Embed Size (px)
DESCRIPTION
Strategy Against Pulmonary Tuberculosis Problems
Citation preview

Strategy Against Pulmonary Tuberculosis
Problems
IKA TRISNAWATI
Pulmonology Department/Internal MedicineDr. Sardjito Hospital Yogyakarta

300+300+2007 110 per 100.000
DIY & Bali: 68 per 100.000

TB in The World
Estimated Cases/yr
Estimated Deaths/yr
TB, all forms 8.8 million 1.6 million
Multidrug-resistant (MDR) TB
424,000 (5%) 116,000 (7%)
Extensively drug-resistant (XDR) TB
27,000 (6%) 16,000 (14%)
Zignol 2006


M. tuberculosis
• Bakteri tahan asam• Ukuran: 0.2~0.3 x 2~5 μm• Tumbuh lambat• Perkembangbiakan intraseluler• Lesi granuloma

Organisme yang disebarkan
• Bicara 0 –200• Batuk 0 –3.500• Bersin 4.500-1.000,000
• Partikel respiratorik diameter besar akan menetap sekitar 1 meter dari sumber
• Partikel kecil mengering dalam inti droplet dan terbawa hembusan angin

Potensi penularan pasien TB atau suspek TB
Faktor yang berisiko menular
TB paru atau larinkTerdapat cavitas di paruBatuk atau diinduksi batukPasien tidak menutup mulut ketika batukSputum: BTA positif Tidak mengikuti program pengobatan
Faktor yang tidak beisiko menular
TB ekstra paru Tidak terdapat cavitas di paru Tidak batuk atau tidak diinduksi batukPasien menutup mulut ketika batukSputum :BTA negatifTelah mendapat pengobatan TB secara adekwatselama setidaknya 2‐3 minggu

Transmision and Progression of Tuberculosis

Evaluation for TB


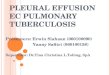
AFB (shown in red) are tubercle bacilli
AFB smear

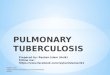
Chest Radiograph
Abnormalities often seen in apical or posterior segments of upper lobe or superior segments of lower lobe
May have unusual appearance in HIV-positive persons
Cannot confirm diagnosis of TB

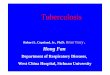
Cultures
•Use to confirm diagnosis of TB
•Culture all specimens, even if smear negative
•Results in 4 to 14 days when liquid medium
systems used
Colonies of M. tuberculosis growing on media

Tuberculin Skin Test
•Inject intradermally 0.1 ml of 5
TU PPD tuberculin
•Produce wheal 6 mm to 10 mm
in diameter•Read reaction 48-72 hours after injection•Measure only induration
•Record reaction in millimeters


Tipe Pasien
Kasus baru• Belum pernah diobati dengan OAT • Atau sudah pernah menelan OAT kurang dari satu bulan (4
minggu).
Kasus kambuh (Relaps)Pasien tuberkulosis yang sebelumnya pernah mendapat
pengobatan tuberkulosis dan telah dinyatakan sembuh atau pengobatan lengkap, didiagnosis kembali dengan BTA positif (apusan atau kultur).

Tipe Pasien
Kasus setelah putus berobat (Default )Pasien yang telah berobat dan putus berobat 2 bulan atau
lebih dengan BTA Positif.
Kasus setelah gagal (failure)Pasien yang hasil pemeriksaan dahaknya tetap positif atau
kembali menjadi positif pada bulan kelima atau lebih selama pengobatan.

Tipe Pasien
Kasus lain :Adalah semua kasus yang tidak memenuhi ketentuan diatas.
Dalam kelompok ini termasuk Kasus Kronik, yaitu pasien dengan hasil pemeriksaan masih BTA positif setelah selesai pengobatan ulangan.
TB paru BTA negatif dan TB ekstra paru, dapat juga mengalami kambuh, gagal, default maupun menjadi kasus kronik. Meskipun sangat jarang, harus dibuktikan secara patologik, bakteriologik (biakan), radiologik, dan pertimbangan medis spesialistik,..

DOTS: Strategi global pengendalian TB
1. Political commitment 2. Smear microscopy 3. Adequate drug supply 4. Treatment observer 5. Recording and reporting

TB Sensitif ObatTB Sensitif Obat

Essential Anti-TB Drug (abbreviation)
Recommended dose (mg/kg)
Daily Intermittent
3 times/week 2 times/week
Isoniazid (H)Rifampicin ®Pyrazinamide (Z)Streptomycin (S)Ethambutol (E)Thioacetazone (T)
5 (4-6010 (8-12)
25 (20-30)15 (12-18)15 (15-20)
2.5
10 (8-12)10 (8-12)
35 (30-40)15 (12-18)30 (25-35)
15 (13-17)10 (8-12)
50 (40-60)15 (12-18)45 (40-50)
Not applicable
Standardised Treatment Regimens by WHO (The essential anti-TB drugs)

Essential Anti-TB Drug (abbreviation)
Mg/day
Adult 70 kg bodyweight
Child 25 kg bodyweight
Isoniazid (H)Rifampicin ®Pyrazinamide (Z)Streptomycin (S)Ethambutol (E)Thioacetazone (T)
350700
1750-
1050-
125250625
-375
-
Daily Dosade

TB Treatment Category
TB patients
Alternative TB Treatment Regimens
Initial phase (daily or 3 times/week)
Continuation phase
I
New smear-positive PTB;New smear-negative PTB with extensive parenchymal involvement;New cases of severe forms of extra-pulmonary TB
2 EHRZ (SHRZ)2 (EHRZ (SHRZ)
2 EHRZ (SHRZ)
6 HE4 HR
4 H3R3
II
Sputum smear-positive;Relaps;Treatment failure;Treatment after interruption.
2 SHRZE / 1 HRZE2 SHRZE / 1 HRZE
5 H3R3E3
5 HRE
III
New smear-negative PTB (other than in category I) new less severe forms of extrapulmonary TB
2 HRZ2 HRZ2 HRZ
6 HE4 HR
4 H3R3
IV
Chronic case (still sputum-positive after supervised retreatment)
Not application(Refer to WHO guidelines for use of second-line drugs
in specialized centres)
Possible Alternative Treatment Regimens for EachTreatment Category (WHO Guidelines)

Latent TB Infection (LTBI)
•Occurs when person breathes in bacteria and it reaches the air sacs (alveoli) of lung • Immune system keeps bacilli contained and under control
• Person is not infectious and has no symptoms

25
LTBI TB DiseaseTubercle bacilli in the body
Tuberculin skin test reaction usually positive
Chest x-ray usually normal Chest x-ray usually abnormal
Sputum smears and cultures negative
Symptoms smears and cultures positive
No symptoms Symptoms such as cough, fever, weight, loss
Not infectious Often infectious before treatment
Not a case of TB A case of TB
LTBI vs TB Disease

Treatment of Latent TB Infection
•Daily INH therapy for 9 months
•Monitor patients for signs and symptoms of hepatitis and peripheral neuropathy
•Alternate regimen – Rifampin for 4 months

Immune Reconstitution Reaction
Paradoxical reaction (immune reconstitution syndrome, IRS): temporary exacerbation of symptoms, signs, or radiographic manifestations of TB after beginning TB treatment, may include:
1. High fever2. Increase in size of lymph nodes3. New lymphadenopathy4. Worsened CNS lesions5. Worsened pulmonary infiltrates6. Increasing pleural effusions
Occurs in HIV-uninfected patients, but more common in HIV-infected patients, especially those on ART

Immune Reconstitution Reaction
Mild-moderate reactions: Symptomatic treatment, NSAIDsContinue TB therapy and ART
Severe reactions (eg, high fever, airway compromise from enlarging lymph nodes, enlarging serosal fluid collections, sepsis syndrome):
Not studied; consider prednisone or methylprednisolone(1 mg/kg daily, with taper after 1-2 weeks)Continue TB therapyContinue ART if possible (unless IRS is life threatening)

Thank You