Embed Size (px)
Citation preview
SCN Epilepsy Pathway Development Paper: Draft V2 10.7.14 Page 1 of 34
Strategic Clinical Networks
Epilepsy Pathway Development
Paper prepared by
Julie Rigby Greater Manchester , Lancashire & South Cumbria SCN [email protected]
Purpose This paper provides an outline of national and local guidelines and activity to facilitate an understanding of the current issues in providing appropriate services for people with epilepsy
Version V2
Status Draft
Date 10th July 2014 Revision History
Version Revision date Summary of changes
V1 N/A
V2 10th July 2014 Changes following discussion with Dr Mark Kellett, Dr Hedley Emsley and Gareth Lord
SCN Epilepsy Pathway Development Paper: Draft V2 10.7.14 Page 2 of 34
Contents 1. Introduction 3
2. Rationale for this work 3
3. Background 4
4. Local activity 5
5. Priority areas for change 7
6. Supporting rapid access to accurate diagnosis 7
7. Decreasing avoidable admissions 9
8. Providing on-going support 11
9. Improving access to ESNs 12
10. Improving transition 13
Appendices
Appendix 1 Epilepsy Overview NICE CG137 15
Appendix 2 Greater Manchester: Overall management of seizure disorders 16
Appendix 3 Greater Manchester: Long term Management of seizures 17
Appendix 4 Epilepsy Journey: Neurological Commissioning Support 18
Appendix 5 Do Once and Share pathway 19
Appendix 6 Pathway for Transient Loss of Consciousness 21
Appendix 7 Guidelines for the Management of First Seizure in the ED 22
Appendix 8 Summary of NASH Audit Report 23
Appendix 9 Cheshire & Merseyside A&E Pathway 27
Appendix 10 Cheshire & Merseyside SCN Education Programme 30
Appendix 11 Protocols for treating convulsive status epilepticus in adults 31
Appendix 12 Protocols for treating convulsive status epilepticus in children 33

SCN Epilepsy Pathway Development Paper: Draft V2 10.7.14 Page 3 of 34
1. Introduction From the 1st April 2013, twelve Strategic Clinical Networks (SCNs) were introduced to the new NHS structures for England in April 2013. Each of the twelve has been tasked to improve services for people with neurological conditions. During the first year of operation each of these SCNs has invested time in reviewing evidence and speaking to stakeholders about areas of health and social care which warrant large scale change. Improving services for people with epilepsy has been identified as a priority by all of the SCNs and is supported by the decision of the RCGP to highlight epilepsy as one of its clinical priorities for 2013 – 16. In April 2013, the RCGP appointed an epilepsy-specific clinical champion, Dr Greg Rogers, a GP with special interest in epilepsy based in Kent. Dr Rogers was a clinical advisor for the report “A Critical Time for Epilepsy in England” (1) which identified that CCGs were not routinely commissioning services for people with epilepsy and highlighted shortfalls in service provision by acute trusts. An earlier driver for improving services for people with epilepsy was the All Party Parliamentary Group on Epilepsy, “Wasted money wasted lives” (2). This report highlighted serious shortfalls in the care of patients with epilepsy and made recommendations for improving service provision in line with NICE guidance. The report stated:
“During the course of our enquiry it has become clear that the case for improving epilepsy services is overwhelming. A vicious circle of social stigma, secrecy and widespread medical ignorance has led to a poor service, from which patients cannot confidently expect good treatment at a primary or secondary level. The waste of money in delivering this inadequate service is almost as appalling as the unnecessary deaths and damage to quality of life experienced by people with epilepsy.”
2. Rationale for this work This paper provides an outline of national policies and guidelines and local initiatives collected from SCNs across the country regarding epilepsy. The decision to review epilepsy care across all SCNs was based on recognition that service provision is variable. This is noted in the Atlas of Variation (3) for three key areas: • The ratio of reported to expected prevalence of epilepsy • The directly standardised rate of elective admissions in persons with epilepsy per
100,000 population • The directly standardised rate of emergency admissions in persons with epilepsy per
100,000 population. It was also recognised that management of the condition is often sub-optimal and frequently associated with emergency admissions to hospital. In the worst cases death may occur as a result of sudden unexpected death in epilepsy (SUDEP) or from status epilepticus. A number of SCNs have already commissioned reports from Neurological Commissioning Support which have highlighted epilepsy as a specific issue in relation to high admission rates, high cost and potentially avoidable co-morbidities. The paper aims to: • Improve understanding of current guidelines and issues in service provision for people
with epilepsy • Increase awareness of local projects / best practice across the country • Identify deliverables for the SCNs e.g. pathways, guidelines, protocols.

SCN Epilepsy Pathway Development Paper: Draft V2 10.7.14 Page 4 of 34
Based on identified deliverables, SCNs aim to support achievement of the following outcomes: • Rapid, accurate diagnosis • Reduction in misdiagnosis • Reduction in variation of care • Reduction in mortality – due to SUDEP and status epilepticus • Reduction in emergency admissions • Reduced length of stay when admissions occur • Improved patient and carer experience • Decreased costs within the system. 3. Background Epilepsy is a common and chronic neurological condition defined as a tendency to have recurrent unprovoked seizures. A seizure is caused by a sudden burst of excess electrical activity in the brain, which temporarily disrupts the normal passage of messages between brain cells (4). Epilepsy leads to significant medical challenges but also has a marked impact on patients’ quality of life (5). Epilepsy is not a single condition: there are over 30 different epileptic syndromes and 38 different types of seizure with some people having multiple problems. Epilepsy affects over 496,000 people in England i.e. 1 in every 105 people (6). It is believed that there are currently 69,000 people with epilepsy who experience recurrent seizures due to sub-optimal management and treatment of their condition (4). Furthermore, the trend of epilepsy mortality appears to be increasing, contrary to the decreasing trend of mortality from all causes amongst the general population. An estimated 40% of adult deaths for people with epilepsy in the UK could be avoided with improved care. Between 1993 and 2005, mortality in which epilepsy was recorded as an underlying cause of death increased by 31% in males and 39% in females (7). It is estimated that around 10,000 to 15,000 people in the UK experience Non-epileptic Attack Disorders (NEAD) which are not caused by disrupted electrical activity in the brain. Non-epileptic seizures can be divided into two types. Organic non-epileptic seizures have a physical cause and include fainting (syncope) and seizures with metabolic causes such as diabetes. Psychogenic non-epileptic seizures have a psychological cause which can be categorised further as: • Dissociative seizures • Panic attacks • Factitious seizures (http://www.nonepilepticattacks.info/1_numbers.html)
Data suggests that better management of NEAD could be beneficial for patients and reduce service costs Around 3 in 4 people with NEAD have previously been diagnosed with epilepsy and taken anti-epileptic drugs: • 1 in 5 people with NEAD have been taken to intensive care units with prolonged
seizures erroneously considered as "status epilepticus" • Nearly 1 in 6 people stop having non-epileptic seizures after the diagnosis has been
explained • 1 in 2 people with NEAD become free of seizures with the right treatment
(http://www.nonepilepticattacks.info/1_numbers.html).
The misdiagnosis rates for epilepsy in the United Kingdom are thought to vary between 20-31% (4). Misdiagnosis can lead to serious consequences for patients in terms of lifestyle with restrictions in driving and employment and stigma often associated with the condition (8). Misdiagnosis most often occurs where patients are initially seen by non-specialist clinicians.

SCN Epilepsy Pathway Development Paper: Draft V2 10.7.14 Page 5 of 34
The average medical cost per patient per year of misdiagnosis is £316.00. This cost is due to: • Inpatient admissions - 45% • Inappropriate prescribing of anti-epileptic drugs (AEDs) - 26% • Outpatient attendances - 16%, and • Primary care - 8% (9). Furthermore, it is estimated that up to 70% of people with epilepsy could achieve seizure control with optimal AED treatment (4), however only 52% of people with epilepsy are seizure-free (10). The benefits of having effective services to support the management of epilepsy include: • Reducing the risk of premature death from SUDEP • Reducing emergency admissions to secondary care by preventing seizures and seizure-
related injuries • Reducing social and financial deprivation of individuals incorrectly diagnosed with
epilepsy and treated with AEDs, and those individuals with epilepsy who are misdiagnosed with a non-epileptic condition
• Reducing the risk of teratogenicity, i.e. foetal malformation and/or developmental disorders in the child, from the inappropriate prescribing of AEDs for patients with epilepsy as well as individuals wrongly diagnosed with epilepsy
• Promoting independent living and employability • Enhancing patient choice, empowerment and self management • Better use of financial and other resources (4). There are certain groups of patients who find it more difficult to access appropriate services and improving the care provided for these patients is crucial to improving services overall. NICE CG137 identifies a number of people with specific needs: • People with learning disabilities • Older people i.e. over 65 years of age • Adolescents transferring from children’s to adult services • Women of child-bearing age (11). 4. Local activity Much of the information is this section is taken from a strategy to improve care for people with epilepsy developed via the Greater Manchester Neurosciences Network. The data collected was based on the following ICD-10 codes: • G40 - epilepsy; • G41 - status epilepticus; • R568 - other and unspecified convulsions. Data for elective admissions for ten PCTs (excluding activity for G41) showed around 270 elective spells at a cost of around £560,000.
Elective admissions – GM PCT Total 2010/11 2011/12 Spells 273 269 Cost £588,326 £542,858
Elective admissions may be required to carry out relevant investigations, or deliver medical or surgical interventions. Low rates of admission are not necessarily an indication of good practice although high rates may indicate inappropriate admissions. High levels of activity are also associated with close locality to a neurosciences centre (3).

SCN Epilepsy Pathway Development Paper: Draft V2 10.7.14 Page 6 of 34
Data collected for the same period for GM PCTs also demonstrated that spells associated with emergency admissions (including admissions against G41) were greater than for elective spells. It was assumed that early, accurate diagnosis and better long-term management for patients could reduce emergency spells in hospital, providing an opportunity to review allocation of resources.
Emergency admissions – GM PCT Total 2010/11 2011/12 Spells 3509 £3,852,324 Cost 4555 £5,353,831
It was also assumed that the data was unlikely to provide the full picture of emergency / non-elective admissions occurring as a result of epilepsy as the information was based on admissions against primary diagnosis. Further analysis of 2010/11 emergency admission data indicated that people with epilepsy were the highest users of emergency care compared with people living with other long-term conditions (Figure 1).
34 33
19
6 4 4
Epilepsy CHD CKD COPD Asthma Diabetes
Emergency admission rates per 1000 weighted population - 2010/11
Figure 1: Emergency admission rates for common long-term conditions
This data indicates that patients with epilepsy account for high numbers of emergency admissions. In addition, epilepsy had the highest ratio of total emergency admissions by total population indicating that individuals with epilepsy are admitted to hospital more often than individuals with other more common long-term conditions. The number of people admitted was estimated by profiling the number of emergency admissions by individuals. In 2011/12, 2281 individuals were admitted across GM and 1828 individuals experienced a single admission to hospital in GM. The majority of people (75%) admitted to hospital experienced a length of stay of 0-2 days.

SCN Epilepsy Pathway Development Paper: Draft V2 10.7.14 Page 7 of 34
5. Priority areas for change The following have been identified, across the SCNs, as priority areas for change to improve the quality and safety of services for people with epilepsy: • Developing integrated care pathways and models of care • Improving diagnosis and reducing misdiagnosis • Improving on-going care for those with a diagnosis of epilepsy to prevent presentation to
Emergency Departments (EDs) • Improving care in EDs • Improving services for children and young people • Improving access to Epilepsy Specialist Nurses (ESNs) • Improving self-care / self-management • Supporting people with specific needs:
People with learning disabilities Older people Adolescents transferring from children’s to adult services Women of child bearing age
• Reviewing the use of new anti-epileptic drugs (AEDs) • Standardising investigations etc. to support the decision for epilepsy surgery • Improving access to research trials. As a starting point the SCNs need to work on issues where the greatest impact can be made for the largest number of patients: • Supporting rapid access to accurate diagnosis • Decreasing avoidable admissions for people with established epilepsy • Providing on-going support via annual reviews and information provision for people with
a diagnosis of epilepsy • Improving access to ESNs • Improving transition for young people moving into adult services. 6. Supporting rapid access to accurate diagnosis The pathway of care for the diagnosis, treatment and on-going management of epilepsy should be supported by evidence based principles of care. Whilst the principles should be adhered to, the model of service delivery may need to be adapted to address local variation in geography, demographics and service availability. A pathway of care is described within the NICE Guideline for epilepsy (CG137) (Appendix1). A number of pathways have also been developed across the SCNs: • Greater Manchester: Overall Management of Seizure Disorders (Appendix 2) • Greater Manchester: Long Term Management of Seizures (Appendix 3) • Epilepsy Journey, Vale of York CCG - Neurological Commissioning Support (Appendix
4). • Do Once and Share Programme: Connecting for Health, 2005 (Appendix 5).
The Greater Manchester work was completed in collaboration with clinicians, commissioners and voluntary sector organisations but the success of the pathway was recognised as being dependent on the development of pathways for transient loss of consciousness e.g. the Central Manchester NHS FT pathway (Appendix 6).

SCN Epilepsy Pathway Development Paper: Draft V2 10.7.14 Page 8 of 34
In order to support effective care, pathways should span primary, secondary and tertiary care and include: • Pathways for first seizure • Pathways for seizures in people with a confirmed diagnosis of epilepsy • Links to pathways for people with functional disorders including non-epileptic attack
disorder (NEAD) • Links to pathways for people experiencing transient loss of consciousness • Support for the psychological well-being of people diagnosed with epilepsy. Epilepsy should be diagnosed safely and accurately through access to epilepsy specialists and specialist investigations, including telemetry monitoring services (video telemetry) as required (4). The key clinical issues in supporting accurate diagnosis: • Ensuring that all individuals with a recent onset suspected seizure are seen by a
specialist i.e. a medical practitioner with training and expertise in epilepsy, within 2 weeks.
• Reducing misdiagnosis by providing rapid access to specialist first seizure clinics to patients with suspected new onset epilepsy
• Ensuring that access to appropriate investigations e.g. electroencephalogram (EEG), magnetic resonance imaging (MRI) and to accurate history from previous notes is available within 4 weeks of it being requested to support diagnosis
• Aiming for a confirmed and precise diagnosis of epilepsy, and accurate classification of seizure type and epilepsy syndrome (4 & 11).
GPs may need specialist support through advice and guidance services to enable them to make appropriate referrals to secondary care neurology services. North of England SCN is supporting an evaluation of an advice and guidance pilot in Newcastle. There is also a proposal to identify a named neurologist to support GPs in each locality to improve communication with a view to developing relationships and ultimately improving the timeliness of referrals. The East of England SCN is supporting an education programme to provide referral guidance to GPs for epilepsy and other neurological conditions. The benefits of accurate diagnosis are: • Improving health outcomes and quality of life as a result of prompt access to specialist
expertise in order to obtain a diagnosis and begin treatment • Avoiding delayed or incorrect diagnoses and subsequent risks and costs • Reduction in emergency admissions • Reducing the costs to the NHS of misdiagnosis, including the cost of inappropriate
prescribing of AEDs and medico legal costs arising from complaints and claims. Actions for SCNs: • Collate all the epilepsy pathways with links to others for transient loss of
consciousness and functional disorders including NEAD to produce one overall pathway of care
• Define / agree standards of care to support key elements of the pathway e.g. around diagnosis, treatment etc.
• Clarify the two-week wait guideline – should this apply to all people presenting with epilepsy?

SCN Epilepsy Pathway Development Paper: Draft V2 10.7.14 Page 9 of 34
7. Decreasing avoidable admissions The Guidelines for the Management of First Seizure in the Emergency Department (ED) (12) highlight that seizures account for 1.2% attendances at EDs with a quarter of these due to first seizure. Eyewitness accounts are often the most useful data to inform diagnosis (13). ED guidelines (12) (Appendix 7) identify evidence based practice around: • Laboratory investigations and bedside tests • Neuroimaging • EEG • Admission • Treatment • Advice • Follow-up The Association of British Neurologists has developed draft standards for unscheduled care which identify that: • Adults referred to hospital with a neurological emergency should have access to care in
an appropriate setting • Adults admitted with a neurological emergency should be able to receive advice for a
neurology specialist at all times • Adults admitted with a neurological emergency should see a neurology specialist within
24 hours of admission to hospital. The National Audit of Seizure Management in Hospitals (NASH) was initiated by Professor Tony Marson and Professor Mike Pearson from the University of Liverpool. With funding provided by pharmaceutical companies, and with a Steering Board comprising representatives from a number of professional medical organisations, patient charities and each of the home nations, it is the first comprehensive audit of epilepsy and seizures in the UK. Two iterations of NASH have taken place (in 2011 and 2013), which between them have collected data on over 8,300 Emergency Department (ED) attendances by adults who have suffered a seizure. In addition, there has been a pilot paediatric audit run across NW England and north Wales alongside NASH2. Whilst NASH uses attendance at ED as a means of identifying patients to be included in the audit, the questions cover the care given prior to attendance, during their episode and their onward care. If epilepsy care is to change then action is needed to address issues across primary, secondary and tertiary care, i.e. the whole patient pathway. Three key findings have emerged from NASH: • Whilst the second audit showed small but significant improvements from NASH1 for
many variables, it is unlikely that these changes would be perceptible to patients • High performing sites tend to perform well across most variables and vice versa; and • The variation between the best performing and least well performing sites is extremely
wide. NB: NASH audit reports have been requester for each SCN area and can be collated by CCG At the moment it is unclear if a further iteration of NASH will take place. However any further audit is unlikely to take place before mid-2015. For further details see appendix 8. Cheshire and Merseyside SCN is supporting a work programme to improve the care delivered in the ED. A multi-professional group has been convened to develop an agreed pathway (Appendix 9). There is also a work-stream to support education of staff working in
SCN Epilepsy Pathway Development Paper: Draft V2 10.7.14 Page 10 of 34
EDs and strengthening links between visiting neurologists and local trusts. The work supporting the development of the education programme to assist junior doctors in ED / MAU is noted in Appendix 10. Cheshire and Merseyside SCN is also working with the North West Ambulance Service to: • Develop a pathway to assist paramedics dealing with patients having a first seizure to
enable a flag to be sent to ensure follow ups are successful and to ensure patients are known to the relevant services, NB People with first seizure will generally be taken to ED
• Develop a pathway for people with established epilepsy who have recovered from their seizure and are uninjured so that they are not taken to the ED. Further clarification is required on the number of patients that this may affect. The pathway will include a mechanism to highlight these patients to a named contact so that the seizure pattern can be reviewed.
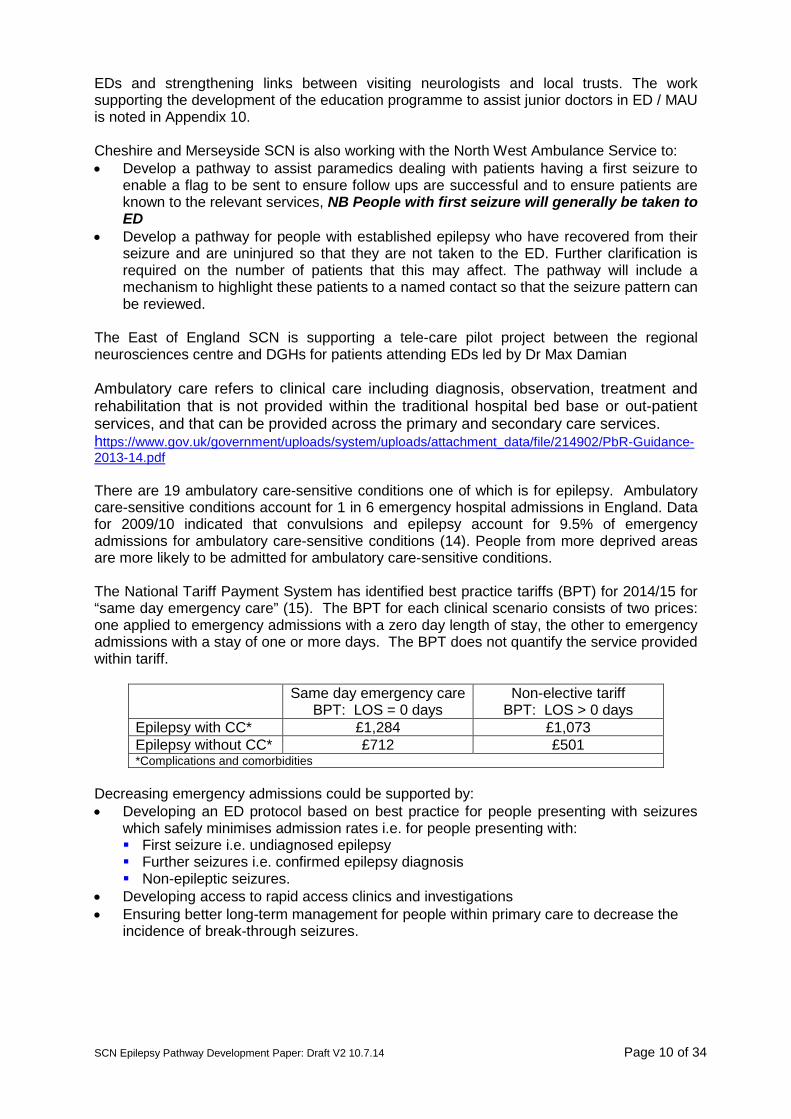
The East of England SCN is supporting a tele-care pilot project between the regional neurosciences centre and DGHs for patients attending EDs led by Dr Max Damian Ambulatory care refers to clinical care including diagnosis, observation, treatment and rehabilitation that is not provided within the traditional hospital bed base or out-patient services, and that can be provided across the primary and secondary care services. https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/214902/PbR-Guidance-2013-14.pdf There are 19 ambulatory care-sensitive conditions one of which is for epilepsy. Ambulatory care-sensitive conditions account for 1 in 6 emergency hospital admissions in England. Data for 2009/10 indicated that convulsions and epilepsy account for 9.5% of emergency admissions for ambulatory care-sensitive conditions (14). People from more deprived areas are more likely to be admitted for ambulatory care-sensitive conditions. The National Tariff Payment System has identified best practice tariffs (BPT) for 2014/15 for “same day emergency care” (15). The BPT for each clinical scenario consists of two prices: one applied to emergency admissions with a zero day length of stay, the other to emergency admissions with a stay of one or more days. The BPT does not quantify the service provided within tariff.
Same day emergency care BPT: LOS = 0 days
Non-elective tariff BPT: LOS > 0 days
Epilepsy with CC* £1,284 £1,073 Epilepsy without CC* £712 £501 *Complications and comorbidities
Decreasing emergency admissions could be supported by: • Developing an ED protocol based on best practice for people presenting with seizures
which safely minimises admission rates i.e. for people presenting with: First seizure i.e. undiagnosed epilepsy Further seizures i.e. confirmed epilepsy diagnosis Non-epileptic seizures.
• Developing access to rapid access clinics and investigations • Ensuring better long-term management for people within primary care to decrease the
incidence of break-through seizures.

SCN Epilepsy Pathway Development Paper: Draft V2 10.7.14 Page 11 of 34
Overall the outcomes for this work would be associated with: • Decreased attendance at the ED • Decrease in emergency admissions • Reduction in the number of patients started on medication inappropriately. National guidelines should be used for patients admitted in status epilepticus (Appendices 11 and 12). In addition, DGHs should liaise with specialist centres e.g. Neurological ICUs to support patient care for example regarding ventilator weaning. Actions for SCNs: • Define the clinical care which should be provided as part of the BPT for ambulatory
care • Clarify the ED tariff and in-patient bed day rate to compare with the BPT for
ambulatory care • Support better liaison between specialist centres and DGHs
8. Providing on-going support People diagnosed with epilepsy require on-going support to ensure that their condition is managed as well as possible. The Quality Outcomes Framework (16) enables GPs to use the incentive scheme to report data on epilepsy against the following indicators: • The practice establishes and maintains a register of patients aged 18 and over receiving
drug treatment for epilepsy • The percentage of patients aged 18 and over on drug treatment for epilepsy who have
been seizure free for the last 12 months recorded in the preceding 12 months • The percentage of women aged 18 or over and who have not attained the age of 55 who
are taking antiepileptic drugs, who have a record of information and counselling about contraception, conception and pregnancy in the preceding 12 months.
City Hospitals Sunderland (13) has described the focus for primary care on annual reviews which include: • Date of last seizure • Seizure frequency • Side effects of AEDs • Adjustment of AEDs according to agreed management plan • Concordance with medication • Check Vitamin D and calcium due to risk of osteoporosis with AEDs • Lifestyle advice • Checking the patient’s understanding of the condition and information provided Patients should be re-referred to secondary care services when: • Seizures persist • There are problems with medication • Neurological signs or symptoms are present • The patient is in status epilepticus – referral via the Emergency Department (ED) • Specialist advice is required e.g. pre-conceptual counselling. Improving self-care and self-management is an important part of optimising care. This can be supported through information provided to patients and education programmes and is often supported through access to ESNs.
SCN Epilepsy Pathway Development Paper: Draft V2 10.7.14 Page 12 of 34
Actions for SCNs: • Support GPs to provide standardised annual reviews • Identify evidence to support the effectiveness of self-management programmes
9. Improving access to ESNs Patients and carers routinely report the benefits of having access to an Epilepsy Specialist Nurse (ESN) (17). Improving access to ESNs would provide patients and carers with support and information which could in turn: • Improve the psychological well-being of people with epilepsy • Reduce the number of deaths associated with epilepsy by emphasising the importance
of concordance with drug regimens • Decrease the incidence of teratogenicity by support offered to women of child-bearing
age • Decrease emergency admissions • Decrease length of stay for patients admitted to hospital • Decrease secondary care outpatient follow-up appointments. Previous work in Greater Manchester involved the development of a specification for services delivered by ESNs, which included a supporting role within the community for patients who find it difficult to access clinic appointments and for GP practices to support delivery of the epilepsy QOF indicators.
The Greater Manchester work also recommended that the ESN service could be improved by: • Developing a pool of ESNs to work across the conurbation reducing concerns about
single handed practitioners and facilitating cover for annual leave, sick leave etc. • Commissioning the ESNs model of care through a “hub and spoke” arrangement hosted
by the Neurosciences Centre with the aim of decreasing appointments in secondary care.
• Facilitating communication between GPs and specialist services and providing greater support to GPs.
The East of England SCN is working with the South Norfolk CCG to develop a community adult ESN service. The previous service was delivered by 1.6 wte ESNs with a caseload of 299 i.e. well-below the expected 3000 patients. Admission rates were also increasing with a cost of £2.6m in 2011/12. The proposal developed options for a gold, silver and bronze standard service based on: • The experience of the ESN • Links with cardiology • Introduction of transition clinics • Nurse prescribing • Delivery of education packages to ambulance services • Support in EDs • Support in care homes • Working with mental health and LD teams More information is available via [email protected]
SCN Epilepsy Pathway Development Paper: Draft V2 10.7.14 Page 13 of 34
Work has also been completed to agree competencies for ESNs working with adults, children and people with learning disabilities. The competencies have been validated by the RCN. Actions for SCNs: • Support the adoption of national competencies for ESNs • Support the development of training programmes to support succession planning for
ESNs • Develop innovative approaches to utilising ESNs to reduce the demand on
neurologists within secondary care
10. Improving transition The following groups have been identified as having specific needs in relation to epilepsy: • People with learning disabilities: Transition is a key time for people with learning
disabilities and for young people in this situation a longer period of transition may be required to accommodate the additional complexity of their clinical and psychological needs.
• Older people: Many older patients experiencing first seizures or transient loss of consciousness are seen in TIA clinics where clinicians may not have experience of diagnosing and treating epilepsy
• Women of child bearing age: This is an area of care which is important to reduce the incidence of teratogenicity. Providers of children’s and obstetrics services need to work together to ensure continuity of care and support for women of child bearing age to receive information regarding contraception, conception, pregnancy, caring for children, breastfeeding and menopause and to ensure that lifestyle issues are addressed for patients in transition from children’s to adult services. Support for the development of pre-conception counselling services for girls and women of childbearing ages could be addressed by collaboration between SCNs focused on neurological conditions and Maternity and Children’s services. Services could be delivered by ESNs directly and indirectly by supporting primary care clinicians (11).
Adolescents transferring from children’s to adult services There is a BPT payable per attendance to follow-up activity captured by a new paediatric epilepsy treatment function code, which has been introduced specifically to capture activity delivered in line with best practice. Activity not meeting best practice will be paid at the outpatient attendance tariff for general paediatrics. The general paediatric tariff (non BPT) is included below for information and comparison (15). Non-best practice tariff
Paediatric epilepsy
Follow-up Attendance: Single Professional
Follow-up Attendance: Multi Professional
Best practice tariff (£)
£123 £160 £170 There are workforce issues for children with epilepsy particularly on discharge into the community. South East Coast SCN is supporting work on transition from ‘Children’s & Young Peoples’ services to adult services. Best practice pathways are under development for three long term conditions including epilepsy supported by a number of key national documents. Young people with long term conditions need preparation as they move from children’s to adult services. All young people with on-going health needs should have a plan developed with them for the transition of their care to adult services, which is co-ordinated by a named person (18). Poorly planned transition from young people’s to adult-oriented health services

SCN Epilepsy Pathway Development Paper: Draft V2 10.7.14 Page 14 of 34
can be associated with increased risk of non-adherence to treatment and loss to follow-up, which can have serious consequences. There are measurable adverse consequences in terms of morbidity and mortality as well as in social and educational outcomes (19). NICE has produced a quality standard for the epilepsies in children and young people (20). The quality standard specifies that services should be commissioned from and coordinated across all relevant agencies encompassing the whole epilepsy care pathway. The standard acknowledges that an integrated approach to the provision of services is fundamental to the delivery of high-quality care by multidisciplinary teams through a local epilepsy clinical network. With specific reference to transition, Quality Statement 9 recommends that young people with epilepsy should have an agreed transition period during which their continuing epilepsy care is reviewed jointly by paediatric and adult services. It notes the need for continuity of care during transition from paediatric services to adult services to enable young people to manage the physical and mental transition from adolescence to adulthood. Good management of transition is considered vital to the development of self-esteem and confidence and provides an opportunity to review the diagnosis, classification, cause and management of a young person's epilepsy before they enter adulthood. Support for better transition services may lead to greater costs e.g. with the provision of joint clinics but it is unlikely that this would be significant, http://www.nice.org.uk/guidance/cmg47 Actions for SCNs: • Use the AQuA work developed by Dr Christian De Goede to support self-management
around transition • Define outcomes associated with access to MDTs for transition which include
vocational and social support • Link with Maternity & Children SCNs to support this work

SCN Epilepsy Pathway Development Paper: Draft V2 10.7.14 Page 15 of 34
Appendix 1 Epilepsy overview (NICE CG 137). Last updated: 21 February 2014
NB: Need to link this group into pathways for people with
other functional disorders

SCN Epilepsy Pathway Development Paper: Draft V2 10.7.14 Page 16 of 34
Appendix 2 Greater Manchester: Overall Management of Seizure Disorders
Primary Care Secondary Care
Management of First Seizures
Disorders
Patient present with suspected
seizure
Patient attends A&E with
suspected Seizure
Refer to specialist Secondary Care
Neurologist or GPSI within 2 weeks
Patient admitted to DGH if other
neurological signs present
Carry out relevant investigations within
4 weeks & start treatment
Not epilepsy – consider other diagnosis. Refer
back to GP or appropriate clinical
service
Epilepsy Diagnosed
Seizures Controlled
Follow up 12 months by a specialist then
refer back to primary care
Review Diagnosis / Management
Refer to tertiary centre – see criteria
Seizures not controlled
Refer to regional/national services – see
criteria
Seizures not controlled
Go to Long Term Management of
Seizures
Seizures not controlled
SCN Epilepsy Pathway Development Paper: Draft V2 10.7.14 Page 17 of 34
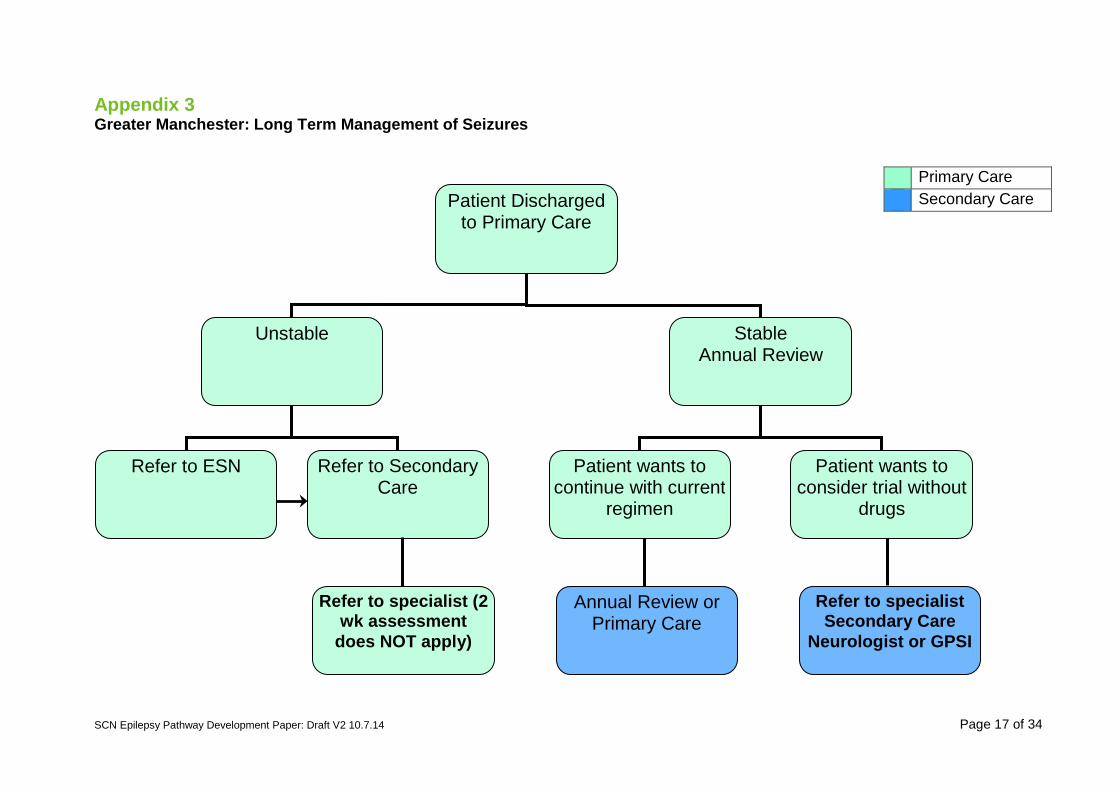
Appendix 3 Greater Manchester: Long Term Management of Seizures
Primary Care Secondary Care
Annual Review or Primary Care
Refer to specialist Secondary Care
Neurologist or GPSI
Patient Discharged to Primary Care
Unstable
Refer to ESN Refer to Secondary Care
Refer to specialist (2 wk assessment
does NOT apply)
Stable Annual Review
Patient wants to continue with current
regimen
Patient wants to consider trial without
drugs

SCN Epilepsy Pathway Development Paper: Draft V2 10.7.14 Page 18 of 34
Appendix 4 Epilepsy Journey, Vale of York CCG – Neurological Commissioning Support

SCN Epilepsy Pathway Development Paper: Draft V2 10.7.4 Page 19 of 34
Appendix 5 Do Once and Share Programme: Connecting for Health 2005 Entry on to pathway via Primary Care or Acute services
Continuation of pathway through specialist services
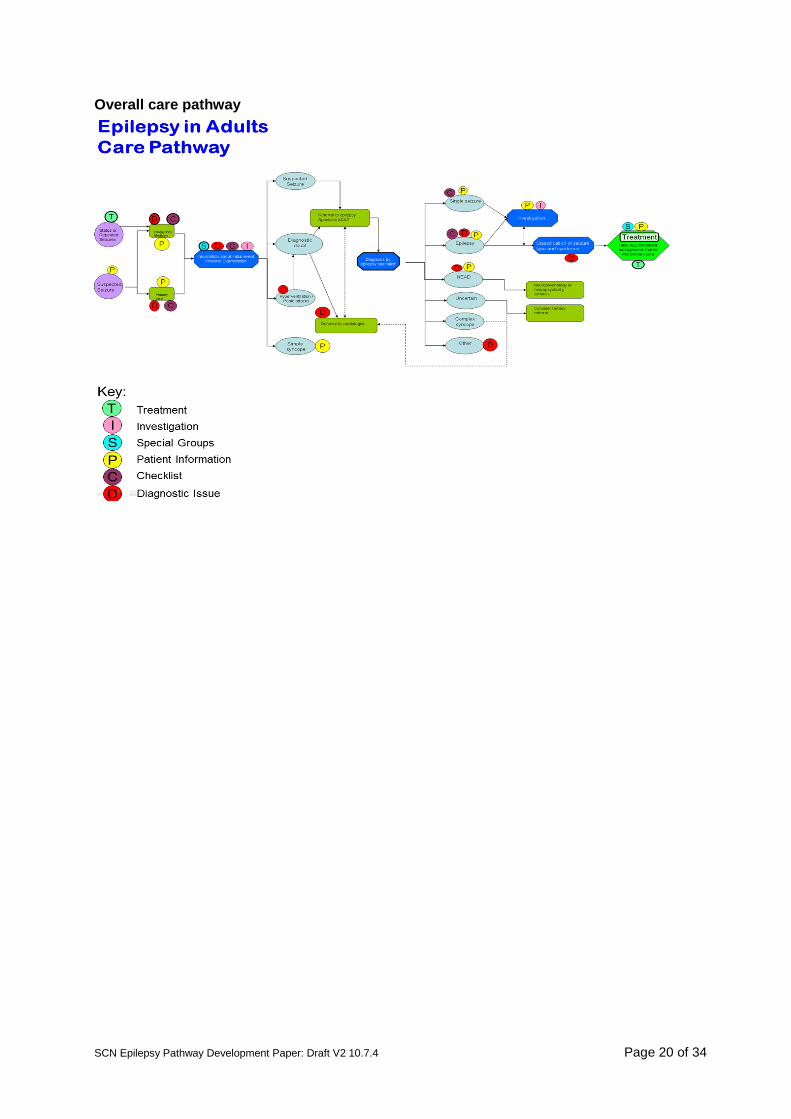
SCN Epilepsy Pathway Development Paper: Draft V2 10.7.4 Page 20 of 34
Overall care pathway

SCN Epilepsy Pathway Development Paper: Draft V2 10.7.4 Page 21 of 34
Appendix 6 Pathway for transient loss of consciousness: Central Manchester NHS FT

SCN Epilepsy Pathway Development Paper: Draft V2 10.7.4 Page 22 of 34
Appendix 7
Guidelines for the Management of First Seizure in the Emergency Department
GEMNet, 2009
The guidelines identify evidence based practice around: 1. Laboratory investigations and bedside tests:
• Determine a Serum glucose and sodium level • Breath alcohol test • Pregnancy test • ECG • Toxicology screen, bedside tests, chest X-ray and lumbar puncture if clinically
indicated
2. Neuroimaging • Neuroimaging when intracranial lesion suspected • Neuroimaging can be deferred in ED when early access is available • MRI preferable to CT except with acutely ill patients
3. EEG
• Not routinely performed in ED or requested by emergency physician 4. Admission
• Discharge from ED for those patients with full recovery, no neurological deficit and normal initial investigations
• Consider admission for those with alcoholism, poor social circumstances or those without a responsible adult to stay with
5. Treatment
• AEDs should not routinely be prescribed in the ED and if they are this should be based on consultation with an epilepsy specialist
6. Advice
• Written and verbal advice about driving and lifestyle 7. Follow-up
• Follow up within 2 weeks if possible with an epilepsy specialist

SCN Epilepsy Pathway Development Paper: Draft V2 10.7.4 Page 23 of 34
Appendix 8 Summary of NASH Adult Report
Introduction The National Audit of Seizure Management in Hospitals (NASH) was initiated by Professor Tony Marson and Professor Mike Pearson from the University of Liverpool. With funding provided by pharmaceutical companies, and with a Steering Board comprising representatives from a number of professional medical organisations, patient charities and each of the home nations, it is the first comprehensive audit of epilepsy and seizures in the UK. There have been two iterations of NASH; NASH1 took place in 2011 and NASH2 took place in 2013. The first audit was based on the 2004 NICE guidelines, and NASH 2 relates also to the revision “NICE CG137 (January 2012)”. Both audits examined the care given to adult patients presenting to an Emergency Department (ED) as a result of a seizure. This is a reasonably clear event from which a series of assessments and actions should follow. A seizure in someone with known epilepsy represents a failure of therapeutic control, so in addition to managing the seizure, an assessment of previous management and revision of therapy should be considered to try and prevent a repeat episode. The aims of the audits were to: • Describe and understand the organisation of care available for people presenting to EDs
with seizures • Describe the variations in care actually delivered; and • Set out options and opportunities for improving care and to share those with the
hospitals, patient organisations and NHS managers in the hope that together they can act to effect improvement.
Taken together, the two NASH audits have examined data on over 8,300 attendances at ED (3,759 from 127 sites in NASH1, and 4,544 from 154 sites in NASH2). The results show that much of the care is far from optimal across the country (see below). However, it is important to note that whilst NASH uses attendance at ED as a means of identifying patients to be included in the audit, the questions cover the care given prior to attendance during their episode and onward care. Consequently, if epilepsy care is to change then action is needed to address the whole spectrum across primary, secondary and tertiary care, i.e. the whole patient pathway. The audits are specific to attendance at EDs and provide an indication of the care received in these facilities. Whilst it is important that care within EDs improves further work is required to understand the service provided to inform diagnosis, initial treatment and on-going support which will decrease the possibility of break through seizures requiring attendance at an ED. Methodology Individual hospitals returned data on at least 30 consecutive adult patients presenting with a seizure detailing both process of care and clinical outcomes. Data was entered on a secure online system. The questions in NASH2 were mostly the same as those in NASH1, with some alterations and additions made based on feedback to the first audit. Findings Three key findings emerge: • Whilst the second audit showed small but significant improvements from NASH1 for
many variables, it is unlikely that these changes would be perceptible to patients • High performing sites tend to perform well across most variables and vice versa; and • The variation between the best performing and least well performing sites is extremely
wide.
SCN Epilepsy Pathway Development Paper: Draft V2 10.7.4 Page 24 of 34
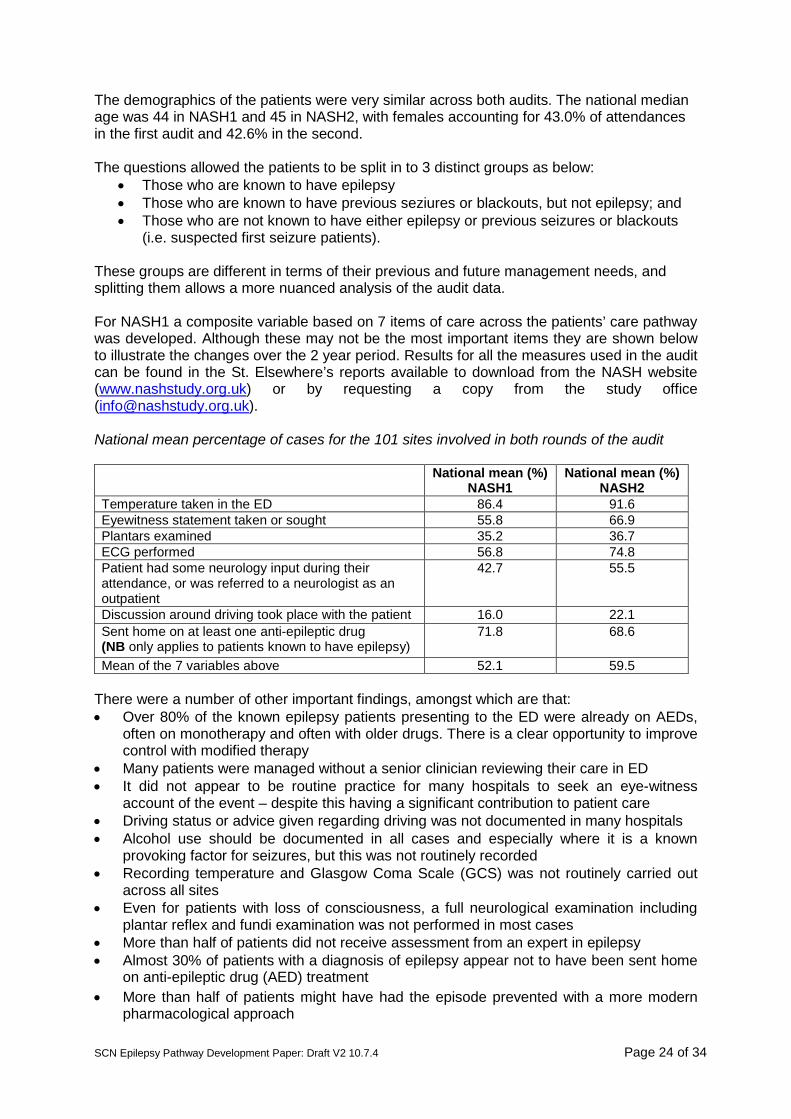
The demographics of the patients were very similar across both audits. The national median age was 44 in NASH1 and 45 in NASH2, with females accounting for 43.0% of attendances in the first audit and 42.6% in the second. The questions allowed the patients to be split in to 3 distinct groups as below:
• Those who are known to have epilepsy • Those who are known to have previous seziures or blackouts, but not epilepsy; and • Those who are not known to have either epilepsy or previous seizures or blackouts
(i.e. suspected first seizure patients). These groups are different in terms of their previous and future management needs, and splitting them allows a more nuanced analysis of the audit data.
For NASH1 a composite variable based on 7 items of care across the patients’ care pathway was developed. Although these may not be the most important items they are shown below to illustrate the changes over the 2 year period. Results for all the measures used in the audit can be found in the St. Elsewhere’s reports available to download from the NASH website (www.nashstudy.org.uk) or by requesting a copy from the study office ([email protected]). National mean percentage of cases for the 101 sites involved in both rounds of the audit National mean (%)
NASH1 National mean (%)
NASH2 Temperature taken in the ED 86.4 91.6 Eyewitness statement taken or sought 55.8 66.9 Plantars examined 35.2 36.7 ECG performed 56.8 74.8 Patient had some neurology input during their attendance, or was referred to a neurologist as an outpatient
42.7 55.5
Discussion around driving took place with the patient 16.0 22.1 Sent home on at least one anti-epileptic drug (NB only applies to patients known to have epilepsy)
71.8 68.6
Mean of the 7 variables above 52.1 59.5 There were a number of other important findings, amongst which are that: • Over 80% of the known epilepsy patients presenting to the ED were already on AEDs,
often on monotherapy and often with older drugs. There is a clear opportunity to improve control with modified therapy
• Many patients were managed without a senior clinician reviewing their care in ED • It did not appear to be routine practice for many hospitals to seek an eye-witness
account of the event – despite this having a significant contribution to patient care • Driving status or advice given regarding driving was not documented in many hospitals • Alcohol use should be documented in all cases and especially where it is a known
provoking factor for seizures, but this was not routinely recorded • Recording temperature and Glasgow Coma Scale (GCS) was not routinely carried out
across all sites • Even for patients with loss of consciousness, a full neurological examination including
plantar reflex and fundi examination was not performed in most cases • More than half of patients did not receive assessment from an expert in epilepsy • Almost 30% of patients with a diagnosis of epilepsy appear not to have been sent home
on anti-epileptic drug (AED) treatment • More than half of patients might have had the episode prevented with a more modern
pharmacological approach
SCN Epilepsy Pathway Development Paper: Draft V2 10.7.4 Page 25 of 34
• Most patients were not under specialist review Onward referral for specialist input occurred for less than half of patients, and of those referred many did not attend.
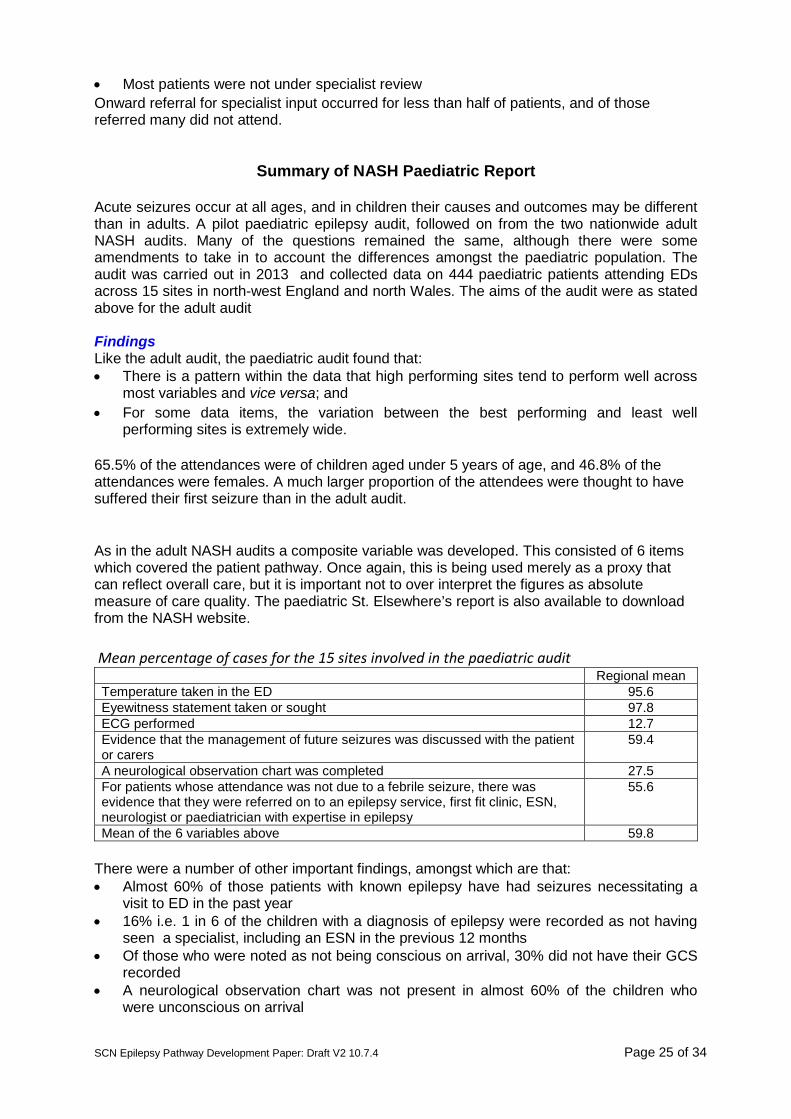
Summary of NASH Paediatric Report
Acute seizures occur at all ages, and in children their causes and outcomes may be different than in adults. A pilot paediatric epilepsy audit, followed on from the two nationwide adult NASH audits. Many of the questions remained the same, although there were some amendments to take in to account the differences amongst the paediatric population. The audit was carried out in 2013 and collected data on 444 paediatric patients attending EDs across 15 sites in north-west England and north Wales. The aims of the audit were as stated above for the adult audit Findings Like the adult audit, the paediatric audit found that: • There is a pattern within the data that high performing sites tend to perform well across
most variables and vice versa; and • For some data items, the variation between the best performing and least well
performing sites is extremely wide. 65.5% of the attendances were of children aged under 5 years of age, and 46.8% of the attendances were females. A much larger proportion of the attendees were thought to have suffered their first seizure than in the adult audit. As in the adult NASH audits a composite variable was developed. This consisted of 6 items which covered the patient pathway. Once again, this is being used merely as a proxy that can reflect overall care, but it is important not to over interpret the figures as absolute measure of care quality. The paediatric St. Elsewhere’s report is also available to download from the NASH website. Mean percentage of cases for the 15 sites involved in the paediatric audit Regional mean Temperature taken in the ED 95.6 Eyewitness statement taken or sought 97.8 ECG performed 12.7 Evidence that the management of future seizures was discussed with the patient or carers
59.4
A neurological observation chart was completed 27.5 For patients whose attendance was not due to a febrile seizure, there was evidence that they were referred on to an epilepsy service, first fit clinic, ESN, neurologist or paediatrician with expertise in epilepsy
55.6
Mean of the 6 variables above 59.8 There were a number of other important findings, amongst which are that: • Almost 60% of those patients with known epilepsy have had seizures necessitating a
visit to ED in the past year • 16% i.e. 1 in 6 of the children with a diagnosis of epilepsy were recorded as not having
seen a specialist, including an ESN in the previous 12 months • Of those who were noted as not being conscious on arrival, 30% did not have their GCS
recorded • A neurological observation chart was not present in almost 60% of the children who
were unconscious on arrival

SCN Epilepsy Pathway Development Paper: Draft V2 10.7.4 Page 26 of 34
• Many patients were managed without a senior review, but of those who did see a specialist nearly all are seen within 4 hours of arrival at ED
• Over 95% of patients had an eyewitness statement • For those children who arrived at ED after experiencing a febrile seizure, very few
underwent unnecessary investigations e.g. EEG and MRI scans which would be carried out to diagnose definite or probable epilepsy
• Documentation on the management of future seizures was recorded in less than 60% of the cases attending ED
St. Elsewhere’s reports are available to download from the NASH website: www.nashstudy.org.uk Further information on NASH can be obtained by emailing the study office: [email protected]

SCN Epilepsy Pathway Development Paper: Draft V2 10.7.4 Page 27 of 34
Appendix 9 Cheshire & Merseyside A&E Pathway
Walton Centre Epilepsy / Seizure Management Pathway
SUSPECTED SEIZURE
Normal rhythm / QRS / PR / QTc AND
Cardiac cause clinically unlikely
Secure and record eyewitness account if
available
ECG
Abnormal ECG • Cardiac cause clinically
possible • Epilepsy unlikely /
uncertain • ECG abnormality likely
to be relevant Seizure clinically likely
SEIZURE PATHWAY
Refer cardiology

SCN Epilepsy Pathway Development Paper: Draft V2 10.7.4 Page 28 of 34
WALTON CENTRE EPILEPSY / SEIZURE PATHWAY
First seizure
Epilepsy / recurrent seizure
Possible causes of symptomatic seizures • Tumour • CVA • Subarachnoid haemorrhage • Trauma • Drugs / alcohol • Encephalitis / meningitis • Cerebral sinus thrombosis • Pregnancy (eclampsia) • Metabolic (eg hyponatraemia;
hypoglycaemia; DKA) Pointers: • Fever, meningism • Focal signs, papilloedema • Persistent and/or sudden onset
headache • Impaired consciousness / altered
mental state >60 minutes • Recurrent (serial) seizures / status • After acute head trauma • Malignancy, immunosuppression,
bleeding tendency, alcoholism
Consider and assess clinically for possible secondary / symptomatic causes (box) • History • Examination (consciousness, fundi,
plantars, temperature, ears, meningism) • Glucose (treat immediately if low) • U&E, FBC, calcium • Toxicology including alcohol level (if
indicated) • Anticonvulsant levels • Pregnancy test (if applicable)
Evidence of serious underlying cause / symptomatic seizure? (See box for list of symptomatic causes and clinical pointers) NO (circle) YES
ADMIT • See status treatment sheet if
required; • consider investigating for causes in
box above scan (CT / MR) • LP if required and safe • CT for haemorrhage / trauma • MRV / CTV required in selected
cases • Request neuro advice
o DGH consult o SpR Walton 0151 525 3611
• Single self-limiting attack • Recovered after 60 minutes • Normal examination and bloods • Senior review
YES (circle) NO
• Discharge with advice sheet LABEL (name, number, address, telephone)
• Affix patient label • Fax this form to 0151 529 5769 WITH:
o clinical notes o eyewitness account o ECG & bloods Tel No:

SCN Epilepsy Pathway Development Paper: Draft V2 10.7.4 Page 29 of 34
WALTON CENTRE
STATUS EPILEPTICUS MANAGEMENT ADVICE Status epilepticus is defined as seizures lasting continuously >30 minutes but initiate status management if convulsions continue >5 minutes or are still on-going on arrival at A&E.
• Airway • Oxygen • IV access and circulation • ECG monitoring (trace may be difficult to read during seizures) • Initial investigations
o FBC; U&E; glucose; gases; toxicology; anticonvulsant levels o ECG when possible
• Always consider possibility of non-epileptic attacks (review notes)
Antiepileptic and other therapy
1. Lorazepam 0.1mg/kg (usually 4mg bolus) IV *
2. 50ml of 50% glucose IV + Pabrinex IVHP if alcohol abuse / nutritional deficiency
3. If seizures stop always give maintenance antiepileptic drugs (AED) therapy - load with phenytoin as below orally or IV; re-start any existing AEDs (reverse any recent reductions or discontinuations);
4. If seizures continue repeat lorazepam 4mg IV and/or start phenytoin 20mg/kg IV at 50mg/minute with ECG monitoring – if seizures continue go to 5.
5. If seizures continue call ITU / anaesthetics; consider intubation; ITU admission; EEG monitoring if available
a. Thiopental 3-5mg/kg bolus then infusion titrated to effect; review dose daily; reduce after 2-3 days as fat stores saturate
b. Midazolam 0.1-0.2mg/kg bolus then infusion as clinically indicated c. Propofol 1-2mg/kg bolus then infusion as clinically indicated
Neurological advice
Contact on-call neurology SpR on 0151 525 3611 for advice if required
*Buccal midazolam 10mg can be used if no IV access / successfully used previously / out of hospital scenario
* If eclamptic seizures use 4g IV magnesium sulphate and liaise with obstetrics

SCN Epilepsy Pathway Development Paper: Draft V2 10.7.4 Page 30 of 34
Appendix 10
Cheshire & Merseyside SCN
Education Programme The work is supporting the development of the education programme to assist junior doctors in ED / MAU to gain a better understanding of seizure management and improve the management of seizures to help reduce A&E admissions. Actions to date: • Option to work with the Deanery to include more in the foundation curriculum around
seizures. • Telephone conversation with BMJ to understand what they can offer via their e-learning
module that supports the Deanery Foundation programme. The BMJ are happy to work with us but it would be on a commissioned basis and the fees would be around £30k for a programme to be produced.
• All training providers have been scoped to identify what is offered. • A meeting has been held with the lead of education at Health Education North West to
get an understanding of where seizures fall within their work priorities and identify support for education.
• An education programme has been drafted and outlined working with an A&E Consultant and an interested neurologist to develop a training programme for delivery by the SCN to each A&E/ MAU department.

SCN Epilepsy Pathway Development Paper: Draft V2 10.7.4 Page 31 of 34
Appendix 11
Protocols for treating convulsive status epilepticus in adults (NICE 2004)
General measures: 1st stage - 0−10 minutes • Secure airway and resuscitate • Administer oxygen • Assess cardiorespiratory function • Establish intravenous access Early status: 2nd stage - 0−30 minutes • Institute regular monitoring • Consider the possibility of non-epileptic status • Emergency AED therapy • Emergency investigations • Administer glucose (50 ml of 50% solution) and/or intravenous thiamine (250 mg) as
high potency intravenous Pabrinex if any suggestion of alcohol abuse or impaired nutrition
• Treat acidosis if severe 3rd stage - 0−60 minutes • Establish aetiology • Alert anaesthetist and ITU • Identify and treat medical complications • Pressor therapy when appropriate Established status: 4th stage - 30−90 minutes • Transfer to intensive care • Establish intensive care and EEG monitoring • Initiate intracranial pressure monitoring where appropriate • Initiate long-term, maintenance AED therapy Refractory status • Blood should be taken for blood gases, glucose, renal and liver function, calcium and
magnesium, full blood count (including platelets), blood clotting, AED drug levels; 5 ml of serum and 50 ml of urine samples should be saved for future analysis, including toxicology, especially if the cause of the convulsive status epilepticus is uncertain. Chest radiograph to evaluate possibility of aspiration. Other investigations depend on the clinical circumstances and may include brain imaging, lumbar puncture.
• Regular neurological observations and measurements of pulse, blood pressure, temperature.
• ECG, biochemistry, blood gases, clotting, blood count, drug levels. Patients require the full range of ITU facilities and care should be shared between anaesthetist and neurologist.
• EEG monitoring is necessary for refractory status. Consider the possibility of non-epileptic status. In refractory convulsive status epilepticus, the primary end-point is suppression of epileptic activity on the EEG, with a secondary end-point of burst-suppression pattern (that is, short intervals of up to 1 second between bursts of background rhythm).

SCN Epilepsy Pathway Development Paper: Draft V2 10.7.4 Page 32 of 34
Emergency AED therapy for convulsive status epilepticus Premonitory stage (prehospital) • Diazepam 10−20 mg given rectally, repeated once 15 minutes later if status continues to
threaten, or midazolam 10 mg given buccally. If seizures continue, treat as below. Early status • Lorazepam (intravenous) 0.1 mg/kg (usually a 4 mg bolus, repeated once after 10−20
minutes; rate not critical). • Give usual AED medication if already on treatment. • For sustained control or if seizures continue, treat as below. Established status • Phenytoin infusion at a dose of 15–18 mg/kg at a rate of 50 mg/minute or fosphenytoin
infusion at a dose of 15−20 mg phenytoin equivalents (PE)/kg at a rate of 50–100 mg PE/minute and/or phenobarbital bolus of 10–15 mg/kg at a rate of 100 mg/minute.
Refractory status • General anaesthesia, with one of: propofol (1–2 mg/kg bolus, then 2–10 mg/kg/hour)
titrated to effect midazolam (0.1–0.2 mg/kg bolus, then 0.05–0.5 mg/kg/hour) titrated to effect thiopental sodium (3–5 mg/kg bolus, then 3–5 mg/kg/hour) titrated to effect; after 2–3 days infusion rate needs reduction as fat stores are saturated anaesthetic continued for 12−24 hours after the last clinical or electrographic seizure, then dose tapered. In the above scheme, the refractory stage (general anaesthesia) is reached 60/90 minutes after the initial therapy. This scheme is suitable for usual clinical hospital settings. In some situations, general anaesthesia should be initiated earlier and, occasionally, should be delayed.
Experience with long-term administration (hours or days) of the newer anaesthetic drugs is very limited. The modern anaesthetics have, however, important pharmacokinetic advantages over the more traditional barbiturates. AED therapy must be given in parallel with emergency treatment. The choice of drug depends on previous therapy, the type of epilepsy, and the clinical setting. Any pre-existing AED therapy should be continued at full dose, and any recent reductions reversed. If phenytoin or phenobarbital has been used in emergency treatment, maintenance doses can be continued orally or intravenously guided by serum level monitoring. Other maintenance AEDs can be started also, with oral loading doses. Care needs to be taken with nasogastric feeds, which can interfere with the absorption of some AEDs. Once the patient has been free of seizures for 12−24 hours and provided that there are adequate plasma levels of concomitant AEDs, then the anaesthetic should be slowly tapered.
SCN Epilepsy Pathway Development Paper: Draft V2 10.7.4 Page 33 of 34
Appendix 12
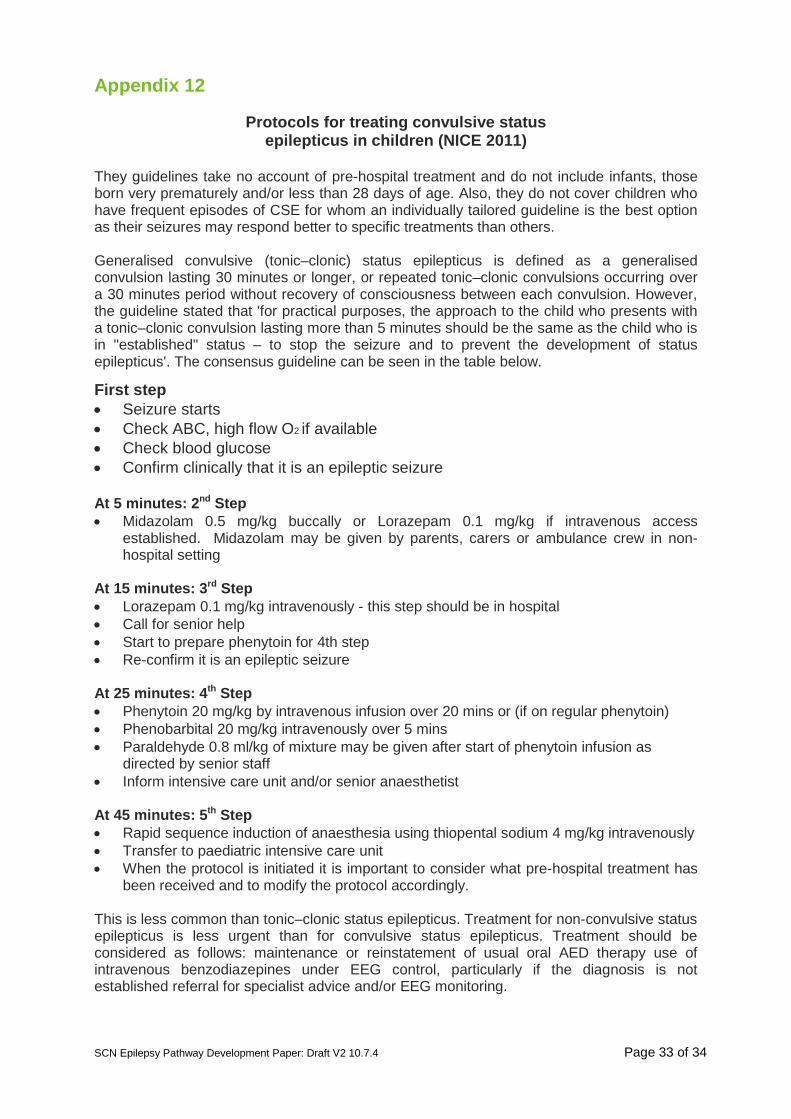
Protocols for treating convulsive status epilepticus in children (NICE 2011)
They guidelines take no account of pre-hospital treatment and do not include infants, those born very prematurely and/or less than 28 days of age. Also, they do not cover children who have frequent episodes of CSE for whom an individually tailored guideline is the best option as their seizures may respond better to specific treatments than others. Generalised convulsive (tonic–clonic) status epilepticus is defined as a generalised convulsion lasting 30 minutes or longer, or repeated tonic–clonic convulsions occurring over a 30 minutes period without recovery of consciousness between each convulsion. However, the guideline stated that 'for practical purposes, the approach to the child who presents with a tonic–clonic convulsion lasting more than 5 minutes should be the same as the child who is in "established" status – to stop the seizure and to prevent the development of status epilepticus'. The consensus guideline can be seen in the table below.
First step • Seizure starts • Check ABC, high flow O2 if available • Check blood glucose • Confirm clinically that it is an epileptic seizure At 5 minutes: 2nd Step • Midazolam 0.5 mg/kg buccally or Lorazepam 0.1 mg/kg if intravenous access
established. Midazolam may be given by parents, carers or ambulance crew in non-hospital setting
At 15 minutes: 3rd Step • Lorazepam 0.1 mg/kg intravenously - this step should be in hospital • Call for senior help • Start to prepare phenytoin for 4th step • Re-confirm it is an epileptic seizure At 25 minutes: 4th Step • Phenytoin 20 mg/kg by intravenous infusion over 20 mins or (if on regular phenytoin) • Phenobarbital 20 mg/kg intravenously over 5 mins • Paraldehyde 0.8 ml/kg of mixture may be given after start of phenytoin infusion as
directed by senior staff • Inform intensive care unit and/or senior anaesthetist At 45 minutes: 5th Step • Rapid sequence induction of anaesthesia using thiopental sodium 4 mg/kg intravenously • Transfer to paediatric intensive care unit • When the protocol is initiated it is important to consider what pre-hospital treatment has
been received and to modify the protocol accordingly. This is less common than tonic–clonic status epilepticus. Treatment for non-convulsive status epilepticus is less urgent than for convulsive status epilepticus. Treatment should be considered as follows: maintenance or reinstatement of usual oral AED therapy use of intravenous benzodiazepines under EEG control, particularly if the diagnosis is not established referral for specialist advice and/or EEG monitoring.

SCN Epilepsy Pathway Development Paper: Draft V2 10.7.4 Page 34 of 34
References 1. Epilepsy Action (2013) A Critical Time for Epilepsy in England. www.epilepsy.org.uk 2. All Party Parliamentary Group on Epilepsy (2007) Wasted money wasted lives 3. NHS Atlas of variation in Health Care (2010) www.rightcare.nhs.uk 4. NICE (2008) Service for the accurate diagnosis of the epilepsies in adults:
Commissioning Guide 5. Fisher et al (2005) Epileptic seizures and epilepsy: definitions proposed by the
International League Against Epilepsy (ILAE) and the International Bureau for Epilepsy (IBE). Epilepsia: 46 (4) 470-2.
6. Joint Epilepsy Council (2011) Epilepsy prevalence, incidence and other statistics 7. Ridsdale. L, Charlton. J, Ashworth. M, et al (2011) Epilepsy Mortality and risk factors
for death in epilepsy: a population based study. British Journal of General Practice: May 271-278
8. Chowdhury, F.A. Nashef, L. Elwes, R.D.C. (2008) Misdiagnosis in epilepsy: a review and recognition of diagnostic uncertainty. European Journal of Neurology: 15; 1034-1042
9. Juarez-Garcia, A. Stokes, T. Shaw, B. Camoosso-Stefinovic, J. Baker, R. (2006) The costs of epilepsy misdiagnosis in England and Wales. Seizure: 15; 598-605
10. Moran et al (2004) Epilepsy in the United Kingdom: seizure frequency and severity, anti-epileptic drug utilization and impact on life in 1652 people with epilepsy. Seizure: 13 (6) 425-433
11. NICE (2012) The epilepsies: the diagnosis and management of the epilepsies in adults and children in primary and secondary care; Clinical Guidelines 137. National Institute for Health and Clinical Excellence; London.
12. GEMNet (2009) Guideline for the Management of First Seizure in the Emergency Department. Guidelines in Emergency Medicine Network
13. Bateman, D.E. & Wingrove, B. (2011) Neurology for General Practitioners including some referral guidance. The Sunderland Hospitals NHS Trust, Sunderland Royal Hospital, Directorate of Neurosciences.
14. Kings Fund (2012) Emergency hospital admissions for ambulatory care-sensitive conditions: identifying the potential for reductions
15. NHS England: National tariff payment system - Annexe 5a National prices https://www.gov.uk/government/publications/national-tariff-payment-system-2014-to-2015
16. Quality and Outcomes Framework 2014/15 http://bma.org.uk/practical-support-at-work/contracts/independent-contractors/qof-guidance
17. Epilepsy Action (2010) Best care: The value of epilepsy specialist nurses. www.epilepsy.org.uk
18. Department of Health (20013) Getting the right start: National Service Framework for children. Standard for Hospital Services
19. Department of Health (2007) Transition: getting it right for young people: Improving the transition of young people with long term conditions.
20. NICE (2013) Quality standard for the epilepsies in children and young people





























