Embed Size (px)
Citation preview

Steps to better asthma careA guide for primary care

Contents1. MONITORING
Annual reviews
Asthma control test
Lung function
Asthma self-management plans
2. ACUTE ASTHMAOxygen
Bronchodilators
Nebulisers
Oral corticosteroidsAntibiotics
3. CHRONIC ASTHMAInhaled therapy Spacers Oral corticosteroids Allergies and allergen avoidance
APPENDICESAsthma control testSelf-management plan for adultsAction plan for childrenTherapySummary of stepwise management in adultsSummary of stepwise management in children <5Summary of stepwise management in children 5-12Asthma transitional care pathway
Annual reviews• Quality and Outcomes Framework (QOF) indicator Asthma 6
concerns reviewing a patient’s asthma control every 15 months • This review should include:
– PEFR – best of three– drug therapy – consider ‘step-down’ in therapy– inhaler technique – consider standardising inhaler types– structured self-management plan - for appropriate patients– exacerbations – consider inhaler combinations– patient’s asthma control – using asthma control test– patient’s height – needed for PEFR– patient’s weight – obesity affects pulmonary function and
increases steroid insensitivity– smoking status – adversely affects all aspects of asthma care.
MONITORING
Asthma control test• Asthma control is best assessed using direct questions like “How many times
a day do you use your inhaler?”• Using broad non-specific questions like “how are you managing your
inhalers?” may under-estimate asthma control
• The Respiratory Managed Clinical Network (MCN) recommends that the asthma control test (ACT) be used at all ‘yearly’ assessments
• The ACT is validated (the RCP 3 questionnaire is not)• The ACT is easy and the patient can quickly fill it in• It gives an excellent indication of asthma control over a period of time (four
weeks) • It provides a numerical score that is easy to interpret• The results of the test are easily translated into actions or changes in
treatment.
MONITORING
• Measuring a PEFR is advised for all patients in a community setting - use the best of three efforts
• In the majority of asthmatics symptom-based monitoring is adequate• Asthma symptom scores can improve asthma control • The addition of PEFR monitoring does not improve care• Patients who have any of the following should be monitored closely:
– poor lung function – permanent reduction in lung function measured by PEFR or spirometry
– exacerbation(s) in the previous year – poor perception of bronchoconstriction – demonstrated during an acute episode
of asthma. The patient’s subjective assessment is milder than an objective assessment and is not commensurate with severity of the situation
– co-existing food allergy– patients who have had an admission to HDU/ITU.
• Spirometry monitoring for uncomplicated asthma, should not be done. It may be specifically indicated in patients who attend a hospital clinic.
Lung function
MONITORING

Asthma self-management plans• There is good evidence that a self-management plan (SMP)
improves the control of asthma in adults and children• All patients would benefit from using an SMP • A personalised asthma action plan (PAAP) is used by carers of
children and patients with learning disability - it has the same proven benefits of an SMP
• For practical reasons target the following specific patients to use an SMP:– patients who are using an ICS inhaler daily – patients who have at any time had an acute episode of asthma
requiring steroids.• All target patients should have the agreed Lothian SMP in place
as part of their asthma care.
MONITORING
Self-management plans for adults and children

Oxygen• Give supplementary oxygen to all hypoxaemic patients with acute
severe asthma to maintain an SpO2 level of 94 to 98%
• All clinicians should have access to an oximeter and be familiar with its use
• Any patient of any age should have their oxygen saturation estimated during and acute asthma episode
• The lack of pulse oximetry should not prevent the use of oxygen• All results below 92% should be believed and not blamed on
instrument malfunction.
ACUTE ASTHMA
Adult oximeters do not work with children

Oxygen• If oxygen saturation falls below 92% and symptoms are not
brought quickly under control consider admitting the patient to hospital
• All adult patients with SpO2 < 92% (irrespective of whether the patient is on air or oxygen) or who have any other features of life threatening asthma require arterial blood gases
• All patients must have oxygen available when being transported to hospital especially when they are known to be hypoxaemic.
ACUTE ASTHMA
Children only have arterial blood gases measured when they are ventilated
Features of life threatening asthma

Bronchodilators• pMDI with a spacer is as effective as a nebuliser in treating mild and
moderate exacerbations of asthma in children and adults• ß-agonist- use the appropriate large or small volume spacer
– adults:• up to 20 puffs, one puff at a time
• all puffs should be spaced every 30 seconds
• maximise ß-agonist dose from the onset of an exacerbation, and for four days thereafter
– children:• up to 10 puffs, one puff at a time
• all puffs should be spaced every 30 seconds
• maximise ß-agonist dose from the onset of an exacerbation and for four days thereafter (four puffs, four times daily).
ACUTE ASTHMA

Nebulisers• Nebulisers should be used in acute asthma with life threatening
features
• Nebulisers can be useful in out-of-hours centres and GP surgeries in relieving an acute attack of asthma
• The nebuliser should be oxygen-driven when possible, using a high flow rate of 6L/min. This reduces the risk of oxygen desaturation which can occur when using air-driven compressors
ACUTE ASTHMA
Features of life threatening asthma

Nebulisers• The initial relief of symptoms may reassure the patient and the
clinician. However, the effects may last a short time and the patient’s symptoms may recur rapidly
• Should relief be temporary the patients should be admitted especially if a child
• All patients who are nebulised must be observed for at least 30 minutes after the administration of the drugs to assess the effect.
ACUTE ASTHMA

Oral corticosteroids
• Doubling the dose of an ICS inhaler at the time of an exacerbation is of unproven value despite being recommended for both adults and children in previous guidelines and management plan
• Oximetry and PEFR measurements should be done repeatedly during an acute asthmatic attack
ACUTE ASTHMA
RHSC letters will detail steroid regimes for children
Lothian Joint Formulary
Adults 40 to 50mg prednisolone 5 days
Children
2 - 5 years 20mg prednisolone 3 days
> 5 years 30-40mg prednisolone 3 days

Antibiotics• Antibiotics continue to be used in Lothian to treat asthma. This
happens both in community and hospital settings
• There is no evidence that they help patients during an acute episode of asthma unless:– asthma not settling after three days and the chest signs change
– there are clear signs of chest infection initially.
ACUTE ASTHMA

Inhaled therapy• Patients should be offered an ICS inhaler if they use their ß-
agonist inhaler more than three times per week or have had an exacerbation in the past two years
• It is generally considered that combination inhalers aid compliance and also have the advantage of guaranteeing that any long-acting β2-agonist is not taken without the inhaled steroids
• Remember to start with lower dose combined inhalers – lower doses are the most cost effective
• Remember step-up and step-down drug regimes
CHRONIC ASTHMA

Inhaler technique• Good inhaler technique is central to good care and control. It must
be repeatedly re-taught• Use the “teach-back’ technique:
– “Please show me how you will use the asthma inhaler, so I can be sure I have given you clear instructions”
CHRONIC ASTHMA

Teach-back techniqueCHRONIC ASTHMA
Adobe Acrobat Document

Inhaler types
• Metered dose inhalers
• forceful propellant therefore gentle inhalation
CHRONIC ASTHMA

Inhaler types
• Dry powder inhalers
• gentle (no) propellant therefore forceful inhalation
CHRONIC ASTHMA

• Rationalise inhaler types
• If possible adult patients should be on:
– all MDI inhalers – all DPI inhalers.
• Children should be on:– an MDI preventer inhaler plus spacer– a reliever inhaler of choice in line with school policy and
ability to use the device.
Inhaler types
CHRONIC ASTHMA

Nebulisers• Nebulisers do not improve control
• Patients can overdose if relief is not quickly achieved, and this is dangerous.
• Patients using nebulisers tend to present later for medical help and so increase the risks of complications, including death, during severe acute episodes
• Nebulisers may be suggested after a hospital assessment in very specific circumstances and only for specific patients
• Evidence from around the world indicates that nebulisers should not be routinely used by patients with chronic asthma.
CHRONIC ASTHMA

Spacers• The spacer should be compatible with the pMDI being used• The drug should be administered by repeated single actuations of
the metered dose inhaler into the spacer, each followed by inhalation
• There should be minimal delay between pMDI actuation and inhalation
• Tidal breathing is as effective as single breaths• Spacers should be cleaned monthly rather than weekly as per
manufacturer’s instructions• Spacers should be washed in water with detergent and allowed to
dry in air before use• Plastic spacers should be replaced at least every 12 months.
CHRONIC ASTHMA

Oral corticosteroids• Occasionally patients may need daily oral steroid maintenance
therapy. This should only be initiated by secondary care• The patient should be monitored in secondary care • The patient will need regular checks for complications eg
osteoporosis and diabetes
• All patients who are prescribed steroids should be given a steroid alert card and monitored for osteoporosis.
CHRONIC ASTHMA
Lothian Joint Formulary

Allergies and allergen avoidance• Increased allergen exposure in sensitised individuals is associated
with:– increase in asthma symptoms– bronchial hyper-responsiveness – deterioration in lung function.
• The identification of an allergen comes primarily from a good, careful, clinical history. There is rarely any advantage in doing tests for a battery of allergens
• Measuring total IgE is of little practical help. Raised levels only confirm sensitisation and do not always correlate with a clinically allergic response. A raised allergen-specific IgE must have a corresponding clinical history. A careful clinical history must precede any IgE testing, especially with suspected food allergy, to confirm allergy
CHRONIC ASTHMA

Allergies and allergen avoidance
• Studies of individual aeroallergen avoidance strategies show that single interventions have limited or no benefit. A multi-faceted approach is more likely to be effective if it addresses all the indoor asthma triggers
CHRONIC ASTHMA
Animal allergens• Animal allergens, particularly from cats and dogs, are potent
provokers of asthma symptoms. It may take up to 18 months after the removal of the animal from the environment for any effect to be felt due to lingering dander
• The reported effects of removal of pets from homes are paradoxical. They show either no benefit for asthma, or the potential for continued high exposure to induce a degree of tolerance
• In homes where there is no cat but still detectable cat allergen, there may be a benefit from introducing additional avoidance measures such as air filters and high efficiency vacuum cleaners for cat allergic patients.
CHRONIC ASTHMA

Dust mites• Measures to decrease house dust mites have been shown to
reduce their numbers, but have not been shown to have an effect on asthma severity.
• Families with evidence of house dust mite allergy and who wish to try mite avoidance may consider the following:– complete barrier bed-covering systems– removal of carpets– removal of soft toys from bed– high temperature washing of bed linen– acaricides to soft furnishings– good ventilation with or without dehumidification.
CHRONIC ASTHMA

Asthma control test

Asthma self-management plan


Asthma action plan for children


Therapy
• There follows the therapy guidance diagrams used in the SIGN guideline
• All guidelines recommend reviewing a patient’s medication and all suggest that doctors should consider a step-down approach when appropriate
• This is done frequently in secondary care when patients are referred for reassessment, but occurs less often in primary care
• In practice GPs and practice nurses often do not step-down medication. We usually presume that a patient with no symptoms is proof of good control, and do not wish to upset the new found clinical improvement by altering the medication again
• The practical result is that patients are often started on too high a dose of inhaler.
SIGN 101 Management of Asthma

Therapy
• Analysis of Lothian prescribing indicates that all prescribing for combined inhalers (LABA/ICS) is rising except for the low dose inhalers. This suggest that patients in Lothian tend to be started on higher dose combined inhalers and not therapy at the lowest dose
• The first prescription of combined inhalers should start at the lowest dose inhaler. If after one month there has been no improvement in the symptom control then a higher dose prescription can be considered (each change in dose needs at least one month to test its full symptomatic effectiveness)
• Starting on the lowest dose of combined inhaler and working up in doses may be a practical strategy for a patient’s clinical care and may have an added benefit for the prescribing budget.
SIGN 101 Management of Asthma

Summary of stepwise management in adults
SIGN 101 Management of Asthma

Summary of stepwise management in children under 5 years of age
SIGN 101 Management of Asthma

Summary of stepwise management in children aged 5 to 12 years
SIGN 101 Management of Asthma

Asthma transitional care pathway


Features of life threatening asthma
return to previous slide
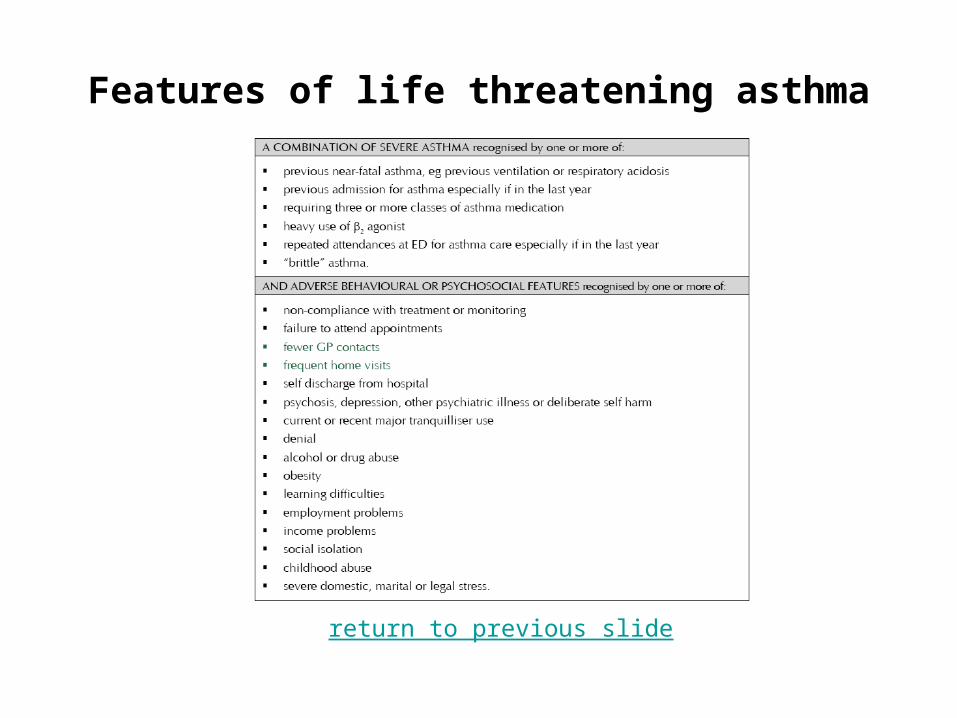
Features of life threatening asthma
return to previous slide





























