Embed Size (px)
Citation preview

Stålberg, EMG analysis
1
Erik Stålberg
UppsalaSweden
What can we assess with EMG?
• Muscle membrane function - spontaneous
• Muscle fibre characteristics; diameter
• MU organization– number of fibers
– grouping
• N-M transmission
• Motor units– total number
– activation; pattern, fullnessStålberg
Parameters to quantify in Conc/Monopolar EMG
• spontaneous activity
• shape of individual MUPs
• jiggle
• recruitment (early, reduced)
• fullness at strong activation
• dynamic changes with time (fatigue)

Stålberg, EMG analysis
2
Spontaneous activity in normal
• insertional activity
• end-plate noise
• ”nerve spikes”
• positive wave at end-plate zone
Visual scoringSpontaneous activity
from the muscle
FINDING• fibrillation potentials, psw• myotonic discharges• CRD• myokymic discharges• myogenic extra discharges
MEASURE AS
• #/ 10 recording sites
• or +, ++, +++, ++++ – few
– moderate
– abundant
• or– spontaneous or
– after provocation
Visual scoringSpontaneous activity
from the nerve
MEASURE AS
• #/ 10 recording sites
• or +, ++, +++, ++++ – few (per time unit)
– moderate
– abundant
• indicate– spontaneous or
– after provocation
FINDING• neuromyotonic discharges• myokymic discharges• muscle cramps• fasciculations• neurogenic extra discharges
Fib, PSW ?
Myotonic Disch. ?
CRD ?
Spontaneous activity in myopathyMuscular dystrophies
Myositis, IBM
Debrancher Glycogenosis
Acid Maltase Deficiency
Hyperkalemic per paralysis
Myotonic conditions
LGMD 1A
Nemaline myopathy
Myotubular myopathy
Mitochondrial myopathy
Carnitine Deficency
Hypothyroid myopathy
Rhabdomyolysis
Toxic - Chloroquine
- Alcoholic
- Statins
- Colchicine
Yes
No
No
Courtesy R.Liguori, modified

Stålberg, EMG analysis
3
Fib, PSW ?
Myotonic Disch. ?
CRD ?
Spontaneous activity in myopathyMuscular dystrophies
Myositis, IBM
Debrancher Glycogenosis
Acid Maltase Deficiency
Hyperkalemic per paralysis
Myotonic conditions
LGMD 1A
Nemaline myopathy
Myotubular myopathy
Mitochondrial myopathy
Carnitine Deficency
Hypothyroid myopathy
Rhabdomyolysis
Toxic - Chloroquine
- Alcoholic
- Statins
- Colchicine
Yes
No
Yes
Fib, PSW ?
Myotonic Disch. ?
CRD ?
Spontaneous activity in myopathyMuscular dystrophies
Myositis, IBM
Debrancher Glycogenosis
Acid Maltase Deficiency
Hyperkalemic per paralysis
Myotonic conditions
LGMD 1A
Nemaline myopathy
Myotubular myopathy
Mitochondrial myopathy
Carnitine Deficency
Hypothyroid myopathy
Rhabdomyolysis
Toxic - Chloroquine
- Alcoholic
- Statins
- Colchicine
Yes
Yes
Yes
Fib, PSW ?
Myotonic Disch. ?
CRD ?
Spontaneous activity in myopathyMuscular dystrophies
Myositis, IBM
Debrancher Glycogenosis
Acid Maltase Deficiency
Hyperkalemic per paralysis
Myotonic conditions
LGMD 1A
Nemaline myopathy
Myotubular myopathy
Mitochondrial myopathy
Carnitine Deficency
Hypothyroid myopathy
Rhabdomyolysis
Toxic - Chloroquine
- Alcoholic
- Statins
- Colchicine
Yes
No
Yes
Fib, PSW ?
Myotonic Disch. ?
CRD ?
Spontaneous activity in myopathyMuscular dystrophies
Myositis, IBM
Debrancher Glycogenosis
Acid Maltase Deficiency
Hyperkalemic per paralysis
Myotonic conditions
LGMD 1A
Nemaline myopathy
Myotubular myopathy
Mitochondrial myopathy
Carnitine Deficency
Hypothyroid myopathy
Rhabdomyolysis
Toxic - Chloroquine
- Alcoholic
- Statins
- Colchicine
Yes
No
No
Stålberg, EMG analysis
4
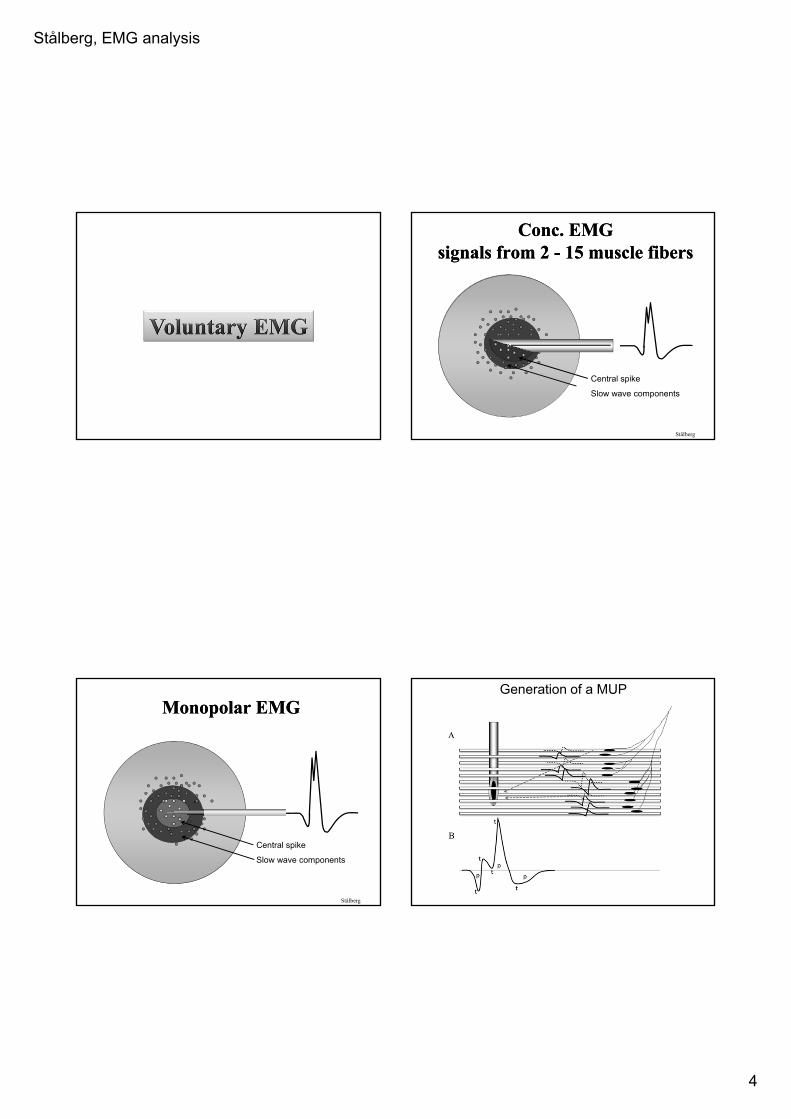
Conc. EMGsignals from 2 - 15 muscle fibers
Conc. EMGsignals from 2 - 15 muscle fibers
Stålberg
Central spike
Slow wave components
Monopolar EMGMonopolar EMG
Stålberg
Central spike
Slow wave components
Generation of a MUP
Stålberg, EMG analysis
5
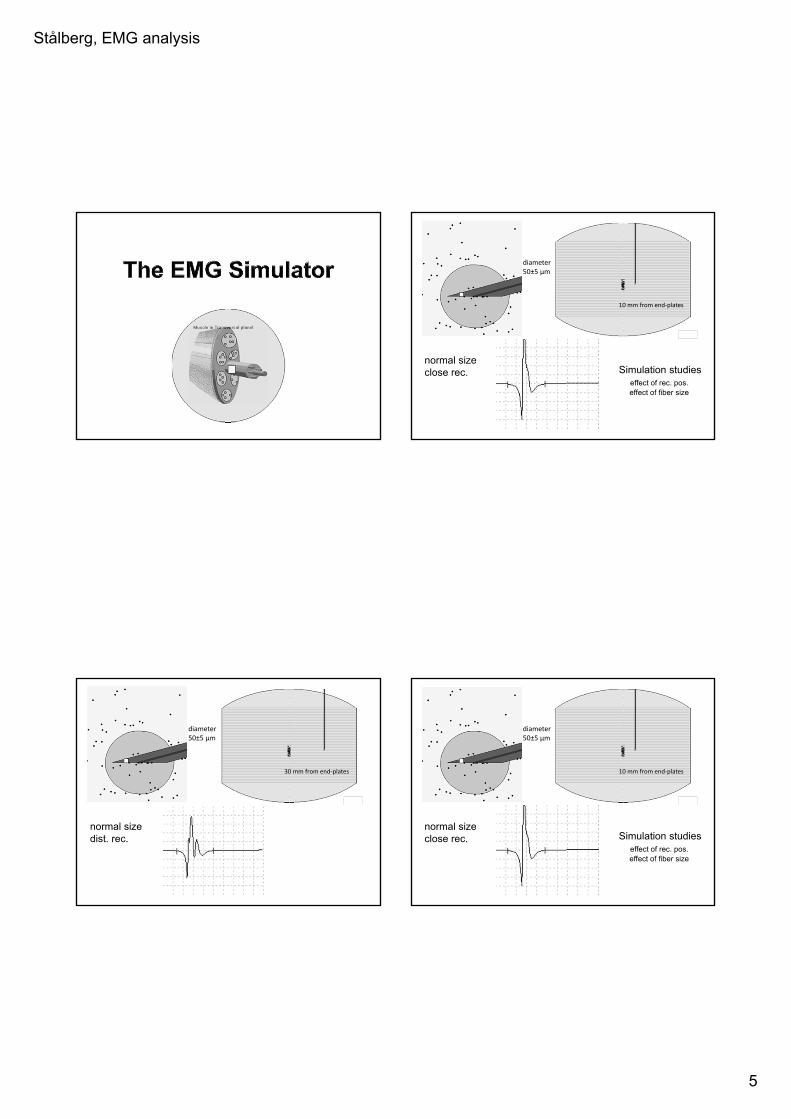
diameter50±5 µm
10 mm from end‐plates
Simulation studieseffect of rec. pos.effect of fiber size
normal sizeclose rec.
diameter50±5 µm
30 mm from end‐plates
normal sizedist. rec.
diameter50±5 µm
10 mm from end‐plates
Simulation studieseffect of rec. pos.effect of fiber size
normal sizeclose rec.

Stålberg, EMG analysis
6
10 mm from end‐plates
diameter40±15 µm
diam. variationclose rec.
30 mm from end‐plates
diameter40±15 µm
diam. variationclose rec.
oppositeside of nmj
end of propat tendon
slowly propSFAPrepolarisation
T
T
T
T
duration
startat nmj
phase
Stålberg
T
T
T
Parameters used in MUP analysis
parameter significance measurement
• Amplitude # fibers/0.5mm peak-peak
• Area # fibers/2 mm within dur
• Duration # fibers in 2.5 mm slope criteria
• Thickness # close fibre area/ampl
• Size index MU size normalized thickness
• Phases temp dispersion 0-cross + 1
• Turns “ change in dir
• Irregularity “ length/ampl
• Rise time closeness to fibre neg-pos peak
• Satellites extreme delay late spike
• Jiggle n-m transm shape stabilityStålberg

Stålberg, EMG analysis
7
This example: Multi MUP analysis
techniques to decompose a mixed signal into its constituents
Decomposition;
Stålberg
A
BC
500 uV
10 ms
Normal
Neuropathy
Myopathy
Multi-MUP analysis in different disorders
Stålberg
Stålberg, EMG analysis
8
AmpLItu d e
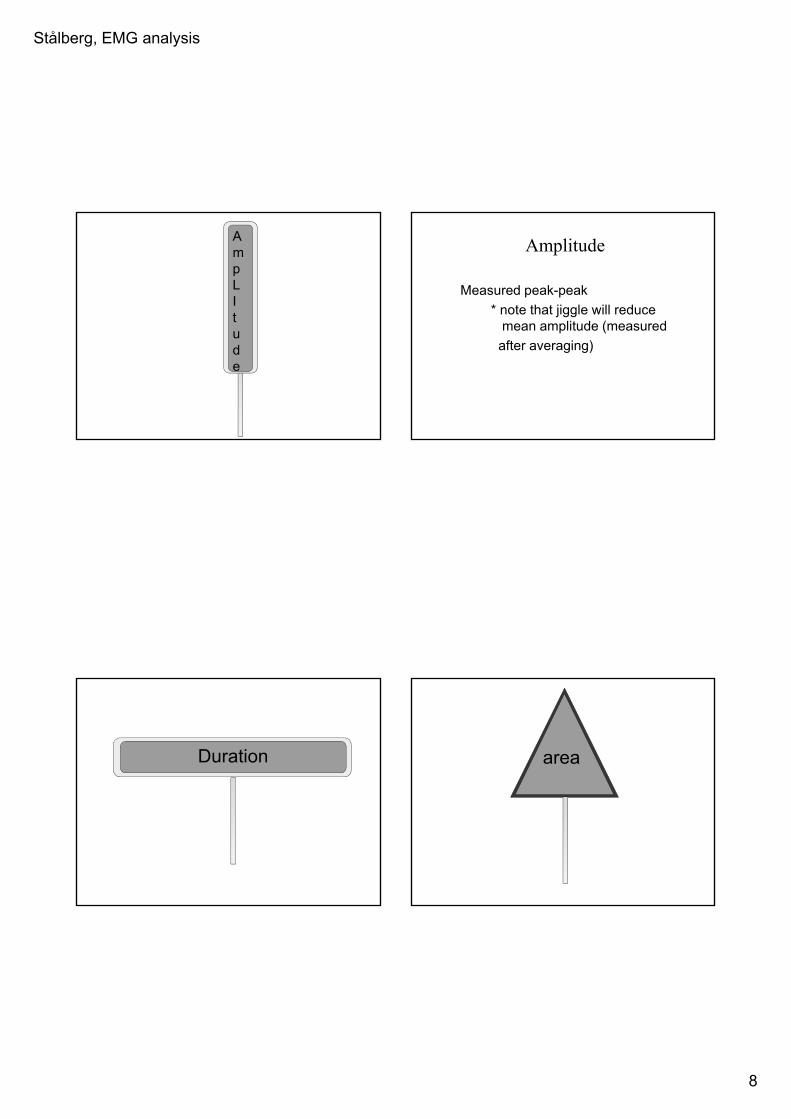
Amplitude
Measured peak-peak
* note that jiggle will reduce mean amplitude (measured
after averaging)
Duration area
Stålberg, EMG analysis
9
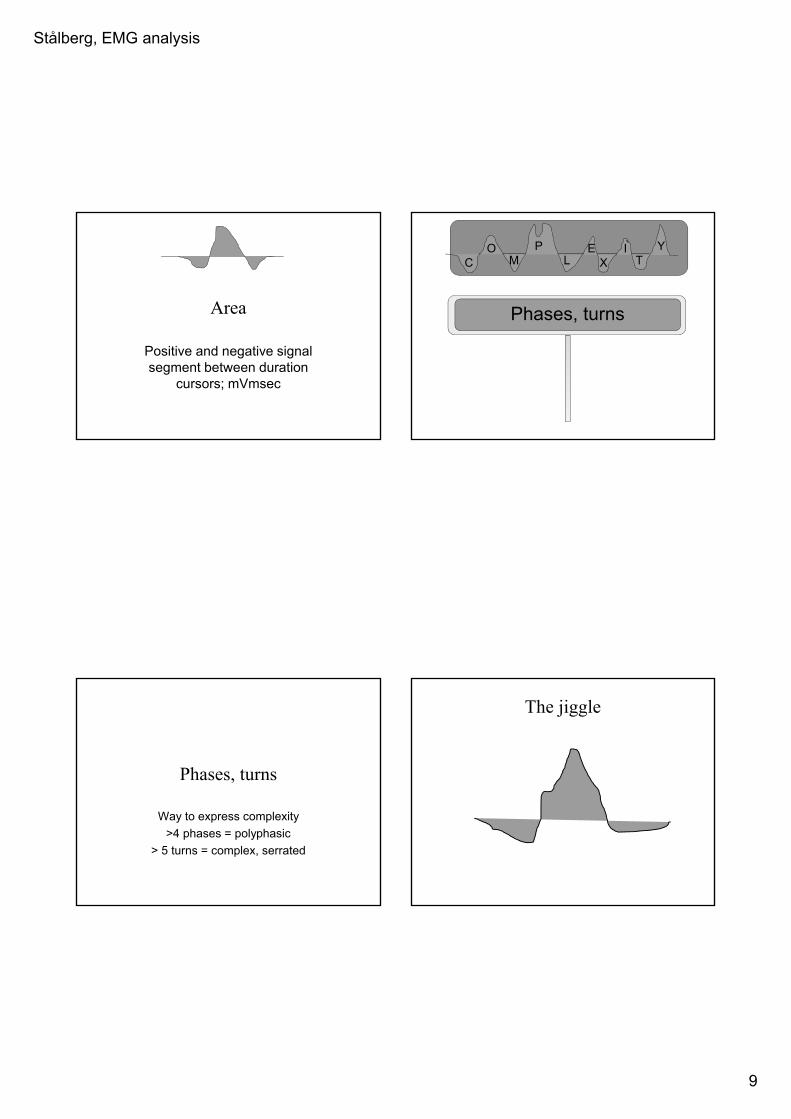
Area
Positive and negative signal segment between duration
cursors; mVmsec
C XE
LP
MO
TI Y
Phases, turns
Phases, turns
Way to express complexity
>4 phases = polyphasic
> 5 turns = complex, serrated
The jiggle

Stålberg, EMG analysis
10
The jiggle The jiggle
The jiggle The jiggle
Stålberg, EMG analysis
11
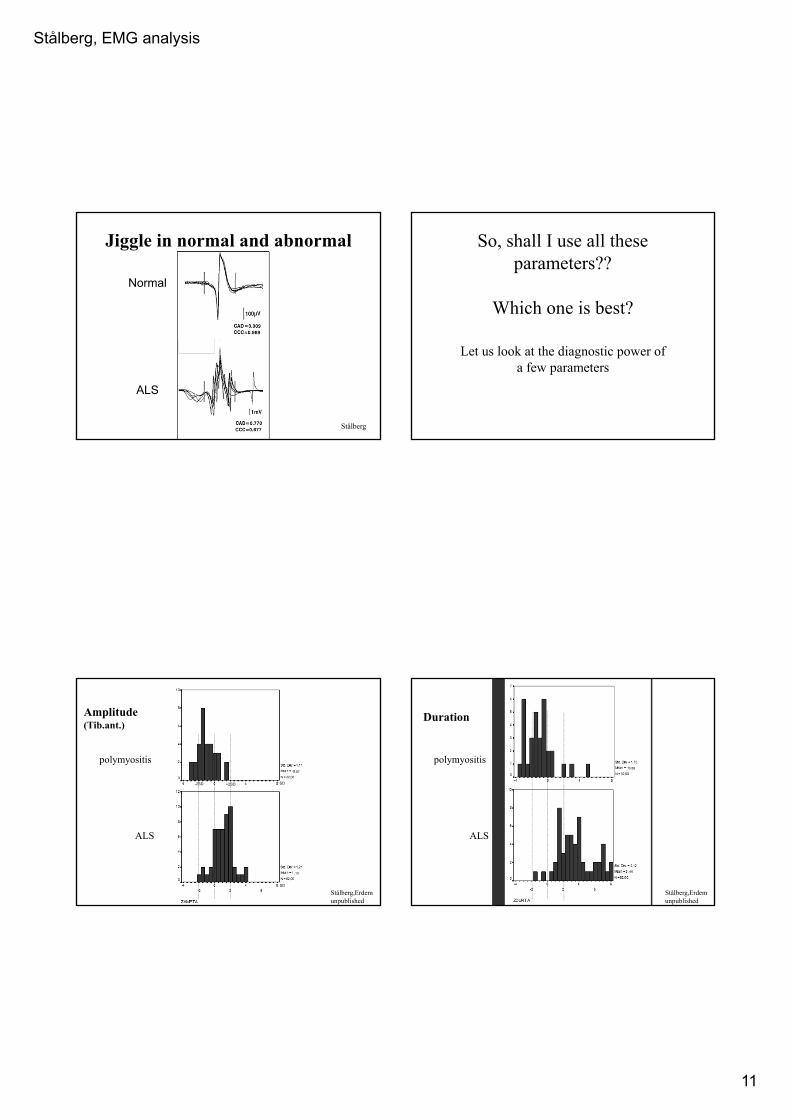
Jiggle in normal and abnormal MUPs
Stålberg
Normal
ALS
So, shall I use all these parameters??
Which one is best?
Let us look at the diagnostic power of a few parameters
Amplitude(Tib.ant.)
0.87
,13
polymyositis
ALS
Stålberg,Erdemunpublished
SD
SD
-2SD +2SD
Duration
0.88
.46
polymyositis
ALS
Stålberg,Erdemunpublished
Stålberg, EMG analysis
12
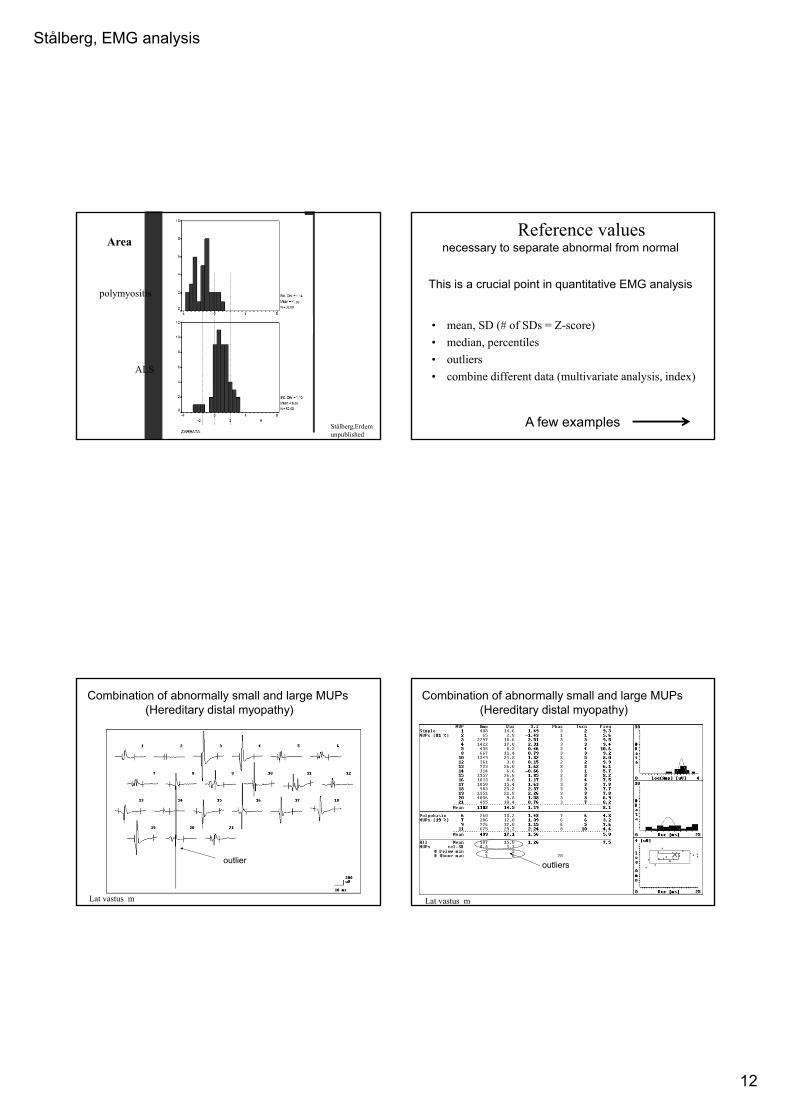
Area
.36
0,85
polymyositis
ALS
Stålberg,Erdemunpublished
Reference valuesnecessary to separate abnormal from normal
This is a crucial point in quantitative EMG analysis
• mean, SD (# of SDs = Z-score)
• median, percentiles
• outliers
• combine different data (multivariate analysis, index)
A few examples
Lat vastus m
outlier
Combination of abnormally small and large MUPs (Hereditary distal myopathy)
Lat vastus m
Combination of abnormally small and large MUPs (Hereditary distal myopathy)
outliers
Stålberg, EMG analysis
13
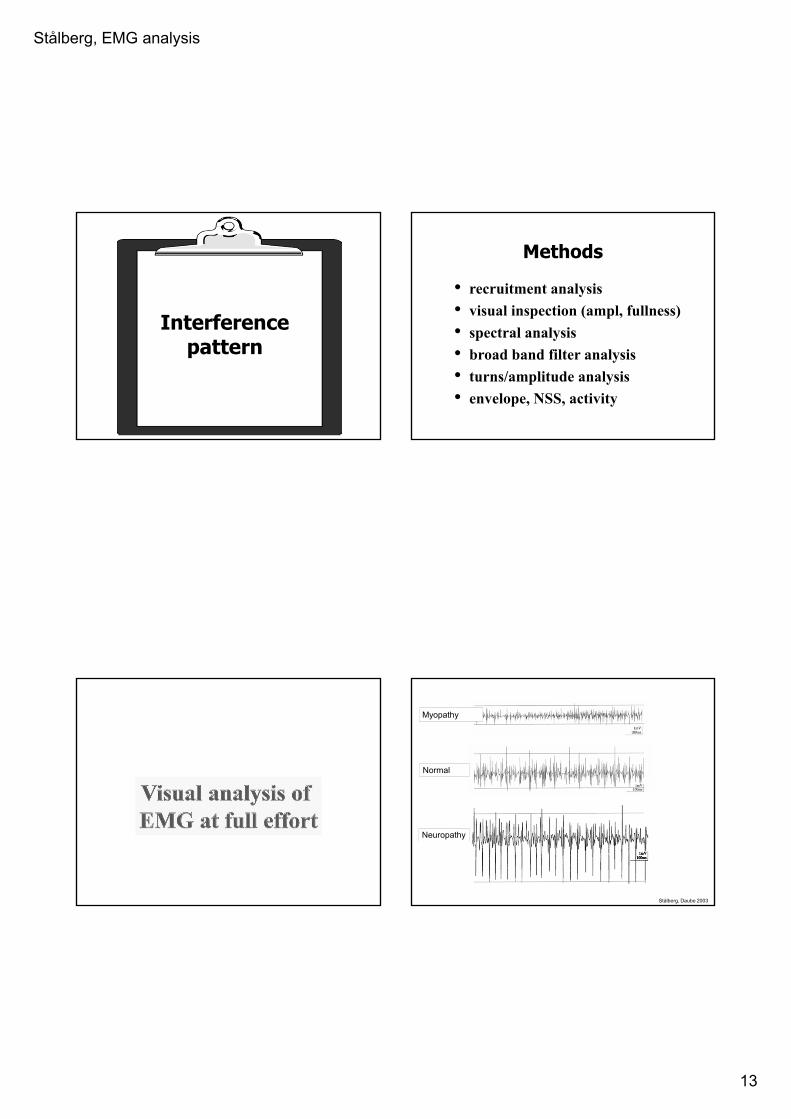
Interferencepattern
Methods
• recruitment analysis
• visual inspection (ampl, fullness)
• spectral analysis
• broad band filter analysis
• turns/amplitude analysis
• envelope, NSS, activity
Stålberg, Daube 2003
Myopathy
Normal
Neuropathy

Stålberg, EMG analysis
14
Frequency bands in EMG, schematic
0
5
10
15
1 2 3 4 5 6 7 8 9 10 11 12
normal
0
5
10
15
20
1 2 3 4 5 6 7 8 9 10 11 12
neuropathy
0
5
10
15
1 2 3 4 5 6 7 8 9 10 11 12
myopathy
0-50 200-300 1000 Hz
0-50 200-300 1000 Hz
0-50 200-300 1000 Hz
“LUCIA”
EMG power spectrum
Neuropathy Normal Myopathy
mBiceps brachii
A Fuglsang-Frederiksen
Turns-Ampl (TA) analysis
normal neuropathymyopathy
Stålberg, EMG analysis
15
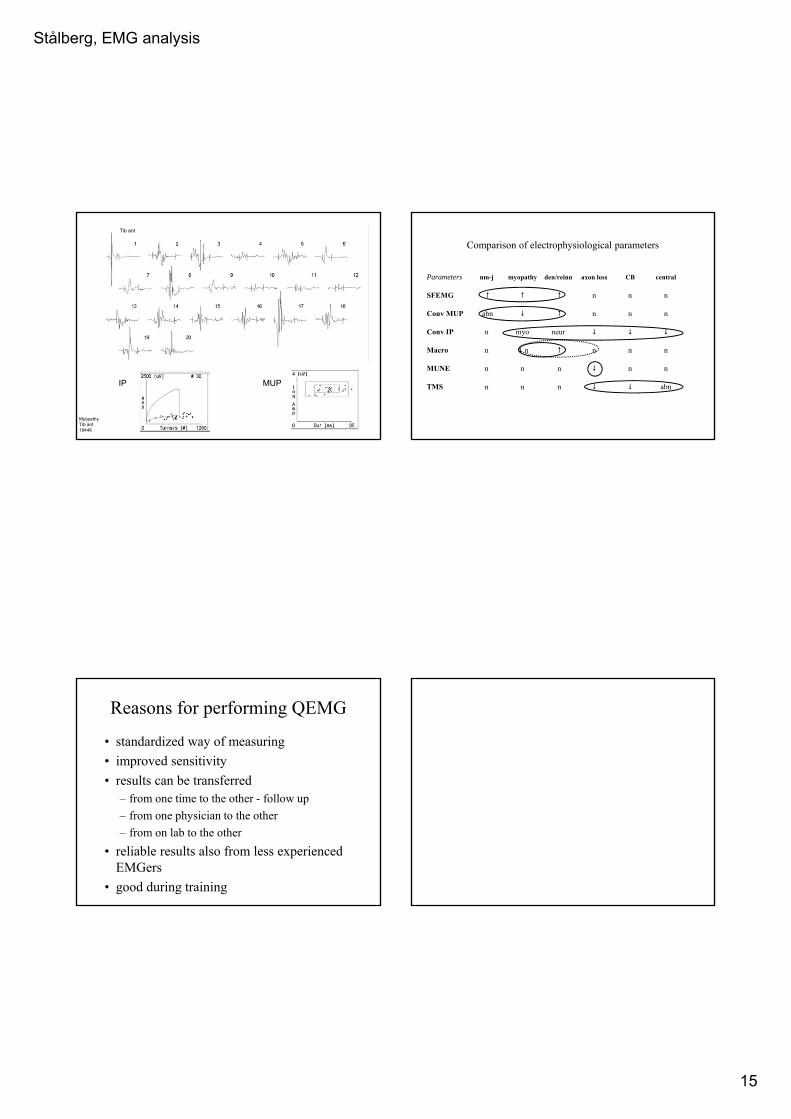
MyopathyTib ant18446
IP MUP
Tib ant
Comparison of electrophysiological parameters
Parameters nm-j myopathy den/reinn axon loss CB central
SFEMG n n n
Conv MUP abn n n n
Conv IP n myo neur
Macro n n n n n
MUNE n n n n n
TMS n n n abn
Reasons for performing QEMG
• standardized way of measuring
• improved sensitivity
• results can be transferred– from one time to the other - follow up
– from one physician to the other
– from on lab to the other
• reliable results also from less experienced EMGers
• good during training








![Periodogram and Ensemble Empirica Mode Decomposition ... · electromyogram EMG signal analysis [1]. In clinical EMG is consist of the waveforms called the Motor Unit Action Potentials](https://img.dokumen.tips/doc/110x75/5fc1600db24ce869895f9284/periodogram-and-ensemble-empirica-mode-decomposition-electromyogram-emg-signal.jpg)




















