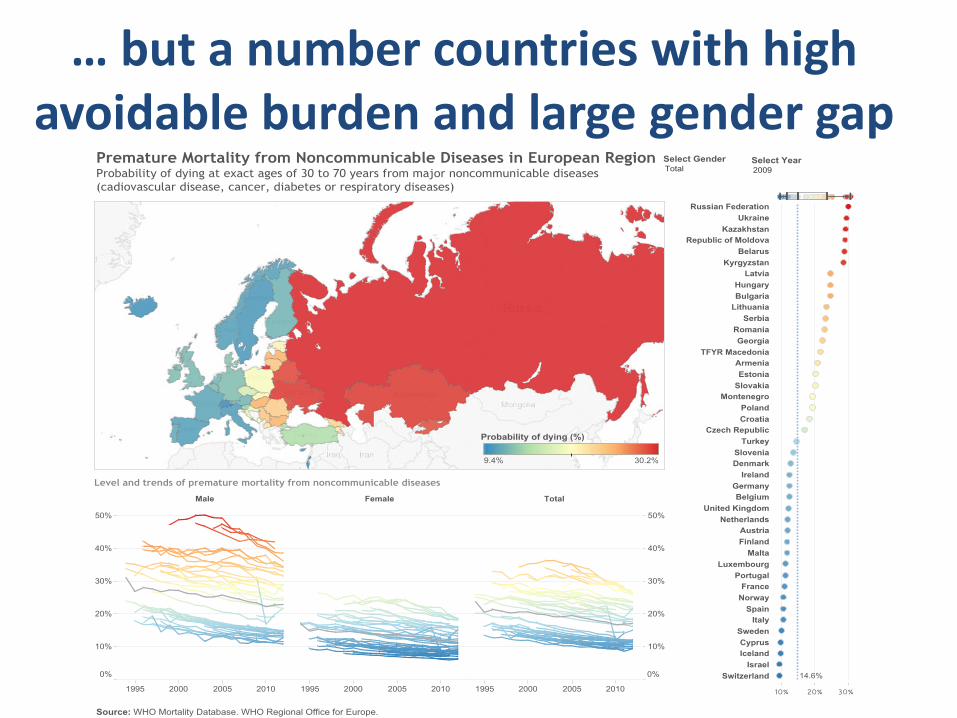
… but a number countries with high avoidable burden and large gender gap

Source: WHO. European mortality database, 2014
Shaped by patterns in premature CVD mortality

Core services Population interventions
Voluntary Global Targets Core interventions
30% reduction in the
prevalence of current tobacco
use
• Wide-range of anti-smoking interventions (FCTC)
– Raising tobacco taxes
– Smoke-free environments
– Warning about the dangers of tobacco and smoke
– Bans on advertising, promotion and sponsorship
20% reduction in the harmful
use of alcohol
• Interventions to prevent harmful alcohol use
– Raising taxes on alcohol
– Restrictions and bans on advertising and promotion
– Restrictions on the availability of retailed alcohol
Halt the rise in diabetes and
obesity
30% reduction in salt intake
10% reduction in inactivity
• Interventions to improve diet and physical activity
– Reducing salt intake and salt content
– Replacing trans-fats with polyunsaturated fat
– Promoting public awareness about diet and activity

Core services Individual health services
Voluntary Global
Targets
Core services
25% reduction in
prevalence of raised
BP
50% of eligible
receive drug therapy
• CVD & Diabetes
– Risk-stratification in primary health care -detection and management of
hypertension, cholesterol, and diabetes through multi-drug therapy
– Prevention in high risk groups and sec. prevention after AMI incl. aspirin
therapy
– Rapid response and secondary care after AMI and stroke
Halt the rise in
diabetes
• Diabetes
– Effective detection and general follow-up
– Patient education and intensive glucose management
– Hypertension management among diabetes patients
– Preventing complications (e.g. eye and foot exam)
• Cancer
– Prevention of liver cancer through hepatitis B immunization
– Screening for cervical cancer and tmt of precancerous lesions
– Early case finding for breast cancer and tmt of all stages

TOBACCO
Implementation status of FCTC in 53 MSs
Source: European Tobacco Control Report 2013: http://www.euro.who.int/__data/assets/pdf_file/0011/235973/European-Tobacco-
Control-Status-Report-2013-Eng.pdf Slide: Kristina Mauer-Stender

NUTRITION & PHYSICAL INACTIVITY Selected global targets in 53 MSs
0 % 20 % 40 % 60 % 80 % 100 %
Breastfeeding
Physical inactivity
Anaemia
Adult obesity
Childhood obesity
Stunting
Wasting
On track off track
Slide: Joao Breda
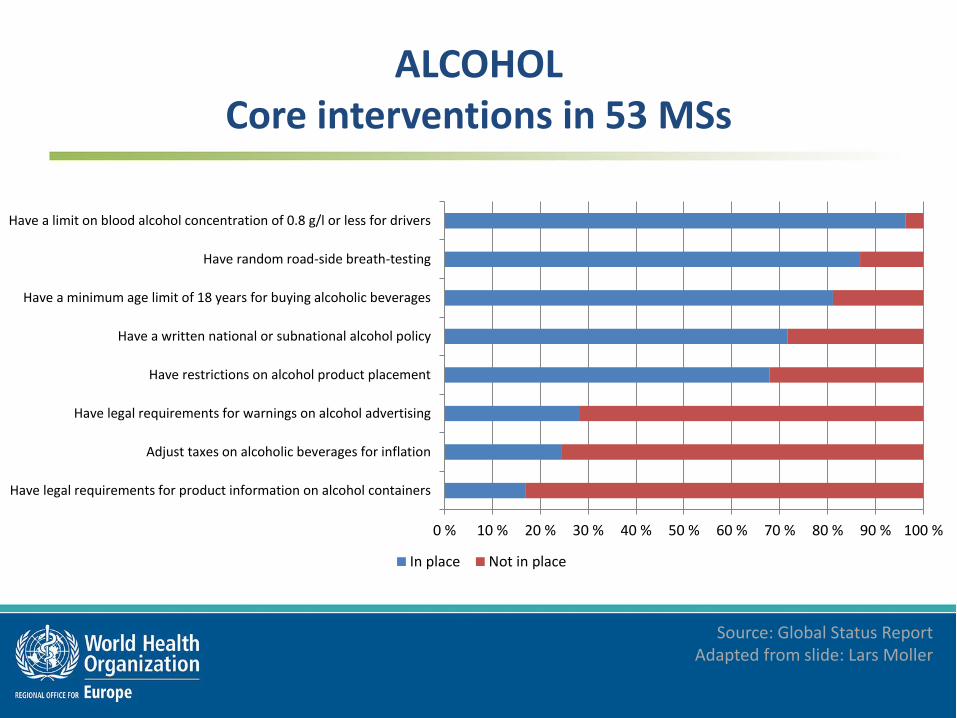
ALCOHOL Core interventions in 53 MSs
0 % 10 % 20 % 30 % 40 % 50 % 60 % 70 % 80 % 90 % 100 %
Have legal requirements for product information on alcohol containers
Adjust taxes on alcoholic beverages for inflation
Have legal requirements for warnings on alcohol advertising
Have restrictions on alcohol product placement
Have a written national or subnational alcohol policy
Have a minimum age limit of 18 years for buying alcoholic beverages
Have random road-side breath-testing
Have a limit on blood alcohol concentration of 0.8 g/l or less for drivers
In place Not in place
Source: Global Status Report Adapted from slide: Lars Moller

Target 9 Evidence from recent STEPS surveys
% adults (40-64 yrs) with a 10 yr CVD risk of 30% or more, or with existing
CVD**
Of these.... % receiving drug therapy and
counselling***
Kyrgyzstan (2013) 17.4% 49.0%
Uzbekistan (2014) 20.2% 58.7%
Turkmenistan (2014) 20.5% N/A
Republic of Moldova (2013)* 23.0% 51.2%
Source: WHO STEPS surveys

Proportion of primary health care facilities which offer a cardiovascular risk stratification for the management of
patients at high risk for heart attack and stroke, 2015
0%
10%
20%
30%
40%
50%
60%
In more than 50%of PHC facilities
In 25% to 50% ofPHC facilities
In less than 25% ofPHC facilities
None
% c
ou
ntr
ies
off
eri
ng
CV
ris
k st
rati
fica
tio
n
WHO European Region EU NIS
Source: NCD Country Capacity Survey 2015

% adults with raised blood pressure* who are NOT currently on medication for it
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Uzbekistan(2014)(18-64 yrs)
Turkmenistan(2014)(18-64 yrs)
Georgia(2010)(18-64 yrs)
Moldova(2013)(18-69 yrs)
Kyrgyzstan(2013)(25-64 yrs)
Female
Male
Both sexes
*Systolic BP >= 140 and/or diastolic BP >=90 mm Hg
Source: WHO STEPS surveys

FINDINGS IN ASSESSMENT COUNTRIES

Assessment countries have enjoyed growth
$0
$5 000
$10 000
$15 000
$20 000
$25 000
$30 000
$35 000
$40 000
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
GD
P p
er
cap
ita,
PP
P (
curr
en
t in
tern
atio
nal
$)
GDP per capita
Armenia Belarus Croatia Estonia Hungary
Kazakhstan Kyrgyzstan Macedonia, FYR Republic of Moldova Portugal
Tajikistan Turkey European Union
Source:

Variation in level of development and priority to health
0%
2%
4%
6%
8%
10%
12%
14%
16%
$-
$5 000
$10 000
$15 000
$20 000
$25 000
$30 000
GD
P p
er c
apit
a (i
nte
rnat
ion
al $
)
GDP per capita & GGHE%GGE (2014)
GDP/capita, PPP ($Int) GGHE (%GGE)
Source:

Premature NCD mortality & development
ARM
CRO
EST
HUN
KAZ
KGZ
MKD
POR
MDA
0
100
200
300
400
500
600
700
800
$- $10 000 $20 000 $30 000 $40 000 $50 000 $60 000
SDR
, maj
or
NC
Ds,
30
-69
ye
ars,
bo
th s
exe
s, p
er
10
0,0
00
(2
01
0)
GDP/capita, PPP ($int) (2010)
Source:

NCD outcomes in assessment countries
• Regional averages masque trouble spots
• Trends are less smooth and more fragile in individual countries (BLR, KGZ, MDA, TAJ)
• Cancer mortality is high and/or stagnating in a number of countries (ARM, HUN, MKD, POR)
• The male – female gap is substantial and not closing in some cases

Score cards Population interventions
Indicator average (1-3)
Raise tobacco taxes 3 2 Not Assessed 2 2 3 1 1 1 1 1.78
Ensure smoke-free environments 3 3 Not Assessed 2 1 1 2 1 1 1 1.67
Issue warnings on the dangers of tobacco and smoking 3 3 Not Assessed 2 2 2 1 1 2 2 2.00
Ban advertising, promotion and sponsorship 3 2 Not Assessed 2 2 2 2 2 1 1 1.89
Provide quit l ines and nicotine replacement therapy 3 1 Not Assessed 1 1 2 1 1 1 1 1.33
Raise taxes on alcohol 1 3 Not Assessed 1 1 1 1 2 1 1 1.33
Restrictions or bans on advertising and promotion 3 2 Not Assessed 2 1 1 3 2 1 1 1.78
Restrictions on retail availability of alcohol 3 3 Not Assessed 3 1 1 1 2 2 1 1.89
Minimum purchase age regulated and enforced 2.5 3 Not Assessed 2 2 2 1 1 1 2 1.83
Allowed blood alcohol content for driving 1.5 2 Not Assessed 2 2 3 3 2 1 2 2.06
Reduce salt intake and salt content on foods 2.5 1 1.5 1 1 1 1 Not Assessed 1 1 1.22
Virtually eliminate trans -fatty acids from the diet 2 1 2 1 1 1 Not AssessedNot Assessed 1 1 1.25
Reduce free sugar intake 1 1 3 1 2 1 1 Not Assessed 1 1 1.33
Increase intake of fruit and vegetables 2 2 2 1 3 1 2 Not Assessed 1 1 1.67
Reduce marketing pressure on children to consume food and non-alcoholic beverages2 1 1.5 1 1 1 1 Not Assessed 2 1 1.28
Promote awareness about diet and activity 2 2 1.5 2 2 1 2 Not AssessedNot Assessed 1 1.69
Overall average (1-3)
2.34 2.00 1.92 1.63 1.56 1.50 1.53 1.50 1.20 1.19 1.63Country average (1-3)
Score by country
Po
pu
lati
on
inte
rven
tio
ns
Anti-
smoking
intervention
s
Intervention
s to prevent
harmful
alcohol use
Intervention
s to improve
diet and
physical
activity

Score cards Individual services
Indicator average (1-3)
Risk stratification in primary health care 3 2 2 Not Assessed 2 2 1 2 Not AssessedNot Assessed 2.00
Effective detection and management of hypertension 1.5 1 2 Not Assessed 1 1 1 1 Not AssessedNot Assessed 1.21
Effective primary prevention in high-risk groups 2 1 2 Not Assessed 2 1 1 1 Not AssessedNot Assessed 1.43
Effective secondary prevention after AMI including acetylsalicylic acid 3 1.5 2 Not Assessed 2 2 3 1 Not AssessedNot Assessed 2.07
Rapid response and secondary care after AMI and stroke 2 2.5 2 Not Assessed 1 1 1 1 Not AssessedNot Assessed 1.50
Effective detection and general follow-up Not Assessed 2 2 1.5 2 1 Not AssessedNot AssessedNot AssessedNot Assessed 1.70
Patient education on nutrition and physical activity and glucose managementNot Assessed 2 1 1.5 1 2 Not AssessedNot AssessedNot AssessedNot Assessed 1.50
Hypertension management among diabetes patients Not AssessedNot Assessed 1 1 1 Not AssessedNot AssessedNot AssessedNot AssessedNot Assessed 1.00
Preventing complications Not AssessedNot Assessed 1 2 1 Not AssessedNot AssessedNot AssessedNot AssessedNot Assessed 1.33
Overall average (1-3)
2.30 1.71 1.67 1.50 1.44 1.43 1.40 1.20 N/A N/A 1.58
Ind
ivid
ual
ser
vice
s CVD and
diabetes
Diabetes
Country average (1-3)
Score by country
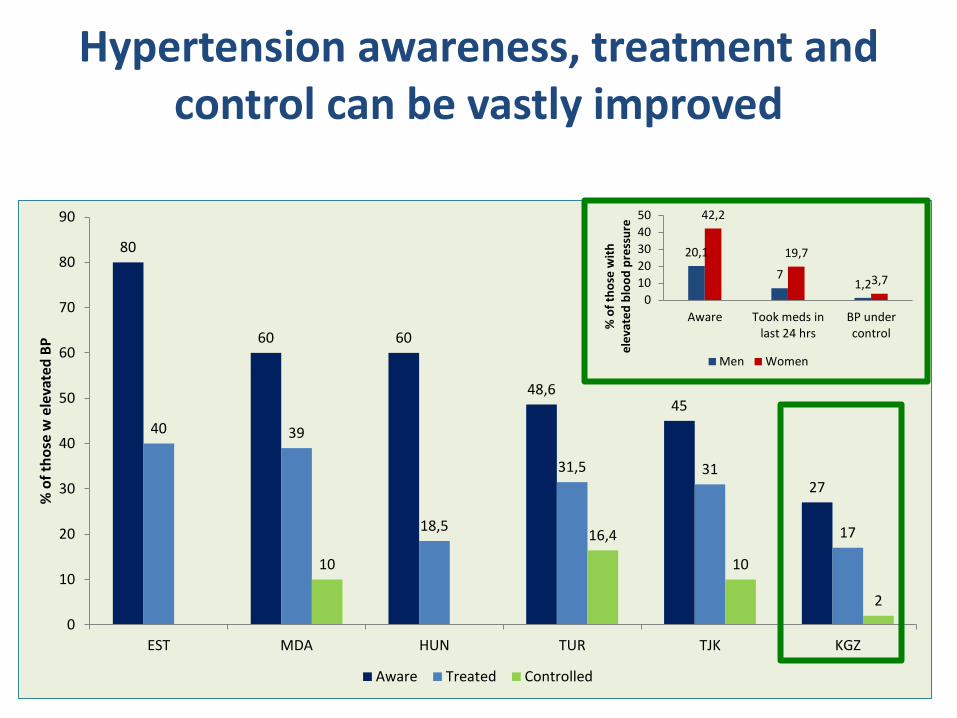
Hypertension awareness, treatment and control can be vastly improved
80
60 60
48,6 45
27
40 39
18,5
31,5 31
17
10
16,4
10
2
0
10
20
30
40
50
60
70
80
90
EST MDA HUN TUR TJK KGZ
% o
f th
ose
w e
leva
ted
BP
Aware Treated Controlled
20,1
7 1,2
42,2
19,7
3,7
0
10
20
30
40
50
Aware Took meds inlast 24 hrs
BP undercontrol
% o
f th
ose
wit
h
ele
vate
d b
loo
d p
ress
ure
Men Women

Political commitment to
NCDs
Explicit priority setting
approaches
Inter-agency action
Empowerment and people
centredness
Effective model of service delivery
Coordination across providers
Regionalization Incentive systems
Integration of evidence into
practice
Distribution and mix of human
resources
Access to quality medicines for
chronic diseases
Effective management
Adequate information solutions
Managing change
Ensuring access and financial
protection
Fifteen health system challenges and opportunities to respond to NCDs

Many countries face health system barriers to scale up NCDs
• Population interventions – Lack of explicit priority setting processes
– Making inter-sectoral action work effectively
• Individual services – Model of care fragmented
– Incentives are insufficient and not aligned
– Pharmaceutical policies need to be more comprehensive
– Information solutions are under-utilized
• Cross-cutting – Empowerment and people-centredness need
greater emphasis
The magic word
A L I G N M E N T

Good practice Estonia scales up CVD prevention and disease
management in PHC
Model of care Integration of evidence
into practice
Incentives Adequate information
solutions

Good practice Turkey scales up cancer screening
16
6
12
63
6
31
76
9
34
83
22
0
10
20
30
40
50
60
70
80
90
Breast Cervical Colorectal
% o
f ta
rge
t p
op
ula
tio
n
Cancer screening coverage rates
2007 2012 2013 2014
Empowerment and people-centredness
Coordination across providers
Adequate information solutions

Political commitment to
NCDs
Explicit priority setting
approaches
Inter-agency action
Empowerment and people
centredness
Effective model of service delivery
Coordination across providers
Regionalization Incentive systems
Integration of evidence into
practice
Distribution and mix of human
resources
Access to quality medicines for
chronic diseases
Effective management
Adequate information solutions
Managing change
Ensuring access and financial
protection
Focus of expert consultation


EXTRA SLIDES JUST IN CASE

The way forward
2012 2013 2014 2015 2016 2017 2018 2019
HUN MDA KGZ TUR TJK
BLR EST CRO
… …
ARM KAZ MKD POR
Guide piloted
and published
Good practice
briefs launched
Synthesis report and launch event
Exploring key policy issues
Enabling cross-country learning
Perfecting the country work
Policy follow-up
… …

Process for country assessments
• Agreement on objectives and scope
• International and local multi-disciplinary teams set up
• Online preparatory meetings to discuss methodology, allocate tasks, and organize
• 5-10 day multi-disciplinary expert mission with feedback loop
• Draft report prepared and circulated for comments in host country and in WHO
• Policy dialogue
• Follow-up steps agreed and work plan
• Report completed and published
Ap
pro
ximate
ly 12
m
on
ths
PR
EPA
RA
TOR
Y
PH
ASE
M
ISSI
ON
P
HA
SE
REP
OR
T W
RIT
ING
&
FO
LLO
W-U
P

Cancer plan Existence of operational
policy/ strategy/ action plan for
cancer
Breast cancer screening General availability of
breast cancer screening (by palpation or
mammogram) at the primary health care
level
Bowel cancer screening
General availability of bowel cancer
screening (by digital exam or
colonoscopy) at the primary health care
level
Cervical cancer screening
General availability of cervical cytology
at the primary health care level
Radiotherapy public system
General availability of radiotherapy in the public system
(number)
Armenia √ √ x √ 2
Azerbaijan x x x x 2
Belarus √ x x x 13
Georgia x √ √ √ 1
Kazakhstan √ √ √ √ 18
Kyrgyzstan √ √ √ √ 1
Republic of Moldova √ √ x √ 1
Russian Federation √ Not recorded x √ 126
Tajikistan √ √ x √ 1
Turkmenistan Not recorded √ x √ 5
Ukraine √ √ x √ 47
Uzbekistan √ √ x √ 16

Country
Programme covering cancer early diagnosis,
treatment & care
Cancer registry Oral morphine
available in public health sector
Availability of community/ home care
for people with advanced/ end stages of
disease
Armenia √ √ × ×
Azerbaijan √ √ × ×
Belarus Not recorded √ √ √
Georgia Not recorded √ × ×
Kazakhstan Not recorded √ × √
Kyrgyzstan √ × √ √
Republic of Moldova √ √ √ √
Russian Federation √ √ √ √
Tajikistan √ √ × ×
Turkmenistan √ √ √ Don’t know
Ukraine √ √ × Don’t know
Uzbekistan √ √ × ×
Source: WHO NCD Country Capacity Survey 2015

ALCOHOL Core interventions in 53 MSs
Source: Global Status Report Adapted from slide: Lars Moller
9 Have legal requirements for product information on alcohol containers
13 Adjust taxes on alcoholic beverages for inflation
15 Have legal requirements for warnings on alcohol advertising
36 Have restrictions on alcohol product placement
38 Have a written national or subnational alcohol policy
43 Have a minimum age limit of 18 years for buying alcoholic beverages
46 Have random road-side breath-testing
51 Have a limit on blood alcohol concentration of 0.8 g/l or less for drivers
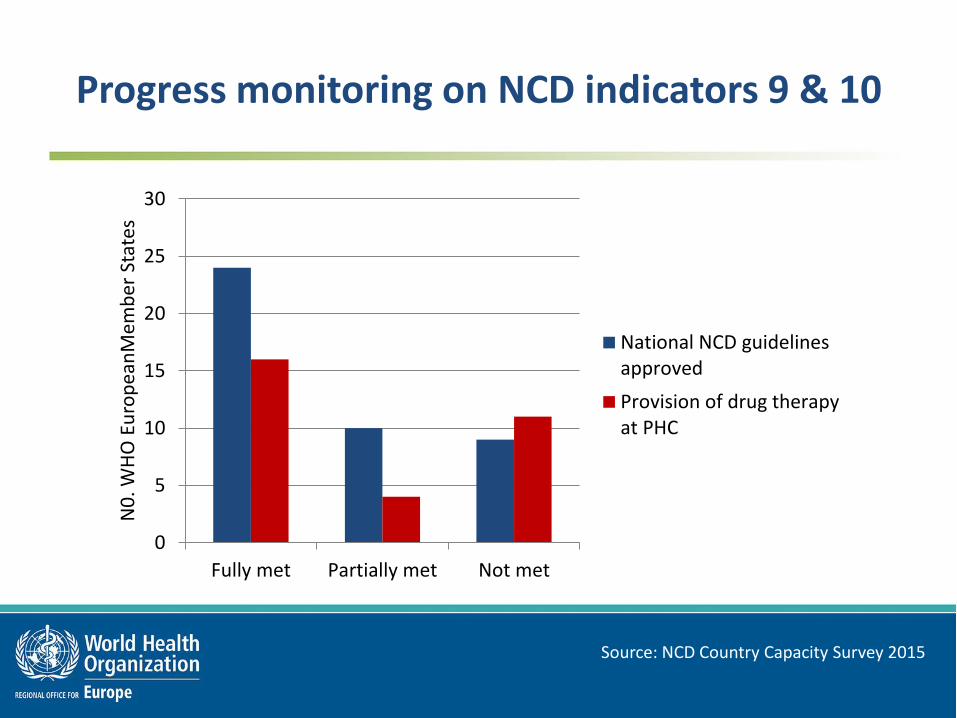
0
5
10
15
20
25
30
Fully met Partially met Not met
N0
. WH
O E
uro
pea
nM
emb
er S
tate
s
National NCD guidelinesapproved
Provision of drug therapyat PHC
Progress monitoring on NCD indicators 9 & 10
Source: NCD Country Capacity Survey 2015





























